Embed Size (px)
Citation preview

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 1/35
Pancreas: Anatomy &Pancreas: Anatomy &
PhysiologyPhysiology

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 2/35
PancreasPancreas
Gland with both exocrine andGland with both exocrine andendocrine functionsendocrine functions
66--10 inch in length10 inch in length 6060--100 gram in weight 100 gram in weight

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 3/35
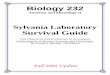
Location: RetroLocation: Retro--peritoneum, 2peritoneum, 2ndnd
lumbar vertebral levellumbar vertebral level
Extends in an oblique, transverseExtends in an oblique, transversepositionposition
Parts of pancreas: head, neck, bodyParts of pancreas: head, neck, body
and tailand tail

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 4/35

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 5/35
PancreasPancreas

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 6/35
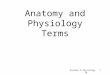
Enzymes of PancreasEnzymes of Pancreas
ProteasesProteases essential for protein digestionessential for protein digestion secreted assecreted as proenzymesproenzymes and requireand require
activation foractivation for proteolyticproteolytic activityactivity duodenal enzyme,duodenal enzyme, enterokinaseenterokinase, converts, converts
trypsinogentrypsinogen toto trypsintrypsin TrypsinTrypsin, in turn, activates, in turn, activates chymotrypsinchymotrypsin,,
elastaseelastase,, carboxypeptidasecarboxypeptidase, and, and
phospholipasephospholipase Within the pancreas, enzyme activation isWithin the pancreas, enzyme activation is
prevented by anprevented by an antiproteolyticantiproteolytic enzymeenzymesecreted by thesecreted by the acinaracinar cellscells

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 7/35
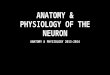
InsulinInsulin
Synthesized in the B cells of the islets of Synthesized in the B cells of the islets of LangerhansLangerhans
80% of the islet cell mass must be80% of the islet cell mass must besurgically removed before diabetessurgically removed before diabetesbecomes clinically apparent becomes clinically apparent
ProinsulinProinsulin, is transported from the, is transported from the
endoplasmic reticulum to the Golgiendoplasmic reticulum to the Golgicomplex where it is packaged intocomplex where it is packaged intogranules and cleaved into insulin and agranules and cleaved into insulin and aresidual connecting peptide, or C peptideresidual connecting peptide, or C peptide

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 8/35
InsulinInsulin
Major stimulantsMajor stimulants
Glucose, amino acids, glucagon, GIP,Glucose, amino acids, glucagon, GIP,
CCK, sulfonylurea compounds,CCK, sulfonylurea compounds, --Sympathetic fibersSympathetic fibers
Major inhibitorsMajor inhibitors
somatostatinsomatostatin,, amylinamylin,, pancreastatinpancreastatin,, --
sympathetic fiberssympathetic fibers

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 9/35
GlucagonGlucagon
Secreted by the A cells of the islet Secreted by the A cells of the islet
Glucagon elevates blood glucose levelsGlucagon elevates blood glucose levelsthrough the stimulation of glycogenolysisthrough the stimulation of glycogenolysis
and gluconeogenesisand gluconeogenesis Major stimulantsMajor stimulants
Aminoacids, Cholinergic fibers, Aminoacids, Cholinergic fibers, --Sympathetic fibersSympathetic fibers
Major inhibitorsMajor inhibitors Glucose, insulin, somatostatin,Glucose, insulin, somatostatin, --
sympathetic fiberssympathetic fibers

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 10/35
SomatostatinSomatostatin
Secreted by the D cells of the islet Secreted by the D cells of the islet
Inhibits the release of growthInhibits the release of growth
hormonehormone Inhibits the release of almost allInhibits the release of almost all
peptide hormonespeptide hormones
Inhibits gastric, pancreatic, and biliaryInhibits gastric, pancreatic, and biliary
secretionsecretion Used to treat both endocrine andUsed to treat both endocrine and
exocrine disordersexocrine disorders

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 11/35
Pancreatic function testsPancreatic function tests

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 12/35
Exocrine functionExocrine function
Secretin testSecretin test
Overnight fast Overnight fast
Double lumen tubeDouble lumen tube
Basal secretionBasal secretion
2u/kg of Secretin2u/kg of Secretin
Four 20 min collections of secretionsFour 20 min collections of secretions
Test for volume, bicarbonate,Test for volume, bicarbonate,amylaseamylase

