Embed Size (px)
Citation preview
Paper Based vs Electronic Based Clinical Records
The effects on hospital statistics
Class 18

Introduction
Recording clinical information is important to the health industry
Access to previous information leads to better diagnosis and treatment in the future [Movig KL, Leufkens HG, Lenderink AW, Egberts AC. Validity of hospital discharge International Classification of Diseases (ICD) codes for identifying patients with hyponatremia. J Clin Epidemiol. 2003 Jun;56(6):530-5.]
Paper-based record / Electronic records
Paper Based vs Electronic Based Clinical Records

Lacks of information of previous studies [Movig KL, Leufkens HG, Lenderink AW, Egberts AC. Validity of hospital discharge International Classification of Diseases (ICD) codes for identifying patients with hyponatremia. J Clin Epidemiol. 2003 Jun;56(6):530-5.]
Electronic patient record (EPR) as the main method in a near future.[Gillies J, Holt A. Anxious about electronic health records? No need to be. N Z Med J. 2003 Sep 26;116(1182):U604.]
It is important to study and to conclude if this new information organization will result in any difference from the old one.
Paper Based vs Electronic Based Clinical Records

Advantages and disadvantages of EPR and paper-based records. Most of the studies conclude that the electronic system is better, although some of them disagree. [ Van der Meijden MJ, Tange HJ, Boiten J, Troost J, Hasman A. An experimental electronic patient record for stroke patients. Part 1: situation analysis. Int J Med Inform. 2000 Sep;58-59:111-25]
Paper Based vs Electronic Based Clinical Records

Main difficulties in the implementation of EPR.[Mohr DN, Carpenter PC, Claus PL, Hagen PT, Karsell PR, Van Scoy RE. Implementing an EMR: paper's last hurrah. Proc Annu Symp Comput Appl Med Care. 1995;:157-61.]
Negligent data introduction.
[Friedman BA. The potential role of physicians in the management of hospital information systems. Clin Lab Med. 1990 Mar;10(1):239-50]
Typing and visualization speed.[Rodriguez NJ, Murillo V, Borges JA, Ortiz J, Sands DZ. A usability study of physicians interaction with a paper-based patient record system and a graphical-based electronic patient record system. Proc AMIA Symp. 2002;:667-71.]
Paper Based vs Electronic Based Clinical Records

Coding errors (ICD). [Movig KL, Leufkens HG, Lenderink AW, Egberts AC. Validity of hospital discharge International Classification of Diseases (ICD) codes for identifying patients with hyponatremia. J Clin Epidemiol. 2003 Jun;56(6):530-5.]
Costs and benefits of EPR.[Ellingsen G, Monteiro E. Big is beautiful: electronic patient records in large Norwegian hospitals 1980s-2001. Methods Inf Med. 2003;42(4):366-70.]
Hospital’s economical survival.[Muller ML, Burkle T, Irps S, Roeder N, Prokosch HU. The diagnosis related groups enhanced electronic medical record. Int J Med Inform. 2003 Jul;70(2-3):221-8.]
Paper Based vs Electronic Based Clinical Records

Objective
The main objective is:
Quantify the differences among diagnosis and procedures recorded before and after the EPR implementation in the paper-based and the electronic-based methods.
Paper Based vs Electronic Based Clinical Records

Methods
Participants and Methods
Type of study: it is longitudinal and observational
We chose two departments to work about (obstetrics and pneumology) and two periods of time (a few months before and after the implementation of EPR)
We treated two databases on SPSS®, each from one of the departments
Each database was divided in two periods, before and after the implementation
Paper Based vs Electronic Based Clinical Records

Inclusion criteria
We made a selection of the main diagnosis on each department: On the obstetrics department we chose those with a
minimum number of 20 cases on the sum of both periods On the pneumology department we chose those with a
minimum number of 10 cases on the sum of both periods
We did two kinds of analyses: a qualitative one and a quantitative one.
Paper Based vs Electronic Based Clinical Records
Methods – 1st PeriodFirst Period
Each DRG code consists on a general code that groups together several diagnoses into one variable
Each database was divided in two periods: Before and After EPR
Qualitative Analysis The qualitative analysis consists on checking the differences
between the GDH before and after the introduction of EPR
By using a statistical test (Chi-square) on SPSS® we have searched for significant differences between GDH from the two groups previously selected
After analyzing the differences in a major perspective we decided to check each GDH individually to quantify the differences by using another Chi-square test.
Paper Based vs Electronic Based Clinical Records

Quantitative Analysis
(it focuses on the number of the diagnosis rather than the type of diagnosis)
We started working with all the diagnosis instead of using only GDH in order to compare the number of diagnosis before and after the implementation
The main test used in this case was a Mann-Whitney test
Paper Based vs Electronic Based Clinical Records

Methods – 2nd Period
Paper Based vs Electronic Based Clinical Records
Second Period
The database used in the first period was changed into one that allowed us to check the frequency of each diagnosis/procedure separately.
The diagnosis/procedures selected were the fifteen with more cases on the sum of the before and after periods.
Using SPSS® the information was analised in two differente ways: General Approach to the data including the 15 diagnosis/procedures,
using a chi-square test. Each diagnosis/procedure was checked for differences between the
two periods of time, using chi-square tests.
Both doctors and coders from both departments were enquired in search for justification for the statistically significant differences found

