Embed Size (px)
Citation preview

Panel Discussion
•Case Presentation and Panel Discussion
•A 33 years old man referred to GI clinic with chief complaint of malaise, lassitude, anorexia, nausea, yellow sclera and abdominal discomfort for 2 weeks.
•No history of liver disease in family members, no history of regular drug use
•Positive history of alcohol ingestion
Presentation of a Case with Alcoholic Liver Disease• Physical examination
• Normal vital signs, no fever
• Yellowish discoloration of skin and sclera
• Mild liver enlargement
• Suspected spleen enlargement
• No ascites
• No encephalopathy
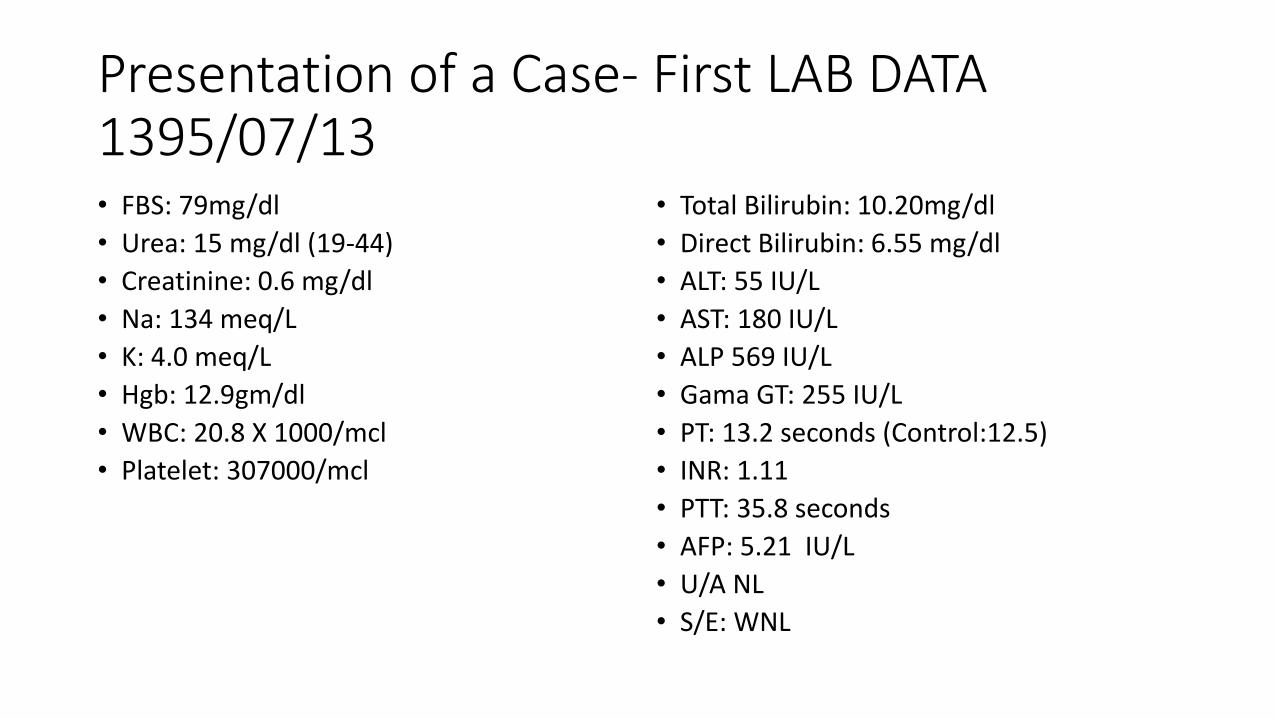
Presentation of a Case- First LAB DATA 1395/07/13 • FBS: 79mg/dl
• Urea: 15 mg/dl (19-44)
• Creatinine: 0.6 mg/dl
• Na: 134 meq/L
• K: 4.0 meq/L
• Hgb: 12.9gm/dl
• WBC: 20.8 X 1000/mcl
• Platelet: 307000/mcl
• Total Bilirubin: 10.20mg/dl
• Direct Bilirubin: 6.55 mg/dl
• ALT: 55 IU/L
• AST: 180 IU/L
• ALP 569 IU/L
• Gama GT: 255 IU/L
• PT: 13.2 seconds (Control:12.5)
• INR: 1.11
• PTT: 35.8 seconds
• AFP: 5.21 IU/L
• U/A NL
• S/E: WNL
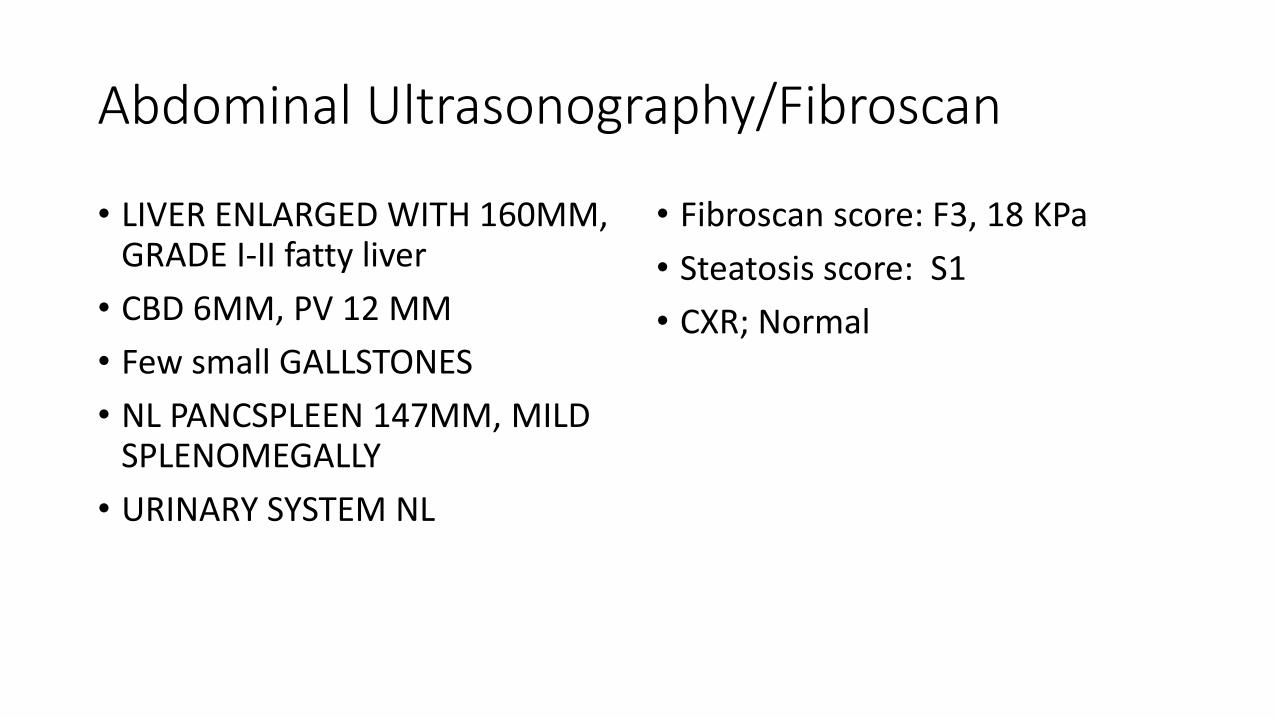
Abdominal Ultrasonography/Fibroscan
• LIVER ENLARGED WITH 160MM, GRADE I-II fatty liver
• CBD 6MM, PV 12 MM
• Few small GALLSTONES
• NL PANCSPLEEN 147MM, MILD SPLENOMEGALLY
• URINARY SYSTEM NL
• Fibroscan score: F3, 18 KPa
• Steatosis score: S1
• CXR; Normal
Questions
•1 - How do you evaluate this patient?
•2- How do you complete the information about history of alcohol ingestion?
•3- What is the value of GGT for diagnosis of alcohol abuse?

