Embed Size (px)
Citation preview

Pancrea'cCys'cLesionsGuidelines:toadoptortoadapt?
FILIPEVILASBOASGastroenterologyDepartment,CentroHospitalardeSãoJoão,Porto

Toadapt!
Pancrea4cCys4cLesionsGuidelines:
toadoptortoadapt?

Agenda
• Importanceoftheproblem
• Importanceoftrustworthyguidelines
• Currentguidelines• Maindifferencesbetweenguidelines:
– Imagingmodali4es
– Indica4onsforEUS-FNA– Cystfluidmarkers/newendoscopicmodali4es
– Indica4onsforsurgery– Surveillance

MCNSCA
PC SB-IPMN

TheproblemofPancrea4cCys4cLesions
AbdominalMRIPreven4vemedicalcare(Germany)
(n=2803;1821men;meanage51years)
2.5%
De Jong et al. Clin Gastroenterol Hepatol 2010 Changetal.Medicine2016
AbdominalCTHealthscreenexam2003-2013(Seoul,Korea)
(n=21745;60%men;meanage58.7years)
2.1%

ClinicalImportance
MunigalaSetal,GastrointestEndosc.2016
Retrospec4velongitudinalcohortstudy
PancCystsCT/MRIN=755ptsVscontrolwithoutcystsN=520215FU1998-2007.
IncidencerateofPaCawas5.08and.32
per1000pa4ent-years
HRPaCainallpa4entswithcystswas
19.64(95%CI,12.12-31.82;P<.0001)
ClinicalImportance
• Malignancyoccursvirtuallyonlyinmucinouscysts;
• Most(~60%)incidentalPCLsareBD-IPMNs
• IPMNcanprogressfromlowertohighergradesofdysplasiaand,ul4mately,PDAC;
• IPMNsonsurveillance:112invasivecancersin3980pts(37caseseries)over14380person-yearsFU
– 2.8%overall,0.72%peryear
ShimizuYetal.Pancreas.2013
ScheimanJMetal.Gastroenterology.2015
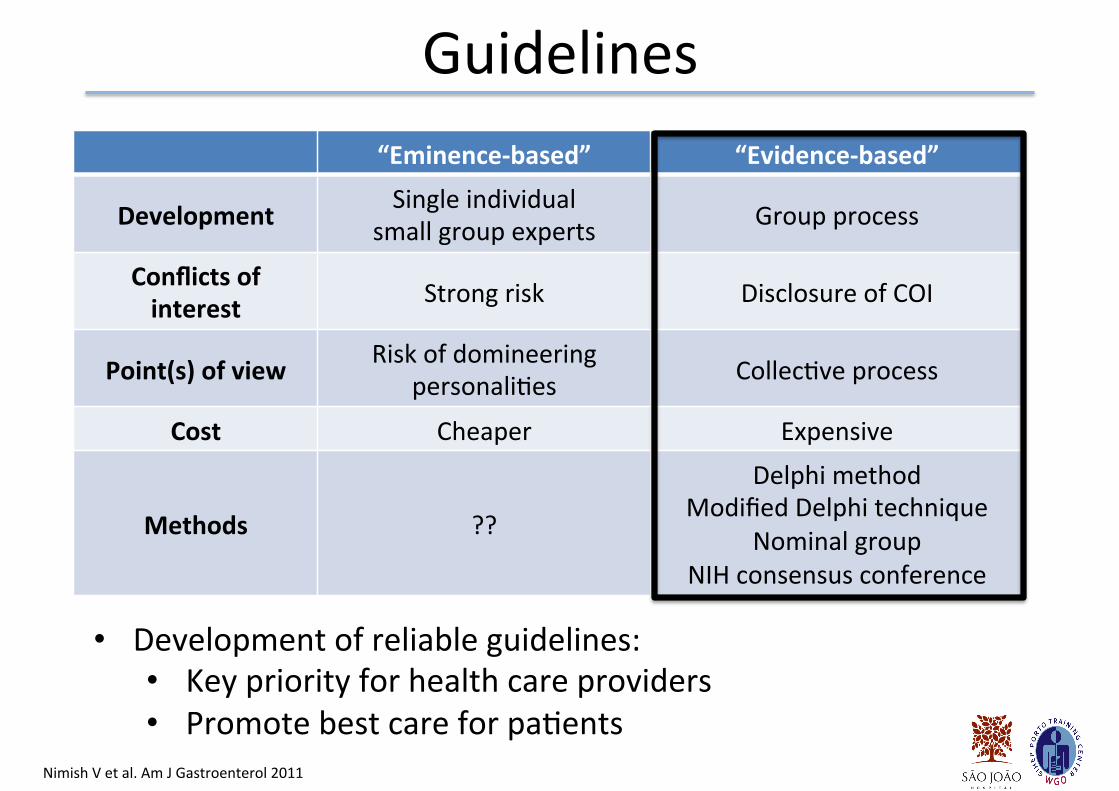
Guidelines
“Eminence-based” “Evidence-based”
Development Singleindividual
smallgroupexpertsGroupprocess
Conflictsofinterest Strongrisk DisclosureofCOI
Point(s)ofview Riskofdomineering
personali4esCollec4veprocess
Cost Cheaper Expensive
Methods ??
Delphimethod
ModifiedDelphitechnique
Nominalgroup
NIHconsensusconference
NimishVetal.AmJGastroenterol2011
• Developmentofreliableguidelines:
• Keypriorityforhealthcareproviders• Promotebestcareforpa4ents

