Embed Size (px)
Citation preview
PANAMERICAN JOURNAL OF TRAUMAINSTRUCTIONS FOR AUTHORS
Manuscripts and related correspondence should be sent to either Dr. Kimball Maull MD or Dr. Ricardo Ferrada MD to the following addresses: Kimball Maull, M.D. FACS, Carraway Medical Center, 1600 Carraway Boulevard, Birmingham, Alabama USA.
1. Manuscript. The original typescript and two high-quality copies of all illustrations, legends, tables and references must be submitted. All copy, including references, must be typed double-spaced on 21 x 27 cm, heavy-duty white bond paper. Margins must be at least 1 inch. A computer diskette containing a file of the article must be included. Files in Word either for IBM-compatible or Apple are preferred. The diskette should be labeled with the author’s names, the title of the article, the type of computer, and the word processing software used.
2. Title. The title must be short, specific and clear. It cannot exceed 45 characters per line, and is limited to two lines. The title page should include the full names, and academic affiliations of all author. Foot notes indicating where the works was done, where orders for reprints should be addressed and those contributing grants for the work should be given at the bottom of the second page. If the manuscript was presented at a meeting, indicate the name of the organization, the place and the date on which it was read.
3. Illustrations. Please send three complete sets of high contrast glossy prints. Figure number, name of senior author, and arrow indicating top should be typed on a gummed label and affixed to the back of each illustration. Cost of color figures, where used, is borne by authors.
4. Summary. A summary of 150 words or less should be submitted in English and Spanish. The summary must include a statement of the problem, methods of study, results and conclusions. A list of key words to be used for indexing should appear at the end of the summary.
5. References. References should be listed in consecutive numerical order as they are cited in the text. Once a reference is cited, all subsequent citations should be to the original number. All references must be cited in the text or tables. References to journal articles should include: authors, title, journal name as abbreviated in Index Medicus, year, volume number, and inclusive page numbers in that order. References to books should include: authors, chapter title, if any; editor in any; title of book; year; city and publisher. Volume and edition numbers, specific pages, and name of translator should be included when appropriate. The author is responsible for the accuracy and completeness of the references and for their correct text citation.
6. Originality & copyright. Manuscripts and illustrations submitted for consideration should not have been published elsewhere except for such preliminary material presented to the Panamerican Trauma Society.
INSTRUCCIONES PARA LOS AUTORES
Los manuscritos y la correspondencia se deben enviar a Ricardo Ferrada MD o Kimball Maull MD a las siguientes direcciones:Ricardo Ferrada, M.D., FACS Departamento de Cirugía, Hospital Universitario del Valle, Calle 5 # 36-08, Cali, Colombia, S.A.
1. Manuscritos. Se debe enviar un original del manuscrito y dos copias de todas las ilustraciones, leyendas, cuadros y referencias. Todas las copias, incluso las referencias, deben ser escritas a doble espacio en papel blanco de 21 x 27 cm. Los márgenes deben ser amplios. Se debe incluir un diskette que contenga el artículo. Son preferibles los archivos en Word IBM compatibles o Apple. El diskette debe ser marcado con el nombre del artículo y de los autores, el tipo de sistema operativo y el procesador de palabras utilizado.
2. Título. El título debe ser corto, claro y específico. No puede exceder de 45 caracteres por línea y está limitado a dos líneas. La página del título incluye el nombre completo y la posición académica de los autores. En la parte inferior de la segunda página se debe indicar dónde se llevó a cabo el trabajo, la dirección para los reimpresos y las donaciones recibidas para su realización. Si el manuscrito se presentó en una reunión científica, indicar el nombre de la organización, el lugar y la fecha de presentación.
3. Ilustraciones. Por favor enviar tres copias completas de las ilustraciones en alto contraste en papel brillante. En la parte posterior de cada ilustración anote el número de la figura, el autor principal y una flecha con la punta hacia el borde superior. Si existen figuras a color, el costo será cubierto por los autores.
4. Resumen. No debe tener más de 150 palabras y debe ser enviado en español y en inglés. El resumen incluye una definición del problema, los métodos de estudio, los resultados y las conclusiones. Al final del resumen se debe adjuntar una lista de palabras claves para efectos de índice.