The CAGE Questionnaire
• 1. Have you ever felt you should cut down on your drinking?
• 2. Have people annoyed you by criticizing your drinking?
• 3. Have you ever felt bad or guilty about your drinking?
• 4. Have you ever had a drink first thing in the morning to steady your nerves or to get rid of a hangover (eye-opener)?
Scoring: Each response is scored as 0 or 1, with a higher
score indicative of alcohol-related problems, and a total of
2 or more clinically significant.
HEPATOLOGY, Vol. 51, No. 1, 2010
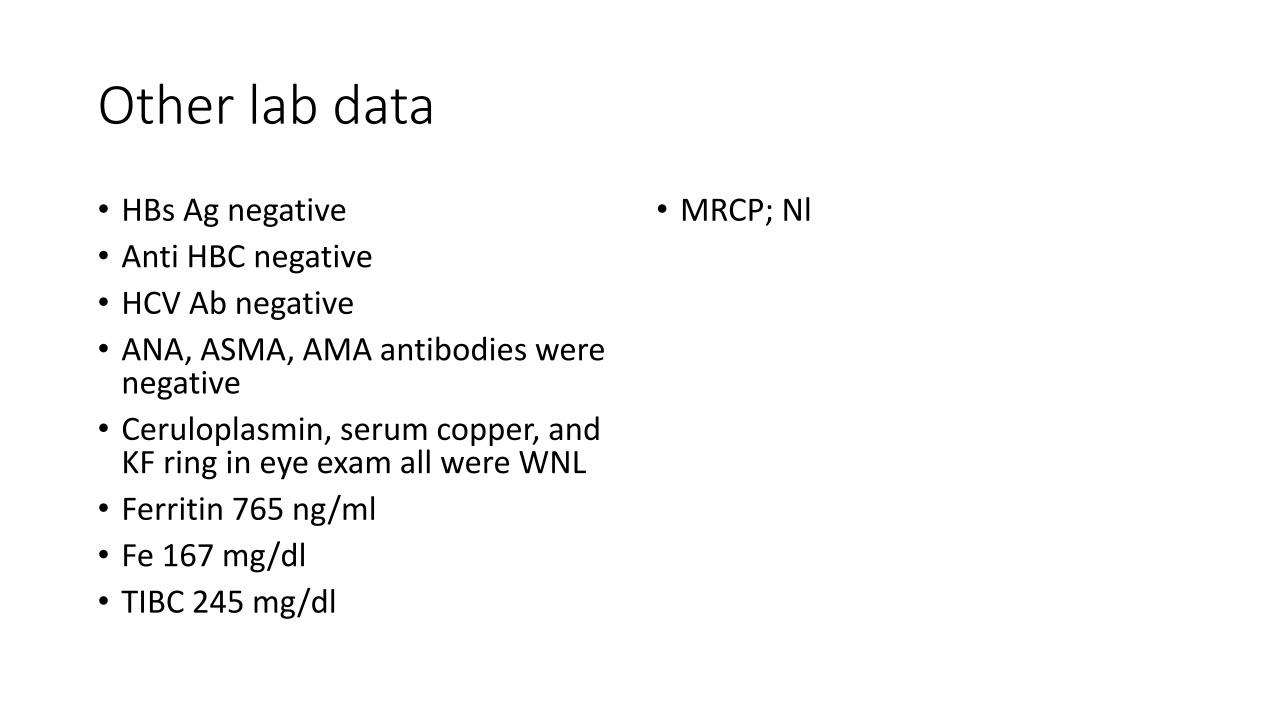
Other lab data
• HBs Ag negative
• Anti HBC negative
• HCV Ab negative
• ANA, ASMA, AMA antibodies were negative
• Ceruloplasmin, serum copper, and KF ring in eye exam all were WNL
• Ferritin 765 ng/ml
• Fe 167 mg/dl
• TIBC 245 mg/dl
• MRCP; Nl

