Embed Size (px)
Citation preview
©Copyright 2011 MediMedia Animal Health. This document is for internal purposes only. Reprinting or posting on an external website without written permission from MMAH is a violation of copyright laws.
Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E1
In collaboration with the American College of Veterinary Surgeons
CE Article3 CECREDITS
Paranasal Sinus Disease in HorsesR. Wayne Waguespack, DVM, MS, DACVSJennifer Taintor, DVM, MS, DACVIMAuburn University
The paranasal sinuses are susceptible to infections that extend from the nasal cavity or from the alveoli of the caudal upper cheek teeth. The diagnosis and treatment of
paranasal sinus disease in horses can be complicated. The large size and complex anatomy of the sinuses can allow a pathologic process to be present for weeks or months before any external signs, such as facial swelling or nasal discharge, are noticed by the owner or veterinarian. This can negatively affect the prognosis for a successful outcome and may make treatment of paranasal sinus disease frustrating for clients and clinicians.
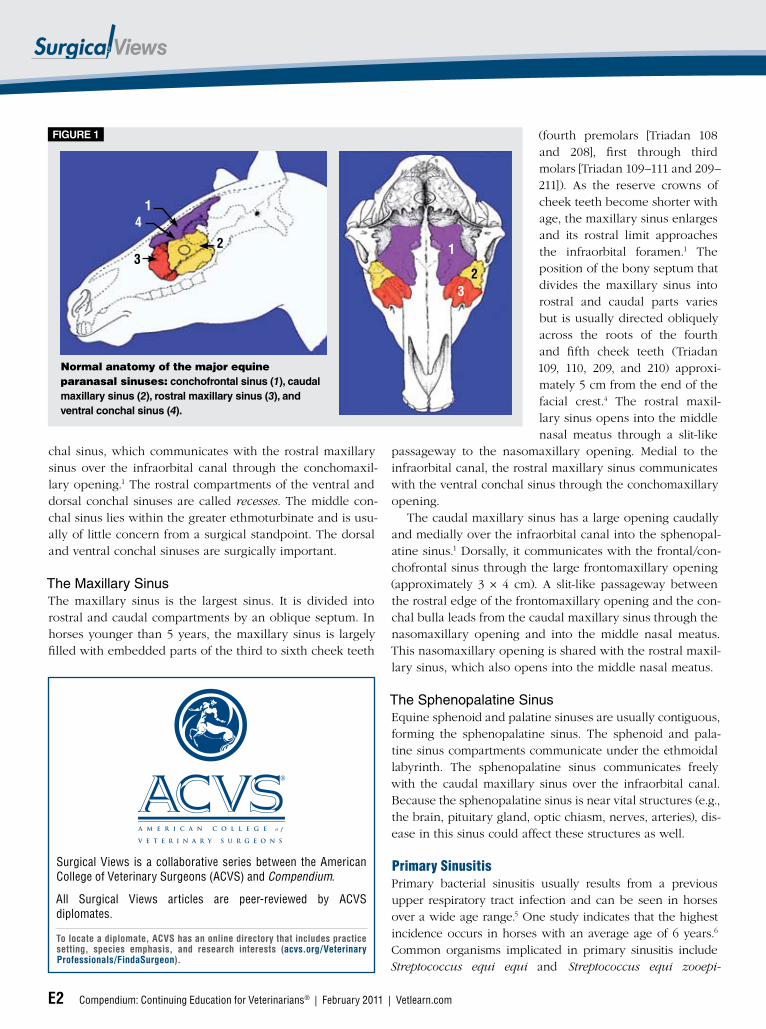
Normal AnatomyThe horse’s extensive paranasal sinus system consists of six pairs of sinuses: the frontal and dorsal conchal sinuses (commonly known as the conchofrontal sinus), the ventral conchal sinus, the sphenopalatine sinus, and the rostral and caudal maxillary sinuses1 (FIGURE 1). The major clinically sig-nificant sinuses are the frontal and maxillary sinuses. All the sinuses communicate with the nasal cavity directly (maxil-lary sinuses) or indirectly (dorsal, middle, and ventral conchal sinuses; frontal sinus; and sphenopalatine sinuses) through the maxillary sinus.1 The conchae (turbinates) are delicate scrolls of bone that are attached laterally in the nasal passage and contain the conchal sinuses. The paranasal sinuses are lined with respiratory mucous membrane composed largely of pseudostratified columnar ciliated epithelium and goblet cells.2 The blood flow to the frontal sinus is provided largely by the ethmoidal artery, and the maxillary sinus is supplied
by branches of the sphenopalatine artery. The major blood supply to the ethmoidal area is the arterial ethmoidal rete, which is formed from anastomosis of the internal and exter-nal ethmoidal arteries, and a minor source is the caudal nasal branch of the sphenopalatine artery.3
The Frontal SinusThe frontal sinus occupies most of the skull medial to the ocular orbit. More specifically, the frontal sinus extends from a point midway between the infraorbital foramen and the medial canthus of the eye to a point midway between the caudal margins of the orbit in mature horses. The right and left frontal sinuses are separated along the midline by a complete septum (FIGURE 1). The sinus overlaps both cranial nasal cavities and occupies the closed part of the dorsal con-cha. The conchofrontal sinus is formed by extensive com-munication between the rostromedial aspect of the frontal sinus and the dorsal conchal sinus. A portion of the floor of the frontal sinus is molded over the ethmoidal labyrinth; ros-trolaterally, there is a large oval communication (frontomaxil-lary aperture) with the caudal maxillary sinus that normally allows natural drainage from the paranasal sinuses.1
The Conchal SinusesEach conchal sinus is divided into a rostral and caudal compartment by a septum. The caudal compartment of the dorsal concha forms the dorsal conchal sinus. The caudal compartment of the ventral concha forms the ventral con-
Abstract: The paranasal sinus system of horses is complex, comprising six pairs of sinuses. Disease processes that can develop in the sinuses include ethmoid hematomas, cysts, neoplasia, and bacterial and fungal infections. Horses that develop paranasal sinus disease vary widely in age. A significant number of clinical conditions involving the paranasal sinuses require a combination of diagnostic tests to determine the specific pathologic process. Because of the anatomic location of the paranasal sinuses and associated chronic conditions that affect many patients, many disease processes involving the paranasal sinuses require surgical correction for a favorable prognosis. Fungal and neoplastic processes of the equine paranasal sinuses have a less favorable prognosis than bacterial and other disease processes.
E2 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
chal sinus, which communicates with the rostral maxillary sinus over the infraorbital canal through the conchomaxil-lary opening.1 The rostral compartments of the ventral and dorsal conchal sinuses are called recesses. The middle con-chal sinus lies within the greater ethmoturbinate and is usu-ally of little concern from a surgical standpoint. The dorsal and ventral conchal sinuses are surgically important.
