Embed Size (px)
Citation preview

SSAT PLENARY
Pancreatic Morphological Changes in Long-Term Follow-Upafter Initial Episode of Acute Alcoholic Pancreatitis
Jussi Nikkola & Irina Rinta-Kiikka & Sari Räty & Johanna Laukkarinen &
Riitta Lappalainen-Lehto & Satu Järvinen & Hanna Seppänen &
Isto Nordback & Juhani Sand
Received: 14 May 2013 /Accepted: 24 June 2013 /Published online: 4 September 2013# 2013 The Society for Surgery of the Alimentary Tract
AbstractObjective The long-term morphological changes induced by a single episode of alcoholic pancreatitis are not known. Our aimwas to study these morphological changes in secretin-stimulated magnetic resonance cholangiopancreatography (S-MRCP)after the first episode of alcohol-associated acute pancreatitis and to evaluate the risk factors and possible protective factorspotentially associated with later chronic findings. We have previously reported 2-year follow-up results in pancreaticmorphology. This study extends the follow-up to 9 years.Patients and Methods In this prospective follow-up study, S-MRCP imaging was performed for 44 (41 M, 3 F; mean age, 46(25–68)years) patients after their first episode of alcohol-associated pancreatitis. Pancreatic morphology was evaluated at3 months and at 2, 7, and 9 years after hospitalization. Recurrent attacks of pancreatitis were studied and pancreatic functionwas monitored by laboratory tests. Patients’ alcohol consumption was evaluated with questionnaires, laboratory markers, andself-estimated alcohol consumption via interview. Smoking and body mass index were annually recorded.Results At 3 months, 32 % of the patients had normal findings in S-MRCP, 52 % had acute, and 16 % had chronic changes. At7 years, S-MRCP was performed on 36 patients with normal findings in 53 %, the rest (47 %) having chronic findings.Pancreatic cyst was present in 36 %, parenchymal changes in 28 %, and atrophy in 28 % of the cases. There were no newchanges in the pancreas in the attending patients between 7 and 9 years (18 patients). Of the patients with only acute findings at3 months, 60 % resolved to normal in 7 years, but the rest (40 %) showed chronic changes later on. The initial attack was mildin 65 %, moderate in 25 %, and severe in 10 % of the patients. Patients with mild first attack had fewer chronic changes at7 years compared to patients with moderate or moderate and severe together (p=0.03, p=0.01). Of the patients in the seventhyear of S-MRCP, 22 % had suffered a recurrent episode of acute pancreatitis (mean, 22 (2–60)months) and 11 % had a clinicaldiagnosis of chronic pancreatitis. At 7 years, 88 % of the patients with recurrences had chronic findings in S-MRCP versus36 %with nonrecurrent pancreatitis (p=0.02). Six (17 %) patients abstained from alcohol throughout follow-up (mean, 8.7 (7–9.1)years), but even one of these developed pancreatic atrophy. Out of the non-abstinent patients who did not sufferrecurrences, 4/22 (18 %) had developed new findings during at follow-up S-MRCP (NS). In univariate analysis, heavysmoking showed no correlation with increased chronic changes compared to nonsmoking.
This study has been selected for the following plenary sessions:21.11.2012 Operatiiviset päivät 2012 (National Surgical Meeting),Helsinki, Finland. 19.5.2013 Digestive Disease Week 2013, Orlando,FL, USA
J. Nikkola : S. Räty : J. Laukkarinen : I. Nordback : J. SandSchool of Medicine, University of Tampere,Tampere, Finland
I. Rinta-KiikkaDepartment of Radiology, Tampere University Hospital,Tampere, Finland
S. Räty : J. Laukkarinen :R. Lappalainen-Lehto : S. Järvinen :H. Seppänen : I. Nordback : J. SandDepartment of Gastroenterology and Alimentary Tract Surgery,Tampere University Hospital, Tampere, Finland
J. Sand (*)Division of Surgery, Gastroenterology and Oncology, TampereUniversity Hospital, Teiskontie 35, 33521 Tampere, Finlande-mail: [email protected]
J Gastrointest Surg (2014) 18:164–171DOI 10.1007/s11605-013-2279-1

Conclusions Morphological pancreatic changes increase with recurrent episodes of acute pancreatitis. Patients with mild firstattack have fewer chronic changes in the pancreas in the long term. However, even a single episode of acute alcoholicpancreatitis may induce chronic morphological changes in long-term follow-up.