• Positive history of daily and regular use of alcoholic beverages for more than 1 year.
• Daily intake of alcohol was about 200-300 cc alcoholic beverages.
• The used beverages have had 40-50% ethanol
Question
•3- How much alcohol intake could be harmful?
•4- How do you classify the amount of alcohol ingestion in clinical practice?

Levels of Chronic Alcohol Use
• Moderate drinkers: up to 2 drinks/day (men) or 1 drink/day (women) Do not disclose increased risk of organ damage compared to abstainers
• High-risk drinking: 4 or more drinks on any day or 8 or more drinks per week for women and 5 or more drinks on any day or 15 or more drinks per week for men.
• Binge drinking is the consumption within about 2 hours of 4 or more drinks for women and 5 or more drinks for men.
The National Institute on Alcohol Abuse and Alcoholism (NIAAA)
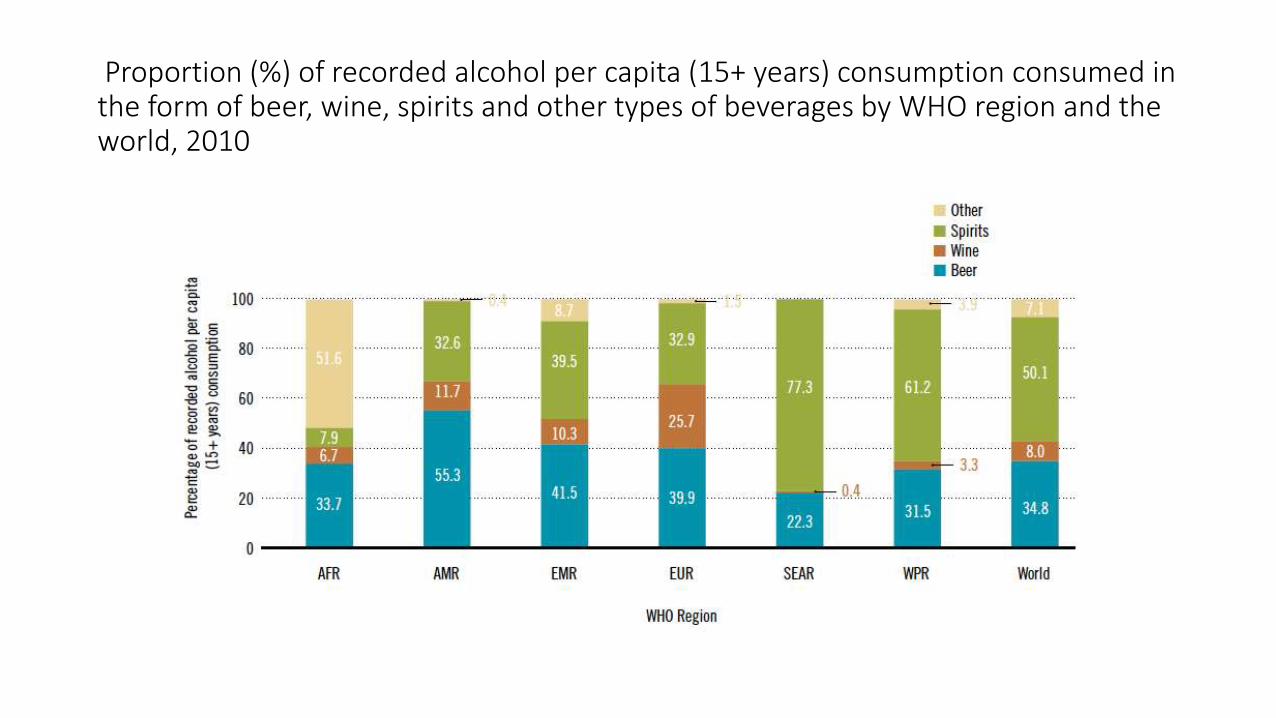
Proportion (%) of recorded alcohol per capita (15+ years) consumption consumed in the form of beer, wine, spirits and other types of beverages by WHO region and the world, 2010