Linear Flow Chart
Paper Based vs Electronic Based Clinical Records
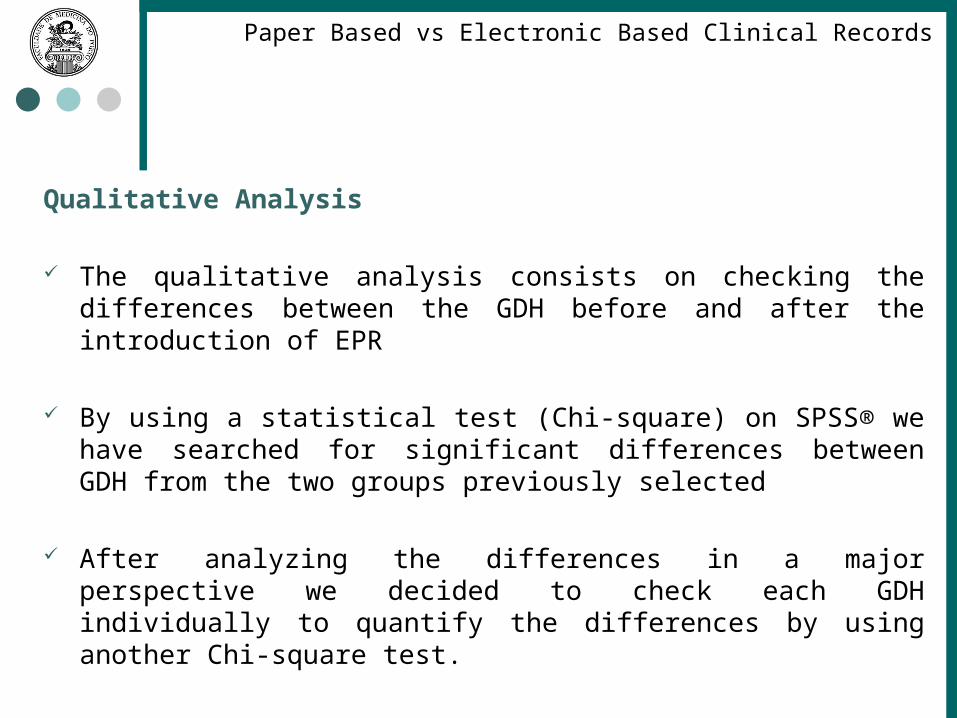
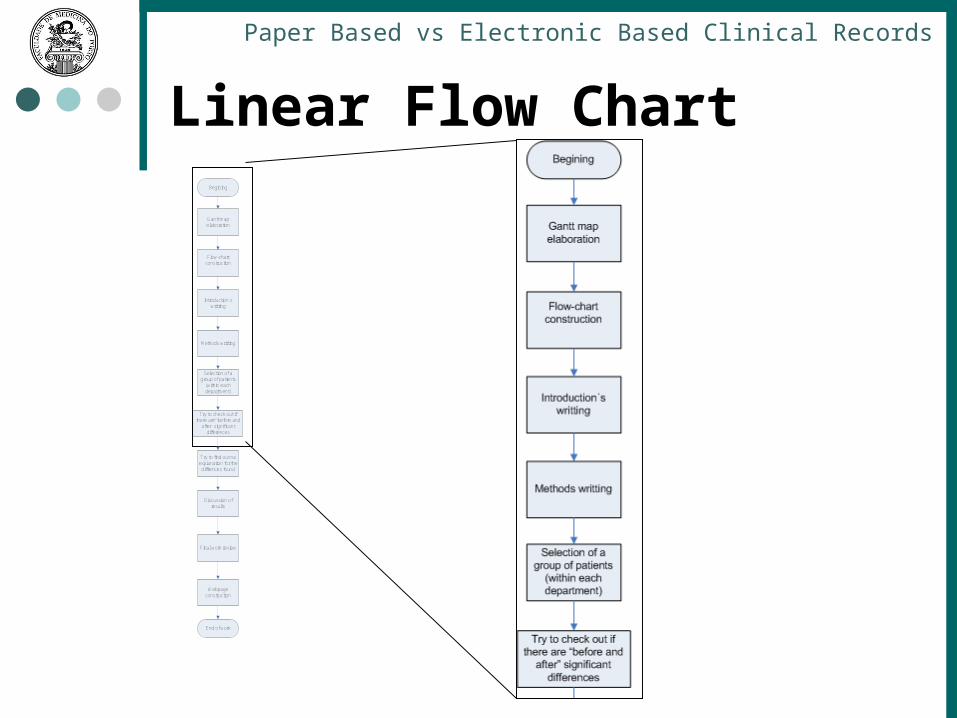
Begining
Gantt map elaboration
Flow-chart construction
Introduction´s writting
Methods writting
Selection of a group of patients
(within each department)
Try to check out if there are “before and
after” significant differences
Try to find out na explanation for the
diffrences found
Discussion of results
Final work review
Webpage construction
End of work
Linear Flow Chart
Paper Based vs Electronic Based Clinical Records
Begining
Gantt map elaboration
Flow-chart construction
Introduction´s writting
Methods writting
Selection of a group of patients
(within each department)
Try to check out if there are “before and
after” significant differences
Try to find out na explanation for the diffrences found
Discussion of results
Final work review
Webpage construction
End of work