The Maxillary SinusThe maxillary sinus is the largest sinus. It is divided into rostral and caudal compartments by an oblique septum. In horses younger than 5 years, the maxillary sinus is largely filled with embedded parts of the third to sixth cheek teeth
(fourth premolars [Triadan 108 and 208], first through third molars [Triadan 109–111 and 209–211]). As the reserve crowns of cheek teeth become shorter with age, the maxillary sinus enlarges and its rostral limit approaches the infraorbital foramen.1 The position of the bony septum that divides the maxillary sinus into rostral and caudal parts varies but is usually directed obliquely across the roots of the fourth and fifth cheek teeth (Triadan 109, 110, 209, and 210) approxi-mately 5 cm from the end of the facial crest.4 The rostral maxil-lary sinus opens into the middle nasal meatus through a slit-like
passageway to the nasomaxillary opening. Medial to the infraorbital canal, the rostral maxillary sinus communicates with the ventral conchal sinus through the conchomaxillary opening. The caudal maxillary sinus has a large opening caudally and medially over the infraorbital canal into the sphenopal-atine sinus.1 Dorsally, it communicates with the frontal/con-chofrontal sinus through the large frontomaxillary opening (approximately 3 × 4 cm). A slit-like passageway between the rostral edge of the frontomaxillary opening and the con-chal bulla leads from the caudal maxillary sinus through the nasomaxillary opening and into the middle nasal meatus. This nasomaxillary opening is shared with the rostral maxil-lary sinus, which also opens into the middle nasal meatus.
The Sphenopalatine SinusEquine sphenoid and palatine sinuses are usually contiguous, forming the sphenopalatine sinus. The sphenoid and pala-tine sinus compartments communicate under the ethmoidal labyrinth. The sphenopalatine sinus communicates freely with the caudal maxillary sinus over the infraorbital canal. Because the sphenopalatine sinus is near vital structures (e.g., the brain, pituitary gland, optic chiasm, nerves, arteries), dis-ease in this sinus could affect these structures as well.
Primary SinusitisPrimary bacterial sinusitis usually results from a previous upper respiratory tract infection and can be seen in horses over a wide age range.5 One study indicates that the highest incidence occurs in horses with an average age of 6 years.6 Common organisms implicated in primary sinusitis include Streptococcus equi equi and Streptococcus equi zooepi-
Surgical Views is a collaborative series between the American College of Veterinary Surgeons (ACVS) and Compendium.
All Surgical Views articles are peer-reviewed by ACVS diplomates.
To locate a diplomate, ACVS has an online directory that includes practice setting, species emphasis, and research interests (acvs.org/Veterinary Professionals/FindaSurgeon).
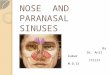
FIGURE 1
Normal anatomy of the major equine paranasal sinuses: conchofrontal sinus (1), caudal maxillary sinus (2), rostral maxillary sinus (3), and ventral conchal sinus (4).
1
1
23
4
23
Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E3
demicus.7,8 Inflammation and swelling in the nasal mucosa caused by a viral or bacterial infection can obstruct the naso-maxillary opening, preventing normal sinus drainage from the rostral and caudal maxillary sinuses and thereby predisposing equine patients to sinusitis or exacerbating it.9 Primary sinus-itis usually involves all the sinus cavities but can be confined to the ventral conchal sinus, which can lead to formation of an abscess that is difficult to detect on radiographs and usu-ally requires surgical exploration and treatment.7 Horses with Cushing’s disease may be predisposed to primary sinusitis. However, in a retrospective study by Tremaine and Dixon,6 only 4.5% (three of 67) of horses with primary sinusitis were also diagnosed with Cushing’s disease.
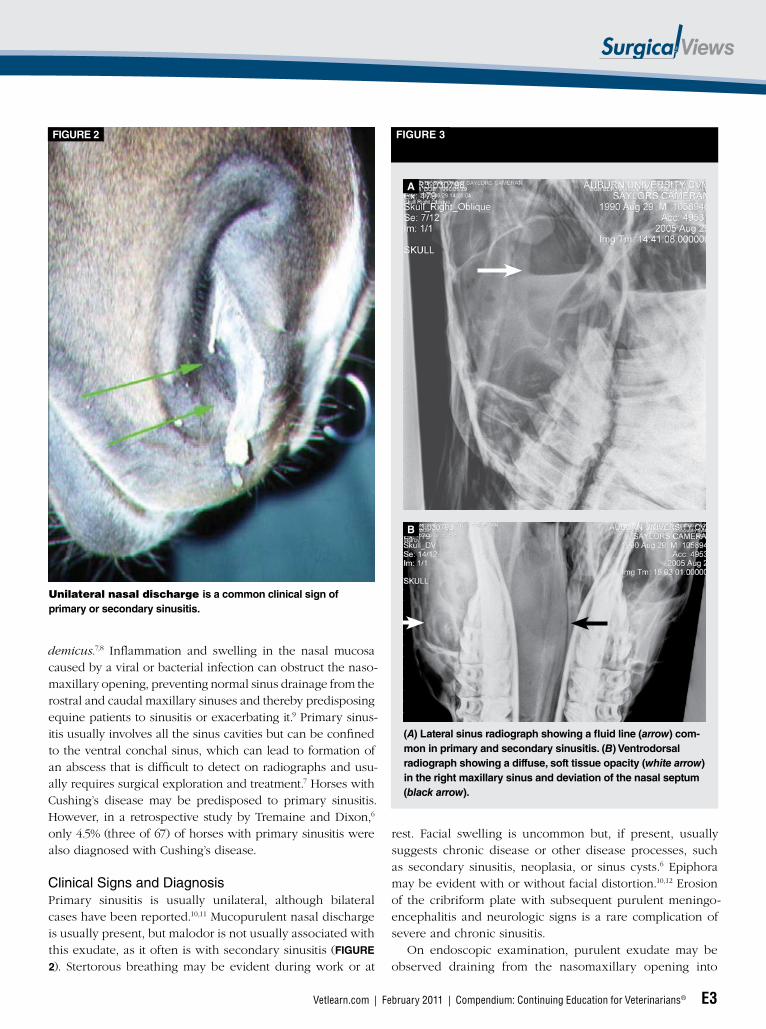
Clinical Signs and DiagnosisPrimary sinusitis is usually unilateral, although bilateral cases have been reported.10,11 Mucopurulent nasal discharge is usually present, but malodor is not usually associated with this exudate, as it often is with secondary sinusitis (FIGURE
2). Stertorous breathing may be evident during work or at
rest. Facial swelling is uncommon but, if present, usually suggests chronic disease or other disease processes, such as secondary sinusitis, neoplasia, or sinus cysts.6 Epiphora may be evident with or without facial distortion.10,12 Erosion of the cribriform plate with subsequent purulent meningo-encephalitis and neurologic signs is a rare complication of severe and chronic sinusitis. On endoscopic examination, purulent exudate may be observed draining from the nasomaxillary opening into
Unilateral nasal discharge is a common clinical sign of primary or secondary sinusitis.
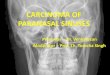
FIGURE 2Sinus radiographs.
FIGURE 3
(A) Lateral sinus radiograph showing a fluid line (arrow) com-mon in primary and secondary sinusitis. (B) Ventrodorsal radiograph showing a diffuse, soft tissue opacity (white arrow) in the right maxillary sinus and deviation of the nasal septum (black arrow).
B
A

E4 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
the middle meatus. On radiographs, opacification of both rostral and caudal maxillary compartments is usually seen. Fluid lines should be evident, and in more severe cases, the contents may appear mineralized (FIGURE 3). If primary sinusitis is confined to the ventral conchal sinus, radiogra-phy may demonstrate a soft tissue density dorsal to the third to fifth cheek teeth and within the ventral conchal sinus.7 However, sinusitis is usually well established on presenta-tion, so radiographic findings are similar to those in FIGURE
3. In one study, concurrent opacification of the frontal sinus was also a common finding and helped differentiate pri-mary from secondary sinusitis.11 Free fluid was more com-mon with primary than with secondary sinusitis.11 Sinoscopy and sinocentesis allow fluid collection for culture and deter-mination of antimicrobial sensitivity. Sinoscopy performed after sinus lavage to remove purulent debris from the sinus may provide clinicians with more information to differenti-ate between primary and secondary sinusitis.