National Institute on Alcohol Abuse and Alcoholism;What Is A Standard Drink?
In the United States, one "standard" drink contains roughly 14 grams of pure alcohol, which is found in: 12 ounces (354cc) of regular beer, 5 ounces (147cc) of wine, 1.5 ounces (44cc) of distilled spirits

Types and Levels of Chronic Alcohol Drinking
Type Men Women
Moderate < 2 drinks/day < 1 drink/day
High Risk ≥ 5 drinks/day ≥ 15 drinks/week
≥ 4 drinks/day≥ 8 drinks/week
Binge drinking
≥ 5 drinks/ 2 hours ≥ 4 drinks/ 2 hours
The National Institute on Alcohol Abuse and Alcoholism (NIAAA)

Question
•5- What risk factors are important for harmful effects of alcohol intake?

Conceptual causal model of alcohol consumption and health outcomes
Possible risk Factors for development of ALD
• Level of alcohol consumption• Dose, Duration, Type of alcohol, Drinking patterns
•Diet
•Gender & Ethnicity
•Genetic factors
•Other risk factors• Obesity, Iron overload, Concomitant viral hepatitis
Pathways of Alcohol-related Harm • Volume of alcohol consumed (Dose–response relationship)
• For all alcohol-attributable cancers, the higher the consumption of alcohol, the larger the risk for these cancers (IARC, 2010; Shield et al., 2013).
• Pattern of drinking• Less harm with the same pattern of drinking while eating (Trevisan et al.,
2001; Stranges, 2004)
• Heavy episodic drinking disappears the cardioprotective effect of low- dose alcohol consumption (Roerecke & Rehm, 2010; 2013).
• Quality of alcohol consumed • Illegal production, with methanol or other toxic substances (Rehm, Kanteres
& Lachenmeier, 2010).
• Illegal, lower cost preparation linked to heavy drinking occasions (Rehm et al., 2014).
Factors associated with Higher Mortality in Chronic Alcoholic Cirrhosis
• Higher consumption of pork meat (high in linoleic acid)
• Higher consumption of unsaturated fats
• Lower consumption of carbohydrate
• More in obese
• More in hyperglycaemia
Naveau S , Giraud V , Borotto E et al . Excess weight risk factor for alcoholic liver disease . Hepatology 1997 ; 25 : 108 – 111 .Raynard B , Balian A , Fallik D et al . Risk factors of fi brosis in alcohol - induced liver disease . Hepatology 2002 ; 35 : 635 – 638 .

A Question
• A- 2, 4, 3, 1
• B- 2, 3, 4, 1
• C- 3, 2, 4, 1
• D- 4, 3, 2, 1
What was found to be the order of prevalence, from highest to lowest, of fatty liver disease among the following groups?
1- Normal weight and non/moderate drinker
2- Obese and heavy drinker
3- Obese and non/moderate drinker
4- Normal weight and heavy drinker
Alcohol-attributable deaths (in thousands) by sex and cause of death in 2004

Question
• Regarding the patient which presented;
• What is your diagnosis?
• Do you suggest another workup?
• Do you suggest liver biopsy for patient?
AASLD PRACTICE GUIDELINESAlcoholic Liver Disease; 2010• Recommendation:
• 1. Clinicians should discuss alcohol use with patients, and any suspicion of possible abuse or excess should prompt use of a structured questionnaire and
• further evaluation (Class I, level C).
• 2. For patients with a history of alcohol abuse or excess and evidence of liver disease, further laboratory tests should be done to exclude other etiologies and to confirm the diagnosis (Class I, level C).
• 3. Patients with ALD and suggestive symptoms should be screened for evidence of other end-organ damage, as appropriate (Class I, level C).
• 4. For patients with a clinical diagnosis of severe AH for whom medical treatment is contemplated, or for those in whom reasonable uncertainty exists regarding the underlying diagnosis, a liver biopsy should be considered. This decision will depend on local expertise and ability in performing a liver biopsy in patients with coagulopathy, the patient’s severity of illness, and the type of therapy under consideration (Class I, level C).