Guidelines
European2018
ACG2018AGA2015
RevisedFukuoka2017
Italian2014
Toomany...Confusing…Howtochoosewhichtofollow?

Cys4clesionsGuidelines
Broadlyconcordant • MD-IPMNs,mixed-IPMNsand
SPNs…à SURGERY
• MCN:nomalignancyifø<4cmandnomuralnodule
• Enhancingsolidnodule/definitesolidnodule≥5mm/+cytology/MPD≥10mm
• SCA:Noneedofresec4onorsurveillance(exceptsymptoma4c)
DiscordantinBD-IPMNs…• EUSIndica4ons
• Impactofcystsize
• Thresholdforsurgery
• Surveillanceintervalsandcessa4on

Reasonsforthecontroversy…
• Dificulttodevelopguidelineswithoutunderstandingthenaturalhistoryofdisease;
• Lowqualityofevidence;
• Keylimita4onofmostofavailableguidelines:– Managementbasedonknowledgeofcysthistology
– Focusedoncystcharacteris4csratherthanthepa4entandtheirul4mateprognosis
• Alwaysconsidertheauthorsandthemethods

SeveralSurgeons,
Gastroenterologists,
Radiologists,
Pathologists
Europe
Considertheauthors…
4Gastroenterologists
NorthAmerica
7Surgeons
3Pathologists
2Oncologists
2Gastroenterologists
America/Asia/Europe

Considerthemethods…
AppraisalofGuidelines,ResearchandEvalua4oninEurope(AGREE)IIinstrument.
FalconiMetal.Pancreatology2015
Allguidelines:scoreslowerthantheminimumAGREE
standardizedscoreregardingRigorofDevelopment

Considerthemethods…
Guideline Consensusprocess
ICG-RevisedFukuoka2017 ConsensusSymposium
AGA2015 GRADEframework
European2018 GRADEframework
ACG2018 GRADEframework
Italian2014 Delphiprocedure;Oxfordcriteria
hqp://www.gradeworkinggroup.org/
GRADE:GradingofRecommenda4onsAssessment,DevelopmentandEvalua4on
Maintopics…
• Ini4alassessment:Imagingmodali4es
• Indica4onsforEUS-FNA• Cystfluidmarkers/Newdiagnos4cmodali4es
• Indica4onsforsurgery• Surveillance:– How?– Interval?– Forhowlong?