Keywords Acute pancreatitis . Alcohol . Recurrentpancreatitis . Pancreatic imaging . Magnetic resonanceimaging
Introduction
The pathogenesis of acute pancreatitis (AP) is not complete-ly understood but premature activation of trypsinogen insidethe acinar cells is the main trigger of autodigestion cascade.1
Gallstones and alcohol are the two main etiological factors,with alcohol the main etiology in recurring and chronicpancreatitis.2,3 The main etiology varies between countriesas does the incidence of AP.4 Alcoholic AP is more commonamong men than women with a peak incidence in the agegroup 35–44 years.5 Heavy alcohol consumption is the mostimportant risk factor6 and a threshold level of four drinks perday has been reported in meta-analysis.7 A minority (5–10 %)of heavy alcohol users, however, develop acute alcoholicpancreatitis. In most cases, the inflammation is mild andself-limiting, but 20 % develop a severe attack in which themortality rate is much higher due to complications from thesystemic inflammatory reaction.8
About half of the patients suffer recurrent attacks in long-term follow-ups and as many as 80 % of recurrences occurduring the first 3 years after the initial attack.9 Persistent alcoholconsumption after the first attack is a major risk factor forrecurrences and development of chronic pancreatitis (CP),10,11
and abstinence has been found to protect against recurrencesand new-onset diabetes even in the long term.12 Mild firstepisode and young age (<45) at the time of the first attack arealso risk factors for recurrences.9 Smoking is a known riskfactor for acute, recurrent, and chronic pancreatitis.2,13
According to current knowledge, recurring episodes ofacute pancreatitis cause tissue damage in the pancreas, whicheventually leads to CP.1 About 15 % of patients with APdevelop CP11 which manifests as pancreatic exocrine andendocrine dysfunction leading to new-onset diabetes andcausing chronic pain.14,15 Genetic predisposition seems tobe linked to increased risk to develop recurrent or chronicpancreatitis. SPINK1, PRSS1, PRSS2, and CFTR are themost-studied loci and recently CLDN2 mutation has beensuggested to accelerate the transition from recurrent pancre-atitis to CP.16 SPINK1 N34S mutation has also been found tobe more common in patients with acute pancreatitis.17
During convalescence (3–6 months after the initial attack),29 % of patients have been reported to have acute changes inthe pancreas (edema) in magnetic resonance imaging (MRI)while 20 % of patients already have chronic changes. Half of
the patients with acute changes in the pancreas have beenreported to have normal findings at 2 years. In former imagingstudies, persistent pseudocysts have been found to be anindependent risk factor for recurrences.18
It still remains debatable whether the gland healscompletely after the first episode of alcoholic pancreatitis.There is a wide range of studies reporting short-term resultsin acute pancreatitis and also of studies on pancreatic mor-phology after severe acute pancreatitis. However, long-termprospective follow-up studies after the initial episode arerare. The aim of this study was to evaluate the course ofpancreatitis in long-term follow-up in patients suffering theirinitial episode of alcoholic pancreatitis focusing on pancre-atic morphology in MRI. We also aimed to evaluate the riskfactors and possible protective factors potentially associatedwith later chronic findings.
Material and Methods
From December 2001 to April 2005, 120 patients diag-nosed with their first acute alcohol-associated pancreati-tis were recruited for a randomized intervention study19
(ClinicalTrials.gov Identifier: NCT00534534). The samepatients were also asked to take part in a long-termprospective secretin-stimulated magnetic resonancecholangiopancreatography (S-MRCP) follow-up study.Two-year follow-up results have previously been reported18
and the present study focuses on the long-term follow-up.Forty-four (41 M, 3 F; mean age, 46 (25–68)years) of thepatients took part in the follow-up. Pancreatic morphologywas evaluated at 3 months, and at 2, 7, and 9 years afterhospitalization. We selected these time points to get longenough yet realistic follow-up to be able to clarify the impactof subsequent events after initial AP to pancreatic morpholo-gy. Patients were prospectively followed-up for recurrencesand patients’ pancreatic function was monitored by laboratorytests. Alcohol consumption was evaluated with question-naires, laboratory markers, and self-estimated alcohol con-sumption via interview. The criterion for abstinence wasself-reported alcohol consumption less than 24 g per 2months,which is in line with the Alcohol Use Disorders IdentificationTest (AUDIT) and Short Alcohol Dependence Data Question-naire (SADD) questionnaires and laboratory markers such asCDT. Smoking and bodymass index (BMI) weremonitored atyearly intervals.
The diagnosis of acute alcoholic pancreatitis was based onthe following criteria: clinical features (epigastric pain, andvomiting), elevated pancreatic enzymes (amylase >3 times
J Gastrointest Surg (2014) 18:164–171 165

over the normal upper margin) and elevated inflammatorymarkers. When needed, CT or US was also performed toconfirm the diagnosis. Alcohol etiology was evaluated byinterview, history, and questionnaires eliciting heavy alcoholconsumption and dependence (AUDIT, SADD).20 Otheretiologies were excluded by patient history, radiologicalimaging, and laboratory tests (serum liver chemistry, lipids,and calcium). Patients with previous episodes or symptomsof pancreatitis or signs indicative of chronic pancreatitiswere excluded from the study. Updated Atlanta criteria wereused to re-evaluate the severity of pancreatitis.21 Diagnosisof chronic pancreatitis was obtained from patient files. Thisinvolved adjusting the patients’ clinical status with imagingfindings and laboratory studies measuring pancreatic function.
