Embed Size (px)
DESCRIPTION
Par Pharma IPR against Jazz
Citation preview

UNITED STATES PATENT AND TRADEMARK OFFICE _____________________
BEFORE THE PATENT TRIAL AND APPEAL BOARD
_____________________
PAR PHARMACEUTICAL, INC. Petitioner
v.
JAZZ PHARMACEUTICALS, INC. Patent Owner
_____________________
Case IPR: Unassigned _____________________
PETITION FOR INTER PARTES REVIEW OF U.S. PATENT NO. 7,895,059 UNDER 35 U.S.C. § 311–319 AND 37 C.F.R. § 42.1–.80, 42.100–.123
Mail Stop “PATENT BOARD” Patent Trial and Appeal Board U.S. Patent and Trademark Office P.O. Box 1450 Alexandria, VA 22313-1450

IPR Petition of U.S. Patent No. 7,895,059
-i-
TABLE OF CONTENTS
I. INTRODUCTION AND STATEMENT OF RELIEF REQUESTED (37 C.F.R. § 42.22(a)) ...................................................................................... 1
II. GROUNDS FOR STANDING (37 C.F.R. § 42.104(a)) ................................. 1
III. STATEMENT OF THE PRECISE RELIEF REQUESTED AND THE REASONS THEREFOR ................................................................................. 1
IV. OVERVIEW .................................................................................................... 2
A. Person of Ordinary Skill In The Art ....................................................... 2
B. State of the Art ....................................................................................... 3
C. The ’059 patent ....................................................................................... 7
V. CLAIM CONSTRUCTION ............................................................................ 9
A. “Exclusive Central Pharmacy” and “Exclusive Computer Database” ................................................................................................ 9
B. “Generating with the computer processor periodic reports via the exclusive computer database” ........................................................ 10
C. “Dispensed to the patient by another pharmacy” ................................. 11
VI. IDENTIFICATION OF CHALLENGE ........................................................ 11
A. EACH OF THE REFERENCES CITED IS AVAILABLE PRIOR ART. ........................................................................................ 12
1. The ACA (PAR1003 – PAR1006) qualifies as “printed publications.” ............................................................................ 13
2. Talk About Sleep, Honigfeld, Elsayed and Lilly ...................... 17
B. Ground 1: Claims 1-16 are obvious over the ACA .............................. 18
1. Comparison of the ’059 Patent Claims to the Prior Art. ........... 19
2. Claim 1 Would Have Been Obvious Over the ACA. ............... 20
3. Claim 2 ...................................................................................... 32
4. Claims 3 and 4 ........................................................................... 33
5. Claim 5 ...................................................................................... 34
6. Claim 6 ...................................................................................... 34
7. Claim 9 ...................................................................................... 34
8. Claim 12 .................................................................................... 35

IPR Petition of U.S. Patent No. 7,895,059
-ii-
9. Claim 13 .................................................................................... 35
10. Claim 14 .................................................................................... 36
11. Claims 7, 10, and 15 ................................................................. 36
12. Claims 8, 11, 16 ........................................................................ 37
C. Ground 2: Claims 1-16 would have been obvious over TAS, in view of Honigfeld and Elsayed, and further in view of Lilly. ............. 39
1. Claim 1 ...................................................................................... 40
2. Claim 2 ...................................................................................... 49
3. Claims 3 and 4 ........................................................................... 49
4. Claim 5 ...................................................................................... 50
5. Claim 6 ...................................................................................... 50
6. Claim 9 ...................................................................................... 51
7. Claim 12 .................................................................................... 51
8. Claim 13 .................................................................................... 52
9. Claim 14 .................................................................................... 52
10. Claims 7, 10, and 15 ................................................................. 52
11. Claims 8, 11, 16 ........................................................................ 53
D. Secondary considerations do not rebut the prima facie case. .............. 54
VII. IT IS MORE LIKELY THAN NOT THAT PETITIONER WILL PREVAIL WITH RESPECT TO AT LEAST ONE OF THE CHALLENGED CLAIMS ............................................................................ 58
VIII. MANDATORY NOTICES (37 C.F.R. § 42.8(a)(1)) .................................... 58
IX. CONCLUSION .............................................................................................. 60

IPR Petition of U.S. Patent No. 7,895,059
-1-
I. INTRODUCTION AND STATEMENT OF RELIEF REQUESTED (37 C.F.R. § 42.22(a))
Par Pharmaceutical, Inc. (“Par”) petitions for inter partes review (“IPR”)
and seeks cancellation of claims 1-16 of U.S. Patent No. 7,895,059 (“the ’059
patent”) (PAR1001). According to Office records, the ’059 patent is assigned to
Jazz Pharmaceuticals, Inc.
Published materials used in an FDA Advisory Committee Meeting (the
“Advisory Committee Art” or “ACA”) render obvious every limitation of the
challenged claims more than a year before the ’059 patent’s earliest effective filing
date, as set forth in Ground 1. In addition, and alternatively, other drug distribution
systems in public use long before the ’059 patent’s earliest effective filing date also
would have rendered the challenged claims obvious to a person of ordinary skill in
the art (“POSA”), as set forth in Ground 2.
For the reasons explained below, Par is at least reasonably likely to prevail
on the asserted Grounds 1 and/or 2 with respect to the challenged claims. Par
requests that this Board institute IPR and cancel each of challenged claims 1-16 of
the ’059 patent.
II. GROUNDS FOR STANDING (37 C.F.R. § 42.104(a))
Par certifies that the ’059 patent is available for IPR and Par is not barred or
estopped from requesting IPR of any of the challenged claims.
III. STATEMENT OF THE PRECISE RELIEF REQUESTED AND THE

IPR Petition of U.S. Patent No. 7,895,059
-2-
REASONS THEREFOR
The Office should institute IPR under 35 U.S.C. §§ 311-319 and 37 C.F.R.
§§ 42.1-.80 and 42.100-42.123, and cancel claims 1-16—all claims—of the ’059
patent as unpatentable under 35 U.S.C. § 103.
IV. OVERVIEW
A. Person of Ordinary Skill In The Art
A POSA is a hypothetical person who is presumed to be aware of all
pertinent art, thinks along conventional wisdom in the art, and is a person of
ordinary creativity. A POSA may work as part of a multi-disciplinary team and
draw upon not only his or her own skills, but also take advantage of certain
specialized skills of others in the team, to solve a given problem. (PAR1007, ¶21.)
For example, a POSA would hold a Bachelor’s or Doctor of Pharmacy degree and
a license as a registered pharmacist with 3-5 years of relevant work experience, or
a computer science undergraduate degree or equivalent work experience and work
experience relating to business applications, for example, including familiarity
with drug distribution procedures. Alternatively, a POSA may have a blend of
computer science and pharmacy drug distribution knowledge and/or experience.
For example, such a POSA may have computer science education qualifications
and experience relating to computerized drug distribution systems, or pharmacy
education qualifications and experience relating to computerized drug distribution
systems. (Id.) A POSA would have had knowledge of the literature concerning

IPR Petition of U.S. Patent No. 7,895,059
-3-
pharmacy practice and prescription drug distribution, such as the prior art
presented herein, that was available before the earliest effective filing date of ’059
patent, including knowledge about methods employed in the art. (Id.) Accordingly,
a POSA would have been well aware of techniques related to the mitigation of the
risk associated with the distribution of potentially hazardous, but therapeutically
beneficial prescription drugs. (Id.)
B. State of the Art
The ’059 patent generally pertains to centralizing the distribution of
hazardous or abuse-prone drugs. The ’059 patent is listed in the United States Food
and Drug Administration’s electronic publication, known as the “Orange Book”
(“OB”), in connection with the prescription drug product Xyrem®. The active
ingredient in Xyrem®—sodium oxybate, the sodium salt of gamma
hydroxybuyrate (“GHB”)—was well-known in the prior art as being susceptible to
diversion and abuse. (PAR1007, ¶47.) So, as a prerequisite to FDA approval, the
sponsor of Xyrem®, with assistance and direction from an FDA advisory
committee, agreed to employ a centralized distribution program to attempt to
reduce abusive and illicit uses of Xyrem®, now known as the Xyrem® Success
Program. By listing the ’059 patent in the FDA’s OB for Xyrem®, Jazz is asserting
that the Xyrem® Success Program is an embodiment of at least one claim of the
’059 patent.

IPR Petition of U.S. Patent No. 7,895,059
-4-
Aside from the explicit disclosure of the ’059 patent’s claimed methods in
the prior art, the mitigation of risks associated with the distribution of potentially
hazardous drugs was well-established in the art before the earliest effective filing
date of the ’059 patent. For example, in 1982, Hoffman-La Roche (“Roche”)
gained approval for Accutane® (isotretinoin), which became known to be a potent
teratogen that was responsible for birth defects. (PAR1007, ¶22.) Under pressure to
respond, Roche developed a Pregnancy Prevention Program for Accutane®. (Id.)
The program included informed consent forms to be completed by the patient and
prescriber, along with patient counseling on the teratogenic risk of Accutane®, the
need to avoid pregnancy, and the use of proper birth control methods. Finally, this
program required that women of childbearing potential must test serum negative
for a pregnancy before beginning treatment. (Id.)
Following in the footsteps of Accutane®, in 1990, Clozaril® (clozapine)
entered the United States market for use with treatment-resistant schizophrenia.
(PAR1007, ¶23.) However, Clozaril® use was associated with agranulocytosis, a
potentially fatal blood disorder resulting in white blood cell loss. (Id.) To mitigate
these risks and control the distribution of Clozaril®, the manufacturer implemented
a national registry system that limited distribution of the drug. (Id.) The
distribution system required registration in an integrated computerized database—
collecting information identifying the patient and the physician—and measuring

IPR Petition of U.S. Patent No. 7,895,059
-5-
the patient’s white blood cell count before filling a prescription. (Id.) If a patient or
physician was non-compliant with the program, the national registry took
corrective action, such as contacting and re-educating the prescribing physician
and/or discontinuing supply of the prescription to the patient. (Id.) Overall, the
Clozaril® distribution system resulted in 97% compliance over its first five years
of implementation. (Id.) While the use of a computer differentiated the Clozaril®
system from the Accutane® system, the use of computers was not novel to
prescription drug distribution, because by 1990 pharmacies had long been using
computers to aid in filling prescriptions. (Id., ¶24.)
Based on the experiences of patients and doctors with Accutane® and
Clozaril®, in 1999, the manufacturers of prescription thalidomide—a known
teratogen—developed a hybrid system, combining the computerized registry
system of Clozaril® and the pregnancy monitoring/prevention, and informed
consent requirements of Accutane®. (Id., ¶25.) This combination of computerized
registry system and preventative testing served to monitor and control the
distribution of the drug. (Id.)
Thus, by 1999, at least three systems for the restricted distribution of
effective, yet hazardous prescription drugs were known in the art and implemented
across the industry. Moreover, while risk management programs were developing
during the 1980s through 1990s, pharmacies had already been using computerized

IPR Petition of U.S. Patent No. 7,895,059
-6-
systems for the distribution of controlled substances, i.e., drugs with potential for
abuse. (Id., ¶¶26, 27.) Aiming to reduce time for dispensing, improve accuracy and
accountability, and streamline record keeping, the distribution of controlled
substances veered toward automation via the implementation of computerized
systems of distribution. (Id., ¶27) Computerized systems were helpful in generating
reports tracking patients who were receiving excessive supplies of controlled
substances. (Id.) Distribution of controlled substances could be tied to information
identifying the patient, the prescribing doctor, the quantity of the drug dispensed,
and the hospital inventory of a drug. (Id.) And, the systems could be queried to
provide data, such as prescriptions by doctor and patient. (Id.) These systems
allowed for detecting patterns of abuse. (Id.)
Given the proclivity for diversion and abuse of GHB, the FDA held advisory
committee meetings as a prerequisite to granting approval to the Xyrem® New
Drug Application (“NDA”). A collection of materials that were used in that
meeting (the “Advisory Committee Art” or “ACA”)—all of which published more
than one year prior to the earliest effective filing date of the ’059 patent—discloses
every limitation of the challenged claims.
Consequently, prior to the earliest effective filing date of the ’059 patent,
prior art existed that would have led a POSA to develop the centralized distribution
systems claimed in the ’059 patent to minimize the risks associated with the