TreatmentTreatment of primary sinusitis is directed at sinus irrigation with a large volume of warm, sterile, physiologic saline and appropriate systemic antimicrobial therapy; however, the patient’s response can be poor in chronic cases.6 Drainage and lavage are accomplished by placing an indwelling cathe-ter percutaneously into the maxillary or frontoconchal sinus or by placing lavage catheters in multiple compartments to facilitate adequate lavage of the paranasal sinuses. Primary
paranasal sinusitis usually resolves in 7 to 10 days with a combination of systemic antimi-crobial therapy and lavage. Some clinicians recommend exercise as part of treatment to stimulate mucus secretion and aid expulsion of sinus exudate. Systemic antimicrobial therapy alone often diminishes or temporarily resolves nasal discharge but rarely eliminates infection. Delayed or ineffective treatment can result in progression of primary sinusitis to osteomy-elitis and advanced necrosis, leading to sig-nificant destruction of soft tissue and bone. Surgical debridement and curettage through a bone flap may be necessary in chronic cases with osteomyelitis and abscessation; how-ever, if the exudate becomes inspissated in the ventral conchal sinus, sinusotomy is war-ranted7,13 (FIGURE 4). This condition should be suspected when primary paranasal sinus-itis does not resolve with the use of systemic antimicrobials and lavage. Diagnostic signs potentially indicating ventral conchal sinus-
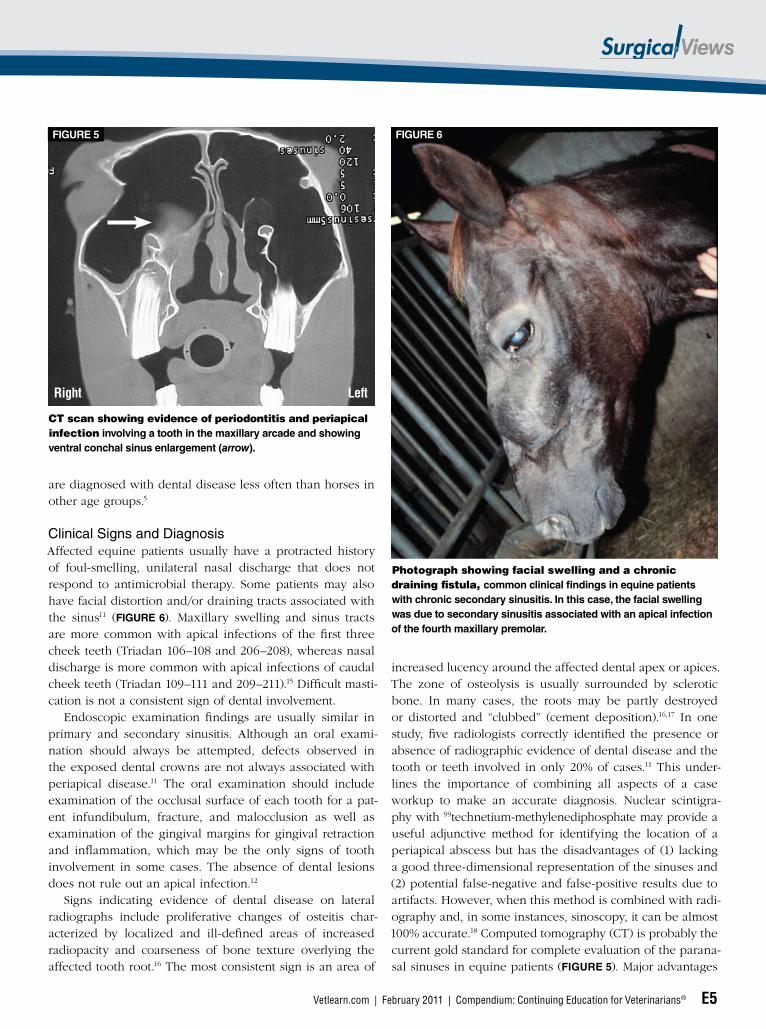
itis are radiographic or computed tomographic evidence of a soft tissue density over the roots of the maxillary fourth premolar (Triadan 108 and 208) and the first (Triadan 109 and 209) and second (Triadan 110 and 210) molars as well as narrowing of the nasal passage caused by accumulation of inspissated exudate in the ventral conchal sinus (FIGURE
5). Surgical treatment includes removal of exudate from the ventral conchal sinus and, if necessary, additional drainage via maxillary sinusotomy or trephination of the frontal sinus. The technique of establishing drainage through a surgically created sinonasal opening has recently been questioned because of potential lack of efficacy.6,9 The surgical opening could alter mucociliary clearance and diminish endogenous production of nitric oxide, which could be bactericidal.6,9 However, in my (R. W. W.) experience, creation of a sino-nasal opening may be necessary to resolve some chronic sinusitis cases. Surgical treatment of inspissated exudate in the ventral conchal sinus can be effective with the patient under general anesthesia or standing sedation.7,9
Secondary SinusitisSecondary sinusitis may be caused by dental disease, facial fractures, granulomatous lesions, or neoplasia. Numerous dental problems can lead to secondary sinus disease; peria-pical disease involving the first molar (Triadan 109 or 209) or the last premolar (Triadan 108 or 208) is the most common.11 Sinusitis secondary to dental disease accounts for at least half of all sinusitis cases.11,12,14 Horses younger than 4 years
Photograph of a frontonasal sinusotomy. This procedure provides the best access to the equine paranasal sinuses and can be performed with the patient either standing or under general anesthesia, depending on the condition being treated.