5. Referencias. Las referencias se citan en orden numérico consecutivo, tal como aparecen en el texto, e incluyen el siguiente ordenamiento: autores, título en el idioma original, nombre de la revista en su forma abreviada según el Index Medicus, año de publicación, volumen de la revista y páginas iniciales y finales. Se recomienda citar hasta cuatro autores en forma completa. Si hay más de cuatro autores, después del tercero, seguido por una coma, se colocan las palabras latinas et al. Las citas de libros incluyen: autores o editor y así se debe identificar (ed.), título del libro, edición, ciudad de publicación, la empresa editorial y año. Las referencias deben ser verificadas por los autores y ésta es una de sus responsabilidades.
6. Originalidad y derechos de autor. Los manuscritos deben ser inéditos y no haber sido publicados en otra parte, excepto como material presentado a la Sociedad Panamericana de Trauma.
PANAMERICAN JOURNAL OF TRAUMAEditors: RICARDO FERRADA, M.D., Cali, ColombiaRAO IVATURY M.D., Richmond, VirginiaDARIO BIROLINI, M.D., Sao Paulo, Brazil
Assistant Editors: SAMIR RASSLAN M.D., Sao Paulo, BrazilANDREW PEITZMAN M.D., Pittsburgh, PennsylvaniaJORGE NEIRA, M.D., Buenos Aires, Argentina
DDDISTRIBUNAwww.libreriamedica.comEDITORIAL Y LIBRERÍA MÉDICA
RAFAEL ANDRADE, M.D.Panama, PanamaJUAN ASENSIO, M.D. Los Angeles, CaliforniaCARLOS BARBA, M.D.Hartford, ConnecticutLUIS BAEZ, M.D.Caracas, Venezuela MARY BEACHLEY, R.N.Baltimore, Maryland RICARDO ESPINOZA M.D.Santiago, ChileEUGENE FAIST, M.D. Münich, GermanyDAVID FELICIANO, M.D. Atlanta, GeorgiaALBERTO GARCIA, M.D. Cali, ColombiaLUIS GRANJA MENA, M.D.Quito, Ecuador GERARDO GOMEZ, M.D. Indianapolis, Indiana FRANCISCO HOLGUIN, M.D.Cartagena, Colombia LENWORTH M. JACOBS, M.D. Hartford, ConnecticutTEOFILO LAMA PICO, M.D.Guayaquil, Ecuador CHARLES LUCAS, M.D.Detroit, Michigan ROBERT MACKERSIE, M.D.San Francisco, CaliforniaKATZIUKO MAEKAWA, M.D.Kitasato, Japan KIMBALL MAULL, M.D. Birmingham, Alabama
ERNEST E. MOORE, M.D. Denver, ColoradoDAVID MULDER , M.D.Montreal, CanadáDAVID ORTEGA, M.D.Lima, Peru RENATO POGGETTI, M.D.Sao Paulo, BrazilABRAHAM I RIVKIND, M.D. Jerusalem, Israel AURELIO RODRIGUEZ, M.D. Pittsburgh, PennsylvaniaCLAYTON SHATNEY, M.D.San Jose, California RAUL COIMBRA M.D.San Diego, CaliforniaJOSE TROSTCHANSY, M.D.Montevideo, UruguayJOSE MARIO VEGA, M.D.San Salvador, El Salvador
SECTION EDITORS Critical Care:DAVID HOYT, M.D. San Diego, California
Emergengy & DisasterSUSAN BRIGGS, M.D.Boston, Massachusetts
Infection: RONALD MAIER, M.D.Seattle, Washington
Nursing:ROBBIE HARTSOCK, R.N.Baltimore, MarylandVIVIAN LANE, R.N.Hartford, Connecticut
Orthopedic Trauma:BRUCE BROWNER, M.D.Hartford, Connecticut
Pediatrics:MARTIN EICHELBERGER, M.D.Washington, D.C.