IPR Petition of U.S. Patent No. 7,895,059
-7-
distribution of hazardous prescription drugs. (Id., ¶28.)
C. The ’059 patent
Against this backdrop, Jazz obtained the ’059 patent. The ’059 patent relates
to “[a] drug distribution system and method [that] utilizes a central pharmacy and
database to track all prescriptions for a sensitive drug.” (PAR1001, Abstract.)
According to the ’059 patent, prescription patterns by physicians and patients are
monitored for abuse using an exclusive central database. Further, physician
eligibility to prescribe the drug is verified via a database, including determining
whether any corrective or approved disciplinary actions have been brought against
the physician. (Id., 1:48-56.) Prior to shipping the prescription drug, the central
pharmacy confirms whether the patient has been educated about the prescription,
and only ships the prescription drug when no abuse is found related to the patient
and prescribing doctor. (Id., 1:59-63 and 8:62-65.) Reports are then generated to
evaluate potential diversion patterns. (Id., 2:19-21.)
The ’059 patent claims are directed to a method of distributing a prescription
drug from an exclusive central pharmacy that comprises: (1) receiving in a
computer processor all prescription requests for any and all patients only at the
exclusive central pharmacy, entering information from the prescription requests
into an exclusive computer database associated with the exclusive central
pharmacy and processing the prescription requests only by the exclusive central

IPR Petition of U.S. Patent No. 7,895,059
-8-
pharmacy using only the exclusive computer database; (2) checking for patterns of
abuse using the exclusive computer database; (3) only providing the prescription
drug to the patient if no abuse is found; and (4) generating periodic reports to
evaluate potential diversion patterns.
During prosecution of the ’059 patent’s parent application, the independent
claims were amended to add the following limitations to overcome prior art
rejections: (1) “all prescriptions for the sensitive drug are processed only by the
exclusive central pharmacy using only the exclusive computer database”; and (2)
“mailing the sensitive drug to the patient only if no potential abuse is found by the
patient to whom the sensitive drug is prescribed and the doctor prescribing the
sensitive drug.”1 (PAR1016, 442 (Amdt. & Reply filed Nov. 2, 2009; see also
PAR1016, 241-248 (Amdt. & Reply filed Aug. 8, 2006) and 303-334 (Appeal
Brief filed July 18, 2007).) Applicants argued that these limitations were not taught
by the cited prior art. (PAR1016, 449 (Amdt. & Reply, filed Nov. 2, 2009).) All
other limitations of the claims were found to have been taught by the cited prior
art. (Id. at 258-262 (Final Rejection, Oct. 18, 2006) and at 420-433 (Decision on
Appeal, Aug. 31, 2009).)
Subsequently, in the Notice of Allowance for the ’059 patent’s parent
application, the Examiner pointed to the above-noted limitations when allowing the
1 Emphasis added throughout unless otherwise noted.

IPR Petition of U.S. Patent No. 7,895,059
-9-
claims, stating: “the closest prior art of record does not teach or fairly suggest that
all prescriptions for GHB are processed only by the exclusive central pharmacy
using only the exclusive computer database. The exclusive computer database is
checked for potential GHB abuse and GHB is provided/mailed only if no potential
abuse is found by the patient to whom GHB is prescribed and the
doctor/authorized prescriber of the GHB.” (Id. at 475-476 (Notice of Allowance)
(emphasis in original).) The’059 patent claims similarly rely on these limitations
for purposes of patentability. However, as demonstrated in this petition, all of these
alleged “novel” limitations were, in fact, not novel. Use of an “exclusive central
pharmacy” and “exclusive computer database” were well-known in the art. (See
§§ VI.B–C.) And the same art also discloses checking the exclusive computer
database for patterns of abuse by both the doctors and patients and only providing
the prescription drug to the patient if no abuse is found. (Id.)
V. CLAIM CONSTRUCTION
Unless otherwise construed herein, the terms of claims 1-16 are to be given
their broadest reasonable interpretation, as understood by one of ordinary skill in
the art in view of the ’059 patent’s specification. See 37 C.F.R. § 42.100(b).
A. “Exclusive Central Pharmacy” and “Exclusive Computer Database”
Claims 1–16 all recite (either explicitly or through incorporation from the
independent claims) the terms “exclusive central pharmacy” and “exclusive

IPR Petition of U.S. Patent No. 7,895,059
-10-
computer database.” During prosecution of the ’730 patent, of which the ’059
patent is a continuation, the applicants defined the term “exclusive” as “single or
sole.” (PAR1016, 402 (Reply Brief, filed Dec. 3, 2007).) Therefore, the terms
“exclusive central pharmacy” and “exclusive computer database” should be
construed to mean a “single or sole pharmacy” and a “single or sole database,”
respectively. (PAR1007, ¶37.)
B. “Generating with the computer processor periodic reports via the exclusive computer database”
Claims 1–13 all recite (either explicitly or through incorporation from the
independent claims) the limitation “generating with the computer processor
periodic reports via the exclusive computer database.” (PAR1001, 9:1-3.) The ’059
patent discloses that “[s]everal queries and reports are run against the database
to provide information which might reveal potential abuse of the sensitive drug,
such as early refills.” (Id., 2:19-21).) Moreover, the ’059 patent discloses that
reports are obtained by running queries against the central database. (Id., 8:22-29.)
Further, the ’059 patent describes different types of queries that are run to obtain
information such as prescriptions written by physician, prescriptions by patient
name, prescriptions by frequency, and prescriptions by dose. (Id., 7:53-67.)
Accordingly, “querying the central database” at least meets the limitation of
“generating … periodic reports,” as would be understood by a POSA. (PAR1007,
¶38.) Hence, under the broadest reasonable construction of the term, “generating

IPR Petition of U.S. Patent No. 7,895,059
-11-
… periodic reports,” should be construed to mean “querying the computer database
to obtain information, such as, prescriptions by physician, prescriptions by patient
name, prescriptions by frequency, and prescriptions by dose.” (Id,)
C. “Dispensed to the patient by another pharmacy”
Claims 7, 10, and 15 recite the limitation “the central pharmacy authorizing
the prescription drug to be dispensed to the patient by another pharmacy.” The
’059 patent does not provide a definition for “dispensed.” Further, the only support
in the ’059 patent for another pharmacy (i.e., not the exclusive central pharmacy)
having any involvement in distributing the drug is where the ’059 patent states,
“[i]n one embodiment, the drug may be shipped to another pharmacy for patient
pickup.” (PAR1001, 2:4-5.) Hence, under the broadest reasonable interpretation,
“dispensed to the patient by another pharmacy” would be understood by a POSA
and should be construed to mean “making the prescription drug that was dispensed
by the central pharmacy available for pick-up by the patient at another pharmacy.”
(PAR1007, ¶45.)
VI. IDENTIFICATION OF CHALLENGE
IPR of the challenged claims of the ’059 patent is requested on the grounds
for unpatentability listed below. Copies of the references are filed herewith. 37
C.F.R. § 42.6(c). The proposed grounds in this Petition are supported by the
Declaration of Dr. Robert Valuck, Ph.D., R.Ph. (PAR1007).

IPR Petition of U.S. Patent No. 7,895,059
-12-
Ground 35 USC Claims Index of References
1 § 103(a) 1-16 Advisory Committee Art (PAR1003-1006)
2 § 103(a) 1-16 Talk About Sleep in view of Honigfeld further in view of Elsayed and further in view of Lilly.
For each asserted ground, Par demonstrates below where each limitation
either exists in the prior art or is rendered obvious, by evaluating the scope and
contents of the prior art, any differences between the art and the challenged claims,
the knowledge of person of ordinary skill in the art, and any available objective
indicia of nonobviousness in accordance with Graham v. John Deere Co., 383 U.S.
1 (1966) and KSR Int’l Co. v. Teleflex, Inc., 550 U.S. 398 (2007).
A. EACH OF THE REFERENCES CITED IS AVAILABLE PRIOR ART.
Each of the references cited in this petition is available as prior art under the
basis for qualification provided for by 35 U.S.C. § 311(b). The ’059 patent was
filed on February 11, 2010 and claims the benefit of the ’730 patent, filed on
December 17, 2002. (See PAR1001.) Patent Owner has not established any earlier
date of invention. Accordingly, December 17, 2002 is its earliest effective filing
date. Each cited prior art reference qualifies independently as (1) having published
before December 17, 2002 or (2) having been publicly disclosed more than a year
prior to the application for patent in the United States.

IPR Petition of U.S. Patent No. 7,895,059
-13-
1. The ACA (PAR1003 – PAR1006) qualifies as “printed publications.”
“[T]he determination of whether a given reference qualifies as a prior art
‘printed publication’ involves a case-by-case inquiry into the facts and
circumstances surrounding the reference’s disclosure to members of the public.”
CBM2013-00047, Paper 11, *16 (Feb. 18, 2014) (citing In re Klopfenstein, 380
F.3d 1345, 1350 (Fed. Cir. 2004)). And “[a] reference is publicly accessible upon a
satisfactory showing that such document has been disseminated or otherwise made
available to the extent that persons interested and ordinarily skilled in the subject
matter or art exercising reasonable diligence, can locate it.” Id. (quoting Kyocera
Wireless Corp. v. Int’l Trade Comm’n, 545 F.3d 1340, 1350 (Fed. Cir. 2008)).
Electronic publications can qualify as “printed publications” as long they
have been disseminated or otherwise made available to a POSA exercising
reasonable diligence. IPR2013-00084, Paper 14, *20-21 (May 17, 2013). And
while indexing is “often relevant to public accessibility, evidence of indexing is not
an absolute prerequisite to establishing online references [] as printed publications
within the prior art.” Id., at *21 (quoting Voter Verified, Inc. v. Premier Election
Solutions, Inc., 698 F.3d 1374, 1380 (Fed. Cir. 2012)). Moreover, institution
cannot be denied because an electronic reference is not accompanied by a
declaration from an author or with other evidence that someone accessed and
received the reference prior to the critical date. IPR2014-00059, Paper 9, *34 (Apr.