Morphologic changes in the pancreas were evaluatedusing S-MRCP. All images were reviewed by the sameradiologist, who was unaware of the patients’ clinical details.Changes were categorized as normal, acute (edema), orchronic (parenchymal changes, pseudocysts, atrophy, ductalchanges/abnormal secretin response, stricture). Pseudocystswere categorized as chronic changes at 3 months. Lankischet al. have reported that in 3 months after hospital discharge,acute fluid collections either disappear (76 %) or develop topseudocysts (24 %).22 Parenchymal changes were notedwhen there was a diffuse decrease in signal intensity in T1-weighted images. The pancreatic parenchyma signal wascompared to the signal of the spleen or peripheral muscles.Another criterion for parenchymal changes was the presenceof segmental dimensional changes without general paren-chymal atrophy. Changes in glandular shape were alsointerpreted as a parenchymal change.23
The MRI modality used was 1.5 T Signa Horizon (GEMedical Systems, Milwaukee, WI, USA) with a phased-array torso coil. Fat-saturated T2-weighted Fast Spin Echoand T1-weighted Spin Echo sequences were first obtained inthe axial plane to assess the position and morphology of thepancreas, followed by the heavily T2-weighted fat-saturatedSingle Shot Fast Spin Echo MRCP sequence in the coronalplane obtained radially at 15° intervals, without and repeat-edly at a 1-min intervals up to 9 min from the injection of100 IU secretinpentahydrochloride (Secrelux; SanochemiaDiagnostics, Neuss, Germany).
Statistical Analysis
Univariate analysis was performed using the chi-square test.p values <0.05 were considered statistically significant.
Ethical Aspects
The study was approved by the ethics committee of TampereUniversity Hospital (R00126). All patients approved atten-dance by providing written consent.
Results
Morphology
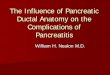
Out of the 44 patients who underwent a baseline S-MRCP,36 attended the seventh year follow-up imaging study. Atbaseline (3 months), 32 % of the patients had normal find-ings in S-MRCP, 52 % had acute (only acute or acute andchronic), and 16 % chronic changes (Table 1). At 7 years,53 % of the patients had normal pancreas while theremaining 47 % had chronic findings. The most commonchronic change at 7 years was pancreatic pseudocyst, whichwas present in 36 % of the patients with chronic changes.Atrophy was present in 28 % and other parenchymal changesin 28 % of the cases (Fig. 1). Eighteen patients took part inthe ninth year S-MRCP. There were no new changes in thepancreas among the patients attending between 7 and 9 years.Alcohol consumption and scores from AUDIT and SADDquestionnaires reported during admission due to the firstepisode are presented in Table 2 along with smoking status,BMI, and severity. Eight patients who participated thesecond-year follow-up imaging study did not want to attendto the seventh year S-MRCP.
In 45% of the patients who had acute findings at 3months,S-MRCP findings resolved to normal in 7 years, but the rest(55 %) showed chronic changes later on. The changes inpancreatic morphology during the follow-up are described inTable 3. All those patients who had both acute and chronicfindings at baseline had chronic findings at 7 years. If thepatient had chronic changes at baseline, these were alsoapparent in the later S-MRCPs. However, 9 patients out of15 (60 %) with only acute changes at baseline resolved tonormal in 7 years while 6 (40 %) developed chronic changes.
Severity
Updated Atlanta criteria20 were used to retrospectively re-evaluate the severity of the first attack. Pancreatitis wassevere in 4 out of 44 (10 %) patients, moderate in 11 out of44 (25 %) patients, and the remaining 65 % had a mild firstattack (Table 2). One of the patients with severe pancreatitis
Table 1 Prevalence of categorized S-MRCP findings in all attendingpatients
Normal (%) Onlyacute (%)
Acute andchronic (%)
Onlychronic (%)
Baseline (n=44) 32 39 14 16
2 Years (n=43) 53 0 7a 40
7 Years (n=36) 53 0 0 47
a One patient had a recurrent attack and another had liver disease at thistime point
166 J Gastrointest Surg (2014) 18:164–171
developed multi-organ failure. All four patients with severepancreatitis were treated in an intensive care unit for a meanof 17 (4–26)days. Among the 36 patients in the long-termfollow-up, four patients (11 %) had severe, seven (19 %)moderate, and the rest 25 (69 %) had mild initial attack. Noneof the patients was operated on for pancreatitis.