Linear Flow Chart
Paper Based vs Electronic Based Clinical Records
Begining
Gantt map elaboration
Flow-chart construction
Introduction´s writting
Methods writting
Selection of a group of patients
(within each department)
Try to check out if there are “before and
after” significant differences
Try to find out na explanation for the
diffrences found
Discussion of results
Final work review
Webpage construction
End of work
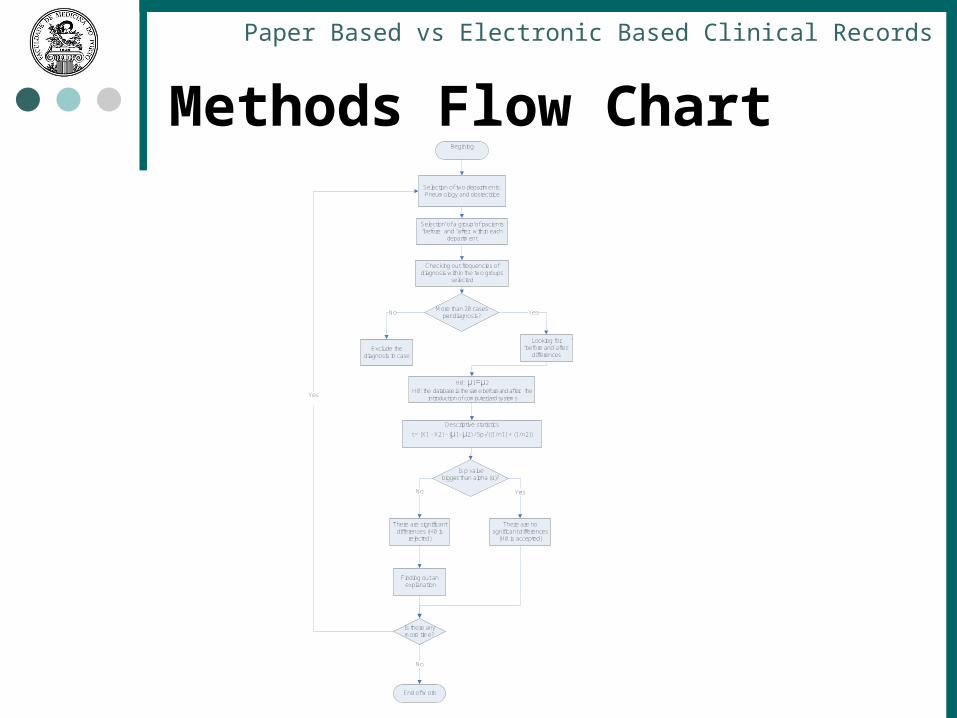
Methods Flow Chart
Paper Based vs Electronic Based Clinical Records
Begining
Is there any more time?
No
End of Work
Is p value bigger than alpha (α)?
Yes No
Yes
Selection of two departments:Pneumology and obstectrice
Selection of a group of pacients “before” and “after” within each
department
Checking out frequencies of diagnosis within the two groups
selected
H0: µ1=µ2H0: the database is the same before and after the
introduction of computerized systems
Descriptive statistics
t = (X1 - X2) - (µ1- µ2) / Sp √((1/ n1) + (1/ n2))
There are significant differences (H0 is
rejected)
There are no sgnificant differences
(H0 is accepted)
Finding out an explanation
More than 20 cases per diagnosis?
Looking for “before and after”
differencesExclude the
diagnosis in case
Yes No

Methods Flow Chart
Paper Based vs Electronic Based Clinical Records
Begining
Is there any more time?
No
End of Work
Is p value bigger than alpha (α)?
Yes No
Yes
Selection of two departments:Pneumology and obstectrice
Selection of a group of pacients “before” and “after” within each
department
Checking out frequencies of diagnosis within the two groups
selected
H0: µ1=µ2H0: the database is the same before and after the
introduction of computerized systems
Descriptive statistics
t = (X1 - X2) - (µ1- µ2) / Sp √((1/ n1) + (1/ n2))
There are significant differences (H0 is
rejected)
There are no sgnificant differences
(H0 is accepted)
Finding out an explanation
More than 20 cases per diagnosis?
Looking for “before and after”
differencesExclude the
diagnosis in case
Yes No