IPR Petition of U.S. Patent No. 7,895,059
-14-
15, 2014). Par need only provide sufficient evidence to demonstrate that the
reference was disseminated publicly or otherwise available. Id. at *34-35 (citing In
re Wyer, 655 F.2d 221, 226 (C.C.P.A. 1981) (finding that no evidence concerning
actual viewing or dissemination of a reference was required when a reference is
deemed to have been “sufficiently accessible to the public and to persons skilled in
the pertinent art”)).
Examination of the ACA materials (PAR1003-PAR1006) demonstrates that
it is a collection of publicly available, printed publications. Orphan Medical
submitted for publication the Xyrem Video and Transcript, the Briefing Booklet,
and the Preclinical Safety Review as briefing materials to the FDA before the
Advisory Committee met on June 6, 2001. Indeed, according to the Federal
Register notice announcing this meeting:
Background material from the sponsor and FDA will be posted 24
hours before the meeting at the Peripheral and Central Nervous
System Drugs Advisory Committee docket site at
http://www.fda.gov/ohrms/dockets/ac/acmenu.htm (Click on the year
2001 and scroll down to the Peripheral and Central Nervous Systems
Drugs meetings.) This is the same website where you can find the
minutes, transcript, and slides from the meeting. This material is
generally posted about 3 weeks after the meeting.
(PAR1015 (emphasis added).) Such “competent evidence of the [FDA’s] general []
practice may be relied upon to establish an approximate time” the ACA would

IPR Petition of U.S. Patent No. 7,895,059
-15-
have become available to a POSA exercising reasonable diligence. IPR2014-
00059, Paper 9, *34 (Apr. 15, 2014) (citing In re Hall, 781 F.2d 897, 899 (Fed.
Cir. 1988)).2 Therefore, based on the stated timelines, the Xyrem Video and
Transcript (PAR1006), the Briefing Booklet (PAR1005), and the Preclinical Safety
Review (PAR1004) were approximately available on the FDA’s website as of June
5, 2001, while the Advisory Committee Transcript and Slides (PAR1003) were
available as of June 27, 2001. Both dates are more than one year prior to December
17, 2002. Additionally, the FDA website that hosts these documents demonstrates
that they were all available by July 13, 2001, at the latest, also qualifying them as
102(b) prior art. (PAR1017 (relevant bullet point highlighted).) And because the
ACA was listed on an FDA website, the address of which was provided in the
Federal Register, the ACA was indexed and accessible to persons of ordinary skill.
The Preclinical Safety Review (PAR1004) contains redactions of the name
of the proposed specialty pharmacy for distribution of Xyrem®—further evidence
that these materials would be, and were intended to be, available to the public,
while small portions, immaterial here, containing confidential information were
2 The Federal Advisory Committee Act also required that “the records,
reports, transcripts, minutes … or other documents which were made available to
or prepared for or by each advisory committee shall be available for public
inspection.” 5 U.S.C. App 2 §10(b) (2001).

IPR Petition of U.S. Patent No. 7,895,059
-16-
hidden. And the Briefing Booklet (PAR1005) states on its cover that it is
“AVAILABLE FOR PUBLIC DISCLOSURE WITHOUT REDACTION”—
confirming that a POSA would have easily been able to obtain it. Cf. IPR2013-
00458, Paper 12, *27 (Jan. 16, 2014) (finding that statements of confidentiality on
a document suggest it was not publicly available).
Other evidence corroborating the public availability of the ACA comes from
the Internet Archive: Wayback Machine (located at
https://archive.org/web/web.php).3 The Wayback Machine demonstrates that, at the
latest, a link to the “Briefing Information” (i.e., the Xyrem Video and Transcript
(PAR1006), the Briefing Booklet (PAR1005), and the Preclinical Safety Review
(PAR1004)) was available online on June 17, 2001. (PAR1018, pg. 5, 6/6
Meeting.) Following this link demonstrates that this art was all available on July 1,
2001, at the latest. (PAR1019.) And the Advisory Committee Transcript and Slides
(PAR1003) were available by October 4, 2001, at the latest—more than one year
prior to December 17, 2002. (PAR1020, pg. 8, 6/6 Meeting.)
Additionally, a POSA “exercising reasonable diligence” would have been
able to locate the ACA. (PAR1007, ¶48; PAR1015.) Notice of the Advisory
3 The Board has not precluded the use of Documents from the Wayback
Machine when making institution decisions. See, e.g., IPR2013-00142, Paper 11,
*9-10 (Aug. 7, 2013).

IPR Petition of U.S. Patent No. 7,895,059
-17-
Committee Meeting was posted in the Federal Register, which indicated that “[a]
main focus of the deliberations will be on risk management issues.” (PAR1007,
¶48; PAR1015.) Moreover, the Federal Register also points a POSA to where the
ACA would be located before and after the meeting. (PAR1007, ¶48; PAR1015.)
A POSA would have known to look in the Federal Register and on the FDA’s
website to obtain information related to existing and proposed risk management
programs. (PAR1007, ¶48.)
In sum, the ACA was a collection of publicly available, printed publications
because it would have been available to and readily located by a POSA exercising
reasonable diligence. Moreover, it was available more than one year prior to the
priority benefit date of the ’059 patent. (PAR1028.)
2. Talk About Sleep, Honigfeld, Elsayed and Lilly
Talk About Sleep (hereinafter “TAS”) is entitled to the §102(b) prior art date
of its publication: February 12, 2001. Honigfeld is entitled to the 102(b) prior art
date of its publication: March 31, 1998. (PAR1034, 3), Elsayed is entitled to the
§102(b) prior art date of its issue: April 4, 2000. (PAR1035, front page.) Lilly is
entitled to a § 102(e) prior art date of November 14, 2001, the filing date of its
earliest provisional application. See, e.g., In re Giacomini, 612 F.3d 1380 (Fed.
Cir. 2010) (PAR1036, front page).

IPR Petition of U.S. Patent No. 7,895,059
-18-
B. Ground 1: Claims 1-16 are obvious over the ACA
As supported by the declaration of Dr. Valuck, claims 1-16 of the ’059
patent would have been obvious over the ACA—Advisory Committee Transcript
and Slides (PAR1003), Preclinical Safety Review (PAR1004), Briefing Booklet
(PAR1005), and Xyrem Video and Transcript (PAR1006). The ACA qualifies as
prior art to the claims of the ’059 patent. (See § VI.A.1) Each publication was
either submitted to the FDA prior to the meeting or is a record of what transpired at
the meeting. And, as announced in the Federal Register, each publication was
readily accessible to the public from a central location on the FDA’s website more
than one year before the priority date for the ’059 patent. (PAR1019.)
A POSA would have had more than ample reason to combine these ACA
materials. The Preclinical Safety Review (PAR1004), Briefing Booklet
(PAR1005), and Xyrem Video and Transcript (PAR1006) were all distributed
together for a single meeting before the FDA seeking approval for prescription
Xyrem®, and the Advisory Committee Transcript and Slides (PAR1003) were a
public transcript of and presentation given at the meeting itself. Moreover, a POSA
would also have had a reasonable expectation of success when combining each of
these materials to arrive at claims 1-16 because they clearly relate to the same
restricted distribution program, which the meeting was convened to discuss.
(PAR1007, ¶52.) Further, the Xyrem Video and Transcript (PAR1006) is

IPR Petition of U.S. Patent No. 7,895,059
-19-
incorporated by reference into the Advisory Committee Transcript and Slides
(PAR1003), and into the Briefing Booklet (PAR1005). (See PAR1003; PAR1005.)
Not only that, but each of the references are all linked from a single page. The
links specify with particularity each of the documents. So, even if they are
considered to be separate references, the base menu page effectively incorporates
by reference each of the different documents, making them obvious to combine.
1. Comparison of the ’059 Patent Claims to the Prior Art.
Independent claim 1 of the ’059 patent recites the following:
A computerized method of distributing a prescription drug under
exclusive control of an exclusive central pharmacy, the method
comprising:
[1.1] receiving in a computer processor all prescription requests,
for any and all patients being prescribed the prescription drug, only at
the exclusive central pharmacy from any and all medical doctors
allowed to prescribe the prescription drug, the prescription requests
containing information identifying patients, the prescription drug, and
various credentials of the any and all medical doctors;
[1.2] requiring entering of the information into an exclusive
computer database associated with the exclusive central pharmacy for
analysis of potential abuse situations, such that all prescriptions for
the prescription drug are processed only by the exclusive central
pharmacy using only the exclusive computer database;
[1.3] checking with the computer processor the credentials of the
any and all doctors to determine the eligibility of the doctors to

IPR Petition of U.S. Patent No. 7,895,059
-20-
prescribe the prescription drug;
[1.4] confirming with a patient that educational material has been
received and/or read prior to shipping the prescription drug;
[1.5] checking the exclusive computer database for potential abuse
of the prescription drug;
[1.6] mailing or sending by courier the prescription drug to the
patient only if no potential abuse is found by the patient to whom the
prescription drug is prescribed and the doctor prescribing the
prescription drug;
[1.7] confirming receipt by the patient of the prescription drug; and
[1.8] generating with the computer processor periodic reports via
the exclusive computer database to evaluate potential diversion
patterns.
(PAR1001, 8:37-9:3 (numbering added for ease of reference to claim limitations).)
The remaining independent claims of the ’059 patent (claims 6, 9, 12, 13,
and 14) recite substantially similar subject matter as claim 1 with slight
differences, i.e, excluding certain limitations, rewording of certain claim terms,
and/or the claims being directed specifically to the distribution of GHB.
2. Claim 1 Would Have Been Obvious Over the ACA.
As explained by Dr. Valuck—an expert in drug safety, drug abuse
prevention, and prescription drug distribution with two decades of experience in
the area—in his accompanying declaration, each limitation of claim 1 is found in
the ACA. (See PAR1007, ¶¶53-85.) For ease of reference, claim 1 is also recited

IPR Petition of U.S. Patent No. 7,895,059
-21-
in its entirety at Section VI.B.1 above.
The ’059 patent provides several flow diagrams, together describing each of
claim 1’s limitations. The representative figure below has been produced based on
those flow diagrams and maps each limitation of claim 1 to a representative flow
diagram step from the figures of the ’059 patent for ease of understanding each
limitation.
Preamble: The ACA explicitly teaches a method of distributing a
prescription drug under exclusive control of an exclusive central pharmacy, as
recited by the preamble of claim 1. For example, ACA discloses distributing the
prescription drugs Xyrem® through a closed distribution system. (PAR1003, Tr.,
177:24-178:11; PAR1007, ¶54.) The ACA’s closed distribution system includes

IPR Petition of U.S. Patent No. 7,895,059
-22-
manufacturing Xyrem® at a single manufacturing facility and providing Xyrem®
to a single national pharmacy that will be its exclusive distributor. (See PAR1003,
Tr., 177:24-178:11 and 183:12-16; PAR1004, pg. 108; PAR1005, pgs. 302, 306,
309, and 311; PAR1006, Tr., pg. 4 n.13; PAR1007, ¶54.)
As discussed in § V.A., the patentee argued during prosecution that
“exclusive” meant “single or sole.” As such, a POSA would have understood that
the “single national specialty pharmacy” described by the ACA with respect to
Xyrem® is synonymous with the claimed “exclusive central pharmacy” in the ’059
patent. (PAR1007, ¶54.) ACA discloses benefitting from using a single national
specialty pharmacy because the prescription drugs are distributed from a central
location and all controls and records are in one place, i.e., at the single national
specialty pharmacy. (See PAR1003, Tr., 177:24-178:11; PAR1005, pg. 299 and
306; PAR1007, ¶¶54, 55.) Accordingly, a POSA would have immediately
appreciated that the ACA’s distribution of Xyrem® is under the exclusive control
of the single or exclusive national specialty pharmacy. (PAR1007, ¶¶54-56.)
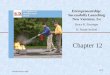
ACA: Figure shows pharmacist at single specialty pharmacy utilizing a computer.