FIGURE 4
Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E5
are diagnosed with dental disease less often than horses in other age groups.5
Clinical Signs and DiagnosisAffected equine patients usually have a protracted history of foul-smelling, unilateral nasal discharge that does not respond to antimicrobial therapy. Some patients may also have facial distortion and/or draining tracts associated with the sinus11 (FIGURE 6). Maxillary swelling and sinus tracts are more common with apical infections of the first three cheek teeth (Triadan 106–108 and 206–208), whereas nasal discharge is more common with apical infections of caudal cheek teeth (Triadan 109–111 and 209–211).15 Difficult masti-cation is not a consistent sign of dental involvement. Endoscopic examination findings are usually similar in primary and secondary sinusitis. Although an oral exami-nation should always be attempted, defects observed in the exposed dental crowns are not always associated with periapical disease.11 The oral examination should include examination of the occlusal surface of each tooth for a pat-ent infundibulum, fracture, and malocclusion as well as examination of the gingival margins for gingival retraction and inflammation, which may be the only signs of tooth involvement in some cases. The absence of dental lesions does not rule out an apical infection.12 Signs indicating evidence of dental disease on lateral radiographs include proliferative changes of osteitis char-acterized by localized and ill-defined areas of increased radiopacity and coarseness of bone texture overlying the affected tooth root.16 The most consistent sign is an area of
increased lucency around the affected dental apex or apices. The zone of osteolysis is usually surrounded by sclerotic bone. In many cases, the roots may be partly destroyed or distorted and “clubbed” (cement deposition).16,17 In one study, five radiologists correctly identified the presence or absence of radiographic evidence of dental disease and the tooth or teeth involved in only 20% of cases.11 This under-lines the importance of combining all aspects of a case workup to make an accurate diagnosis. Nuclear scintigra-phy with 99technetium-methylenediphosphate may provide a useful adjunctive method for identifying the location of a periapical abscess but has the disadvantages of (1) lacking a good three-dimensional representation of the sinuses and (2) potential false-negative and false-positive results due to artifacts. However, when this method is combined with radi-ography and, in some instances, sinoscopy, it can be almost 100% accurate.18 Computed tomography (CT) is probably the current gold standard for complete evaluation of the parana-sal sinuses in equine patients (FIGURE 5). Major advantages
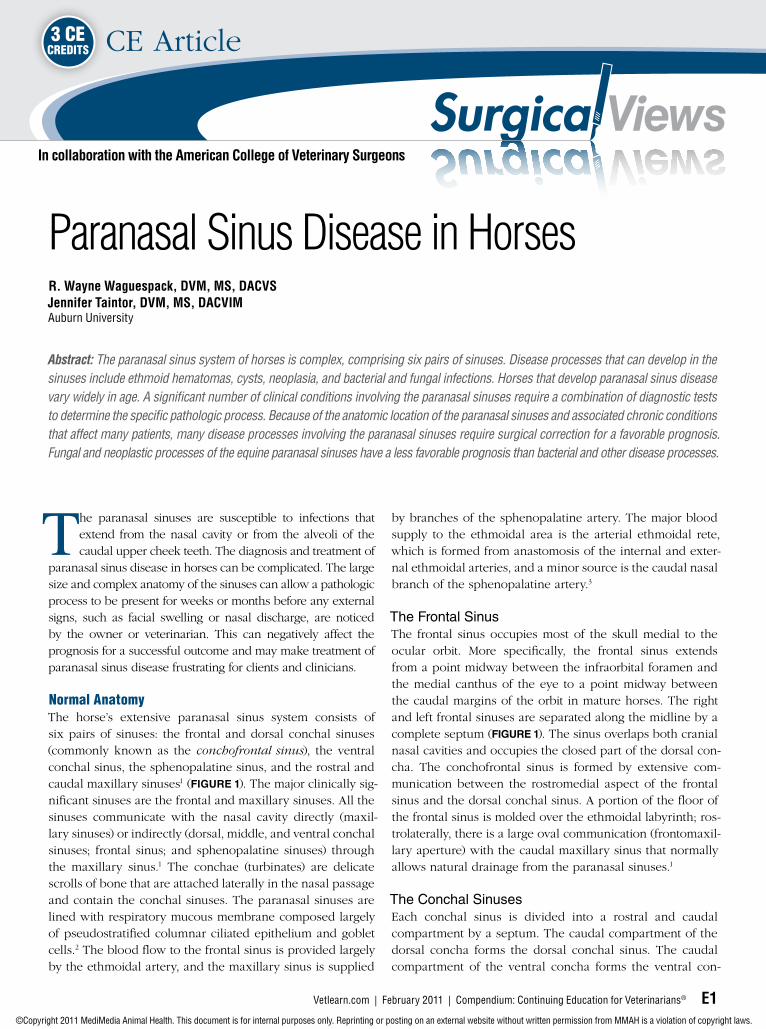
CT scan showing evidence of periodontitis and periapical infection involving a tooth in the maxillary arcade and showing ventral conchal sinus enlargement (arrow).
Photograph showing facial swelling and a chronic draining fistula, common clinical findings in equine patients with chronic secondary sinusitis. In this case, the facial swelling was due to secondary sinusitis associated with an apical infection of the fourth maxillary premolar.
FIGURE 5 FIGURE 6
Right Left
E6 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
of CT include no superimposition of structures as seen on radiographs. In addition, fluid densities can be character-ized, individual tooth roots can be visualized well, and the condition of the sinus openings can be evaluated.19,20 Disadvantages of CT include the need for general anesthesia; however, CT can be performed just before surgery to avoid additional expense and recovery from anesthesia. Magnetic resonance imaging can also be used to evaluate the sinuses, especially when CT is not available.
TreatmentSecondary sinusitis is treated by removing the diseased tooth or other primary problem and abnormal mucosa, irrigating the sinus cavity, and administering systemic antimicrobials. Diseased tooth roots are usually removed via oral extraction, trephination over the appropriate region of the maxillary sinus, or sinusotomy of the frontonasal or maxillary bones. During repulsion, care should be taken to properly seat the punch to avoid trauma to the hard palate and surround-ing alveolar bone. Intraoperative radiographs should be obtained to ensure that all of the affected bone and tooth was removed. After the affected tooth is successfully repelled, dental packing is placed to prevent communication between the sinuses and oral cavity. This is necessary to prevent con-tamination of the sinuses and allow healing of the alveolar bone. Veterinarians have used several materials as dental
packing, such as polymethylmethacrylate and plaster of Paris. The sinus mucosa or membrane must also be removed as completely as possible to avoid postoperative drainage. The affected sinus should be thoroughly and frequently lavaged as described for primary sinusitis. Unsuccessful treatment can be attributed to persistent osteitis, abscesses, failure to remove all the involved root and infected bone, and failure to treat for obligate anaerobes.21
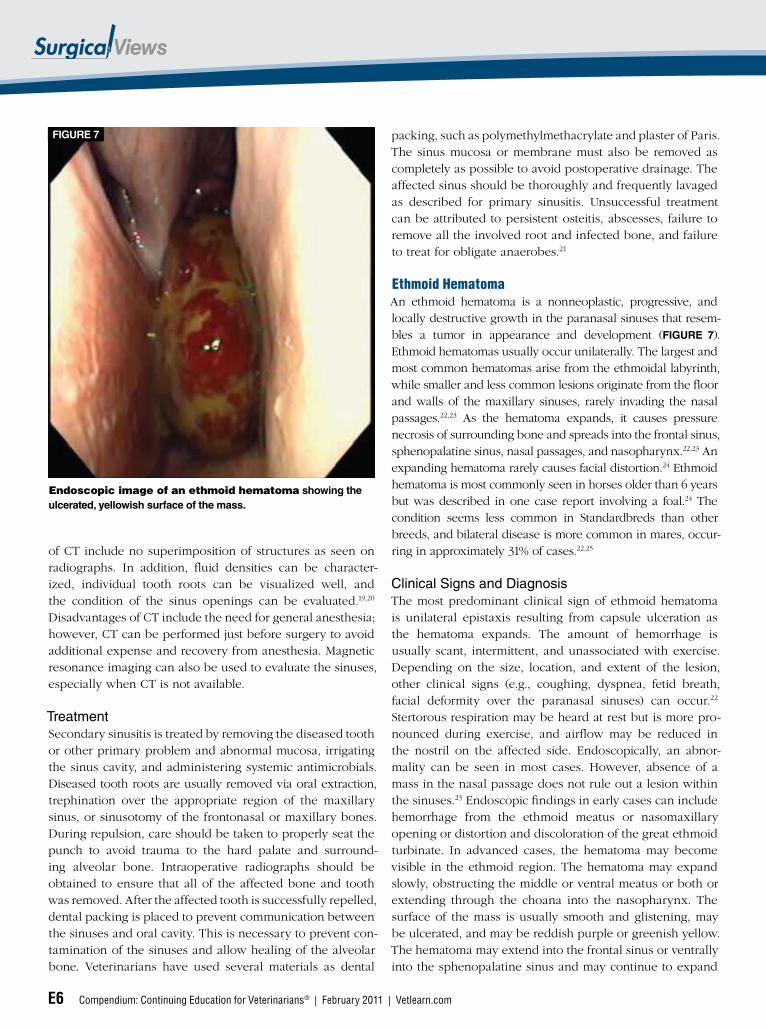
Ethmoid HematomaAn ethmoid hematoma is a nonneoplastic, progressive, and locally destructive growth in the paranasal sinuses that resem-bles a tumor in appearance and development (FIGURE 7). Ethmoid hematomas usually occur unilaterally. The largest and most common hematomas arise from the ethmoidal labyrinth, while smaller and less common lesions originate from the floor and walls of the maxillary sinuses, rarely invading the nasal passages.22,23 As the hematoma expands, it causes pressure necrosis of surrounding bone and spreads into the frontal sinus, sphenopalatine sinus, nasal passages, and nasopharynx.22,23 An expanding hematoma rarely causes facial distortion.24 Ethmoid hematoma is most commonly seen in horses older than 6 years but was described in one case report involving a foal.24 The condition seems less common in Standardbreds than other breeds, and bilateral disease is more common in mares, occur-ring in approximately 31% of cases.22,25
Clinical Signs and DiagnosisThe most predominant clinical sign of ethmoid hematoma is unilateral epistaxis resulting from capsule ulceration as the hematoma expands. The amount of hemorrhage is usually scant, intermittent, and unassociated with exercise. Depending on the size, location, and extent of the lesion, other clinical signs (e.g., coughing, dyspnea, fetid breath, facial deformity over the paranasal sinuses) can occur.22 Stertorous respiration may be heard at rest but is more pro-nounced during exercise, and airflow may be reduced in the nostril on the affected side. Endoscopically, an abnor-mality can be seen in most cases. However, absence of a mass in the nasal passage does not rule out a lesion within the sinuses.23 Endoscopic findings in early cases can include hemorrhage from the ethmoid meatus or nasomaxillary opening or distortion and discoloration of the great ethmoid turbinate. In advanced cases, the hematoma may become visible in the ethmoid region. The hematoma may expand slowly, obstructing the middle or ventral meatus or both or extending through the choana into the nasopharynx. The surface of the mass is usually smooth and glistening, may be ulcerated, and may be reddish purple or greenish yellow. The hematoma may extend into the frontal sinus or ventrally into the sphenopalatine sinus and may continue to expand
Endoscopic image of an ethmoid hematoma showing the ulcerated, yellowish surface of the mass.