Three out of four patients (75 %) with severe first attackhad chronic changes at 2 and 7 years. Six out of sevenpatients (86 %) with moderate first attack had chronicchanges at 7 years. Patients with mild pancreatitis had fewerchronic changes at 7 years (8/25, 32 %) than did patients whoinitially had moderate (p=0.03) or moderate or severe pan-creatitis (p=0.01; Table 4).
Recurrent Attacks
Eight out of the 36 (22 %) patients who attended the seventhyear S-MRCP had suffered a recurrent episode of acute pan-creatitis (mean, 22 (2–60)months) and four of these patients(11 %) had had a clinical diagnosis of chronic pancreatitis. At
7 years, 88 % (7 out of 8) of patients with recurrences hadchronic findings in S-MRCP versus 36 % (10 out of 28) withnonrecurrent pancreatitis (p=0.02; Table 4).
Alcohol Consumption
Overall 7 out of 36 (19 %) patients presented with newchronic findings after 2 years. Six (17 %) patients maintainedabstinence through the follow-up (mean, 8.7 (7–9.1)years).One of these developed pancreatic atrophy at age 63 but theothers had normal pancreas. Out of the non-abstinent pa-tients with no recurrences, 4/22 (18 %) developed newfindings at follow-up S-MRCP (NS; Table 4).
Smoking
Five out of the seven patients with new chronic findings after2 years were smokers. These patients smoked a mean of 13(2–23) cigarettes per day. In univariate analyses, smokingwas not correlated with increased prevalence of chronicchanges (Table 4). Out of the four patients who developedchronic pancreatitis, three were smokers, reportedly smokinga mean 18 (16–23) cigarettes per day at follow-up.
Pseudocysts
Eleven patients who participated in the second and seventhyear imaging studies had a pseudocyst at 2 years. Five ofthese patients had a recurrence (p=0.04) of which two de-veloped chronic pancreatitis and three were diagnosed withnew diabetes in 5–7 years after hospitalization. Of the sixpatients with no recurrence, one developed new diabetes at6 years and other impaired glucose metabolism at 7 years;three patients were diagnosed with diabetes before.
Two patients with recurrence had normal morphology at2 years and one had other chronic changes than pseudocysts(parenchymal changes, abnormal secretin dilatation, and atro-phy). As mentioned earlier, the patients took part in a random-ized intervention study, where 120 patients were randomizedto either initial intervention during hospitalization only or to
Fig. 1 S-MRCP imagingfindings at baseline,2 and 7 years
Table 2 Demographics of patient material on admission, n=44
Age mean 46 (25–68)
Sex
Male 41 (93 %)
Female 3 (7 %)
AUDIT points mean 19 (5–32)
SADD points mean 13 (0–33)
Alcohol consumption (grams/2 months) mean 3,520 (770–11,400)
Smoking
Yes 30 (68 %)
No 14 (32 %)
BMI mean 28 (21–35)
Severity
Mild 29 (66 %)
Moderate 11 (25 %)
Severe 4 (10 %)
J Gastrointest Surg (2014) 18:164–171 167
repeated interventions at 6-month intervals. The interventionconsisted of a 30-min counseling session by a trained nurse tomake patients aware of the dangers of alcohol to the pancreasand encouraging patients to take responsibility to stopdrinking.19 Half of the patients in long-term follow-up werein the repeated intervention study arm, while half were in theinitial intervention group only. There were no other differ-ences between these groups.
Discussion
Long-term pancreatic morphological changes induced by asingle episode of alcoholic pancreatitis have not been
thoroughly studied before. The main purpose of this studywas to prospectively evaluate the natural healing process ofthe pancreas in a non-assorted patient cohort. The mainfindings were that in the long-term patients with recurrentepisodes have chronic changes in the pancreas significantlymore often. Patients with mild first attack of acute pancrea-titis had fewer chronic changes in long-term follow-up.Smoking and BMI were not identified as independent riskfactors in this patient group. Pseudocyst at 2 years correlatedwith recurrences as previously reported.18
CTand abdominal US are the preferred imaging modalitiesin the acute phase of the pancreatitis. MRI and endoscopicultrasound (EUS) are the primary tools for specifying theetiology and evaluating parenchymal and ductal abnormalitiesin chronic pancreatitis. MRI is a non-invasive technique com-pared to EUS and superior in diagnosing pancreatic ductalvariations accompanied with iv-administered secretin.24,25
The sensitivity of S-MRCP for early chronic pancreatitis is92% and the specificity 75%.26,27 As a non-ionizing radiationmodality, it is also safe for the patient and ensures much higherpatient compliance. While EUS is sensitive in detectingchronic pancreatitis, the limitation in almost close to 10 yearsof follow-up is the operator dependence of the procedure. CTor ERCP have been reported to identify calcifications betterthan MRI, but MRCP is superior to CT in detecting compli-cations of CP.28 In this study, the same experienced radiologistdiagnosed and categorized all the S-MRCP images withoutinformation on the patients’ clinical details.