Plastic Surgery:DAVID REATH, M.D.Knoxville, Tennessee
Prehospital Care:ALEJANDRO GRIFE, M.D.Mexico, Mexico
Coordinación Editorial:DISTRIBUNAEditorial y Librería Médica Autopista Norte 123 - 93Fax: (1) 2132379Tel: (1) 2132379 - (1) 2158535 Celular: 3108739208 - 3157938377Apartado Aéreo: 265006Bogotá - Colombia w w w . l i b r e r i a m e d i c a . c o mImpreso: Editora Guadalupe
CONTENT CONTENIDO
PANAMERICAN JOURNAL OF TRAUMA
1. ABDOMINAL COMPARTMENT SYNDROME: FINDING & FIXING Rao R. Ivatury MD FACS.
4. ALL TERRAIN VEHICLE (ATV) CRASHES Kimball I. Maull MD FACS.
7. DEFINING STABILITY - THE REAL PLOBLEMMichael Rhodes MD FACS.
9. DELAYED LAPAROTOMY - WHAT NOW?David Feliciano MD FACS.
13. INTESTINAL FISTULAS: TECHNICAL TIPS FOR SUCESSFUL CLOSUREGlen Tinkoff MD FACS.
17. KIDS AND COMPLICATIONS - WHAT YOU NEED TO KNOWDavid P. Mooney MD FACS.
20. NONOPERATIVE MANAGEMENT OF GUNSHOT WOUNDSThomas M. Scalea MD FACS.
23. NURSE CLINICIANS - WHAT IS THEIR ROLE?Kathleen D. Martin MSN RN CCRN.
30. PENETRATING CARDIAC TRAUMA Ricardo Ferrada MD MsP FACS.
35. PROPHYLAXIS IN THE ICU: WHAT WORKS AND WHAT DOESN’TMichael D. Pasquale MD FACS FCCM.
43. SOLID ORGANS - ARE THEY ALL THE SAME?J. Wayne Meredith MD FACS.
50. SURGICAL SIMULATION IN TRAUMA CARELenworth M. Jacobs MD MPH FACS.
55. THE BLUSHING CT SCAN - WHOSE VENUE?Stuart E. Mirvis MD FACR.
Point Counterpoint Presentations. Atlantic City, 2003.
Panam J Trauma 2004, 11:1
1
ABDOMINAL COMPARTMENT SYNDROME: FINDING & FIXINGRao R. Ivatury, MD, FACS.
Professor of Surgery, Emergency medicine and Physiology Virginia Commonwealth University. Director of Trauma and Critical Care. Medical College of Virginia Hospital Richmond, Virginia
Intraabdominal pressure (IAP) elevation or intraabdominal hypertension (IAH) occurs in a variety of clinical situations: bowel distension from ileus or mechanical obstruction, large accumulation of ascitic fluid, extensive abdominal trauma treated by intraabdominal packing, or closure of the abdominal wall under tension. In non-abdominal pathology, IAH may result from third-space fluid accumulation into the bowel wall and the peritoneal cavity during aggressive crystalloid resuscitation. Extensive burns and multiple trauma are the usual clinical scenarios (the so-called secondary abdominal compartment syndrome (ACS).
IAH may result in profound physiologic effects that may culminate in organ dysfunction and failure. ACS is a constellation of these physiologic sequelae of IAH. It is characterized by a tensely distended abdomen, elevated intraabdominal pressure, a rise in airway pressures, inadequate ventilation with hypoxia and hypercarbia and disturbed renal function, among others.
FINDING IAH AND ACS : MEASURE INTRA-ABDOMINAL PRESSURE
While a variety of techniques, such as measuring the inferior vena caval pressure, intragastric pressure or intraperitoneal pressure, are available to evaluate IAP, the most widely used method is to use bladder pressure as a surrogate. About 50 ml of saline are introduced into the urinary bladder through the urethral catheter. The tubing of the collecting bag is clamped and a needle is inserted into the specimen-collecting port of the tubing
proximal to the clamp and is attached to a manometer. Bladder pressure, measured in cm H2O, is the height at which the level of the saline column stabilizes with the symphysis pubis as the zero point. The catheter may be connected to bedside monitors through a transducer and the bladder pressure may be monitored continuously in mm Hg, where 1 mm of mercury equals 1. 36 CMS of water.
WHAT IS THE CRITICAL LEVEL OF IAP THAT REQUIRES TREATMENT?