Imagingmodali4es
Guideline Imagingrecomenda'onICG(RevisedFukuoka2017)
Pancrea4cprotocolCTorMRCPforcysts>5mmsize
AGA2015 MRI
European2018 MRI-MRCPand/orCT
ACG2018 MRIorCT
Italian2014 MRI-MRCPand/orCT

Indica4onsforEUS-FNA
Guideline EUS-FNAICG(RevisedFukuoka2017) *Worrisomefeatures
AGA2015 **≥2high-riskfeaturesEuropean2018 Clinicalorradiologicalfeaturesofconcern;
HyperenhancementonCH-EUS
ACG2018 Cystsinwhichthediagnosisisunclear,andwherethe
resultsarelikelytoaltermanagement
Italian2014 “suspicious”morphologicalfeaturesoruncertain
radiologicdiagnosis
*Worrisomefeatures:pancrea44s,cyst≥3cm,enhancingmuralnodule<5mm,thickened/enhancingcystwalls,mainductsize
5-9mm,abruptchangeincaliberofpancrea4cductwithdistalpancrea4catrophy,lymphadenopathy,
increasedserumCA19-9,cystgrowthrate>5mm/2years
**AGAHigh-riskfeatures:dilatedMPD(≥5mm),≥3cmcystornon-enhancingsolidcomponent

EUS-FNA
• Diagnosemainductinvolvement
• Confirmasolidcomponent
• Diagnosehigh-gradedysplasiaorcancer
• Cyststhathaveclearindica'onforresec'onbasedonimaging/symptomsdonotneedEUS!

EUS-FNA
Retrospec4vecohortstudy
210ptswithPCLshadEUS2004-2015.
Therequirement≥2HRFwouldhave
decreasedthenumberofEUS
proceduresby91%,butreducedthesensi'vityforpancrea'cmalignancyto50%.
DivyanshooRetal.SurgEndosc.2018

CystFluidAnalysis/Newmodali4es
Guideline CEA Biochemistry Cytology Molecularanalysis
Comments
ICG(RevisedFukuoka2017) M amylase inves4ga4onal
KRAS/GNAS
Inves4ga4onal
EUS-FNAfor
citologyand
molecular
iss4ll
considered
inves'ga'onal
AGA2015 R R Inves4ga4onal
European2018 R Lipase RKRAS/GNAS
(condi4onal)
Brushcitologyandforcepsbiopsynot
recommended
ACG2018 R - RNotreadyfor
clinicalprac4ce
Brushcitology
andforceps
biopsynot
recommended
Italian2014 R amylase R -
CA19.9when
CEA
indeterminate
R:recommended;M:men4oned;-notmen4oned

CystFluidAnalysis
• CEA:– Level≥192ng/mLdis4nguishesmucinous,fromnon-mucinouscysts(Sens75%;Spec84%)
– Inaccuratetopredictgrade!
• Cytology:– Meta-analysis:42%Sens;99%Specdifferen4a4ngmucinousvsnon-mucinous
• KRAS/GNAS/othermolecularmarkers– Costlyandmaynotaddtostandardanalysis!
GillisAetal.HPB(Oxford)2015
NgamruengphongSetal.DigLiverDis.2013
BruggeWRetal.Gastroenterology2004

Vilas-BoasFetal.JClinGastroenterol.2018
• Through-the-needleforcepsbiopsy(Moray-USEndoscopy)
• ContrastEnhancedEndoscopicUltrasound
• Cytologybrush(Echobrush®)
• Needlewithsidefenestra4on(Procore–Cook)
• CystoscopyandPancreatoscopy(Spyglass®)
• ConfocalLASEREndomicroscopy(nCLE)

Surgery
Guideline Symptoms MPD Muralnodule
Posi'vecitology Size Comments
ICG(RevisedFukuoka2017)
+
jaundice≥10mm
+
5mmcut-off+ -*
HRS,
Considerlifeexpectancy,
comorbidi'esandloca'on
AGA2015 NA dilated + + -**and/or2
features
European2018
+
Jaundice,
acute
pancrea44s
≥10mm
(5-9.9mm
rela4ve
indica4on)
+
5mmcut-off+
≥4cm
(rela4ve
indica4o
n)
Growthrate≥5mm/year,new-
onsetDM
elevatedCA19.9
ACG2018
+
Jaundice,
acute
pancrea44s
≥5mm + +≥3cm
Growthrate≥3mm/year,new-
onsetDM
elevatedCA19.9
Italian2014 + ≥10mm + +
Familyhistory(≥2firstdegree
rea4ves*cystsizealoneisnotanappropriateparametertoindicatesurgeryBUTconsidersurgery>2cm,youngfitpts
**posi4vecitologyand/orbothsolidcomponentandMPDdila4on