Alcohol is the main cause of recurrent pancreatitis. Earlierlong-term follow-up studies have reported that 41–48 % ofpatients with alcoholic pancreatitis suffer from recurrentattacks.9,29–31 A multicenter study of five European coun-tries reported recurrent episodes in 37 % patients with alco-holic pancreatitis.32,33 In our study, recurrent pancreatitiswas significantly correlated to increased pancreatic damage.
Table 4 Normal versus chronic pancreatic morphology at 7 years,n=36
Normal (%) Chronic (%) p value
Smoking
Yes (26) 14 (54) 12 (46)
No (10) 5 (50) 5 (50) NS
Mean BMI
>28 (18) 8 (44) 10 (56)
<28 (18) 11 (61) 7 (39) NS
Severity
Severe (4) 1 (25) 3 (75)
Moderate (7) 1 (14) 6 (86)
Mild (25) 17 (68) 8 (32) 0.03, 0.01
Recurrent episodes
Yes (8) 1 (13) 7 (88)
No (28) 18 (64) 10 (36) 0.02
a Significant when compared to moderate and moderate or severe firstpancreatitis
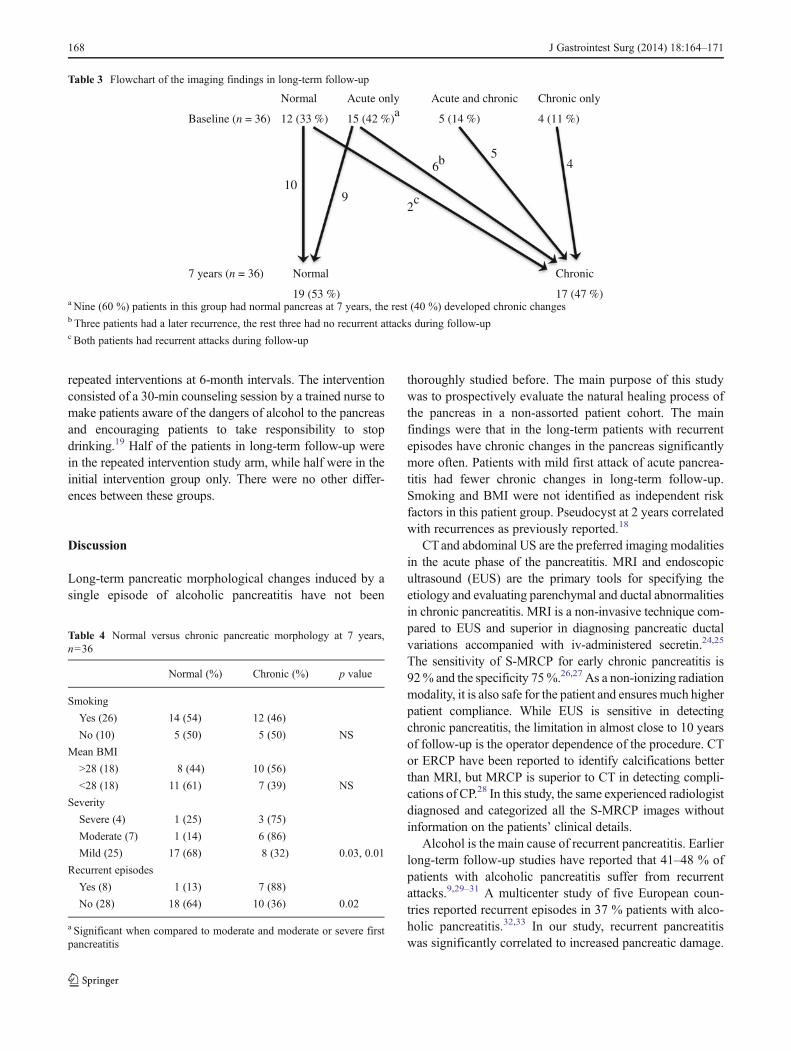
Table 3 Flowchart of the imaging findings in long-term follow-up
Normal Acute only Acute and chronic Chronic only
Baseline (n = 36) 12 (33 %) 15 (42 %)a 5 (14 %) 4 (11 %)
7 years (n = 36) Normal
19 (53 %)
Chronic
17 (47 %)
10
29
65
4b
c
a Nine (60 %) patients in this group had normal pancreas at 7 years, the rest (40 %) developed chronic changesb Three patients had a later recurrence, the rest three had no recurrent attacks during follow-upc Both patients had recurrent attacks during follow-up
168 J Gastrointest Surg (2014) 18:164–171

The original Atlanta classification dividing patients intomild or severe acute pancreatitis was introduced in 1992.34
In order to achieve a more consistent and clearer classifica-tion, a revision was completed in 2012 using easily identifi-able clinical and radiologic criteria to classify the severity ofacute pancreatitis into three classes.21 We used these updatedcriteria to re-evaluate the severity of the first attack using ourgathered data and hospital patient files. Patients with mildpancreatitis developed fewer chronic changes in the longterm than did patients with moderate or the group of moder-ate and severe pancreatitis together (p=0.03 and 0.01). Thegroup of patients with severe pancreatitis was not big enoughto be compared alone. In light of these findings, the newupdated Atlanta criteria seem to work well even in predictingthe morphological outcome of pancreatitis in the long term.