Burch and associates described a grading system of elevated IAP: Grade I (10-15 cm of H2O ), Grade II (15-25 CMS of H2O ), Grade III (25-35 CMS of H2O) and Grade IV (> 35 CMS of H2O) and suggested that most of the patients with Grade III and all of the patients with Grade IV elevations in IAP should have abdominal decompression. Even at lower pressures, the onset of the syndrome of ACS should prompt abdominal decompression. Our practice is to consider a persistent elevation of IAP beyond 20-25 cm H2O (15-19 mm Hg) as IAH and institute therapy, even in the absence of established signs of ACS. Current studies suggest that IAH (defined as IAP > 20 -25 cm of H2O) may be an earlier phenomenon that, when uncorrected, lead to the full manifestations of ACS. IDENTIFICATION OF PATIENTS “AT RISK” AND PREVENTION OF IAH: FINDING IT Anticipate in these situations: 1. Preoperative hypovolemic shock and massive fluid resuscitation e.g. Burns, peritonitis, pancreatitis, ruptured AAA, GI hemorrhage, multiple or multisystem injuries, 2.

Panam J Trauma
2 Marzo 2004
Abdominal Comparment Syndrome: Finding & Fixing
3Vol. 11 Number 1
Increased intra-abdominal fluid accumulation: e.g. Ascites, excessive fluid resuscitation, coagulopathy and abnormal bleeding, peritonitis, ruptured AAA, pelvic and retroperitoneal hematomas, intestinal obstruction. 3. Mechanical increase in pressure: e.g. “damage-control” surgery with intraabdominal packing, sudden intra-abdominal reduction of long-standing hernial contents (loss of right of domain), tension pneumothorax, massive hemothorax, “chronic” abdominal compartment syndrome from morbid obesity, intestinal obstruction. In these patients at risk, attempt prevention of IAH and ACS by “not closing the abdomen” (“open abdomen”) at the initial operation.
The “open abdomen” approach offers several advantages. First, It provides a rapid method of abbreviating the laparotomy and transporting the patient to the intensive care unit for resuscitation. Second, in a significant number of patients, it may actually prevent IAH. In patients that do develop IAH and ACS, the technique of “open abdomen” facilitates an expedient bedside abdominal decompression. When continued transfusion requirements and IAH suggests an on-going bleeding and ineffective packing, it enables a prompt and more efficient repacking, as well as identification and control of surgical bleeders. As experience with the open abdomen approach has evolved, the incidence of iatrogenic complications such as bowel fistulas or fluid losses may be reduced.
TREATMENT OF IAH AND ACS: FIXING IT
When to Consider Treatment?
A critical level of IAP at 25 CMS of H2O (18.3 mm Hg) should trigger careful monitoring of IAP and prompt treatment if it continues to increase. Obviously, any of the features of A CS should trigger abdominal decompression.
Treatment Approaches
The first step in the evaluation of an increased IAP, especially in the presence of agitation and restlessness, is to sedate and, if necessary, chemically paralyze the patient. If the bladder pressures are still high and/or systemic manifestations of IAH (as described above) are
evident, the appropriate treatment, in most instances, is abdominal decompression.
In patients without previous laparotomy and when “secondary ACS” occurs from massive resuscitation or during non-operative management of liver and spleen injuries, the IAH may be relieved by repeated paracentesis with or without ultra-sound guidance. Excellent results with this approach are reported in small series.
If the abdomen is left “ open “ at previous laparotomy, IAH may be treated by opening of the temporary closure (mesh, plastic or towel clips etc); evacuation of the abdomen of fluid and blood; removal of abdominal packs (with repacking, if necessary) and enlargement of the abdominal space to accommodate the edematous and swollen contents. If the abdomen is previously closed by fascial sutures, a formal operating room celiotomy should be performed to decompress the pressure.