IPR Petition of U.S. Patent No. 7,895,059
-23-
Moreover, ACA teaches and illustrates that the distribution of the
prescription drugs under the exclusive control of the single or exclusive national
specialty pharmacy is computerized, as claimed. (See PAR1003, Slides, pg. 146,
reproduced above w/annotation; PAR1006, Tr., pg. 10 n.42; V5 00:09-00:27,4 V7
00:00-00:16; PAR1007, ¶55.) To the extent the Board concludes that the
illustration is not an explicit teaching—and Par posits that it is—ACA at least
nevertheless implicitly teaches how its closed distribution system is computerized.
For example, ACA teaches receiving data from prescription requests (which can be
thousands of requests) at the specialty pharmacy and entering the data into a
registry. (See PAR1003, Tr., 16:4-7, 24:21-25, 259:4; PAR1005, cover letter, pg.
1; PAR1007, ¶55, emphasis added).)
The collected data provide “centrally located, real-time data [that] will be
invaluable to identification of suspicious [behavior].” (PAR1005, pg. 304 and 311;
PAR1007, ¶55.) From this disclosure, a POSA would have immediately envisaged
that the single national pharmacy utilized a computer so that prescription
information could be collected and physician prescribing patterns and patient
activity could be monitored in real-time. (PAR1007, ¶55.) Accordingly, a POSA
would have understood that ACA teaches a computerized method of distributing a
4 Citations to the Xyrem Video (PAR1006) will be provided as VX YY:YY,
where VX = PAR1006, Video, part X.

IPR Petition of U.S. Patent No. 7,895,059
-24-
prescription drug from a central location—because the need to enter, access, and
store large amounts of information would be accelerated and, thus, facilitated by
using a computer. (PAR1007, ¶56.)
Step 1.1: Step 1.1 recites, in part, “receiving in a computer processor all
prescription requests....” ACA discloses that the single national pharmacy receives
“a number of unique prescribing forms for Xyrem® which will be necessary in
order for the prescription to be filled.” (See PAR1003,Tr. 180:6-16; Slides, pg.
151; PAR1005, pg. 310; PAR1006, Tr., pg. 5 n.20; V7 00:00-00:16; PAR1007,
¶58.) A POSA would have immediately recognized that the unique prescribing
forms are synonymous with the claimed prescription requests. (PAR1007, ¶58.)
Further, a POSA would have understood that the single national pharmacy receives
the prescribing forms for all patients being prescribed the prescription drug. (Id.)
Moreover, ACA explicitly teaches that the unique prescribing forms are
received from any and all medical doctors allowed to prescribe the prescription
drug. For example, ACA discloses that once the single national pharmacy receives
the prescription form, the central pharmacy checks the eligibility of the prescribing
doctor to prescribe Xyrem® and also checks the patient’s eligibility to receive the
prescription. (See PAR1003, Tr., 181:1-22; Slides, pg.152-153; PAR1004, pg. 109;
PAR1005, pgs. 310; PAR1006, Tr., pg. 6 n.21; PAR1007, ¶59.) As explained by
ACA, these eligibility checks ensure (1) that the physician has a valid medical

IPR Petition of U.S. Patent No. 7,895,059
-25-
license, prescribing privileges, and no actions pending against him; and (2) the
veracity of the patient’s identity and receipt of a prescription for GHB. (See
PAR1003, Tr., 181:1-22; Slides pg. 152-153; PAR1004, pg. 109; PAR1005, pg.
306; PAR1006, Tr., pg. 6 n.21 and n.24; PAR1007, ¶59.)
A POSA reviewing the ACA would have known that in order to perform the
eligibility checks, the special prescription forms would be received from any and
all doctors and would include “information identifying patients, the prescription
drug, and various credentials of the any and all medical doctors,” as recited in
claim 1. (PAR1007, ¶¶59, 60.) It is with this information in hand that the single
national pharmacy described by ACA would (1) cross-reference the external DEA
National Technical Information Services database and state medical board records
to identify doctors allowed to prescribe the prescription drug; (2) check the
veracity of the patient and his prescription; and (3) determine what drug to
dispense and when to do so. (Id., ¶60.)
Additionally, as discussed above, ACA teaches that the distribution process
of the single national pharmacy could be performed using a computer. (See
PAR1003, Slides, pg. 146; PAR1006, Tr., pg. 10 n.42; V5 00:09-00:27, V7 00:00-
00:16; PAR1007, ¶61.) For the same reason, ACA teaches that the prescription
requests are received in a computer processor, if not explicitly, at least implicitly.
(PAR1007, ¶¶55, 61.) For example, ACA recognizes the necessity of collecting

IPR Petition of U.S. Patent No. 7,895,059
-26-
data for a significant number of patients, thus implying utilizing a conventional
computer to accelerate processing of prescriptions. (PAR1003, Tr., 24:21-25;
PAR1005, cover letter, pg. 1; PAR1007, ¶61.) Moreover, ACA discloses
registering “every patient and prescribing physician” in “a secure database”
(PAR1004, pg. 110; PAR1007, ¶61.) and ACA shows that the pharmacy staff
receives a prescription request and enters the prescription request into a computer.
(See PAR1006, V7 00:00-00:16; PAR1007, ¶61.) Therefore, ACA discloses that
“all prescriptions from any and all doctors for any and all patients” are received in
the computer processor.
Furthermore, a POSA would have immediately envisaged using a computer
to receive and organize prescription requests, as pharmacies were doing this prior
to the effective filing date of the ’059 patent, and computers are shown in ACA.
(PAR1007, ¶¶24, 61.) And POSA would have known that a secure database, which
could house information for a large number of patients, as described by ACA,
would normally be accessed using a computer. (Id., ¶61) Here, a POSA would
have at once envisaged that ACA teaches that prescription requests are entered into
the secure database that is accessible via a computer. A POSA likewise would have
at once envisaged that achieving the disclosed benefits of using an exclusive
central pharmacy would be more realized through the use of the disclosed
computer, allowing for quicker entry, access, compiling and analysis of data.

IPR Petition of U.S. Patent No. 7,895,059
-27-
(PAR1007, ¶¶61-62.)
Step 1.2: ACA explicitly describes an exclusive computer database
associated with the exclusive central pharmacy. (Id., ¶69.) As discussed above,
ACA discloses a centralized location for all prescription controls and records. (See
PAR1003, Tr., 177:24-178:11; Slides, pg. 146-147; PAR1005, pg. 306; PAR1006,
Tr., pg. 6 n.24; PAR1007, ¶64.) And ACA further explains that such controls and
records are kept in a “central data repository.” (Id.) A POSA would have
understood this “central data repository” to be synonymous with the claimed
“exclusive computer database” in the ’059 patent, because all the controls and
records are kept at a single location (i.e., exclusive), namely the central data
repository. (PAR1007, ¶64.) Prior to filling a prescription, the central data
repository allows for the identification of potential abuse situations, such as any
duplicate prescriptions, any attempts of over-prescribing, or any attempts at over-
use by patients. (See PAR1003, Tr., 184:24-185:6; Slides, pg. 158; PAR1005, pgs.
311; PAR1006, Tr., pg. 7 n.25 and pg. 8 n.29; PAR1007, ¶65.)
ACA also discloses that information from the prescription request is entered
into the exclusive computer database. As discussed earlier, ACA discloses
registering every patient and prescribing physician in the database. (See PAR1003,
Tr., 16:4-7, 259:4; PAR1004, pg. 110; PAR1007, ¶66.) The information that is
registered in the database includes the physician’s name, address, telephone and

IPR Petition of U.S. Patent No. 7,895,059
-28-
facsimile numbers, DEA and state license numbers and prescribing frequency.
(PAR1004, p. 110; PAR1005, p. 306; PAR1006, Tr., pg. 6; PAR1007, ¶66.)
Utilizing the database allows for ready access to this information, organized
according to prescriptions by physician, patient, frequency, and/or dose. (See
PAR1004, pp. 110, 114; PAR1005, pg. 304; PAR1006, Tr., pg. 4 n.13-14 and pg. 7
n.25; PAR1007, ¶66.) Further, ACA discloses that upon receiving the unique
prescription request forms at the single national pharmacy, the pharmacy collects
data that aids in determining proper timing for prescription refills. (See PAR1003,
Tr. 259:4-11; Slides, pg. 158; PAR1004, pg. 110; PAR1006, Tr., pg. 4 n.13-14 and
pg. 7 n.25; PAR1007, ¶¶64, 66.) A POSA, therefore, would have at once envisaged
that to achieve the benefits described by ACA (e.g., analysis of potential abuse
situations), the information from the prescription forms would have been collected
and entered into the disclosed central data repository (i.e., exclusive computer
database). (PAR1007, ¶67.)
Step 1.3: ACA explicitly discloses performing a number of checks to
determine if the prescribing physician is eligible to administer prescriptions upon
receiving a prescription request at the single national pharmacy. These checks
include checking the relevant external DEA database and the appropriate state
medical board specific to the prescriber in question. (See PAR1003, Tr., 181:1-22;
Slides pg. 152-153; PAR1004, pg. 109; PAR1005, pg. 306 and 310; PAR1006, Tr.,

IPR Petition of U.S. Patent No. 7,895,059
-29-
pg. 6 n.21 and n.24; PAR1007, ¶69.) A POSA also would have immediately
envisaged performing such credential checking using a computer, because doing so
would make it easier to check sources such as the DEA’s National Technical
Information Services. (PAR1007, ¶69.)
Step 1.4: ACA explains that “each patient, when they get their first
prescription of Xyrem® will receive a multi-faceted educational program called
the Xyrem Patient Success Program[.]” (PAR1003, Transcript, 182:3-8; PAR1007,
¶71.) Notably, by listing the ’059 patent in the Orange Book for Xyrem®, Jazz is
asserting that the Xyrem® Success Program is a commercial embodiment of at
least one of the ’059 patent claims. ACA also describes modifying the distribution
system to confirm with a patient that educational material has been received and/or
read prior to shipping the prescription drug. (See PAR1003, Tr., 371:10-12 and
374:7-20; PAR1004, pg. 115; PAR1007, ¶72.) A POSA would have understood
this teaching to explicitly disclose confirming that the patient received and/or read
educational materials before shipping the prescription drug. (PAR1007, ¶72.)
Step 1.5: ACA explicitly describes checking for potential abuse. As
explained above, ACA’s central data repository “allows for identification of a
number of unusual types of behavior, including any duplicate prescriptions, any
attempts of over-prescribing, or any attempts at over-use by patients.” (PAR1003,
Transcript, 184:24-185:4; PAR1007, ¶74.) Moreover, ACA discloses flagging for

IPR Petition of U.S. Patent No. 7,895,059
-30-
monitoring and documenting “repeat instances of lost, stolen, destroyed, or spilled
prescriptions/supplies.” (PAR1004, pg. 110; PAR1007, ¶74.)
Steps 1.6-1.7: ACA explicitly discloses shipping the prescription drug to a
patient via a courier service and/or mail-order based system. (Claim 1, step 1.6;
See PAR1003, Tr., 178:5-6 and 182:17-23; Slides, pg. 146; PAR1004, pg. 109 and
115; PAR1005, pg. 302, 304, and 311; PAR1006, V10 00:40-V11 00:31;
PAR1007, ¶76.) Further, ACA explicitly discloses that the prescription drug is
only mailed or sent by courier if no potential abuse is found by the target patient
and prescribing physician based on verifying the stored information. (PAR1003,
Tr., 184:24-185:7; Slides, pgs. 158-159; PAR1005, pgs. 304, 305, and 311;
PAR1006, Tr., pg. 8 n.29 and pg. 9 n.38; PAR1007, ¶¶ 74, 77.) And the stated
benefit is that this “information is available prior to filling the prescription so
appropriate pharmacist intervention can occur.” (PAR1003, Tr., 184:24-185:7;
Slides, pgs. 158-159; PAR1006, Tr., pg. 8 n.29 and pg. 9 n.38; PAR1007, ¶77
(emphasis added).) Moreover, ACA discloses making the prescription drug
inaccessible to those who might abuse it, thus maintaining responsible distribution.
(See PAR1003, Tr., 185:9-14; Slides pg. 142; PAR1005, pgs. 298, 305, 308, and
311; PAR1007, ¶77.) Hence, a POSA would have understood the ACA to disclose
mailing or sending by courier the drug only where there is no potential for abuse.
(PAR1007, ¶77.)