IPMNs:Individualizeddecision...
Considerthepa'ent!!!
EuropeanGuidelines
Del-ChiaroMetal.Gut.2018
Preemp4vesurgeryCancersurgery
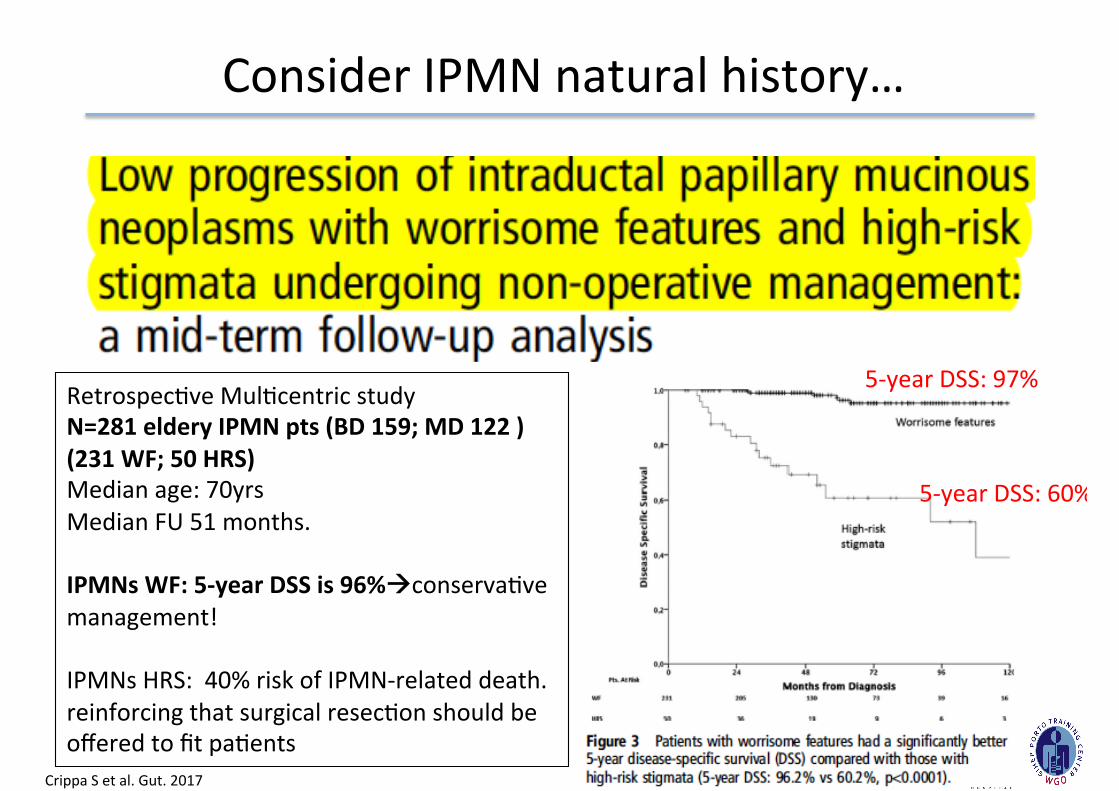
ConsiderIPMNnaturalhistory…
Retrospec4veMul4centricstudy
N=281elderyIPMNpts(BD159;MD122)(231WF;50HRS)Medianage:70yrs
MedianFU51months.
IPMNsWF:5-yearDSSis96%àconserva4ve
management!
IPMNsHRS:40%riskofIPMN-relateddeath.
reinforcingthatsurgicalresec4onshouldbe
offeredtofitpa4ents
CrippaSetal.Gut.2017
5-yearDSS:97%
5-yearDSS:60%