FIGURE 7

Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E7
into the caudal or rostral maxillary sinus. Radiographs are useful in determining the size, location, and extent of sinus involvement. The hematoma appears as a smooth-walled, well-circumscribed density that contrasts well with air in the sinus. Because CT provides a cross-sectional view of the skull, it is useful for determining the exact location and extent of the hematoma involvement (FIGURE 8). A tentative diagnosis can be made from the history, clinical signs, endo-scopic appearance, and radiographic findings, but a defini-tive diagnosis can be made only through histopathologic examination of the involved tissue.
TreatmentIf the lesion is not treated, the prognosis is unfavor-able because the hematoma usually enlarges, eventually obstructing the nasal passages and leading to dyspnea.22,26 Ablation of the intranasal portion of the hematoma with a neodymium:yttrium (Nd:YAG) laser and/or intralesional injection of 4% formaldehyde solution can be performed as standing procedures through an endoscope.25,27 Lesions limited to the ethmoid recess that are less than 5 cm in diameter respond more readily to endoscopic Nd:YAG laser therapy but can also be treated with formaldehyde injection. Intralesional 4% formaldehyde treatment is inexpensive and usually free of complications. However, most lesions need to be reinjected with formalin repeatedly, with a period of 3 to 4 weeks between treatments. If the hematoma extends into the sinus, intralesional injection of 4% formaldehyde solu-tion into the sinus component can lead to severe sinusitis, conchal necrosis, and, rarely, destruction of the cribriform plate with subsequent brain damage.28 Surgical treatment for lesions that fail to respond to intralesional formaldehyde injections involves removal of the entire lesion through a frontonasal bone flap with or without ablation by an Nd:YAG laser.25,29 This procedure is usually performed with the patient under general anesthesia in lateral recumbency. The frontonasal approach allows greater access to the lesion because the hematoma may be enclosed in bone. The origin of the hematoma must be removed, which may be difficult if it lies within the ethmoid labyrinth or sphenopalatine sinuses. Identifying the origin may also be difficult due to significant intraoperative hemorrhage originating from the damaged nasal and sinus mucosae or the ethmoid hematoma. It is not unusual to create a communication between the sinus and nasal passage with complete removal of the hematoma. Before surgery, it is recommended to have the horse cross-matched and have a blood donor immediately available for transfusion in case of substantial hemorrhage. In the litera-ture, the recurrence rate after surgical removal of ethmoid hematomas is estimated to be 0% to 44.4%,22,25,30,31 and long-term remission of clinical signs is reportedly 33%.6 Bilateral
lesions have a reported recurrence rate of 43% compared with an 8% rate for unilateral hematomas.25 Repeat endos-copy is recommended every 6 months because recurrence is usually recognized within the first 6 to 12 months following surgery. Recurrence should be based on endoscopic find-ings, not the presence or absence of clinical signs, because evidence of epistaxis does not always indicate recurrence of the lesion.25,27
Sinus CystSinus cysts are extensive lesions of unknown etiology that are single or loculated, fluid-filled (yellow acellular fluid) cavities with an epithelial lining32 (FIGURE 9). They develop in the maxillary sinuses and ventral conchae but can extend into the frontal sinus and nasal cavity.29,32–36 Abnormal devel-opment of embryonic germ tissue (developmental dental cysts) and cystic development caused by repeated submu-cosal hemorrhage (mucoid maxillary sinus cysts) have been proposed as etiologic factors.32,33,35 Histologic examination of excised tissue may help differentiate the two. Most cysts do not have dental involvement. In most reports, histologic findings from excised tissues have been relatively nonspe-cific and have included granulation tissue, neovasculariza-tion, ulceration, and, occasionally, mineralization and bony trabeculation in the cyst wall. In some horses, the cyst appeared to be a part of the sinus lining; in other horses, the sinus appeared to be occupied by a cystic mass that had grown out from the turbinates. A congenital form is a reported cause of facial swelling and dyspnea since birth in foals.37,38 Previously, sinus cysts were thought to occur in young horses only, but studies have confirmed the diagnosis of sinus cysts in older horses.32,33,39
CT scan of an ethmoid hematoma. The hematoma com-pletely fills the paranasal sinuses. (Courtesy of Dan Burba, Louisiana
State University)
FIGURE 8

E8 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
Clinical Signs and DiagnosisThe major clinical signs of a sinus cyst are facial swelling, nasal discharge, sinus dullness on percussion, and airway obstruction. The nasal discharge is usually not hemorrhagic or malodorous.32 On endoscopic examination, the nasal passage appears narrow and the ventral conchae may appear enlarged, or the cyst may
be observed in the nasal passage. Radiographic features are often nonspecific, including dif-fuse sinus opacification, occasional gas–soft tissue interfaces, thickening of overlying bone, distortion of the tooth roots, deviation of the nasal septum, and mineralized densities within the sinus.32,39 Sinocentesis typically results in a large quantity of viscous, clear to amber fluid. Cytologic examination of this fluid is usually unrewarding.
TreatmentSurgical removal of the cyst and involved conchal lining carries a good prognosis for complete recovery. Irrigation of the sinus after surgery removes debris and blood clots from the sinus, accelerating postoperative recovery. The sinuses are frequently so disrupted by the cyst that a large communication is established into the nasal passages after surgery, result-ing in recurrent, but clinically insignificant, mucous discharge in some patients. The recur-rence rate is low with surgical excision.32
Wounds and FracturesBlunt injuries to the frontal sinus and nasal bones caused by kicks from other horses or collisions with fixed objects can cause open or closed wounds to the sinuses (FIGURE 10). Many wounds go unnoticed because the frac-ture fragments may be forced into the sinus cavity and either the skin detaches from the bone or the integrity of the skin is not dis-rupted. As healing occurs, the fracture callus produces a firm subcutaneous swelling along the fracture line, or if there is a depression fracture, a facial concavity is present.