Methods Flow Chart
Paper Based vs Electronic Based Clinical Records
Begining
Is there any more time?
No
End of Work
Is p value bigger than alpha (α)?
Yes No
Yes
Selection of two departments:Pneumology and obstectrice
Selection of a group of pacients “before” and “after” within each
department
Checking out frequencies of diagnosis within the two groups
selected
H0: µ1=µ2H0: the database is the same before and after the
introduction of computerized systems
Descriptive statistics
t = (X1 - X2) - (µ1- µ2) / Sp √((1/ n1) + (1/ n2))
There are significant differences (H0 is
rejected)
There are no sgnificant differences
(H0 is accepted)
Finding out an explanation
More than 20 cases per diagnosis?
Looking for “before and after”
differencesExclude the
diagnosis in case
Yes No
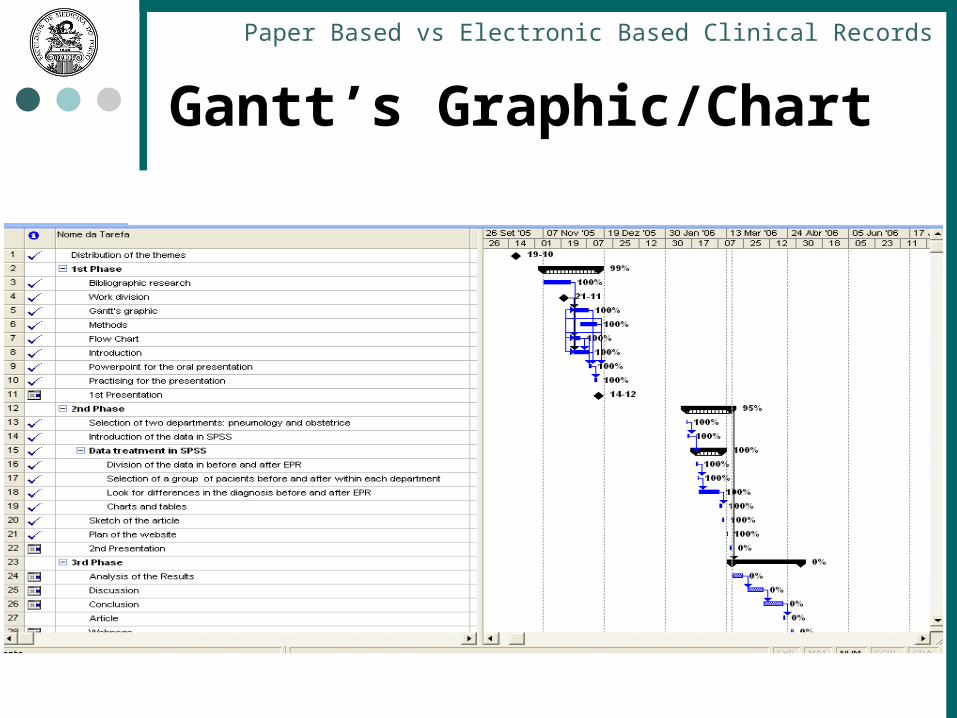
Gantt’s Graphic/Chart
Paper Based vs Electronic Based Clinical Records

1st Period
Paper Based vs Electronic Based Clinical Records
1st Period

Results
Paper Based vs Electronic Based Clinical Records
Departament Before After
Obst 887 975
Pneumo 292 293
Table 1 - Total number of individuals on both departments, before and after the EPR implementation.

Results - Obstetrics department
others384383381380379373372371370362
GDH Diagnosis' code
60,0%
50,0%
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depois
antes
Graph 1 – Comparison between the two groups
GDH code
Diagnosis description
362 ENDOSCOPIC TUBAL INTERRUPTION
370 CESAREAN SECTION WITH CC
371 CESAREAN SECTION WITHOUT CC
372 VAGINAL DELIVERY WITH COMPLICATING DIAGNOSES
373 VAGINAL DELIVERY WITHOUT COMPLICATING DIAGNOSES
379 THREATENED ABORTION
380 ABORTION W/O D&C
381 ABORTION WITH D&C, ASPIRATION CURETTAGE OR HYSTEROTOMY
383 OTHER ANTEPARTUM DIAGNOSES WITH MEDICAL COMPLICATIONS
384 OTHER ANTEPARTUM DIAGNOSES WITHOUT MEDICAL COMPLICATIONS
Table 2 – Description of the GDH code from the selected diagnosis.
Paper Based vs Electronic Based Clinical Records

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
others384383381380379373372371370362
GDH Diagnosis' code
60,0%
50,0%
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depois
antes
Graph 1 – Comparison between the two groups
Table 4 – % of each diagnosis on both periods
GDH cod
e
Before (%) After (%)
362 2,7 0
370 3,5 3,2
371 26,2 19,3
372 3,4 4,0
373 46,3 53,4
379 2,0 1,4
380 3,0 3,4
381 2,9 3,0
383 1,6 2,5
384 4,7 5,2
others 3,6 4,6

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
others384383381380379373372371370362
GDH Diagnosis' code
60,0%
50,0%
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depois
antes
Graph 1 – Comparison between the two groups
Chi-Square Tests
45,670a 10 ,000
54,925 10 ,000
1,203 1 ,273
1862
Pearson Chi-Square
Likelihood Ratio
Linear-by-LinearAssociation
N of Valid Cases
Value dfAsymp. Sig.
(2-sided)
0 cells (,0%) have expected count less than 5. Theminimum expected count is 11,43.
a.