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 13/35
FLOW BICARBON ATE, AND ENZY ME CHANGES OBSERVED IN FLOW BICARBON ATE, AND ENZY ME CHANGES OBSERVED IN PATIENTS WITH VARIOUS PANCREATIC DISORDERSPATIENTS WITH VARIOUS PANCREATIC DISORDERS
DisorderDisorder PatternPattern Flow rateFlow rate Max. bicarbMax. bicarbconcentrationconcentration
Enzyme secretionEnzyme secretion
EndEnd--stagestagepancreatitis,pancreatitis,advancedadvanced
pancreatic cancerpancreatic cancer
Total insufficiencyTotal insufficiency DecreasedDecreased DecreasedDecreased DecreasedDecreased
ChronicChronicpancreatitispancreatitis
QualitativeQualitativeinsufficiencyinsufficiency
NormalNormal DecreasedDecreased NormalNormal
Pancreatic cancerPancreatic cancer QuantitativeQuantitative
insufficiencyinsufficiency
DecreasedDecreased NormalNormal NormalNormal
MalnutritionMalnutrition Isolated enzymeIsolated enzymedeficiencydeficiency
NormalNormal NormalNormal DecreasedDecreased
HemochromatosisHemochromatosisZollingerZollinger--EllisonEllisonsyndrome, varioussyndrome, various
cirrhosescirrhoses
HypersecretionHypersecretion IncreasedIncreased NormalNormal NormalNormal

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 14/35
Fecal fat test Fecal fat test
Distinguish between pancreatic dysfunctionDistinguish between pancreatic dysfunctionand intestinal malabsorptionand intestinal malabsorption
In Pancreatic disease when lipase secretionIn Pancreatic disease when lipase secretionis reduced by 90%is reduced by 90%-- 2424--hour fecal fat hour fecal fat content is elevated to more than 20 g.content is elevated to more than 20 g.
Intestinal dysfunctionIntestinal dysfunction -- Steatorrhea withSteatorrhea with
low levels of fecal fat low levels of fecal fat UseUse-- Efficacy of pancreatic enzymeEfficacy of pancreatic enzyme
replacement replacement

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 15/35
The dimethadione (DMO) The dimethadione (DMO) test test
Pancreas degrades TrimethadionePancreas degrades Trimethadione(anticonvulsant ), and secretes its(anticonvulsant ), and secretes its
metabolite, DMO.metabolite, DMO. TrimethadioneTrimethadione -- 0.45 g Po TID for 30.45 g Po TID for 3
days.days.
Secretin test is performed.Secretin test is performed. The duodenal output of DMO The duodenal output of DMO
measuredmeasured
Impaired in exocrine insufficiencyImpaired in exocrine insufficiency

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 16/35
The Lundh test The Lundh test
Based on endogenous secretion of secretin andBased on endogenous secretion of secretin andCCK in addition to pancreatic secretionCCK in addition to pancreatic secretion
Overnight fast Overnight fast
Basal collection of duodenal fluidBasal collection of duodenal fluid
Meal of 18 g of corn oil, 15 g of casein, and 40 gMeal of 18 g of corn oil, 15 g of casein, and 40 gof glucose in 300 mL of water.of glucose in 300 mL of water.
ThirtyThirty--minute collectionsminute collections -- for 2 hoursfor 2 hours
Analyzed for trypsin, amylase, and lipase Analyzed for trypsin, amylase, and lipase
Abnormal in patients with chronic pancreatitis Abnormal in patients with chronic pancreatitis
LimitationsLimitations -- Need for duodenal intubationNeed for duodenal intubation
Abnormal Abnormal -- Dis. involving the GI mucosaDis. involving the GI mucosa

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 17/35
Triolein breath test Triolein breath test
Noninvasive test of exocrine insufficiencyNoninvasive test of exocrine insufficiency
25 grams of corn oil containing 5 mCi of 25 grams of corn oil containing 5 mCi of [14C]triolein is given orally[14C]triolein is given orally
4 hours later4 hours later -- metabolite 14Cmetabolite 14C--carbon dioxidecarbon dioxidemeasured in breathmeasured in breath
In fat digestion or malabsorption less than 3% of In fat digestion or malabsorption less than 3% of the [14C]triolein dose per hour measured.the [14C]triolein dose per hour measured.
Test repeated after oral pancreatic enzymeTest repeated after oral pancreatic enzyme
replacement.replacement. In exocrine insufficiency achieve a normal rate of In exocrine insufficiency achieve a normal rate of
excretion of 14Cexcretion of 14C carbon dioxide, whereas patientscarbon dioxide, whereas patientswith enteric disorders show no improvement with enteric disorders show no improvement