IPR Petition of U.S. Patent No. 7,895,059
-31-
Furthermore, ACA explicitly describes limitation 1.7 (confirming receipt).
ACA explains that “after the Rapid Trac System shows that the package has been
received by the patient, the specialty pharmacist will call the patient within 24
hours not only to confirm receipt of that package but also to reiterate certain
important points with the patient.” (PAR1003, Tr., 184:10-15; PAR1007, ¶79.)
Step 1.8: As discussed above in § V.B, a POSA would have understood that
the limitation of “generating…periodic reports” entails querying the computer
database to obtain prescription information organized by, for example, physician,
patient name, frequency, and/or dosage amount. In this context, ACA discloses this
limitation at least implicitly, if not explicitly. For example, ACA discloses using
the central data repository to identify patterns of abuse and diversion. (See
PAR1003, Tr., 184:24-185:7; Slides, pg. 158; PAR1005, pg. 306, 307, and 311;
PAR1007, ¶82.) And ACA describes preventing diversion and illicit use, as well as
providing assistance to “law enforcement for investigation and prosecution
efforts,” as a goal of its distribution system (PAR1003, Tr., 15:6-8; PAR1004, pg.
110; PAR1005, pp. 298, 301 and 306-308; PAR1007, ¶82.) Moreover, ACA
discloses generating data by “recording prescribers, patients, and dosing that could
provide information for any possible investigations and prosecutions for state and
federal authorities” using a computer (PAR1006, Tr., pg. 4 n.13-14; V5 00:10-
00:27; PAR1007, ¶83.) From the prescription information entered into the

IPR Petition of U.S. Patent No. 7,895,059
-32-
database, the database can be queried to provide information such as
“[p]rescriptions by physician specialty … by patient name … by volume
(frequency) … [and] by dose.” (PAR1004, pg. 110; PAR1007, ¶83.) ACA also
discloses that the “Xyrem risk management system ensures that the centralized
pharmacy will identify patients who are attempting to duplicate prescriptions. All
data collected will be available to state and federal authorities, on whatever
timeframe they determine to be appropriate.” (PAR1005, p. 307; PAR1007, ¶83.)
At the very least, the “timeframe” referred to therein implies a periodic reporting.
(PAR1007, ¶83.) A POSA would have understood that such data generation and
querying via the central data repository is synonymous with generating periodic
reports via the exclusive computer database to evaluate potential diversion
patterns, as claimed, using a computer. (PAR1007, ¶83; see PAR1006, Tr., pg. 10
n.42; V5 00:10-00:27, V13 00:17-00:31; PAR1003, Tr., 24:21-24; PAR1005,
cover letter, pg. 1; PAR1007, ¶¶83-84.)
3. Claim 2
Claim 2 depends from claim 1, and further specifies that “the exclusive
central pharmacy controls the exclusive computer database.” (PAR1001, 9:4-5.)
ACA discloses this feature as discussed above, stating that the single national
specialty pharmacy (i.e., exclusive central pharmacy) controls the central data
repository (i.e., exclusive computer database). (See PAR1003, Tr. 177:24-178:11,

IPR Petition of U.S. Patent No. 7,895,059
-33-
184:24-185:7; Slides, pg. 147; PAR1004, pg. 108; PAR1005, pp. 304, 306;
PAR1006, Tr., pg. 4 n.13-14 and pg. 6 n.24; V5 00:09-00:27, V7 00:00-00:16;
PAR1007, ¶87.)
4. Claims 3 and 4
Claims 3 and 4 depend from claim 1 and further specify “selectively
blocking shipment of the prescription drug to a patient.” (Claim 3; PAR1001, 9:6-
7) and blocking shipment of the prescription drug upon association of an abuse
pattern with a patient. (Claim 4; PAR1001, 9:8-10.) ACA explicitly discloses these
features by instructing to deploy appropriate pharmacist intervention, such as
contacting authorities and flagging any inappropriate prescription requests, once
potential abuse situations are identified. (See PAR1003, Tr., 184:24-185:7; Slides
pg. 158; PAR1006, Tr., pg. 8 n. 29, pg. 9 n. 38; PAR1007, ¶89.) Additionally, such
intervention includes blocking shipment of the prescription drug to a patient prior
to filling a prescription in order to make the prescription drugs inaccessible to
those who would use it inappropriately. (See PAR1003, Tr., 184:24-185:7; Slides
pp. 142, 158; PAR1005, pg. 308; PAR1007, ¶90.) Accordingly, ACA explicitly
would have taught a POSA to selectively block a shipment of the prescription drug
to a patient, because ACA emphasizes the importance of preventing drug abuse
and the discretionary ability of the pharmacist to prevent a shipment of the drug to
identified patients. (PAR1007, ¶90.)

IPR Petition of U.S. Patent No. 7,895,059
-34-
5. Claim 5
Claim 5 depends from claim 1, and further specifies that the prescription
drug comprises gamma hydroxy butyrate (“GHB”). The active ingredient in
Xyrem®, the focus of ACA, was known as GHB. (See, e.g., PAR1003, Tr., 9:12-
17; PAR1007, ¶91; see also generally PAR1004; PAR1005; PAR1006.)
6. Claim 6
Claim 6 is an independent claim with similar limitations to those recited in
claim 1. The only differences between claim 6 and claim 1 are: (1) the term
“medical doctors” in “any and all medical doctors allowed to prescribe a
prescription drug” in claim 1 is replaced with “authorized prescribers.” (PAR1001,
9:19.); (2) the “exclusive computer database” is “under exclusive control of the
central pharmacy,” instead of “associated with the exclusive central pharmacy”
(Id., 9:24-25.); and (3) instead of “mailing or sending by courier the prescription
drug,” as in claim 1, claim 6 requires “providing the prescription drug.” (Id., 9:42.)
These differences do not change how ACA is applied to the claims. (PAR1007,
¶93.) As explained above, ACA discloses all of the features of claim 1.
Accordingly, the ACA also discloses and renders obvious all steps of claim 6. (Id.)
7. Claim 9
Likewise, the limitations of independent claim 9 are similar to those in claim
6. The only difference is that claim 9 recites GHB as the prescription drug. As
explained above for claim 5, Xyrem®—the drug to which ACA is directed—is

IPR Petition of U.S. Patent No. 7,895,059
-35-
GHB. (See PAR1003, Tr., 9:12-17.) Accordingly, the ACA also discloses all the
steps of claim 9. (PAR1007, ¶94.)
8. Claim 12
The limitations of claim 12 are similar to the limitations of claim 9. The only
difference is that instead of “providing GHB to the patient,” as recited by claim 9,
claim 12 requires “mailing or sending by courier GHB to the patient.” (PAR1001,
11:9.) This difference does not change the application of ACA to the claims, and
ACA discloses mailing or sending GHB by courier to the patient. (See PAR1003,
Tr., 178:5-6 and 182:17-23; Slides, pg. 146; PAR1004, pg. 109 and 115;
PAR1005, pg. 302, 304, and 311; PAR1006, V10 00:40-V11 00:31; PAR1007,
¶95.) As such, the ACA discloses and renders obvious all steps of claim 12.
9. Claim 13
“[M]anufacturing GHB and providing manufactured GHB only to the
exclusive central pharmacy”; ACA explicitly discloses that Xyrem®, known to
contain the active pharmaceutical ingredient GHB, is manufactured at one single
manufacturing facility and sent to one single national specialty pharmacy for
distribution. (See PAR1003, Tr., 178:3-5, 9:12-17; PAR1007, ¶97.)
The remaining limitations of claim 13: Each remaining limitation of claim
13 is identical to the limitations of claim 12. Accordingly, the ACA also discloses
and renders obvious all the remaining steps of claim 13. (PAR1007, ¶98.)

IPR Petition of U.S. Patent No. 7,895,059
-36-
10. Claim 14
The limitations of claim 14 are similar to those of claim 6 with the exception
being that claim 14 does not require the step of “generating with the computer
processor periodic reports via the exclusive computer database to evaluate
potential diversion patterns,” recited by claim 6. (PAR1001, 9:49-51.) Thus the
ACA discloses and renders obvious all steps of claim 14. (See § VI.B.6; PAR1007,
¶100.)
11. Claims 7, 10, and 15
Each of claims 7, 10, and 15 require that the central pharmacy authorizes the
prescription drug to be dispensed to the patient by another pharmacy.5 (PAR1001,
9:52-55, 10:35-38, and 12:37-40.) The ACA explicitly discloses shipping the
prescription GHB from the exclusive central pharmacy to another pharmacy for
patient pick-up. (PAR1004, pg. 110; PAR1007, ¶102.) Additionally, it is
envisioned that mechanisms will be put in place to “verify[] the second pharmacy’s
ability to protect against diversion of GHB before shipping.” (Id.) Therefore, the
benefits of preventing diversion and illicit use discussed in the disclosed
5 “As discussed in § IV.C., dispensed to the patient by another pharmacy”
would be understood by a POSA to mean “making the prescription drug that was
dispensed by the central pharmacy available for pick-up by the patient at another
pharmacy.”

IPR Petition of U.S. Patent No. 7,895,059
-37-
distribution program are left intact. Thus, the ACA explicitly discloses situations
that require having another pharmacy make available the medication. One such
situation would be if mandated by the patient’s insurance provider, as described by
ACA. (PAR1004, pg. 110; PAR1007, ¶102.)
12. Claims 8, 11, 16
Claims 8, 11, and 16 depend from claims 7, 10, and 15, respectively, and
further specify that “another pharmacy places controls on the distribution” of the
prescription drug or GHB. (PAR1001, 9:56-58; 10:39-40; 12:41-43.) The controls
are selected from the group consisting of:
confirming with the patient that the educational material has been
received and/or read by the patient, confirming receipt of the
prescription drug by the patient, contacting the patient’s insurance
company, questioning early refill requests by the patient, flagging
repeat instances of lost, stolen, destroyed or spilled prescriptions,
flagging that the patient paid cash for the prescription drug, flagging
early requests to refill the prescription drug, and limiting the
prescription to a supply of limited duration.
(PAR1001, 9:59-67, 10:41-50, 12:44-52.)
The ACA implicitly discloses that another pharmacy places controls on the
distribution. For example, the ACA discloses that the central pharmacy may
authorize another pharmacy to provide the prescription drug while putting in place
a “mechanism for verifying the second pharmacy’s ability to protect against

IPR Petition of U.S. Patent No. 7,895,059
-38-
diversion of GHB before shipping the drug there.” (PAR1004, pg. 110; PAR1007,
¶104.) ACA also explicitly discloses various controls that are placed on the
exclusive central pharmacy, which are similar to the controls recited by claims 8,
11, and 16. Those controls include (1) confirming with the patient that the
educational material has been received and/or read by the patient; (2) confirming
receipt of the prescription drug by the patient; (3) contacting the patient’s
insurance company; (4) flagging repeat instances of lost, stolen, destroyed or
spilled prescriptions; and (5) limiting the prescription to a supply of limited
duration. (PAR1003, Tr., 184:10-15, 371:10-12; Slides, pg. 157; PAR1004, pgs.
109, 110, and 115; PAR1006, Tr., pg. 7 n.26 and pg. 9 n. 35; PAR1007, ¶105.)
A POSA would have understood that the ACA discloses placing the same
controls on the distribution of the prescription drug by the “another pharmacy.”
(PAR1007, ¶105.) Such controls placed on the “another pharmacy” would be in
line with the ACA’s express goals of preventing abuse and diversion. (PAR1003,
Tr., 184:24-185:7; Slides, pgs. 158-159; PAR1005, pgs. 304, 305, and 311;
PAR1006, Tr., pg. 8 n.29 and pg. 9 n.38; PAR1007, ¶105.) Therefore, a POSA
would have understood that ACA discloses the claimed method of the authorized
another pharmacy placing controls on the distribution of the prescription drug,
because it discloses (1) placing such controls on distribution, (2) authorizing
another pharmacy to provide the drug with a “mechanism for verifying the second

IPR Petition of U.S. Patent No. 7,895,059
-39-
pharmacy’s ability to protect against diversion,” and (3) such a method would be in
line with the goals of the ACA’s disclosure. (PAR1007, ¶105.)
In sum, following the teachings of the combined Advisory Committee
references, a POSA would have combined the disclosed limitations as claimed
with no change to their respective functions. And the combination claimed in the
’059 patent yields nothing more than what was predicted in the Advisory
Committee references. Moreover, the claimed method steps were discussed in
detail in the prior art Advisory Committee references exactly as recited in the ’059
patent, and the art explained the techniques of reducing abuses of GHB to be had
by applying those steps. Such techniques would have been readily apparent and
predictable to a POSA, especially given the POSA’s own knowledge with drug
distribution procedures and minimizing abuses. Accordingly, the combined ACA
would have rendered claims 1-16 of the ’059 patent obvious to a POSA, even in
light of any secondary considerations (discussed in § VI.D.).
C. Ground 2: Claims 1-16 would have been obvious over TAS, in view of Honigfeld and Elsayed, and further in view of Lilly.
As supported by the declaration of Dr. Valuck, claims 1-16 of the ’059
patent would have been obvious over TAS as modified by Honigfeld, Elsayed, and
Lilly. A POSA would have had more than ample reason to combine each reference,
because TAS, Honigfeld, and Elsayed are all directed to the same endeavor—
controlled distribution of hazardous, but potentially beneficial, prescription drugs.