The abdomen is decompressed, abdominal fluid and/or blood evacuated, hemostasis obtained or assured and bowel compromise is ruled out. The results of abdominal decompression are usually rather dramatic, with a decreased inspiratory pressure, improved gas exchange, lessened systemic vascular resistance and increased cardiac index and oxygen delivery. The gut appearance will be better and if measured, oxygenation of the gut will be improved. A brisk increase in urinary output follows. Some have described a reperfusion syndrome immediately after abdominal decompression in some of their patients with ACS and recommended mannitol and bicarbonate infusion as pretreatment to avoid this complication. Once abdominal decompression is achieved, it is the usual practice to leave the abdominal fascia and skin “open” with some type of foreign material at the skin level to prevent evisceration. These materials include various absorbable or non-absorbable types of mesh, an artificial burr device, sterilized GU bags with or without a zipper (“the Bogota bag”), dressings with moist gauze or Vi-drapes, “vacuum-pack” . All have, in common, the goals of preventing evisceration, allowing enlargement of the abdominal cavity, keeping the IAP low and preventing reoccurrence of IAH and ACS. All have the potential problems of secondary bacterial infection of the peritoneal cavity, fluid shifts from the
Panam J Trauma
2 Marzo 2004
Abdominal Comparment Syndrome: Finding & Fixing
3Vol. 11 Number 1
exposed bowel and peritoneum, injury to the bowel with subsequent formation of fistulae, These mandate a very careful and skilled intensive care.
When the resuscitation is successful and the patients are stable’ they should undergo an attempt at definitive closure. Primary fascial closure may be possible in a surprisingly large number of patients (approximately 50% to 60%) after trauma.The recent approach to the “open abdomen” is some variant of the “vacuum-pack” technique. It consists of a polyethylene sheet over the viscera, a moist sterile surgical towel over the sheet, drains over the towel and a suction applied to the drains. The fascia is gradually approximated by multiple trips to the O.R. till a tensionless fascial closure is achieved.
If definitive closure is not feasible, the four alternatives are: 1. raise skin flaps on either side of the midline and suture them together (accepting a large fascial defect that can be repaired at a later date), 2. use a composite fascial prosthesis with an outer nonabsorbable mesh and an inner absorbable one to prevent dense adhesions that are usually the rule with non-absorbable mesh, 3. apply split thickness skin graft to the granulating surface of the bowel and 4. separate the components of the abdominal wall and close the defect by fascial transposition.
SUMMARY
1. The routine use of IAP monitoring is indicated in all patients “at risk”, ( includes most of the massively injured patients or critically ill patients in the ICU)
2. The critical level of IAP that becomes IAH is around 20-25 CMS of H2O,
3. IAH may be an earlier phenomenon that, when persistent or neglected, may lead to the complete manifestations of ACS,
4. ACS may manifest at much lower pressures than previously recognized, and
5. Prophylaxis and aggressive and prompt treatment
of IAH is recommended to prevent ACS from becoming an irreversible syndrome.
BIBLIOGRAPHY
1. Ivatury RR, Diesel L, Porter JM et al: Intra-abdominal hypertension and the abdominal compartment syndrome. Surg.Clin.North.Am. 77:783-800, 1997.
2. Ivatury RR, Porter JM, Simon RJ et al: Intra-abdominal hypertension after life threatening abdominal trauma: Incidence, prophylaxis and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J. Trauma 44 :1016-1021, 1998.
3. Saggi BH, Sugerman HJ, Ivatury RR et al: Abdominal compartment syndrome. J Trauma 45: 597-609, 1998.
4. Burch JM, Moore EE, Moore FA et al: The abdominal compartment syndrome. Surg.Clin.North.Amer. 76:833-842,1996.
5. Widergren JT, Battisella FD: The open abdomen treatment for intraabdominal compartment syndrome. J.Trauma. 37:158, 1994.
6. Maxwell RA, Fabian TC, Croce MA et al: Secondary abdominal compartment syndrome: an underappreciated manifestation of severe hemorrhagic shock. J.Trauma. 47:995-999, 1999.
7. Mayberry JC, Mullins RJ, Crass RA et al: Prevention of abdominal compartment syndrome by absorbable mesh prosthesis closure. 132:957-961, 1997.
8. Barker DE, Kaufman HJ, Smith LA:et al: Vacuum- pack technique of temporary abdominal closure: a 7-year experience with 112 patients. J Trauma 48:201-6; 2000.
9. Fabian TC, Croce MA, Pritchard FE et al: Planned ventral hernia: staged management for acute abdominal wall defects. Ann. Surg. 219:643-650, 1994.
10. Miller PR, Thompson JT, Faler BJ et al: Late fascial closure in lieu of ventral hernia: the next step in open abdomen management. J Trauma. 53: 843-9, 2002.