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 18/35
Paraaminobenzoic(PABA) acidParaaminobenzoic(PABA) acidtest test
Noninvasive test of pancreatic insufficiencyNoninvasive test of pancreatic insufficiency
NN--benzoylbenzoyl--ll--tyrosyltyrosyl--PABA is cleaved byPABA is cleaved bychymotrypsin to form PABA.chymotrypsin to form PABA.
PABA is absorbed from the small intestinePABA is absorbed from the small intestineexcreted in the urineexcreted in the urine
One gram of BTOne gram of BT--PABA in 300 mL of waterPABA in 300 mL of wateris given orally, and urine collections areis given orally, and urine collections are
obtained for 6 hours.obtained for 6 hours. Patients with chronic pancreatitis excretePatients with chronic pancreatitis excrete
less than 60% of the ingested dose of BTless than 60% of the ingested dose of BT--PABA.PABA.

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 19/35
Islet hormoneIslet hormone -- PP levelsPP levels
Basal and meal stimulated levels of plasma PP measuredBasal and meal stimulated levels of plasma PP measured Overnight fast Overnight fast-- Test meal consisting of 20% protein, 40%Test meal consisting of 20% protein, 40%
fat, and 40% carbohydrate is givenfat, and 40% carbohydrate is given Basal levelsBasal levels
NormalNormal-- 100 to 250 pg/mL)100 to 250 pg/mL)Less than 50 pg/mL in severe chronic pancreatitisLess than 50 pg/mL in severe chronic pancreatitis
After meal PP After meal PP --Normally rise to 700 to 1,000 pg/mLNormally rise to 700 to 1,000 pg/mL
Reduced to 250 pg/mL in severe disease.Reduced to 250 pg/mL in severe disease. LimitationsLimitations Depends on intact pancreatic innervation, depressed inDepends on intact pancreatic innervation, depressed in
cases of diabetic autonomic neuropathy, after truncalcases of diabetic autonomic neuropathy, after truncalvagotomy and antrectomyvagotomy and antrectomy

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 20/35
DIFFERENTI AL DI AGNOSIS OF INTESTIN AL ANDDIFFERENTI AL DI AGNOSIS OF INTESTIN AL ANDPANCREATIC STEATORRHEAPANCREATIC STEATORRHEA
ParameterParameter Intestinal steatorrheaIntestinal steatorrhea PancreatitisPancreatitis
Fecal fat Fecal fat <20 g monoglycerides and<20 g monoglycerides anddiglycerides; soapydiglycerides; soapyconsistencyconsistency
>20 g tnglycendes; only>20 g tnglycendes; onlyseepageseepage
DD--XyloseXylose LowLow NormalNormal
Secretion test Secretion test NormalNormal Abnormal Abnormal
SmallSmall--bowel seriesbowel series Abnormal Abnormal NormalNormal
SmallSmall--bowel biopsybowel biopsy Abnormal Abnormal NormalNormal
Lunch mealLunch meal NormalNormal Abnormal AbnormalPABA test PABA test NormalNormal Abnormal Abnormal
PP response to test mealPP response to test meal NormalNormal LowLow
Treatment with pancreaticTreatment with pancreaticenzymesenzymes
No changeNo change Improvement Improvement

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 21/35
Endocrine functionEndocrine function
Oral GTTOral GTT
Confirm the diagnosis of diabetes.Confirm the diagnosis of diabetes.
Indirect assessment of the insulin responseIndirect assessment of the insulin response
to an oral glucose load.to an oral glucose load. Overnight fastlngOvernight fastlng
2 basal blood samples for Blood sugar2 basal blood samples for Blood sugar
Oral glucose load of 40 g/m2 is given overOral glucose load of 40 g/m2 is given over10 minutes.10 minutes.
Blood samples are drawn every 30 minutesBlood samples are drawn every 30 minutesfor 2 hoursfor 2 hours

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 22/35
INTERPRETATION OF ORAL GLUCOSE TOLERANCEINTERPRETATION OF ORAL GLUCOSE TOLERANCETEST RESULTSTEST RESULTS
InterpretationInterpretation FastingFasting
glucoseglucosevaluevalue(mg/dL)(mg/dL)
IntermediateIntermediate
glucoseglucosevaluevalue(mg/dL)(mg/dL)
22--HourHour
glucoseglucosevaluevalue(mg/dL)(mg/dL)
NormalNormal <115<115 andand All values All values<200<200
andand 140140
ImpairedImpairedglucoseglucosetolerancetolerance
<140<140 andand Any value Any value200200
andand 140140 199199
DiabeticDiabetic 140 or140 or<140<140
(Glucose(Glucosetolerancetolerancetest not test not
necessary)necessary)
andand Any value Any value200200
andand 200200
Non diagnosticNon diagnostic Any combination of glucose values that does not fit into another Any combination of glucose values that does not fit into another
categorycategory