In this study population, smoking and BMI were notcorrelated with the prevalence of chronic changes in the longterm, although smoking has clearly earlier been associatedwith progression to CP.2 However, 71 % (5/7) patients withnew chronic changes after 2 years were smokers. Also, 83 %(5/6) of the patients who initially had only acute findings butlater developed chronic findings were smokers (Table 3).The effect of smoking on pancreatic morphology requiresfurther investigation. In general, smoking is very commonamong patients with chronic alcohol abuse, and thus amongpatients suffering alcoholic pancreatitis. Almost 70 % of thepatients were smokers in this study population with nosignificant change in patients’ smoking habits duringfollow-up. Thus, it was not possible to show significantdifferences between smoking and nonsmoking groups in thispatient cohort. One weakness regarding the evaluation of thepossible effect of smoking on pancreatic morphology wasthat we did not record smoking in pack years from the timebefore the first attack of acute pancreatitis.
In the present study, half of the patients with recurrencesprogressed to chronic pancreatitis (overall 11 %). One ofthese patients had initially severe necrotizing pancreatitis,the other three had initially mild first attack. They all devel-oped new chronic findings in follow-up. Three of these fourpatients were smokers. Patients with no recurrences did notdevelop CP. This finding could support the hypothesis of atransition from alcoholic AP to CP35 In a Danish prospectivelong-term study, 24 % of the patients with first alcoholic APprogressed to CP in a mean of 3.5 years.36 Lankisch et al.reported that patients who survived a second attack are at thehighest risk to develop CP. Both studies found smoking asthe most important risk factor for transition.2
We were unable to significantly demonstrate the pos-sible impact of abstinence on pancreatic morphology.Abstinence has been found to fully protect againstrecurrences.12 In this study, abstainers did not sufferrecurrent episodes. There was one single abstainer with
new pancreatic atrophy at 7 years at the age of 63,while the others did not develop new changes whenabstinent. On the other hand, pancreatic atrophy mayalso be associated with normal aging even without anypathologic progression.26 Complete abstinence afteracute alcoholic pancreatitis is rarely achieved. Attentionshould be paid to decrease recurrences in alcoholicpancreatitis. Nordback et al. have demonstrated thatactive interventions with 6 months intervals decreaserecurrences effectively and also help to decrease pa-tients’ dependency on alcohol.19
Conclusion
Morphological pancreatic changes increase with recurrentepisodes of acute pancreatitis. Patients with mild first epi-sode assessed with the updated Atlanta criteria had fewerchronic changes in the pancreas even in the long term.However, independent of severity, even a single episode ofacute alcoholic pancreatitis may induce chronic morpholog-ical changes in long-term follow-up.
References
1. Apte MV, Pirola RC, Wilson JS. Mechanisms of alcoholic pancrea-titis. Journal of Gastroenterology & Hepatology 2010;25:1816–26.
2. Lankisch PG, Breuer N, Bruns A, Weber-Dany B, Lowenfels AB,Maisonneuve P. Natural history of acute pancreatitis: a long-termpopulation-based study. Am J Gastroenterol 2009;104:2797–805.
3. Yadav D, O’Connell M, Papachristou GI. Natural historyfollowing the first attack of acute pancreatitis. Am J Gastroenterol2012;107:1096–103.
4. Yadav D, Lowenfels AB: Trends in the epidemiology of the firstattack of acute pancreatitis: a systematic review. Pancreas2006;33:323–30.
5. Lankisch PG, Assmus C,Maisonneuve P, Lowenfels AB. Epidemiologyof pancreatic diseases in Lüneburg County. Pancreatology 2002;2:469–77.
6. Kristiansen L, Gronbaek M, Becker U, Tolstrup JS. Risk of pan-creatitis according to alcohol drinking habits: a population basedcohort study. Am J Epidemiol 2008;168:932–7.
7. Irving HM, Samokhvalov AV, Rehm J. Alcohol as a risk factor forpancreatitis. A systematic review and meta-analysis. JOP 2009;10:387–92.
8. Frossard JL, Steer ML, Pastor CM. Acute pancreatitis. Lancet2008;371:143–52.
9. Pelli H, Sand J, Laippala P, Nordback I. Long-term follow-up afterthe first episode of acute alcoholic pancreatitis: time course and riskfactors for recurrence. Scand J Gastroenterol 2000;35:552–5.