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Diagnosis: “Parto Vaginal sem complicações” (GDH373)
In a first phase we searched for general differences in the GDH.Secondly we searched for differences on each individual GDH. This is an example of a GDH where we found statistically significant differences. The other cases are: “Cesariana sem complicações” (GDH371); and “Laqueação de trompas via laparoscópia” (GDH362).

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Descriptives
2,5175 ,03716
2,4445
2,5904
2,4376
2,0000
1,225
1,10686
1,00
6,00
5,00
1,00
1,067 ,082
1,123 ,164
2,5590 ,03790
2,4846
2,6334
2,4655
2,0000
1,401
1,18355
1,00
6,00
5,00
1,00
1,177 ,078
1,170 ,156
Mean
Lower Bound
Upper Bound
95% ConfidenceInterval for Mean
5% Trimmed Mean
Median
Variance
Std. Deviation
Minimum
Maximum
Range
Interquartile Range
Skewness
Kurtosis
Mean
Lower Bound
Upper Bound
95% ConfidenceInterval for Mean
5% Trimmed Mean
Median
Variance
Std. Deviation
Minimum
Maximum
Range
Interquartile Range
Skewness
Kurtosis
Antes_ou_Depoisantes
depois
n_ddxStatistic Std. Error

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Although it seems obvious that this isn’t a normal distribution we decided to confirm by doing an one sample K-S Test.

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
One-Sample Kolmogorov-Smirnov Test
887
2,5175
1,10686
,288
,288
-,194
8,565
,000
975
2,5590
1,18355
,298
,298
-,196
9,307
,000
N
Mean
Std. Deviation
Normal Parameters a,b
Absolute
Positive
Negative
Most ExtremeDifferences
Kolmogorov-Smirnov Z
Asymp. Sig. (2-tailed)
N
Mean
Std. Deviation
Normal Parameters a,b
Absolute
Positive
Negative
Most ExtremeDifferences
Kolmogorov-Smirnov Z
Asymp. Sig. (2-tailed)
Antes_ou_Depoisantes
depois
n_ddx
Test distribution is Normal.a.
Calculated from data.b.
Ranks
887 929,36 824343,50
975 933,45 910109,50
1862
Antes_ou_Depoisantes
depois
Total
n_ddxN Mean Rank Sum of Ranks
Test Statisticsa
430515,5
824343,5
-,175
,861
Mann-Whitney U
Wilcoxon W
Z
Asymp. Sig. (2-tailed)
n_ddx
Grouping Variable: Antes_ou_Depoisa.
Mann-Whitney
The 1-sample K-S test confirmed that it wasn’t a normal distribution as
p<0,01 , so it is <0,05.
As it wasn’t a normal distribution we had to do a non-parametric
test for two independent variables.As we can see p=0,861 which is >0,05, so we accept nule
hypothesis.

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
others475,00101,0099,0095,0094,0092,0089,0088,0085,0082,0079,0076,0075,00
SELECT
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depoisantes
GDH code Diagnosis description
75 MAJOR CHEST PROCEDURE
76 OTHER RESPIRATORY SYSTEM OR PROCEDURES WITH CC
79 RESPIRATORY INFECTIONS AND INFLAMATIONS, AGE >17, WITH CC
82 RESPIRATORY NEOPLASM
85 PLEURAL EFFUSION WITH CC
88 CHRONIC OBSTRUCTIVE PULMONARY DISEASES
89 PNEUMONIA AGE 18 OR OLDER WITH COMPLICATION, BACTERIAL, VIRAL, AND BRONCHIAL PNEUMONIA AND
PLEURISY.
92 INTERSTICIAL LUNG DISEASE WITH CC
94 PNEUMOTHORAX WITH CC
95 PNEUMOTHORAX WITHOUT CC
99 RESPIRATORY SIGND AND SYMPTOMS WITH CC
101 OTHER RESPIRATORY SYSTEM DIAGNOSES W CC
475 RESPIRATORY SYSTEM DIAGNOSIS WITH VENTILATION SUPPORT
Graph 2 – Comparison between the two groups
Table 5 – Description of the GDH code from the selected diagnosis.

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
others475,00101,0099,0095,0094,0092,0089,0088,0085,0082,0079,0076,0075,00
SELECT
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depoisantes
Graph 2 – Comparison between the two groups
GDH code Before (%) After (%)
75 1,7 2,7
76 2,7 2,1
79 8,5 6,8
82 37,2 26,7
85 2,0 2,1
88 10,2 11,6
89 5,8 7,5
92 2,0 2,1
94 1,0 3,1
95 4,8 5,1
99 2,4 2,7
101 2,4 5,8
475 1,4 2,4
Others 17,7 19,2
Table 7 – % of each diagnosis on both periods

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
others475,00101,0099,0095,0094,0092,0089,0088,0085,0082,0079,0076,0075,00
SELECT
40,0%
30,0%
20,0%
10,0%
0,0%
Per
cen
t
depoisantes
Graph 2 – Comparison between the two groups
Chi-Square Tests
15,796a 13 ,260
16,110 13 ,243
,214 1 ,644
585
Pearson Chi-Square
Likelihood Ratio
Linear-by-LinearAssociation
N of Valid Cases
Value dfAsymp. Sig.
(2-sided)
0 cells (,0%) have expected count less than 5. Theminimum expected count is 5,49.
a.