Clinical Signs and DiagnosisEpistaxis and subcutaneous emphysema are common clinical signs of sinus trauma, but dyspnea and epiphora are also possible. In acute cases, it may be possible to feel a hema-toma and fracture fragments. Severe trauma to the head and sinuses can cause ocular and
central neurologic signs. The configuration of the fracture is often defined more readily by physical examination rather than radiography; however, radiographic examination of frac-tures is indicated to detect additional fractures and determine whether there is involvement of the rostral or dorsal aspect of the cranial vault. Fracture fragments and fluid lines from blood
Photograph of a sinus cyst involving the entire conchofrontal sinus. Note the loculated, yellow cystic structure characteristic of a sinus cyst. The cyst is filled with yellow, acellular fluid.
Photograph showing a depression fracture of the maxillary bone. This fracture is unstable, requiring internal fixation. Adequate surgical exposure is needed to fully evaluate and reduce the fracture.
FIGURE 9
FIGURE 10

Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E9
within affected sinuses can be seen on standard radiographic views, but oblique views may be necessary to demonstrate injury. Patients with fractures near the cranial vault should be thoroughly evaluated and monitored for the presence or development of neurologic signs such as blindness, mental depression, ataxia, or vestibular dysfunction. Depression frac-tures involving the orbit cause the globe to collapse into the sinuses and the third eyelid to prolapse.
TreatmentMild, stable depression fractures can be left untreated if cosmesis is not important. Unstable fractures, markedly depressed facial fractures, and fractures of the zygomatic arch should be treated surgically for ocular health. Surgical correction is performed with the patient under general anes-thesia and usually not for at least 24 hours after injury due to possible complications secondary to cranial trauma.40
General goals for surgical repair of facial fractures include reconstruction of facial contours and reduction of potential sequestrum and sinusitis formation by incorporating or dis-carding bony fragments devoid of a blood supply. Surgical reduction of simple depression fractures should initially be attempted through stab incisions to minimize disruption of surrounding soft tissue structures that provide stability and blood flow to the fracture. Successful surgical reconstruc-tion of more extensive facial fractures may require complete field exposure via a generous skin incision.41 Depressed fragments should be elevated and free fragments collected. Fragments can be connected using monofilament absorbable suture or stainless-steel suture. A Steinmann pin or small drill bit can be used to create holes for suture placement. Secure apposition of subcutaneous tissue and skin adds sta-bility and provides access to a blood supply. When fractures near the medial canthus are reconstructed, a special attempt should be made to salvage the nasolacrimal canal. Surgical creation of communication between the proximal part of the nasolacrimal duct and the maxillary sinus has been success-ful when salvage is not possible.42 Equine patients should recover from anesthesia with the surgical site bandaged and, when possible, with a padded head guard. Extensive fractures that invade the sinus or nasal cav-ity should be treated with systemic antimicrobials before surgery and for 10 to 14 days after surgery. Open defects secondary to the initial traumatic event can result from skin or bone loss involving the sinus or nasal cavity. Delayed repair of sinus defects using muscle flaps or periosteal flaps has also been described.43,44
Sinus NeoplasiaNeoplasia of the paranasal sinuses is rare in horses. Although several reports of individual cases have been reported in the
literature, the incidence of sinus neoplasia is approximately less than 1% of sinus diseases.6,45–48 In older horses, reported tumor types include squamous cell carcinoma (SCC; the most common), adenocarcinoma, fibrosarcoma, osteoma, osteo-sarcoma, myxoma, myxosarcoma, and unspecified carcino-mas; in young horses (younger than 2 years), fibrosarcoma, osteoma, and osteosarcoma are typically reported.6,45–58
Although tumors can develop at a variety of sites within the paranasal sinuses, certain tumor types have a predi-lection for development at specific locations, most likely as a result of the histologic differences of mucosae. SCCs and bony tumors are frequently encountered in the maxil-lary sinus, while adenocarcinomas appear more commonly in the frontal sinus.6,45,47,51 While these tumors are locally aggressive, expanding into surrounding tissue, metastasis is rare.
Clinical Signs and DiagnosisThe most common clinical signs of neoplasia include unilat-eral mucopurulent or purulent nasal discharge, facial swell-ing, and reduced nasal airflow. Additional reported clinical signs include epistaxis, bilateral nasal discharge, dyspnea, ocular discharge, epiphora, head shaking, localized lymph node involvement, and neurologic deficits. Because of the tortuous ostia between the nasal cavity and paranasal sinus, nasal endoscopic examination of the paranasal sinuses is not possible.6,59 The paranasal sinuses can be directly examined by sinoscopy; however, mucopu-rulent material or the tumor may prevent adequate visual-ization.6,59 Radiography combined with CT of the sinuses provides the most definitive information regarding the loca-tion of the mass and the extent of involvement of surround-ing tissues, but these diagnostic tools cannot differentiate
CT scan of a horse with osteosarcoma involving the left nasal cavity and paranasal sinuses (arrows). Radiography combined with CT of the sinuses provides the most definitive information regarding the location of the mass and the extent of involvement of surrounding tissues. Definitive diagnosis was made by histopathologic examination of a biopsy specimen of the mass.
FIGURE 11

E10 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
between neoplasia and sinonasal masses6,47,49 (FIGURE 11). Definitive diagnosis can be made by histopathologic exami-nation of a biopsy specimen of the mass, preferably from deep within the tumor because a superficial sample may show only inflammatory cells or necrotic debris.6,45–49,58,60
Treatment and PrognosisSurgical treatment is typically unrewarding due to the extent of local destruction at the time of diagnosis and the pro-pensity for recurrence, especially with carcinomas.45,47,49,60,61 However, osteomas respond well to surgical removal because they are benign and usually form well-circumscribed lesions with pedunculated or sessile attachments.46,47,49,55,57,60,61 Use of external beam radiation therapy as a primary treatment (only for SCCs) and an adjunct to surgical removal (only for fibromas) has reportedly been somewhat successful in treat-ing paranasal neoplasia in equine patients.47,62,63 For other types of neoplasia, there are not enough data regarding the efficacy of external beam radiation therapy.
Fungal InfectionsFungal infections of the paranasal sinuses are rare. Saprophytes (e.g., Cryptococcus neoformans, Coccidioides immitis, Allescheria boydii, Pseudallescheria boydii), com-monly found in manure and soil, are typically reported. These organisms have been isolated from granulomas in the fron-tal, maxillary, sphenopalatine, and conchal sinuses.6,47,49,64–66 These granulomas can cause progressive bone destruction, resulting in involvement of localized structures, such as the eyes and brain. Although fungal infection has been reported to disseminate to other organs, such as the lungs and jeju-num, it is extremely rare.47 Localized or diffuse sinusitis caused by Aspergillus and Penicillium spp has also been reported.47 When dealing with horses with cryptococcosis, veterinarians and owners need to remember the zoonotic potential of Cryptococcus spp.58
Clinical Signs and DiagnosisClinical signs of fungal infection are similar to those of neo-plasia and sinusitis: unilateral nasal discharge, facial defor-mity, and obstructed airflow. Depending on the size of the granuloma and involvement of localized tissues, blindness, exophthalmos, and swelling of the periorbital region may be observed. Radiographic examination of the sinuses may show a soft tissue density of the affected sinus, while endoscopic examination of the sinuses may show a lobulated or non-lobulated mass extending from the paranasal sinus into the nasal cavity. Aspiration or biopsy of the mass is needed to make a definitive diagnosis.