10. Pelli H, Lappalainen-Lehto R, Piironen A, Sand J, NordbackI. Risk factors for recurrent acute alcohol-associated pancrea-titis: a prospective analysis. Scand J Gastroenterol 2008;43:614–21.
J Gastrointest Surg (2014) 18:164–171 169
11. Takeyama Y. Long-term prognosis of acute pancreatitis in Japan.Clin Gastroenterol Hepatol 2009;7:15–7.
12. Nikkola J, Räty S, Laukkarinen J, Seppänen H, Lappalainen-LehtoR, Järvinen S, Nordback I, Sand J. Abstinence after first acutealcohol-associated pancreatitis protects against recurrent pancreati-tis and minimizes the risk of pancreatic dysfunction. AlcoholAlcohol 2013;doi: 10.1093/alcalc/agt019.
13. Sadr-Azodi O, Andrén-Sandberg Å, Orsini N, Wolk A. Cigarettesmoking, smoking cessation and acute pancreatitis: a prospectivepopulation-based study. Gut 2012;61:262–7.
14. Sand J, Nordback I. Acute pancreatitis: risk of recurrence and lateconsequences of the disease. Nat Rev Gastroenterol Hepatol.2009;6:470–7.
15. Braganza JM, Lee Sh, McCloy RF, McMahon MJ. Chronic pan-creatitis. Lancet 2011;377:1184–97.
16. Whitcomb DC, LaRusch J, Krasinskas AM, Klei L, Smith JP, BrandRE, Neoptolemos JP, Lerch MM, Tector M, Sandhu BS, Guda NM,Orlichenko L; Alzheimer’s Disease Genetics Consortium, Alkaade S,Amann ST, Anderson MA, Baillie J, Banks PA, Conwell D, CotéGA, Cotton PB, DiSario J, Farrer LA, Forsmark CE, Johnstone M,Gardner TB, Gelrud A, GreenhalfW, Haines JL, HartmanDJ, HawesRA, Lawrence C, Lewis M, Mayerle J, Mayeux R, Melhem NM,Money ME, Muniraj T, Papachristou GI, Pericak-Vance MA,Romagnuolo J, Schellenberg GD, Sherman S, Simon P, Singh VP,Slivka A, Stolz D, Sutton R, Weiss FU, Wilcox CM, Zarnescu NO,Wisniewski SR, O’Connell MR, Kienholz ML, Roeder K, BarmadaMM, Yadav D, Devlin B. Common genetic variants in the CLDN2and PRSS1-PRSS2 loci alter risk for alcohol-related and sporadicpancreatitis. Nat Genet. 2012;44:1349–54.
17. Tukiainen E, Kylänpää ML, Kemppainen E, Nevanlinna H, Paju A,Repo H, Stenman UH, Puolakkainen P. Pancreatic secretory trypsininhibitor (SPINK1) gene mutations in patients with acute pancrea-titis. Pancreas 2005;30:239–42.
18. Pelli H, Lappalainen-Lehto R, Piironen A, Järvinen S, Sand J,Nordback I. Pancreatic damage after the first episode of acutealcoholic pancreatitis and its association with the later recurrencerate. Pancreatology 2009;9:245–51.
19. Nordback I, Pelli H, Lappalainen-Lehto R, Järvinen S, Räty S, Sand J.The recurrence of acute alcohol-associated pancreatitis can be reduced:a randomized controlled trial. Gastroenterology 2009;136:848–55.
20. Nordback I, Sand J, Andrén-Sandberg Å. Criteria for alcoholicpancreatitis—results of an international workshop in Tampere,Finland, June 2006. Pancreatology 2007;7:100–4.
21. Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, SarrMG, Tsiotos GG, Vege SS; Acute Pancreatitis ClassificationWorking Group. Classification of acute pancreatitis—2012: revi-sion of the Atlanta classification and definitions by internationalconsensus. Gut 2013;62:102–11.
22. Lankisch PG, Weber-Dany B, Maisonneuve P, Lowenfels AB.Pancreatic pseudocysts: prognostic factors for their developmentand their spontaneous resolution in the setting of acute pancreatitis.Pancreatology 2012;12:85–90.
23. Balci NC. MRI assessment of chronic pancreatitis. Diagn IntervRadiol 2011;17:249–54.
24. Mariani A, Arcidiacono PG, Curioni S, Giussani A, Testoni PA.Diagnostic yield of ERCP and secretin-enhanced MRCP and EUSin patients with acute recurrent pancreatitis of unknown aetiology.Digestive and Liver Disease 2009;41:753–8.