IPR Petition of U.S. Patent No. 7,895,059
-40-
(PAR1007, ¶107.) And a POSA would have had a reasonable expectation of
success of combining each reference, because doing so would have been nothing
more than combining prior art methods according to known techniques in order to
yield predictable results and/or use of known techniques to improve similar
methods in the same way.
Par incorporates herein the background information on Xyrem®, GHB,
Orphan Medical, and prior art restricted distribution programs discussed above and
with respect to Ground 1, and will not repeat them here.
1. Claim 1
Preamble: TAS discloses distributing Xyrem® through a “specialty
distribution system that will utilize a central pharmacy that will handle the delivery
of medicine to the patients,” (PAR1033, 1: ¶¶1-2, 5, 8-10; PAR1007, ¶108.)
Step 1.1: TAS discloses receiving prescription requests at a single central
pharmacy controlled by the Xyrem® sponsor. (PAR1033, 1: ¶¶ 8-9; PAR1007,
¶110.) TAS states: “to order Xyrem, a physician will write a prescription and fax
that to the central pharmacy. That pharmacy will process the prescription request
… and then set up a delivery time directly to [sic] the patient so that they may
receive their medicine.” (PAR1033, 1: ¶¶ 8-9.) Moreover, a POSA would have
found it obvious to modify TAS’ central pharmacy to receive prescription requests
using a computer processor into a single computer database, because it was well-

IPR Petition of U.S. Patent No. 7,895,059
-41-
known that pharmacies could use a single computer processor and database in
order to receive and fill prescription requests, as taught by the combination of
Honigfeld and Elsayed.
Honigfeld discloses a Clozaril National Registry (CNR) system used for the
centralized and controlled distribution of the prescription drug clozapine, “[t]he
heart” of which “is an integrated, computerized confidential database that is
maintained by the manufacturer,” (PAR1034, 6:2, ¶4; 4:2, ¶4; ; PAR1007, ¶111.),
in which all prescribers, pharmacists, and patients must be registered. (PAR1034,
4:2, ¶4; PAR1007, ¶111.) Once registered, the prescribing doctor sends the
pharmacy a prescription request, along with a reporting form that contains
information identifying the patient and the prescription drug. (See PAR1034, 5:1,
¶1; Fig. 1.; PAR1007, ¶111) Thus, Honigfeld teaches using a single computer
database to receive prescriptions and distribute prescription drugs. Moreover, a
POSA would have understood that the receipt of each prescription by CNR’s
computerized database would have been accomplished via a computer processor,
because it was well-known in the art that the transmission of data (e.g. prescription
requests) to a pharmacy, as described by Honigfeld, would have been
accomplished utilizing a computer processor. (PAR1007, ¶111)
Elsayed discloses distributing hazardous, but therapeutically beneficial
prescription drugs by registering patients, prescribers, and pharmacies in a

IPR Petition of U.S. Patent No. 7,895,059
-42-
“computer readable storage medium.” (PAR1035, 1:13-17, 3:21-23; 4:57-60, 7:28-
32; PAR1007, ¶112.) Registration takes place via on-line transmission of
prescription information—such as the doctor’s name, address, DEA number, and
hospital affiliation; the drug being prescribed; and the patient’s name, address, and
date of birth—to an authorized recipient. (PAR1035, 4:21-41, 5:23-37, and 5:40-
53; PAR1007, ¶112.) A POSA would have known that the “[s]uitable computer
readable storage media” disclosed in Elsayed included computerized databases.
(See, e.g., PAR1034, 4:2, ¶4; PAR1007, ¶112.) It would thus have been obvious to
a POSA from Elsayed that Honigfeld’s system could utilize a similar mechanism
to allow on-line transmission of prescriptions to CNR’s single computerized
database. (PAR1007, ¶¶113–114.) Such a modification would have been nothing
more than combining steps of prior art methods to yield predictable results. (Id.)
TAS, Honigfeld, and Elsayed would thus render step 1.1 obvious to a POSA.
TAS, Honigfeld, and Elsayed are all directed to the same endeavor—controlled
distribution of prescription drugs. A POSA would have had a reason to modify the
specialty distribution system disclosed in TAS to make use of the computerized
restricted distribution methods of Honigfeld and Elsayed, because it would have
allowed for the responsible distribution and the large scale, efficient centralization
and prescription of drugs—the exact goals of TAS, Honigfeld, and Elsayed.
(PAR1033, 2: ¶10; PAR1034, Abstract, 6:2,¶3-7:1,¶2; PAR1035, 1:14-17;

IPR Petition of U.S. Patent No. 7,895,059
-43-
PAR1007, ¶114.) And a POSA could have done so with a reasonable expectation
of success; both Honigfeld and Elsayed disclose computerized methods of
restricted distribution of a drug, and benefits that result in maintaining patient
compliance and in monitoring and controlling distribution. (See, e.g., PAR1034,
5:1, ¶2; PAR1035, 2:63-65 and 10:13-21; PAR1007, ¶114.) Furthermore, a POSA
could have applied Honigfeld and Elsayed to restrict distribution of a prescription
drug, such as Xyrem®. (See, e.g., PAR1035, 7:28-32.; PAR1007, ¶114.)
Steps 1.2 and 1.3: As discussed above for limitation 1.1, the combination of
TAS, Honigfeld and Elsayed discloses the receipt of prescription requests via a
computer processor into a single computer database of a central pharmacy. TAS as
modified by Honigfeld and Elsayed also discloses steps 1.2 and 1.3. Information
used in Honigfeld’s registration process includes the physician’s name, physician’s
DEA/ID number, and the patient’s initials, Social Security number (SSN), gender,
and date of birth. (See step 1.1 and PAR1007, ¶18.) Similarly, Elsayed discloses
registering patients and doctors in a computer readable storage medium via on-line
transmission of information—including the patient’s name, address, and date of
birth—to the drug’s distributor or an otherwise authorized recipient of such
information. (PAR1035, 4:21-41, 5:23-37, and 5:40-53, PAR1007, ¶119.) Thus,
Honigfeld and Elsayed combined teach entering the information recited by steps
1.2 and 1.3 into the single computer database.

IPR Petition of U.S. Patent No. 7,895,059
-44-
A POSA would also have understood to combine the restricted distribution
systems in Honigfeld and Elsayed with TAS’s single pharmacy for Xyrem.
(PAR1007, ¶121.) A POSA reading TAS would have had a reason to incorporate
Honigfeld and Elsayed’s teachings of registering physicians and patients into a
centralized computer database and checking that database (i.e., the claimed
information recited by limitations 1.2 and 1.3), because doing so would have
accomplished TAS’s purpose of regulating the distribution of Xyrem. (PAR1033,
1: ¶¶8-9; PAR1007, ¶¶116–117.) Moreover, Honigfeld and Elsayed also
recognized the same need as TAS—centralizing information needed to fill
prescription requests in a secure and regulated manner. (See, e.g., PAR1034, 5:1,
¶2; PAR1035, 2:63-65 and 10:13-21.) Thus, combining the teachings of TAS,
Honigfeld, and Elsayed in a manner meeting limitations 1.2 and 1.3 would have
been nothing more than combining steps of prior art methods to yield predictable
results. (PAR1007, ¶117.)
Step 1.4: Elsayed discloses that, prior to prescribing a drug, the prescriber
may counsel the patient on the drug’s various risks and benefits. (PAR1035, 6:4–
9). Elsayed also discloses that the prescriber can provide literature materials—
such as educational brochures and patient instruction videos—for a prescription
drug, and require the patient to fill out an informed consent form acknowledging
that the patient understands the risks associated with the drug and that the patient

IPR Petition of U.S. Patent No. 7,895,059
-45-
will behave in accordance with the prescriber’s counsel. (PAR1035, 6:26–20,
7:33–45.) It would have been obvious to a POSA to use such an “informed consent
form” to confirm the patient had received and/or read educational material.
(PAR1007, ¶124).
Steps 1.5 and 1.6: As discussed above, Honigfeld discloses screening
patients through a central computer database to prevent patients from receiving the
drug if a hazardous situation is indicated. (PAR1034, 4:2, ¶3.) Additionally, the
database provides data related to non-compliance with the drug’s distribution
system, which can result in the inability of the patient to receive the drug or the
doctor to prescribe the drug. (PAR1034, 5:1, ¶2.) Elsayed also discloses using a
computer readable storage medium to monitor and authorize distribution of
potentially hazardous prescription drugs (PAR1035, 4:50-57, 5:40-53, 5:59-61, and
10:13-17.) Likewise, Elsayed teaches checking the patient’s eligibility to receive
the drug before dispensing. (PAR1035, 9:65-10:2.) The computer readable storage
medium “may serve to deny access, dispension, or prescriptions” of hazardous
prescription drugs to patients and by doctors who fail to abide by the disclosed
methods. (PAR1035, 10:17-21.) A POSA would have found it obvious that
screening and denying access to prescription drugs (as described by Honigfeld and
Elsayed) would have included checking for abuse and not mailing (as described by
TAS) the drug to the patient if abuse was indicated. (PAR1007, ¶129.)

IPR Petition of U.S. Patent No. 7,895,059
-46-
Further, Lilly shows such techniques were well-known in the art. In Lilly,
when a pharmacist receives a new prescription request, the pharmacist, “utilizes …
pharmaceutical computer data to compare the new prescriptive medication with
respect to the medication history of the selected prescriptive medication purchaser”
and based on the medication history the pharmacist may accept or decline to fill
the prescription. (PAR1036, ¶[0039]; see also PAR1037, pp. 3:¶¶3-6 and; 8: Table
1.6) Lilly’s system helps pharmacies and government oversight entities (e.g., the
DEA) identify “potential medication abuse by identification of needless
prescription duplications … and multi-source interstate prescriptive medication
abuse.” (PAR1036, ¶[0054]; see also PAR1037, p.3:¶¶4-7.)
A POSA would have understood that TAS, Honigfeld, Elsayed, and Lilly
were combinable in a manner to result in steps 1.5 and 1.6. (PAR1007, ¶128.) TAS
discloses receiving prescription requests for Xyrem at a central pharmacy and
Honigfeld also discloses centralizing such a process to a single location.
(PAR1033, 1: ¶¶ 8-9; PAR1034, 4:2, ¶4, 6:2, ¶4, 5:1, ¶1; Fig. 1; PAR1007, ¶127.)
Honigfeld and Elsayed both recognize the need to prevent the dispensing of
6 Lilly claims priority to U.S. Ser. No. 60/332,807 (“’807 application)
(AMN1036) filed November 14, 2001. The limitations disclosed by Lilly are
disclosed by the ’807 application. Thus, Lilly qualifies as prior art to the claims
under 35 U.S.C. § 102(e) as of the ’807 application’s filing date.