TreatmentTreatment of fungal infection consists of surgical removal or debulking and/or antifungal therapy. Topical application of amphotericin B, miconazole, and natamycin; local injec-tion of amphotericin B; and/or systemic administration of iodides, amphotericin B, and ketoconazole have been used with variable effects in treating sinus granulomas.45,47,61,64 A horse with P. boydii sinusitis had a successful outcome after topical application of miconazole and systemic administra-tion of sodium iodide.64 Topical application of enilconazole or natamycin has had favorable results in treating Aspergillus spp sinusitis.47,67 However, the prognosis for successful treat-ment of fungal infections of the paranasal sinuses tends to be guarded or unfavorable.
ConclusionParanasal sinus disease can be diagnosed and treated suc-cessfully with the appropriate combination of medical and surgical therapy. However, paranasal sinus disease in horses can be complicated. The large size and complex anatomy of the sinuses can allow a pathologic process to be present for weeks or months before external signs, such as facial swelling or nasal discharge, are noticed by the owner or veterinarian. This can negatively affect the prognosis for a successful outcome and may make treatment of paranasal sinus disease frustrating for clients and veterinarians.
References1. Hillmann DJ. In: Skull. 5th ed. Philadelphia: WB Saunders; 1975.2. Hare WCD. Equine respiratory systems. In: Getty R, ed. Sisson and Grossman’s the Anatomy of the Domestic Animals. Philadelphia: WB Saunders; 1975:498-523.3. Bell BTL, Baker GJ, Abbott LC, et al. The macroscopic vascular anatomy of the equine ethmoidal area. Anat Histol Embryol 1995:39-45.4. Dyce KM, Sack WO, Wensing CJC. The head and ventral neck of the horse. In: Text-book of Veterinary Anatomy. Philadelphia: WB Saunders; 1987:470.5. Lane JG, Gibbs C, Meynink SE, et al. Radiographic examination of the facial, nasal and paranasal sinus regions of the horse: I. Indications and procedures in 235 cases. Equine Vet J 1987;19:466-473.6. Tremaine WH, Dixon PM. A long-term study of 277 cases of equine sinonasal disease. Part 1: Details of horses, historical, clinical and ancillary diagnostic findings. Equine Vet J 2001:274-282.
Key Facts
• Theparanasalsinusesofhorsesareclinicallysignificant due to associated severe and chronic disease processes and potential secondary involvement of surrounding anatomic structures.
• Thediagnosisandtreatmentofparanasalsinusdisease can be difficult.
• Mostdiseaseprocessesinvolvingtheparanasalsinuses of horses require surgical intervention for a favorable prognosis.

Vetlearn.com | February 2011 | Compendium: Continuing Education for Veterinarians® E11
7. Schumacher J, Honnas C, Smith B. Paranasal sinusitis complicated by inspissated exudate in the ventral conchal sinus. Vet Surg 1987;16:373-377.8. Ruggles AJ, Ross MW, Freeman DE. Endoscopic examination of normal paranasal sinuses in horses. Vet Surg 1991;20:418-423.9. Schumacher J, Dutton DM, Murphy DJ, et al. Paranasal sinus surgery through a frontonasal flap in sedated, standing horses. Vet Surg 2000;29:173-177.10. Coumbe K, Jones R, Kenward J. Bilateral sinus empyema in a six-year old mare. Equine Vet J 1987:559.11. Gibbs C, Lane JG. Radiographic examination of the facial, nasal and paranasal si-nus regions of the horse. II. Radiological findings. Equine Vet J 1987;19:474-482.12. Mason BJ. Empyema of the equine paranasal sinuses. JAVMA 1975;167:727-731.13. Schumacher J, Crossland LE. Removal of inspissated purulent exudate from the ventral conchal sinus of three standing horses. JAVMA 1994;205:1312-1314.14. Boulton C. Equine nasal cavity and paranasal sinus disease: a review of 85 cases. Equine Vet Sci 1985:268.15. Dixon PM, Tremaine WH, Pickles K, et al. Equine dental disease, part 4: a long-term study of 400 cases: apical infections of cheek teeth. Equine Vet J 2000:182-194.16. Gibbs C. Dental imaging. In: Baker GJ, Easley J, eds. Equine Dentistry. Philadel-phia: WB Saunders; 1999:139-169.17. Baker GJ. Some aspects of equine dental radiology. Equine Vet J 1971:46-51.18. Barakzai S, Tremaine H, Dixon P. Use of scintigraphy for diagnosis of equine para-nasal sinus disorders. Vet Surg 2006;35:94-101.19. Probst A, Henninger W, Willmann M. Communications of normal nasal and paranasal cavities in computed tomography of horses. Vet Radiol Ultrasound 2005;46:44-48.20. Henninger W, Frame EM, Willmann M, et al. CT features of alveolitis and sinusitis in horses. Vet Radiol Ultrasound 2003;44:269-276.21. Boswell JC, Schramme MC, Livesey LC, et al. Use of scintigraphy in the diagnosis of dental disease in four horses. Equine Vet Educ 1999:165-169.22. Cook WR, Littlewort MC. Progressive haematoma of the ethmoid region in the horse. Equine Vet J 1974;6:101-108.23. Sullivan M, Burrell MH, McCandlish IA. Progressive haematoma of the maxillary sinus in a horse. Vet Rec 1984;114(8):191-192.24. Colbourne CM, Rosenstein DS, Steficek BA, et al. Surgical treatment of progres-sive ethmoidal hematoma aided by computed tomography in a foal. JAVMA 1997;211: 335-338.25. Rothaug PG, Tulleners EP. Neodymium:yttrium-aluminum-garnet laser-assisted excision of progressive ethmoid hematomas in horses: 20 cases (1986-1996). JAVMA 1999;214:1037-1041.26. Stickle RL. Nasal polyp in a horse: follow-up of a previously reported case. Vet Med Small Anim Clin 1978;73:911-917.27. Schumacher J, Yarbrough T, Pascoe J, et al. Transendoscopic chemical ablation of progressive ethmoidal hematomas in standing horses. Vet Surg 1998;27:175-181.28. Frees KE, Gaughan EM, Lillich JD, et al. Severe complication after administra-tion of formalin for treatment of progressive ethmoidal hematoma in a horse. JAVMA 2001;219:939, 950-952.29. Freeman DE, Orsini PG, Ross MW, et al. A large frontonasal bone flap for sinus surgery in the horse. Vet Surg 1990;19:122-130.30. Greet TR. Outcome of treatment in 23 horses with progressive ethmoidal haema-toma. Equine Vet J 1992;24:468-471.31. Specht TE, Colahan PT, Nixon AJ, et al. Ethmoidal hematoma in nine horses. JAVMA 1990;197:613-616.32. Lane JG, Longstaffe JA, Gibbs C. Equine paranasal sinus cysts: a report of 15 cases. Equine Vet J 1987;19:537-544.33. Cannon JH, Grant BD, Sande RD. Diagnosis and surgical treatment of cystlike le-sions of the equine paranasal sinuses. JAVMA 1976;169:610-613.34. Dixon P. Equine maxillary cysts. Equine Pract 1985;7:25-33.35. Shappell K, Baker GJ. Diagnosis and surgical treatment of a frontal-maxillary sinus cyst in a horse. Compend Contin Educ Pract Vet 1987;9:1226-1229.36. Woodford NS, Lane JG. Long-term retrospective study of 52 horses with sinonasal cysts. Equine Vet J 2006;38:198-202. 37. Beard WL, Robertson JT, Leeth B. Bilateral congenital cysts in the frontal sinuses