25. Thevenot A, Bournet B, Otal P, Canevet G, Moreau J,Buscail L. Endoscopic ultrasound and magnetic resonancecholangiopancreatography in patients with idiopathic acute pancrea-titis. Dig Dis Sci 2013;doi:10.1007/s10620-013-2632-y.
26. Czakó L. Diagnosis of early-stage chronic pancreatitis bysecretin-enhanced magnetic resonance cholangiopancreatography. JGastroenterol 2007;42:113–7.
27. Testoni PA, Mariani A, Curioni A, Giussani A, Masci E.Pancreatic ductal abnormalities documented by secretin-enhanced MRCP in asymptomatic subjects with chronic pan-creatic hyperenzymemia. Am J Gastroenterol 2009;104:1780–6.
28. Choueiri NA, Balci NC, Alkaade S, Burton FR. Advancedimaging of chronic pancreatitis. Curr Gastroenterol Rep 2010;12:114–20.
29. Appelros S, Borgstrom A. Incidence, aetiology and mortality rateof acute pancreatitis over 10 years in a defined urban population inSweden. Br J Surg 1999;86:465–70.
30. Gislason H, Horn A, Hoem D, Andrén-Sandberg Å, Imsland AK,Søreide O, Viste A. Acute pancreatitis in Bergen, Norway. A studyon incidence, etiology and severity. Scandinavian Journal ofSurgery 2004;93:29–33.
31. Lund H, Tonnesen H, Tonnesen MH, Olsen O. Long-term recur-rence and death rates after acute pancreatitis. Scand J Gastroenterol2006;41:234–8.
32. Gullo L, Migliori M, Oláh A, Farkas G, Levy P, Arvanitakis C,Lankisch P, Beger H. Acute pancreatitis in five European countries:etiology and mortality. Pancreas 2002;24:223–7.
33. Gullo L, Migliori M, Pezzilli R, Oláh A, Farkas G, Levy P,Arvanitakis C, Lankisch P, Beger H. An update on recurrent acutepancreatitis: data from five European countries. Am J Gastroenterol2002;97:1959–62.
34. Bradley EL III. A clinically based classification system for acutepancreatitis. Summary of the International Symposium on AcutePancreatitis, Atlanta, GA, September 11 through 13, 1992. ArchSurg 1993;128:586–90.
35. Ammann RW, Muellhaupt B. Progression of alcoholic acute tochronic pancreatitis. Gut 1994;35:552–6.
36. Nojgaard C, Becker U, Matzen P, Andersen JR, Holst C, BendtsenF. Progression from acute to chronic pancreatitis. Pancreas2011;40:1195–200.
Discussant
Dr. Nicholas Zyromski (Indianapolis, Indiana): Pancrea-tic morphological changes in a long-term follow-up after firstepisode of acute alcoholic pancreatitis.Nikkola, et al.
These Finnish authors provide a strong contribution to ourknowledge of acute alcoholic pancreatitis natural history.The major strength of this study lies in the diligent, long-term (9 years!) follow-up of an extremely challenging patientpopulation. The authors found that a primary episode ofsevere pancreatitis (as opposed to mild or moderate severity)was accompanied by recurrent pancreatitis episodes andpancreatic morphologic changes.
Questions:1. Did morphologic changes seen on secretin-stimulated
MRCP correlate with clinical exocrine and endocrineinsufficiency rates?How does this knowledge influence clinical practice(are you more likely to offer decompression ofpseudocyst prior to symptom development)?
170 J Gastrointest Surg (2014) 18:164–171

Closing Discussant
Dr. Jussi Nikkola: Patients who had normal pancreatic mor-phology at seven years had not developed chronic pancreatitis infollow-up, while 24% (4/17) of patients with chronic changes atseven years had developed clinically significant pancreatic exo-crine insufficiency (p=0.04). These patients had all gonethrough a recurrent episode or episodes of pancreatitis.
Seventen percent (3/18) of patients who had normal mor-phology at seven years had developed new diabetes. Amongpatients with chronic findings at seven years 42 % (5/12) hada new diagnose of diabetes during follow-up (NS) (patientswith diabetes diagnosed before or during hospitalizationexcluded). One patient who had chronic pancreatitis didn’tdevelop diabetes but the rest three did.
Pseudocyst at two years was noted as a risk factorfor recurrences as Pelli et al. previously reported. Oc-currence of persistent pseudocyst, even asymptomatic,should thus probably favor active drainage. No addi-tional risk factors were found in this study. We man-aged to report important observations of long-termchanges in pancreatic morphology during natural courseof acute alcoholic pancreatitis. Main findings were thatrecurrent episodes are connected to increased pancreaticdamage and patients with mild first attack have lesschronic changes during follow-up. Attention should bepaid to decrease recurrences in alcoholic pancreatitis.Nordback et al. have demonstrated that active interven-tions with six-months intervals decrease recurrenceseffectively.
J Gastrointest Surg (2014) 18:164–171 171