Question
• With diagnosis of acute alcoholic hepatitis on the clinical and lab findings
• How do you assess the severity of acute liver disease ?
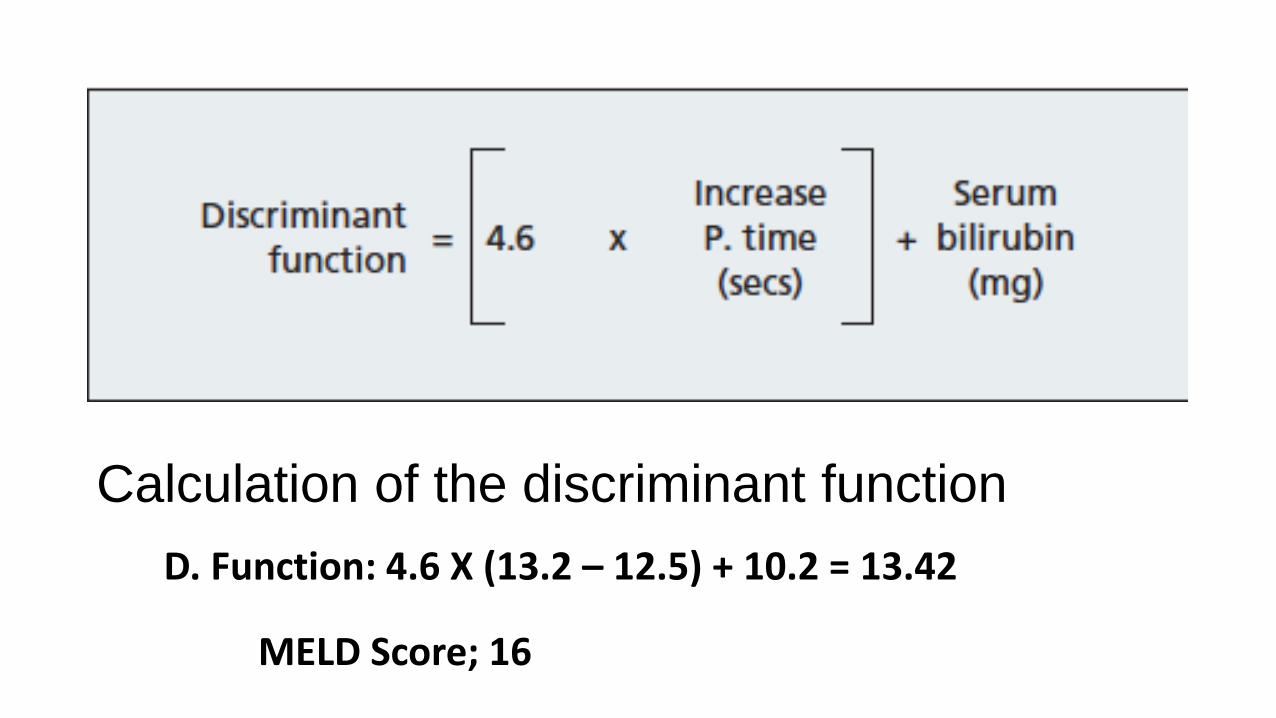
Calculation of the discriminant function
D. Function: 4.6 X (13.2 – 12.5) + 10.2 = 13.42
MELD Score; 16
Question
• How do you manage this patient?
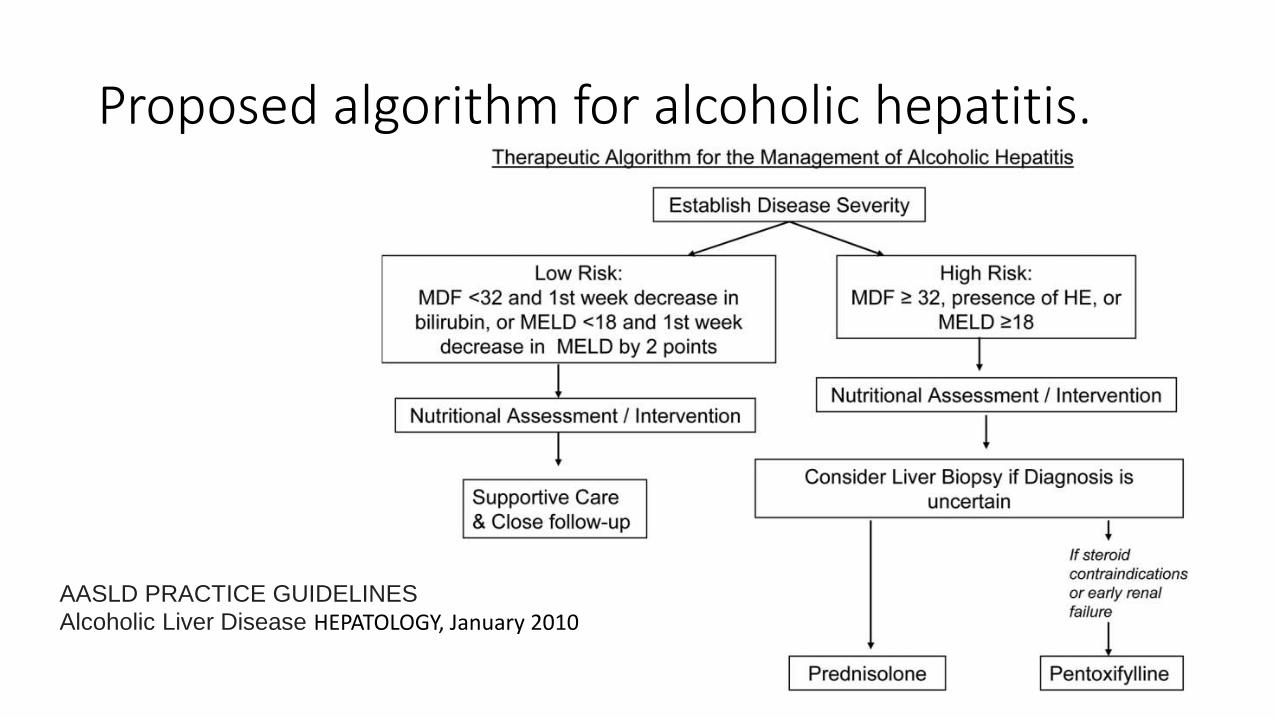
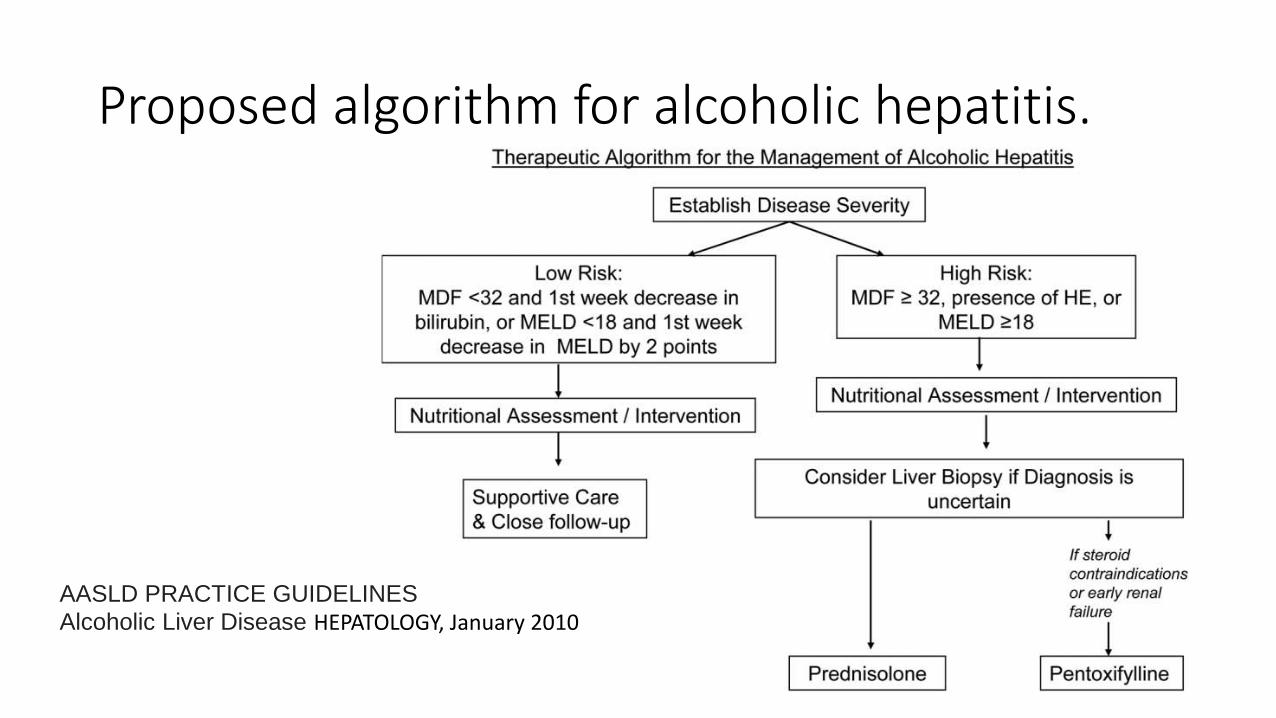
Proposed algorithm for alcoholic hepatitis.
AASLD PRACTICE GUIDELINES
Alcoholic Liver Disease HEPATOLOGY, January 2010
AASLD PRACTICE GUIDELINESAlcoholic Liver Disease; 2010• Recommendations:
• 6. In patients with evidence of alcohol-induced liver disease, strict abstinence must be recommended, because continued alcohol use is associated with disease progression (Class I, level B).
• 7. Naltrexone or acamprosate may be considered in combination with counseling to decrease the likelihood of relapse in patients with alcohol abuse/dependence in those who achieve abstinence (Class I, level A).
Presentation of a Case
• For patient abstinence from alcohol was advised and put on vitamin B1 300mg per day, multivitamin tablets three per day, Livergol, and lactulose was started. He suggested to be in close follow up and re-checking of LFT 1 week later.
• After 1 week the patient’s symptoms were not changed except some irritability
• You see the lab data in the next slide:

Presentation of a Case- Second LAB DATAat 1395/07/20 • FBS: 85 mg/dl
• Urea: 18 mg/dl (19-44)
• Creatinine: 1.0 mg/dl
• Na: 135 meq/L
• K: 4.0 meq/L
• Hgb: 12.9 gm/dl
• WBC: 19.8 X 1000/mcl
• Platelet: 307000/mcl
• Total Bilirubin: 12.10 mg/dl
• Direct Bilirubin: 9.55 mg/dl
• ALT: 85 IU/L
• AST: 190IU/L
• ALP 545 IU/L
• PT: 17.2 seconds (Control:12.5)
• INR: 1.7
• PTT: 35.8 seconds
Question
• What is your suggestion?
• Do you suggest steroids for him?
Proposed algorithm for alcoholic hepatitis.
AASLD PRACTICE GUIDELINES
Alcoholic Liver Disease HEPATOLOGY, January 2010

Calculation of the discriminant function
Discriminant function= 4.6 X (17.2 – 12.5 seconds) + 12.10 = 33.72
MELD Score: 22
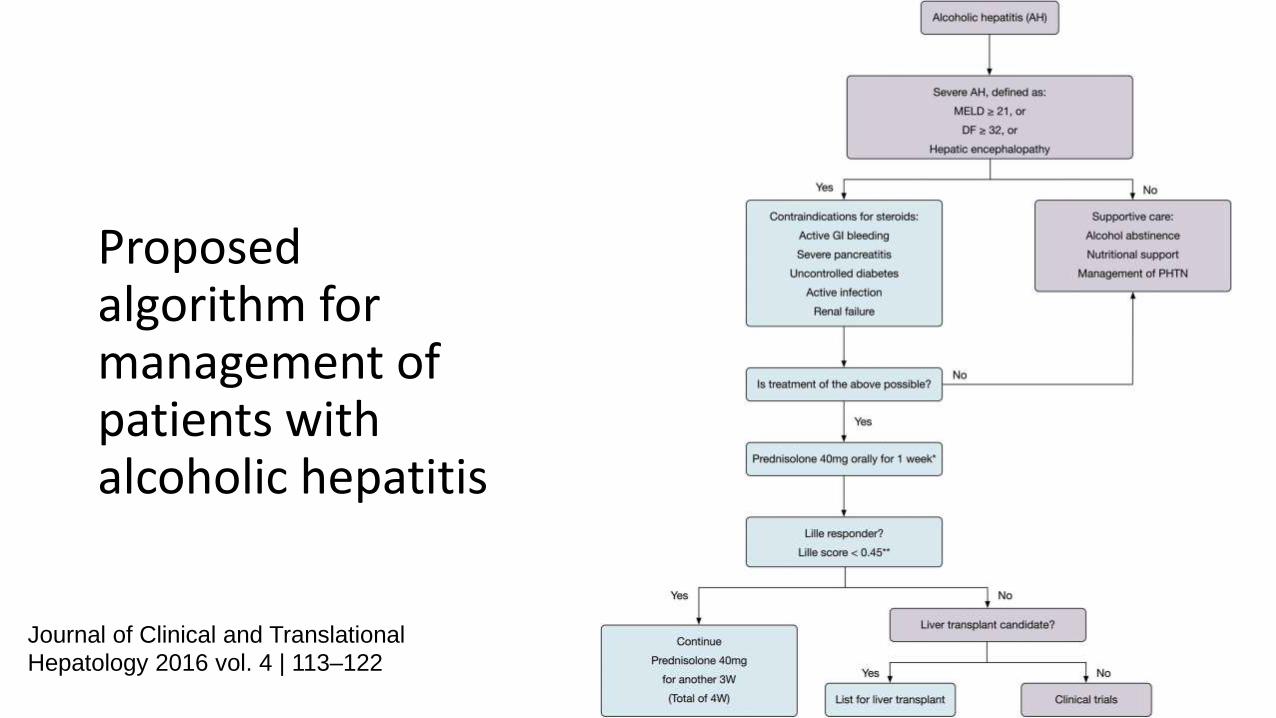
Proposed algorithm for management of patients with alcoholic hepatitis
Journal of Clinical and Translational
Hepatology 2016 vol. 4 | 113–122
Effects of Corticosteroids in Acute Alcoholic Hepatitis
• Only in patients with severe AH (defined as DF $ 32, or MELD $ 21, or presence of hepatic encephalopathy) and no contraindications is advised
• Reducing pro-inflammatory cytokines such as tumor necrosis factor (TNF)-a, and increasing anti-inflammatory cytokines such as interleukin 10.
Taieb J, Mathurin P, Elbim C, Cluzel P, Arce-Vicioso M, Bernard B, et al. Blood neutrophil functions and cytokine release in severe alcoholic hepatitis: effect of corticosteroids. J Hepatol 2000;32:579–586. doi: 10.1016/ S0168-8278(00)80219-6