IPR Petition of U.S. Patent No. 7,895,059
-47-
prescription drugs when a patient is not in compliance with established checks and
requirements. (See, e.g., PAR1034, 5:1, ¶2; PAR1035, 2:63-65 and 10:13-2;
PAR1007, ¶129.) A POSA would recognize that one of the checks TAS’
centralized pharmacy could use would be entering, maintaining and checking
information that indicates the abuse, misuse, or diversion of the prescription drug,
as disclosed by Lilly. (PAR1036, ¶¶ [0039], [0054]; see also PAR1037 pp. 3:¶¶2–
4, 6; 4:¶¶4-7,; 5:¶¶2-3 and, Fig. 1; 6:¶4; 7: Table 2, and 8: Table 1; PAR1007,
¶129.) Such checks for abuse or diversion were well-known in the industry and
modifying the combination of TAS, Honigfeld and Elsayed with the teachings of
Lilly would have been nothing more than use of known techniques to improve
similar methods in the same way. (PAR1007, ¶¶128–129.)
Step 1.7: TAS discloses that the dispensing pharmacy will call the patient to
set up a delivery time and then deliver the drug directly to the patient so that they
may receive their medicine. (PAR1033, 1). This has the effect of confirming the
patient’s receipt of the drug because it sets up a time at which the drug will be
delivered to the patient. (PAR1007, ¶131). Further, as of 2002, commercial
shippers (e.g., UPS, the U.S. Postal Service, and Federal Express) provided
tracking and delivery confirmation, such that confirming receipt of the prescription
drug would have been implicit in the step of shipping it as TAS disclosed. (Id.)

IPR Petition of U.S. Patent No. 7,895,059
-48-
Step 1.8: Honigfeld discloses using, “a large, full-time CNR staff is charged
with reviewing data on a retrospective basis.” (PAR1034, 5; PAR1007, ¶135.) The
staff’s “primary function is to identify discrepancies, such as missing data or low
WBCs associated with continued prescriptions.” (Id.) Elsayed discloses that
registering the patient, prescriber, and pharmacy in a computer readable medium
provides a means to monitor and authorize distribution of contraindicated drugs to
patients, and that the computer readable storage media may serve to deny access,
dispension, or prescriptions of drugs to patients, pharmacies, or prescribers who
fail to abide by the distribution program. (PAR1035, 10:13–20; PAR1007, ¶136.)
Likewise, Lilly discloses methods to prevent misuse and abuse of prescription
drugs by tracking prescriptions for drugs and/or controlled substances. (PAR1036,
¶[0032]; see also PAR1037, pp. 3:¶¶3-6 and 8: Table 1; PAR1007, ¶136). One step
for doing so is that when a patient or medication purchaser requests that the
pharmacist fill a new prescription medication, a pharmacy with a pharmacist may
use computer data to compare the new prescription with respect to the medication
history of the purchaser, and that the pharmacist may accept or decline to fill the
new prescription. (PAR1036, ¶[0039]; see also PAR1037, pp. 3:¶¶3-6 and; 8:
Table 1; ; PAR1007, ¶136) Further still, Lilly discloses that “[t]he DEA may
review [prescription] data to determine areas where violations may be occurring,”
such as abuse or misuse (PAR1036, ¶[0054]; see also PAR1037, pp. 4:¶¶4-7,;

IPR Petition of U.S. Patent No. 7,895,059
-49-
5:¶¶2-3 and, Fig. 1,; 6:¶4; 7: Table 2, and 8: Table 1; PAR1007, ¶136.) As such,
one of ordinary skill would have recognized that reports could be generated to
determine patterns of prescription misuse, abuse, or diversion. (PAR1007, ¶137.)
2. Claim 2
Claim 2 depends from claim 1, and further specifies that “the exclusive
central pharmacy controls the exclusive computer database.” (PAR1001, 9:4-5.)
TAS discloses that all prescriptions for Xyrem® will be sent to a single specialty
pharmacy that will fill the prescription requests. (PAR1033, ¶9.) Elsayed discloses
that the pharmacy may maintain patient information in the database. (PAR1035,
4:60–66). And as TAS discloses that all prescriptions for Xyrem will be sent to a
central pharmacy, the central pharmacy would be best positioned to control the
databases disclosed in Honigfeld, Elsayed, and Lilly (See PAR1007, ¶139).
3. Claims 3 and 4
Claims 3 and 4 depend from claim 1 and further specify “selectively
blocking shipment of the prescription drug to a patient.” (Claim 3; PAR1001, 9:6-
7) and blocking shipment of the prescription drug upon association of an abuse
pattern with a patient. (Claim 4; PAR1001, 9:8-10.) As discussed above in steps
1.5 and 1.6, Honigfeld and Elsayed disclose selectively blocking the provision of
the drug to the patient. (See also PAR1007, ¶141.) Further still, as discussed above
with regard to step 1.8, Lilly discloses selectively blocking provision of the drug to

IPR Petition of U.S. Patent No. 7,895,059
-50-
a patient if there are indications of abuse or misuse. (PAR1036, ¶[0039]; see also
PAR1037 pp. 3:¶¶3-4, 6 and; 8: Table 1; PAR1007, ¶141.). TAS discloses that all
prescriptions for Xyrem® will be mailed from a central pharmacy. (PAR1033,
1:¶9). It thus would have been obvious to block shipment of Xyrem® selectively if
any patient abuse or misuse is detected.
4. Claim 5
Claim 5 depends from claim 1, and further specifies that the prescription
drug comprises gamma hydroxy butyrate (“GHB”). TAS discloses the distribution
of Xyrem, which contains GHB. (See, e.g., PAR1003, 1: ¶8, 9; PAR1007, ¶142.)
5. Claim 6
Claim 6 is an independent claim with limitations similar to those in claim 1.
The only differences are: (1) the term “medical doctors” in “any and all medical
doctors allowed to prescribe a prescription drug” in claim 1 is replaced with
“authorized prescribers.” (PAR1001, 9:19.); (2) the “exclusive computer database”
is “under exclusive control of,” instead of “associated with,” the “exclusive central
pharmacy” (Id., 9:24-25.); and (3) instead of “mailing or sending by courier the
prescription drug only if no potential abuse is found by the patient to whom the
prescription drug is prescribed,” claim 6 requires “providing the prescription drug
only provided information in the exclusive computer database is not indicative of
potential abuse” (Id., 9:42.). These do not change how the prior art—TAS in view

IPR Petition of U.S. Patent No. 7,895,059
-51-
of Honigfeld, Elsayed, and Lilly—are applied to the claims, and each of these
limitations is disclosed in the prior art as identified above. (PAR1007, ¶144.)
“Authorized prescribers” would include “any and all medical doctors;” having an
“exclusive computer database” under “exclusive control of the central pharmacy”
is obvious for the same reasons identified in regard to claim 2, and “mailing or
sending” the prescription drug is one method of providing the drug to a patient.
Further, the cited prior art discloses checking databases for potential abuse and
selectively blocking shipment to the patient if potential abuse is found. (See steps
1.5 and 1.6, supra; see also claims 3 and 4, supra.) As such, TAS in view of
Elsayed, Honigfeld, and Lilly renders claim 6 obvious. (PAR1007, ¶144.)
6. Claim 9
The limitations of independent claim 9 are similar to those in claim 6. The
only difference is that claim 9 recites GHB as the prescription drug. TAS discloses
the distribution of Xyrem, which contains GHB. (See, e.g., PAR1003, ¶¶8, 9;
PAR1007, ¶145.)
7. Claim 12
The limitations of claim 12 are similar to the limitations of claim 9, though
instead of “providing GHB,” as recited by claim 9, claim 12 requires “mailing or
sending by courier GHB.” (PAR1001, 11:9.) TAS discloses shipping Xyrem,
which contains GHB, to patients. (See, e.g., PAR1003, 1:¶¶8, 9; PAR1007, ¶146.)

IPR Petition of U.S. Patent No. 7,895,059
-52-
8. Claim 13
The only difference between claims 12 and 13 is that claim 13 recites the
additional steps of “manufacturing GHB; and providing manufactured GHB only
to the exclusive central pharmacy.” TAS discloses that Xyrem®, which contains
GHB, will be manufactured and provided to one single pharmacy for distribution.
(See PAR1033, 1: ¶9; PAR1007, ¶147.) Accordingly, the prior art also discloses all
of the remaining limitations of claim 13. (PAR1007, ¶147.)
9. Claim 14
The limitations of claim 14 are similar to those of claim 6 with the exception
being that claim 14 does not require the step of “generating with the computer
processor periodic reports via the exclusive computer database to evaluate
potential diversion patterns,” as recited by claim 6. (PAR1001, 9:49-51.) As such,
TAS in view of Elsayed, Honigfeld, and Lilly discloses all of the limitations of
claim 14 because it discloses all steps of claim 6. (See § VI.C.6; PAR1007, ¶147.)
10. Claims 7, 10, and 15
Each of claims 7, 10, and 15 require that the central pharmacy authorizes the
prescription drug to be dispensed to the patient by another pharmacy.7 (PAR1001,
7 A POSA would understand “dispensed to the patient by another pharmacy”
to mean “making the prescription drug that was dispensed by the central pharmacy
available for pick-up by the patient at another pharmacy.” (See § IV.C.)