of a horse. JAVMA 1990;196:453-454.38. Sanders-Shamis M, Robertson JT. Congenital sinus cyst in a foal. JAVMA 1987;190:1011-1012.39. Embertson RM. Upper airway conditions in older horses, broodmares, and stal-lions. Vet Clin North Am Equine Pract 1991;7:149-164.40. Levine SB. Depression fractures of the nasal and frontal bones of the horse. J Equine Med Surg 1979;3:186-190.41. Turner AS. Surgical management of depression fractures of the equine skull. Vet Surg 1979;8:29-33.42. Wilson DG, Levine S. Surgical reconstruction of the nasolacrimal system in the horse. Equine Vet Sci 1990;11:232-234.43. Campbell ML, Peyton LC. Muscle flap closure of a frontocutaneous fistula in a horse. Vet Surg 1984;13:185-188.44. Schumacher J, Auer JA, Shamis L. Repair of facial defects with periosteal flaps in two horses. Vet Surg 1985;14:235-239.45. Head KW, Dixon PM. Equine nasal and paranasal sinus tumours. Part 1: review of the literature and tumour classification. Vet J 1999;157:261-278.46. Hilbert BJ, Little CB, Klein K, et al. Tumours of the paranasal sinuses in 16 horses. Aust Vet J 1988;65:86-88.47. Freeman DE. Sinus disease. Vet Clin North Am Equine Pract 2003;19:209-243, viii.48. Tremaine WH, Clarke CJ, Dixon PM. Histopathological findings in equine sinonasal disorders. Equine Vet J 1999;31:296-303.49. Trotter GW. Paranasal sinuses. Vet Clin North Am Equine Pract 1993;9:153-169.50. Barakzai SZ, Dixon PM. Sinonasal myxoma in a four-year-old thoroughbred geld-ing. Vet Rec 2003;152:210-211.51. Chan CW, Collins EA. Case of angiosarcoma of the nasal passage of the horse: ultrastructure and differential diagnosis from progressive haematoma. Equine Vet J 1985;17:214-218.52. Hill FW, Moulton JE, Schiff PH. Exophthalmos in a horse resulting from an adeno-carcinoma of the frontal sinus. J S Afr Vet Assoc 1989;60:104-105.53. Reynolds BL, Stedham MA, Lawrence 3rd JM, et al. Adenocarcinoma of the frontal sinus with extension to the brain in a horse. JAVMA 1979;174:734-736.54. Schmotzer WB, Hultgren BD, Watrous BJ, et al. Nasomaxillary fibrosarcomas in three young horses. JAVMA 1987;191:437-439.55. Schumacher J, Smith BL, Morgan SJ. Osteoma of paranasal sinuses of a horse. JAVMA 1988;192:1449-1450.56. Scotty NC, Ford M, Williams 3rd F, et al. Exophthalmia associated with paranasal sinus osteoma in a Quarter horse mare. J Vet Diagn Invest 2004;16:155-160.57. Steinman A, Sutton GA, Lichawski D, et al. Osteoma of paranasal sinuses in a horse with inspiratory dyspnoea. Aust Vet J 2002;80:140-142.58. van Maanen C, Klein WR, Dik KJ, et al. Three cases of carcinoid in the equine na-sal cavity and maxillary sinuses: histologic and immunohistochemical features. Vet Pathol 1996;33:92-95.59. Ruggles AJ, Ross MW, Freeman DE. Endoscopic examination and treatment of paranasal sinus disease in 16 horses. Vet Surg 1993;22:508-514.60. Baker GJ. Equine nasal and paranasal tumours. Vet J 1999;157:220-221.61. Tremaine WH, Dixon PM. A long-term study of 277 cases of equine sinonasal dis-ease. Part 2: treatments and results of treatments. Equine Vet J 2001;33:283-289.62. Orsini JA, Baird DK, Ruggles AJ. Radiotherapy of a recurrent ossifying fibroma in the paranasal sinuses of a horse. JAVMA 2004;224:1454, 1483-1486.63. Walker MA, Schumacher J, Schmitz DG, et al. Cobalt 60 radiotherapy for treatment of squamous cell carcinoma of the nasal cavity and paranasal sinuses in three horses. JAVMA 1998;212:848-851.64. Davis PR, Meyer GA, Hanson RR, et al. Pseudallescheria boydii infection of the nasal cavity of a horse. JAVMA 2000;217:674, 707-709.65. Nickels FA. Diseases of the nasal cavity. Vet Clin North Am Equine Pract 1993;9: 111-121.66. Scott EA, Duncan JR, McCormack JE. Cryptococcosis involving the postorbital area and frontal sinus in a horse. JAVMA 1974;165:626-627.67. Stewart A. Antifungal therapy for horses. Compend Contin Educ Vet 2005;27: 871-876.
E12 Compendium: Continuing Education for Veterinarians® | February 2011 | Vetlearn.com
1. Which teeth are associated with the maxillary sinuses?
a. only the first through fourth cheek teeth
b. only the fifth and sixth cheek teeth c. only the fourth premolar and the first
through third molars d. only the first through fourth molars
2. The ventral conchal sinus communicates with the
a. caudal maxillary sinus. b. rostral maxillary sinus. c. frontal sinus. d. none of the above
3. Which bacterial species are often implicated in primary sinusitis?
a. Staphylococcus spp b. Streptococcus spp c. Corynebacterium spp d. Enterobacter spp
4. Which condition should be suspected if primary sinusitis fails to resolve?
a. fungal infection of the sinuses b. inspissated exudate in the ventral
conchal sinus
c. inspissated exudate in the maxillary sinus
d. none of the above (Primary sinusitis always resolves with time.)
5. The most common cause of secondary sinusitis is
a. dental disease. b. neoplasia. c. facial fracture. d. primary sinusitis.
6. The most consistent radiographic sign of secondary sinusitis due to dental disease is
a. a fluid line in the sinuses. b. an area of increased lucency around
the affected tooth apex. c. a soft tissue opacity associated with
the affected sinus. d. osteitis.
7. The most predominant clinical sign of ethmoid hematoma is
a. exercise intolerance. b. stridor. c. unilateral epistaxis. d. bilateral epistaxis.
8. Etiologic factors associated with sinus cysts include
a. dental disease. b. abnormal development of embryonic
tissue. c. trauma. d. chronic primary sinusitis.
9. The most common neoplasia of the sinuses is
a. lymphosarcoma. b. SCC. c. fibrosarcoma. d. osteomas.
10. A ____________ sp has been associated with fungal granulomas of the sinuses.
a. Conidiobolus b. Pythium c. Cryptococcus d. Aspergillus
3 CECREDITS CE TEsT This article qualifies for 3 contact hours of continuing education credit from the Auburn University College of Veterinary
Medicine. Subscribers must take individual CE tests online and get real-time scores at Vetlearn.com. Those who wish to apply this credit to fulfill state relicensure requirements should consult their respective state authorities regarding the applicability of this program.
©Copyright 2011 MediMedia Animal Health. This document is for internal purposes only. Reprinting or posting on an external website without written permission from MMAH is a violation of copyright laws.