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 23/35
Intravenous glucose tolerance testIntravenous glucose tolerance test
Eliminates the GI influences on glucoseEliminates the GI influences on glucosemetabolism that affects the oral GTTmetabolism that affects the oral GTT
I V bolus of 0.5 g of glucose per kg over 2I V bolus of 0.5 g of glucose per kg over 2to 5 minutes.to 5 minutes.
Blood samplesBlood samples -- every 10 minutes for 1every 10 minutes for 1hour.hour.
The decline in glucose concentrationThe decline in glucose concentration(percentage of disappearance per minute) (percentage of disappearance per minute) is called the K value.is called the K value.
A K value of 1.5 or higher is normal. A K value of 1.5 or higher is normal.

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 24/35
Intravenous arIntravenous argginine test inine test
Arginine stimulates the secretion of islet hormones Arginine stimulates the secretion of islet hormones
Diagnosis of hormoneDiagnosis of hormone--secreting tumorssecreting tumors
Overnight fast, and given a 30Overnight fast, and given a 30--minute infusion of minute infusion of
0.5 g of arginine per kilogram.0.5 g of arginine per kilogram. Blood samples are taken every 10 minutesBlood samples are taken every 10 minutes
Radioimmunoassays are performed for the specificRadioimmunoassays are performed for the specifichormones in question.hormones in question.
This test is particularly useful for the diagnosis of This test is particularly useful for the diagnosis of
glucagonglucagon--secreting tumorssecreting tumors Elevations of plasma glucagon to above 400Elevations of plasma glucagon to above 400
pg/mL usually indicate apg/mL usually indicate a glucagonomaglucagonoma

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 25/35
Tolbutamide response test Tolbutamide response test
Useful in detecting hormoneUseful in detecting hormone--secreting tumors.secreting tumors. Sulfonylurea stimulates insulin secretion.Sulfonylurea stimulates insulin secretion. Overnight fasting, basal blood samples are drawn.Overnight fasting, basal blood samples are drawn. One gram of sodium tolbutamide is given intravenouslyOne gram of sodium tolbutamide is given intravenously
Blood glucose level is monitored for 1 hour.Blood glucose level is monitored for 1 hour. Blood samples for radioimmunoassay of insulin or otherBlood samples for radioimmunoassay of insulin or other
suspected hormones, such as somatostatin obtained.suspected hormones, such as somatostatin obtained. In normal patients, the blood glucose level falls to 50% of In normal patients, the blood glucose level falls to 50% of
basal values after 30 minutes.basal values after 30 minutes. Sustained hypoglycemia with hypersecretion of insulin isSustained hypoglycemia with hypersecretion of insulin is
consistent with anconsistent with an insulinomainsulinoma.. In the case of aIn the case of a somatostatinomasomatostatinoma, somatostatin levels are, somatostatin levels are
more thanmore than twice as hightwice as high as the prevailing normal valuesas the prevailing normal valuesfor the particular somatostatin radioimmunoassayfor the particular somatostatin radioimmunoassay

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 26/35
Acute pancreatitis Acute pancreatitis
Blood InvestigationsBlood Investigations CBC,LFT, serumCBC,LFT, serumcalcium, serum amylase andcalcium, serum amylase and lipaselipase, ABG, ABG
Chest Xray (for exclusion of perforatedChest Xray (for exclusion of perforatedviscus) viscus)
Abdominal Xrays (for detection of "sentinel Abdominal Xrays (for detection of "sentinelloop", gallstones which are radioopaque inloop", gallstones which are radioopaque in
10%) 10%) CT abdomenCT abdomen
U/S abdomenU/S abdomen
MRI /MRAMRI /MRA

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 27/35
Chr. PancreatitisChr. Pancreatitis
Study of exocrine pancreatic functionStudy of exocrine pancreatic function
CTCT-- size, duct, stone, mass lesionssize, duct, stone, mass lesions
ERCPERCP--Duct size, stenosis, obstruction,Duct size, stenosis, obstruction,stones, therapeutic stentingstones, therapeutic stenting

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 28/35
Pancreatic neoplasm'sPancreatic neoplasm's
CBC, LFT, Amylase, LipaseCBC, LFT, Amylase, Lipase
CaCa--1919--99-- 80% accurate, prognosis and f/u80% accurate, prognosis and f/u
Genetic testingGenetic testing-- Genetic syndromeGenetic syndrome
associated with hereditary pancreaticassociated with hereditary pancreaticcancercancer--(Peutz(Peutz--Jeghers, HereditaryJeghers, Hereditarypancreatitis, FAMMM, HNPCC)pancreatitis, FAMMM, HNPCC)
Genetic MutationsGenetic Mutations--DPC4 gene(18Q)DPC4 gene(18Q)--
missing in 90% of pancreatic cancers. K missing in 90% of pancreatic cancers. K--ras mutations common. Also changes inras mutations common. Also changes inp53 and p16 tumor suppressor genes.p53 and p16 tumor suppressor genes.