IPR Petition of U.S. Patent No. 7,895,059
-53-
9:52-55, 10:35-38, and 12:37-40.) As an initial matter, both Elsayed and Honigfeld
disclose that individual pharmacies may fill prescriptions for a particular drug, so
long as those pharmacies are registered with the distribution programs disclosed
therein. (PAR1034, 4; PAR1035, 4:50-66; 5:56–64; PAR1007, ¶151.) TAS
discloses that Xyrem will be available through a specialty distribution system that
will utilize a central pharmacy to handle delivery of medicine to the patients.
(PAR1033, 1: ¶8; PAR1007, ¶151.) As such, combining TAS with Elsayed and
Honigfeld allows a POSA to arrive at a method in which a central pharmacy
delivers drugs to other registered pharmacies for pick up, rendering obvious the
limitations of claims 7, 10, and 15. (PAR1007, ¶151.)
11. Claims 8, 11, 16
Claims 8, 11, and 16 depend from claims 7, 10, and 15, respectively, and
further specify that “another pharmacy places controls on the distribution” of the
prescription drug or GHB. (PAR1001, 9:56-58; 10:39-40; 12:41-43.) The controls
are selected from the group consisting of:
confirming with the patient that the educational material has been
received and/or read by the patient, confirming receipt of the
prescription drug by the patient, contacting the patient’s insurance
company, questioning early refill requests by the patient, flagging
repeat instances of lost, stolen, destroyed or spilled prescriptions,
flagging that the patient paid cash for the prescription drug, flagging
early requests to refill the prescription drug, and limiting the

IPR Petition of U.S. Patent No. 7,895,059
-54-
prescription to a supply of limited duration.
(PAR1001, 9:59-67, 10:41-50, 12:44-52.) As claims 8, 11, and 16 all recite that the
controls are “selected” from this group, only one control need be selected and
disclosed in the prior art for this claim to be rendered obvious. Elsayed renders the
control of “confirming with the patient that educational material has been received
and/or read” obvious for the reasons identified above with regards to step 1.4.
(PAR1007, ¶153.) Elsayed also discloses the additional control of “limiting the
prescription to a supply of limited duration,” as it discloses that “the drug is
preferably prescribed and dispensed to the patient in a limited amount, with a
prescription amount of no more than about 28 days being preferred, and preferably
with no refills being permitted.” (PAR1035, 9:29–32). Honigfeld also limits
prescription duration to no more than one week, linked to a current white blood
cell count. (See PAR1034, 5). As such, Talk About Sleep in view of Honigfeld,
Elsayed, and Lilly renders claims 8, 11, and 16 obvious. (PAR1007, ¶¶153–155.)
D. Secondary considerations do not rebut the prima facie case.
In addition to Par’s strong prima facie obviousness showing outlined above,
secondary considerations must be taken into account, although they do not
necessarily control the obviousness conclusion. See Newell Cos., Inc. v. Kenney
Mfg. Co., 864 F.2d 757, 768 (Fed. Cir. 1988). And in cases where a strong prima
facie obviousness showing exists, the CAFC has repeatedly held that even relevant

IPR Petition of U.S. Patent No. 7,895,059
-55-
secondary considerations supported by substantial evidence may not amount to a
showing of non-obviousness. See, e.g., Leapfrog Enterprises Inc. v. Fisher-Price
Inc., 485 F.3d 1157, 1162 (Fed. Cir. 2007). Moreover, objective evidence must be
attributable to the claimed invention, and aside from what is unclaimed or in the
prior art. In re Kao, 639 F.3d at 1068 (“Where the offered secondary consideration
actually results from something other than what is both claimed and novel in the
claim, there is no nexus to the merits of the claimed invention”). Jazz may argue
that secondary considerations of commercial success, long-felt but unmet need,
failure of others, copying, and unexpected superior results exist.
Jazz, by its Orange Book listing of the ’059 patent, contends that Xyrem®
must be distributed in conjunction with Xyrem®’s risk management program
claimed therein. However, Jazz cannot show that any alleged commercial success
was not due to an element in the prior art or the pharmaceutical effect of the active
ingredient. Additionally, Orphan itself indicated that the claimed risk management
program, which is disclosed in the Advisory Committee Art, would not contribute
to commercial sales because it would “eliminate[] the opportunity to ‘fill the retail
distribution pipeline.’” (PAR1005, pg. 309; PAR1007, ¶160.) Moreover,
commercial success is weak evidence in the context of products that require
regulatory approval, such as drugs. Merck & Co., Inc. v. Teva Pharms. USA, Inc.,
395 F.3d 1364, 1377 (Fed. Cir. 2005) (finding that commercial success of a drug

IPR Petition of U.S. Patent No. 7,895,059
-56-
subject to FDA approval was weak because regulatory barriers prevented other
companies from competing).
Jazz may also argue that a long-felt but unmet need is fulfilled because
Xyrem® would not have been approved by the FDA but for the Xyrem® risk
management program. However, there was no persistent, unmet need in the art for
a controlled distribution system. (PAR1007, ¶162.) Indeed, there were already in
place various risk management programs for the controlled distribution of
hazardous prescription drugs by December of 2002, as evidenced by the
Accutane®, Clozaril®, and prescription thalidomide distribution programs that
restricted distribution to only registered pharmacies, doctors, and patients.
Even if there had been a need in the art for an improved distribution program
for prescription drugs subject to abuse and diversion, there is no evidence to
suggest that the distribution programs already in the prior art could not have
satisfied that need. (PAR1007, ¶163.) Lastly, there were no inadequacies in the
technical knowledge that prevented the development of the claimed distribution
program. (Id.) All of the limitations of the claims of the ’059 patent were in the
prior art and did not require advances in technical knowledge to put them in place
to arrive at the claimed program. Instead, the FDA required the development of the
claimed distribution program as part of the approval process for Xyrem®. Friskit,
Inc. v. Real Networks, Inc., 2009 WL 59182, *6 (Fed. Cir. 2009) (nonprecedential)

IPR Petition of U.S. Patent No. 7,895,059
-57-
(long-felt need should be a need created by inadequacies in the technical
knowledge, not one due to business-driven market forces) (PAR1007, ¶164.)
Orphan admitted during prosecution of the parent to the ’059 patent that:
[T]he Applicant and the Food and Drug Administration (FDA) were
involved in relating to a new indication for the drug gamma hydroxyl
butyrate (GHB), and how the patent application [for the ’730 patent]
was borne out of this FDA approval process.”
(PAR1016, Amendment & Response, filed Nov. 2, 2009, pg. 9.) Similarly, Jazz
cannot point to failure of others to arrive at the claimed distribution methods. As
noted above, efficacious distribution programs for hazardous, but therapeutically
beneficial, prescription drugs were known in the art prior to December of 2002.
(Id., ¶165.) These distribution programs were successful in preventing the harms
associated with prescribing these drugs to patients. (Id.) Thus, Jazz cannot
successfully allege previous failures or long-felt but unresolved need weigh in
favor of the non-obviousness of the claims of the ’059 patent. (Id.)
Jazz cannot also argue that the development of distribution programs for
generic sodium oxybate by Par or other generic pharmaceutical companies
constitutes copying. Evidence of copying simply is not probative of non-
obviousness in the generic drug context. See Bayer Healthcare Pharms. v. Watson
Pharms., Inc., 713 F.3d 1369, 1377 (Fed. Cir. 2013).
Finally, Jazz may allege that the inventions claimed in the ’059 patent

IPR Petition of U.S. Patent No. 7,895,059
-58-
achieve unexpected results by enabling the beneficial treatment of narcolepsy
with Xyrem®. As an initial matter, any beneficial results of Xyrem® are likely a
result of the treatment of narcoleptic patients with GHB, and not the claimed
distribution program. (PAR1007, ¶167.) And, the use of GHB to treat narcolepsy
was well-known in the art by December of 2002. (Id.) Moreover, the claimed
distribution program does not have a significant and practical advantage over the
closest prior art that discloses all of the limitations of the claimed distribution
program. In re De Blauwe, 736 F.2d 699, 705 (Fed. Cir. 1984) (unexpectedly
superior results must establish that the alleged invention in the challenged claims
achieved unexpectedly superior results with respect to the results of the closest
prior art). As such, Jazz’s arguments of unexpected results fail. (PAR1007, ¶167.)
VII. IT IS MORE LIKELY THAN NOT THAT PETITIONER WILL PREVAIL WITH RESPECT TO AT LEAST ONE OF THE CHALLENGED CLAIMS
This petition, supported by the Valuck Dec. (PAR1007), amply
demonstrates that it is more likely than not that Par will prevail with respect to at
least one challenged claim.
VIII. MANDATORY NOTICES (37 C.F.R. § 42.8(a)(1))
The Real Party-In-Interest (37 C.F.R. § 42.8(b)(1)) is: Par
Pharmaceutical, Inc., (“Par”). Notice of Related Matters (37 C.F.R. §
42.8(b)(2)): Jazz has asserted the ’059 patent in two related litigations: Jazz

IPR Petition of U.S. Patent No. 7,895,059
-59-
Pharms, Inc. v. Par Pharm., Inc., 2:13-cv-07884 (D.N.J. Dec. 27, 2013)
(consolidated with Jazz Pharms., Inc. v. Amneal Pharms., LLC, 2:13-cv-00391
(D.N.J.); and Jazz Pharms, Inc. v. Roxane Laboratories, Inc., 2:10-cv-06108
(consolidated) (D.N.J. Nov. 22, 2010). The ’059 patent is also the subject of a
Covered Business Method Patent Review Petition: Par Pharmaceutical, Inc. et al.
v. Jazz Pharms., Inc., CBM2014-00149 (filed June 24, 2014). Five related patents,
U.S. Patent 8,475,988, 7,668,730, 8,589,182, 7,765,106 and 7,765,107 are the
subject of the following respective Covered Business Method Patent Petitions:
Amneal Pharms, LLC et al. v. Jazz Pharms., Inc., CBM2014-00150 (filed July 7,
2014); Par Pharm. Inc. et al. v. Jazz Pharms, Inc., CBM2014-00151 (filed July 9,
2014) and CBM2014-00153 (filed July 9, 2014); Par Pharm. Inc. et al. v. Jazz
Pharms, Inc., CBM2014-00161 (filed August 4, 2014); and Par Pharm. Inc. et al.
v. Jazz Pharms, Inc., CBM2014-00175 (filed August 18, 2014).
Designation of Lead and Back-Up Counsel (37 C.F.R. § 42.8(b)(3)):
Lead Counsel Back-Up Counsel
Aziz Burgy (Reg. #51,514) ARENT FOX LLP 1717 K Street NW Washington, DC 20036-5342 202.857.6378 (telephone) 202.857.6395 (facsimile) [email protected]
Bradford C. Frese (Reg. #69,772) ARENT FOX LLP 1717 K Street NW Washington, DC 20036-5342 202.857.6496 (telephone) 202.857.6395 (facsimile) [email protected]
Notice of Service Information (37 C.F.R. § 42.8(b)(4)): Please direct all
correspondence to counsel at the above address. Par consents to email service at:

IPR Petition of U.S. Patent No. 7,895,059
-60-
IX. CONCLUSION
For the reasons above, Par requests that the Board institute IPR of all claims
of the ’059 patent, and cancel those claims. Attached are a Power of Attorney, an
Exhibit List, and copies of the references per § 42.10(b), § 42.63(e), and § 42.6(c).
The required fees are to be paid via withdrawal from Deposit Account No. 01-2300
(Customer ID No. 04372), and the Office is authorized to charge fee deficiencies
and credit overpayments to the same account.
Respectfully Submitted,
Aziz Burgy Registration No. 51,514 Attorney for Petitioner
Date: January 8, 2015 ARENT FOX LLP 1717 K Street, NW Washington, DC 20006 202.857.6000

IPR Petition of U.S. Patent No. 7,895,059 Certificate of Service
CERTIFICATION OF SERVICE (37 C.F.R. §§ 42.6(e), 42.105(a))
The undersigned hereby certifies that the above-captioned “Petition for Inter
Partes Review of U.S. Patent No. 7,895,059 Under 35 U.S.C. § 311–319 and 37
C.F.R. § 42.1–.80, 42.100–.123” including its supporting evidence (EXHIBITS
1001-1039), was served in its entirety on January 8, 2015, upon the following
parties via Express Mail:
Schwegman Lundberg & Woessner/Jazz Pharmaceutical P.O. Box 2938 Minneapolis MN 55402 Patent owner’s correspondence address of record for U.S. Patent No. 7,895,059
F. Dominic Cerrito Eric C. Stops Gabriel P. Brier QUINN EMANUEL URQUHART & SULLIVAN LLP 51 Madison Avenue 22nd Floor New York, NY 10010
Richard G. Greco RICHARD G. GRECO PC 90 State Street, Suite 700 Albany, New York 12207 John V. Biernacki Jones Day North Point 901 Lakeside Avenue Cleveland, OH 44114
Additional addresses known to Petitioner as likely to effect service

IPR Petition of U.S. Patent No. 7,895,059 Certificate of Service
Respectfully Submitted,
Aziz Burgy Registration No. 51,514 Attorney for Petitioner
Date: January 8, 2015 ARENT FOX LLP 1717 K Street, NW Washington, DC 20006 202.857.6000