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
Diagnosis:“Neoplasias Respiratórias”(GDH82) Regarding pneumology, we followed the same procedure we used for obstretics. We searched for differences both generally and individually for significant GDH’s. Here is one exemple we found. The other significant GDH we found was “Outros diagnósticos de aparelho respiratório com complicações” (GDH101).

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
Descriptives
8,1877 ,28006
7,6365
8,7389
7,8790
7,0000
22,982
4,79393
1,00
20,00
19,00
5,50
,936 ,142
,272 ,284
7,4144 ,25710
6,9084
7,9204
7,0738
7,0000
19,302
4,39340
1,00
20,00
19,00
6,00
1,050 ,143
1,100 ,284
Mean
Lower Bound
Upper Bound
95% ConfidenceInterval for Mean
5% Trimmed Mean
Median
Variance
Std. Deviation
Minimum
Maximum
Range
Interquartile Range
Skewness
Kurtosis
Mean
Lower Bound
Upper Bound
95% ConfidenceInterval for Mean
5% Trimmed Mean
Median
Variance
Std. Deviation
Minimum
Maximum
Range
Interquartile Range
Skewness
Kurtosis
Antes_e_Depoisantes
depois
n_diagStatistic Std. Error

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
Although it seems obvious that this isn’t a normal distribution we decided to confirm by doing an one sample K-S Test.

Results – Pneumology department
Paper Based vs Electronic Based Clinical Records
One-Sample Kolmogorov-Smirnov Test
293
8,1877
4,79393
,147
,147
-,095
2,517
,000
292
7,4144
4,39340
,111
,111
-,075
1,903
,001
N
Mean
Std. Deviation
Normal Parameters a,b
Absolute
Positive
Negative
Most ExtremeDifferences
Kolmogorov-Smirnov Z
Asymp. Sig. (2-tailed)
N
Mean
Std. Deviation
Normal Parameters a,b
Absolute
Positive
Negative
Most ExtremeDifferences
Kolmogorov-Smirnov Z
Asymp. Sig. (2-tailed)
Antes_e_Depoisantes
depois
n_diag
Test distribution is Normal.a.
Calculated from data.b.
Ranks
293 305,00 89366,00
292 280,96 82039,00
585
Antes_e_Depoisantes
depois
Total
n_diagN Mean Rank Sum of Ranks
Test Statisticsa
39261,000
82039,000
-1,726
,084
Mann-Whitney U
Wilcoxon W
Z
Asymp. Sig. (2-tailed)
n_diag
Grouping Variable: Antes_e_Depoisa.
Mann-Whitney
The 1-sample K-S test confirmed that it wasn’t a normal distribution as
p<0,01 , so it is <0,05.
As it wasn’t a normal distribution we had to do a non-parametric
test for two independent variables.As we can see p=0,084 which is >0,05, so we accept nule
hypothesis.

2nd Period
Paper Based vs Electronic Based Clinical Records
2nd Period

others
664,01
661,21
661,11
661,01
659,71
658,11
656,11
654,21
650,00
648,81
648,21
644,21
631,00
V27.0
V25.2
Dia
gn
osi
s
40,0%30,0%20,0%10,0%0,0%
PercentAfterBefore
Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
General (differences were found)
Pearson Chi-Square126,435(
a)15 ,000
Likelihood Ratio134,712 15 ,000
Linear-by-Linear Association 9,705 1 ,002
N of Valid Cases4728
Value dfAsymp. Sig.
(2-sided)
a 0 cells (,0%) have expected count less than 5. The minimum expected count is 24,56.
Diagnosis - Obstetrics

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Diagnosis - Obstetrics
Diagnosis where differences were found
V25.2 - Request for sterillization654.21 - Previous cesarean section664.01 – First-degree perineal laceration661.11 - Secondary uterine inertia648.21 - Anemia656.11 - Rhesus isoimmunization
others
664,01
661,21
661,11
661,01
659,71
658,11
656,11
654,21
650,00
648,81
648,21
644,21
631,00
V27.0
V25.2
Dia
gn
osi
s
40,0%30,0%20,0%10,0%0,0%
PercentAfterBefore

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Procedures - Obstetrics
General (differences were found)
Pearson Chi-Square532,269(
a)15 ,000
Likelihood Ratio584,291 15 ,000
Linear-by-Linear Association 37,784 1 ,000
N of Valid Cases8136
Value dfAsymp. Sig.
(2-sided)
0 cells (,0%) have expected count less than 5. The minimum expected count is 58,69.
others
99,29
99,21
99,18
93,57
90,59
88,78
75,35
75,34
74,10
73,60
73,59
72,71
57,94
3,91
3,90
Pro
ced
ure
s
15,0%10,0%5,0%0,0%
PercentAfterBefore