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 29/35
CAT scanCAT scan -- Spiral CTSpiral CT-- Cuts taken throughCuts taken throughpancreas both in a arterial phase and apancreas both in a arterial phase and aportal venous phaseportal venous phase
Local disease and metastatic diseaseLocal disease and metastatic disease MRCPMRCP--Non invasive, assess biliary tract in aNon invasive, assess biliary tract in a
jaundiced pt jaundiced pt ERCPERCP--90% accurate, in pts whom no mass90% accurate, in pts whom no mass
is seen, brushings for biopsyis seen, brushings for biopsy U/SU/S EUSEUS-- Detect early lesions <2cm, L.N Detect early lesions <2cm, L.N
assessment, vascular involvement, FN ACassessment, vascular involvement, FN AC

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 30/35
Cystic neoplasmsCystic neoplasms
CT scanCT scan
SerousSerous mutilocular ,centralmutilocular ,central
calcification,calcification, MucinousMucinous-- more common in body andmore common in body and
tail, 30% malignant potential, needstail, 30% malignant potential, needs
to be resectedto be resected ERCPERCP-- IPMN, common in the headIPMN, common in the head
and mucin secreted from the ductsand mucin secreted from the ducts

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 31/35
Functional endocrine neoplasmsFunctional endocrine neoplasms
InsulinomasInsulinomas Monitored fast test Monitored fast test Insulin to glucose ratio >0.4 (N <0.3)Insulin to glucose ratio >0.4 (N <0.3) Elevated CElevated C--peptide and propeptide and pro--insulin levelsinsulin levels CT, EUSCT, EUS STS (Somatostatin receptor scintigraphySTS (Somatostatin receptor scintigraphy--
Octreotide scan)Octreotide scan)-- Local tumorsLocal tumors--75%, metastatic75%, metastatic--65%, significant false negatives65%, significant false negatives
Visceral angiography Visceral angiography-- not performed anymorenot performed anymore Selective arterial calcium stimulation test(GDA,Selective arterial calcium stimulation test(GDA,
splenic, Inferior Panc. Duo. Art )splenic, Inferior Panc. Duo. Art ) Intraop ultrasoundIntraop ultrasound

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 32/35
GastrinomaGastrinoma Serum gastrinSerum gastrin-- Fasting gastrin>200pgm/mlFasting gastrin>200pgm/ml >1000pgm.ml pathgnomonic>1000pgm.ml pathgnomonic Gastric acid analysisGastric acid analysis--Basal Acid Output>15mEq/hrBasal Acid Output>15mEq/hr
(Non(Non--ulcerogenic causesulcerogenic causes -- Atrophic gastritis, Atrophic gastritis,Pernicious anemia, Vagotomy)Pernicious anemia, Vagotomy)
Secretin Stimulation test Secretin Stimulation test-- Increase by 200 pgm/mlIncrease by 200 pgm/mlabove the basal levelabove the basal level
CT, EUSCT, EUS SRSSRS-- more sensitive than in Insulinomamore sensitive than in Insulinoma Selective arterial secretin stimulation test Selective arterial secretin stimulation test IntraIntra--op ultrasoundop ultrasound

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 33/35
VIPOMA VIPOMA
BMPBMP-- Hypokalemia, Metabolic acidosisHypokalemia, Metabolic acidosis
Elevated VIP levelsElevated VIP levels-- repeated testingrepeated testingrequiredrequired
Gastric acid levelsGastric acid levels-- Achlorohydria Achlorohydria
CT, EUSCT, EUS

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 34/35
GlucagonomaGlucagonoma
HyperglycemiaHyperglycemia
HypoproteniemiaHypoproteniemia Glucagon levelsGlucagon levels
CT, EUSCT, EUS

8/7/2019 Pancrease ANATOMY AND PHYSIOLOGY
http://slidepdf.com/reader/full/pancrease-anatomy-and-physiology 35/35
SomatostatinomaSomatostatinoma
HyperglycemiaHyperglycemia
HypocholorohydriaHypocholorohydria Somatostatin level>100pgm/mlSomatostatin level>100pgm/ml
diagnosticdiagnostic