Data from clinical trials and meta-analysesof corticosteroids in AH have been conflicting• A recent Cochrane meta-analysis concluded that, overall, there is no
clear evidence that steroids are effective in the management of AH.
• However, this meta-analysis concluded that corticosteroids did significantly reduce mortality in the subgroup of trials with patients with a Maddrey score of 32 or higher or in patients who had hepatic encephalopathy.
• In addition, this study showed that steroids reduced mortality in low bias-risk studies.
Corticosteroids for Acute Alcoholic Hepatitis
• Mathurin et al. analyzed individual data from five randomized controlled trials and showed that steroids have survival advantage for severe AH (defined as DF $ 32 or hepatic encephalopathy), with a 28 day survival of 85% among treated patients compared to 65% for patients receiving placebo (p = 0.001).
• Prednisolone 40 mg for a total of 4 weeks (28 days) or other regimens have been used in the trials. Prednisolone is preferred (but not demonstrated to be better) over prednisone, as the latter requires conversion within the liver to its active form, prednisolone.
Singal AK, Walia I, Singal A, Soloway RD. Corticosteroids and pentoxifylline for the treatment of alcoholic hepatitis:
Current status. World J Hepatol 2011;3:205–210. doi: 10.4254/wjh.v3.i8.205
Treatment of AH
• Alcoholic abstinence and supportive care• Alcohol abstinence is the most important predictor for determining long-term
survival in patients with AH. • In the study by Potts et al., 5 year survival was significantly higher in AH patients who
remained abstinent compared to those AH patients who relapsed or continued to drink (75%vs. 27% and 21%, respectively, p = 0.005).33
• Nutritional support• Management of complications of portal hypertension• Medical therapy
• Corticosteroids• Pentoxifylline; is a phosphodiesterase inhibitor and a possible TNF-a inhibitor• Anti TNF agents; Infiliximab• N- acetyl cysteine
Contraindications for Steroids
• Renal failure
• Active gastrointestinal bleeding
• Uncontrolled hyperglycemia
• Acute pancreatitis
• Psychosis
• Infection

• Oral prednisolone 50 mg/day was added to previous drugs and insisted on continuation of abstinence. Anxiolytics was suggested for his irritability.
Lab data at 1395 08 15
FBS: 94 mg/dl
CREAT: 0.8 mg/dl
CHOLEST 310 mg/dl
LDL 242 mg/dl
U ACID 3.7 mg/dl
TB 2.9 mg/dl
DB 1.9 mg/dl
AST 177 IU/L
ALT 195 IU/L
• 1- What is your decision?• A- Continue prednisolone indefinitely
• B- Discontinue prednisolone and starting Pentoxifylline (PTX)
• C- Adding Pentoxifylline (PTX) to steroids
• D- Discontinue all medications and staring atorvastatin and azathiorpine
• 2- How do you assess the steroid response?
• 3- Do you suggest another treatments?

LAB DATA AT 17/12/1395
• CREAT 1.0 • TB 1.5• DB 0.6• ALT 47• AST 66• ALP 264• GGT 129.9
• PT 13.5• INR 1.1• ALB 4.5• TP 8.1
The alcohol use was discontinued. Pentoxifylline was added to his treatment and the prednisolone was tapered after 2 months, and Pentoxifylline was continued.
How do you follow the patient?

• Questions
• Other comments?