Results - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Procedures - Obstetrics
Procedures where differences were found
75.35 - Other diagnostic procedures on fetus and amnion99.18 - Injection or infusion of electrolytes73.59 - Other manually assisted delivery90.59 - Microscopic examination of blood88.78 - Diagnostic ultrasound of gravis uterus73.6 - Episiotomy75.34 -Fetal monitoring, not otherwise specified99.29 - Injection or infusion of other therapeutic or prophylactic substance72.71 -Vacuum extraction with episiotomy93.57 - Aplication of other wound dressing
others
99,29
99,21
99,18
93,57
90,59
88,78
75,35
75,34
74,10
73,60
73,59
72,71
57,94
3,91
3,90
Pro
ced
ure
s
15,0%10,0%5,0%0,0%
PercentAfterBefore

Results - Pneumology department
Paper Based vs Electronic Based Clinical Records
General (differences were found)
Diagnosis - Pneumology
Pearson Chi-Square26,081(a) 15 ,037
Likelihood Ratio26,158 15 ,036
Linear-by-Linear Association 2,551 1 ,110
N of Valid Cases4564
Value dfAsymp. Sig.
(2-sided)
a 0 cells (,0%) have expected count less than 5. The minimum expected count is 24,67.
others
786,30
519,80
512,80
511,90
491,21
486,00
428,00
401,90
305,10
285,90
250,00
198,30
162,90
162,30
V15.82
Dia
gn
osi
s
80,0%60,0%40,0%20,0%0,0%
PercentAfterBefore
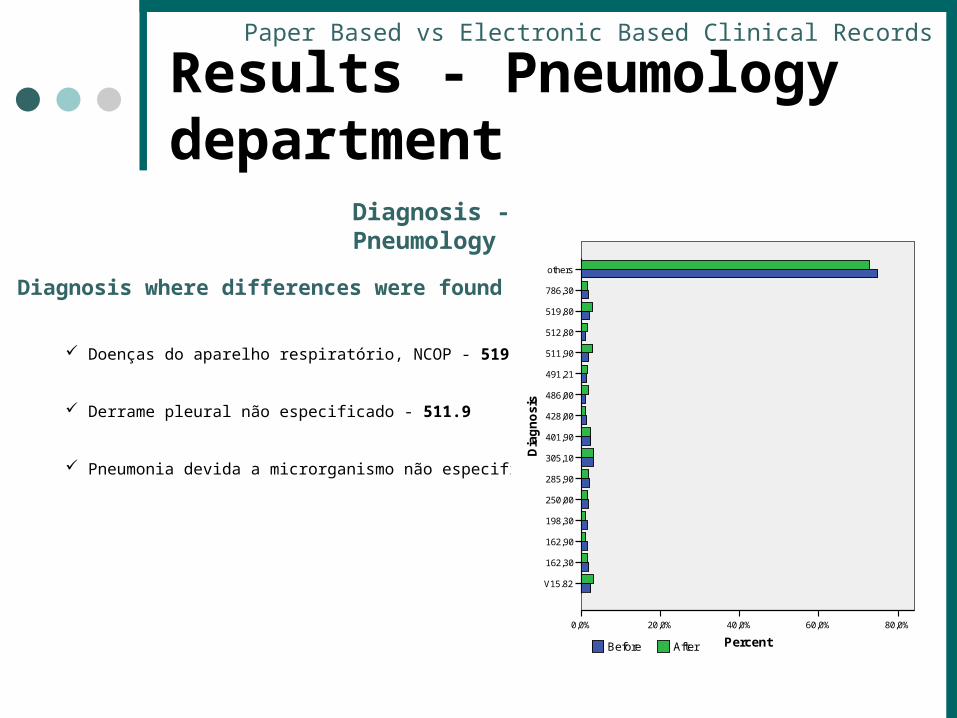
Results - Pneumology department
Paper Based vs Electronic Based Clinical Records
Diagnosis - Pneumology
Diagnosis where differences were found
Doenças do aparelho respiratório, NCOP - 519.8
Derrame pleural não especificado - 511.9
Pneumonia devida a microrganismo não especificado - 486
others
786,30
519,80
512,80
511,90
491,21
486,00
428,00
401,90
305,10
285,90
250,00
198,30
162,90
162,30
V15.82
Dia
gn
osi
s
80,0%60,0%40,0%20,0%0,0%
PercentAfterBefore

Results - Pneumology department
Paper Based vs Electronic Based Clinical Records
Procedures - Pneumology
General (differences were found)
Pearson Chi-Square23,089(a) 15 ,082
Likelihood Ratio23,157 15 ,081
Linear-by-Linear Association 1,181 1 ,277
N of Valid Cases5235
Value dfAsymp. Sig.
(2-sided)
a 0 cells (,0%) have expected count less than 5. The minimum expected count is 44,60.
others
99,29
99,23
99,21
99,19
99,18
93,96
93,94
90,59
89,65
89,52
87,49
87,44
87,41
34,91
34,04
Pro
ced
ure
s
30,0%20,0%10,0%0,0%
PercentAfterBefore