Pa4ent-orientedPCNManagement
Retrospec4vecohort(2005-2010)
N=1800ptswithPCNs;MedianFU=5.7yrs
Stra4fiedbasedonCharlsoncomorbidityindexandbaselinecystfeatures
402deaths–22%(43pancca;359non-pancrea'c)
Pa4ent-relatedfactors+cystfeaturesàhelp
guidePCNmanagement
KwokKetal.AmJGastroenterol.2017

IPMNs:importanceofgrowthrate...
KwongWetal.DigDisSci2015
Retrospec4veMul4centricstudy
N=284pts(BD-IPMNwithoutWForHRS)
FUmedian56months.
Growthrate≥5mm/year-->HR19.5(95%CI2.4-157.8)

Surveillance…mucinouscysts
Guideline Follow-upindica'ons Stopsurveillance
ICG(RevisedFukuoka2017)
<1cm–CT/MRin2-3years
1-2cm–CT/MRyearlyx2thenlengthenas
appropriate
*2-3cm–EUSin3-6monthsthenlengthenas
appropriate
*>3cm–MRI/EUSevery3-6monthsupto1year
Lifelong
(un4lnotfitforsurgery)
AGA2015 MRIa{eroneyearthenMRIevery2yearsStableappearanceaoer
fiveyears
European2018EUS/MRIandCA19-9a{ersixmonths
then
EUS/MRIandCA19-9yearly
Lifelong
(un4lnotfitforsurgery)
Intensifica'onaoer5yrs?
ACG2018 Cystsizeguidessurveillance
(similartoICG)
Whennotfitforsurgery,
assessu'lityinthose>75years
Italian2014 Cystsizeguidessurveillance
(similartoICG)Lifelong
*considersurgeryinyoungfitpa4entswithneedforprolongedsurveillance

Stopsurveillance?No!
CrippaSetal.AmJGastroenterol.2017
Retrospec4veMul4centricstudy
N=144pts(BD-IPMNwithoutWForHRS)withFU>5years(yearlyMRI/MRCP)
MedianFU84months.Rateofmalignancy2%;12yearDSS98.6%
New-onsetofWF/HRSin26pts(18%)aoermedianFU71and77.5months.Oneoutofsixpa4entsdevelopedWF/HRSbeyond5yearsofsurveillance.
Persistentsurveillanceisrequired.Indeed,closerfollow-upevalua'onsshouldbeconsideredaoer5yearsfromini'aldiagnosis.

Stopsurveillance?Maybe…
PergoliniIetal.Gastroenterology2017
Retrospec4veunicentricstudy
N=577ptsBD-IPMNundersurveillance
MedianFU82months.363ptssurveillance>5yrsOverall,45pa4ents(7.8%)developedpanc
malignancy,5ofthemaoer10yrsofFURiskofmalignancy,almost8%,lastedfor10years
ormore
Cyststhatremain1.5cmformorethan5yearsmightbeconsideredlow-risk

Whichguidelineshouldwefollow?
RevisedFukuoka AGA EuropeanThemostaggressive
towardsurgeryThemostconserva4ve
Themostaggressive
towardsurveillance
Leastlikelytomissa
malignancy
Higherpossibilityfor
missingamalignancyIndividualizeddecision
“Livewithunnecessarysurgery” “Livewithuncertainty” “Livewithexcessive
cost”
AdaptedfromTimothyB.Gardner,DDWClinicalSymposium2017

Take-Homemessages
• Fullmul4disciplinarydiscussionupfront!!
• Surgeryathigh-volumecenters!
• Discusstheop4onswiththepa4ents
– Alltheevidencerelatedtothemanagementofpancrea4ccystsisgradedasverylow
quality
– Highrisks4gmatahavethehighestPPVformalignancy
• Treatmentandsurveillancedecisions:
– Decisiontoobservevsresecto{enremainsindividual
– Considerlifeexpectancy,comorbidi4esandloca4on
– Mostpa4entswilldiewiththecystratherthanfromit…
• Strictadherencetoapar'cularguidelineisprobablynotthebestop'onàADAPT!!