Results - Pneumology department
Paper Based vs Electronic Based Clinical Records
Procedures - Pneumology
Procedures where differences were found
Injecção ou infusão de electrolitos - 99.18
others
99,29
99,23
99,21
99,19
99,18
93,96
93,94
90,59
89,65
89,52
87,49
87,44
87,41
34,91
34,04
Pro
ced
ure
s
30,0%20,0%10,0%0,0%
PercentAfterBefore

Diagnosis where differences were found
Admissão para esterilização - V25.2
História de parto por cesariana, parto referenciado, c/ ou s/ condição anteparto - 654.21
Laceração períneo do primeiro grau - 664.01
Inércia uterina secundária - 661.11
Anemia complicando um parto referenciado, com ou sem menção de condição anteparto - 648.21
Isoimunização Rh condição anteparto com parto referenciado - 656.11
Discussion - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Diagnosis - Obstetrics The increase in the number of cases, may possibly be justified by the attempt to reduce the practise of episiotomy.

Discussion - Obstetrics department
Paper Based vs Electronic Based Clinical Records
Procedures - Obstetrics
Procedures where differences were found
Actos de diagnóstico no feto e âmnio NCOP - 75.35
Parto manual assistido, não classificável em outra parte - 73.59
Exame microscópico NCOP do sangue - 90.59
Ultra - 88.78
Episiotomia - 73.6
Monitorização fetal NCOP - 75.34 (*)
Extracção por ventosa com episiotomia - 72.71
Injecção ou infusão de electrolitos - 99.18
Injecção ou infusão de substancia terapêutica - 99.29
Aplicação de outros pensos para feridas - 93.57
the increase of the registration of this procedures contradicts the increase of the diagnose 664.01 (Laceração do perínio do primeiro grau). We found no explanation for this fact.
it increased because it became indispensable in every case of non tranquilizer fetal state.
Large increase of cases. There are two possible reasons: more available devices; and the existence of a phd theses in course, related to the decrease of the cesarians by non tranquilizer fetal state.
The decrease of this three procedures are the result of an intentional reduction of the registration of this kind of methods, because they are a kind of procedure that is done in almost every treatment and it not necessary neither useful to keep this type of information.

Discussion - Pneumology department
Paper Based vs Electronic Based Clinical Records
Diagnosis - Pneumology
Diagnosis where differences were found
Doenças do aparelho respiratório, NCOP - 519.8
Derrame pleural não especificado - 511.9
Pneumonia devida a microrganismo não especificado - 486
The increase of this diagnoses is related to the management of the distribution of the patients between departments. The patients were usually randomly distributed between the internal medicine and the pneumology departments. But recently, the pneumology department is taking care of the delicated cases, like the ones above, which justifies the difference found.

Discussion – Pneumology department
Paper Based vs Electronic Based Clinical Records
Procedures - Pneumology
Procedures where differences were found
Injecção ou infusão de electrolitos - 99.18
The decrease of this procedure is the result of an intentional reduction of the registration of this kind of methods, because they are a kind of procedure that is done in almost every treatment and it not necessary neither useful to keep this type of information.

Diagnosis/Procedures Code Increase/ Decrease %
Diagnosis Obstetrics
Request for sterillization V25.2 Decrease -64,29%
Previous cesarean section 654.21 Decrease -48,28%
First-degree perineal laceration 664.01 Increase84,6
2%
Secondary uterine inertia 661.11 Decrease -88,89%
Anemia 648.21 Decrease -50,00%
Rhesus isoimmunization 656.11 Increase 14,06%
Procedures Obstetrics
Other diagnostic procedures on fetus and amnion75.35 Increase
48,19%
Other manually assisted delivery 73.59 Increase 43,06%
Microscopic examination of blood 90.59 Increase
35,59%
Diagnostic ultrasound of gravis uterus 88.78 Increase 42,31%
Episiotomy 73.6 Increase25,4
2%
Fetal monitoring, not otherwise specified 75.34 Increase 21,43%
Vacuum extraction with episiotomy 72.71 Increase 37,93%
Injection or infusion of electrolytes 99.18 Decrease -73,68%
Injection or infusion of other therapeutic or prophylactic substance 99.29 Decrease -53,62%
Aplication of other wound dressing 93.57 Decrease
-96,43%
Diagnosis Pneumology
Other diseases of respiratory system, not elsewhere classified 519.8 Increase
47,37%
Unspecified pleural effusion 511.9 Increase 55,56%
Pneumonia, organism unspecified 486 Increase 88,89%
Procedures Pneumology
Injection or infusion of electrolytes 99.18 Decrease -34,29%

AknowledgmentsWe would like to thank the professors Ricardo Correia,
Cristina Santos and Clara Tavares, without whose helpwe would not be able to finish our work.
We are also grateful to Dr. Fernando Lopes,responsible EPR codification, Dra. Ana Rosa and Dra.Raquel Mota, from the obstetrics department, and finally Dr. Agostinho Marques, from the pneumology department.
Finally, we would like to thank to Professor Altamiro,for his precious help and guidance throughout the year.
Paper Based vs Electronic Based Clinical Records