Panam J Trauma 2004, 11:1
4
All Terrain Vehicle (ATV) Crashes
5Vol. 11 Number 1
ALL TERRAIN VEHICLE (ATV) CRASHES Kimball I. Maull, MD, FACS.
Director, Trauma Center at Carraway Birmingham, Alabama
Riders wanted – only risk-takers need apply. Yamaha ATV Promotional Brochure – 2003
INTRODUCTION
All terrain vehicles (ATVs) are 3 and 4 wheeled motorized means of transportation intended for recreational use on various types of unpaved terrain. They have large low-pressure tires, seats designed to be straddled, handlebars for steering, and engines which range from 30cc to 500cc displacement. The vehicles range from 100 to 300 lbs and have been imported and sold in the United States since 1972.
Between 1983 and 1986, ATV-related injuries increased from 32,100 to 106,000 per year, a jump of greater than 300% and resulted in an investigation by the US Consumer Product Safety Commission (CPSC). As a result, a consent decree was issued in 1988 between the CPSC and the ATV distributors which called for the following safety measures:
1.Discontinue the manufacture anddistribution of 3 wheeled ATVs.2.Implement nationwide trainingprogram.3.Develop voluntary standards to make ATVs safer.4.Provide safety warnings to prospective buyers5.Institute age restrictions on sale of vehicles
There is good evidence that these safety measures were beneficial. Injuries declined from a high of 300,000 in 1987 to approximately 50,000 in 1993 and have remained relatively constant. Annual fatalities dropped
from 900 to 250 during the same period.(1) However, the consent decree was agreed upon for a period of 10 years and expired in 1998. This prompted a review of patterns, characteristics, and trends in ATV usage which was published in 1999.(2) Much of this report draws from the conclusions of this and other studies and a review of ATV-related trauma at the Carraway Medical Center from 1999-2001.
METHODS
The Trauma Registry yielded 17 patients injured in ATV crashes over the 2 year period ending September, 2001. Each medical record was scrutinized for demographic data, mechanism of injury, helmet use, organ systems injured, alcohol and other drug use, need for operative management, complications, and outcome, including survival and estimation of long term impairment.
RESULTS
Patients ranged in age from 14 to 66 years and all but 1 were male. Average length of hospital stay(LOS) was 8.4 days(range 1-58 days). Fourteen of the 17 patients required confinement in the intensive care unit(ICU) with an average ICU LOS of 6.4 days(range 1-49days). Seven patients arrived by air medical transport and 3 were taken directly to the operating room upon arrival. Two patients died of their injuries (mortality 13%) and 3 patients required long term rehabilitation(18%). Data on helmet use was not available on 7 patients. Of the other 10 patients, only 1 was wearing a helmet at the time of injury. Rollover was documented as the injury mechanism in 6 patients. Alcohol contributed to the ATV crash in 4 patients. Cocaine was positive in 4 patients, amphetamine in 1 patient and marijuana in 2 patients.
Panam J Trauma 2004, 11:1
4
All Terrain Vehicle (ATV) Crashes
5Vol. 11 Number 1
However, these results likely underestimate the use of alcohol and recreational drugs.
Organ system injuries are listed below:
CNS 10 Maxillofacial 5 Thoracic 7 Abdominopelvic 4 Musculoskeletal 8
Operative management was required in 10 patients(60%). Complications included myoglobinemia, paralysis, respiratory failure, pneumonia, and jaundice.
DISCUSSION
In 1985, in a paper entitled “The three wheeler – a menace to the pre-adolescent child”, Golladay et al cited the inherent dangers and instability of the 3-wheeled ATV(3). By the following year, the CPSC received reports on 415 ATV deaths, 377 were on 3-wheeled models. In the 1999 report by Rodgers, he documents that although 3-wheeled ATVs have not been sold since 1988, they continue to account for 20% of ATVs in use(2).
Despite a growing body of evidence of the safety concerns regarding ATVs, they keep getting bigger and more powerful, and their appeal to our youth is pervasive. The average size engine in use in 1989 was 190cc, in 1999 it was 250cc, and current engines sizes of 660cc are now available. Speeds can reach 75 miles per hour. In 1988, Greene & Metzler found that most ATV crashes occurred at low speed, in good weather, and during daylight hours(4). More recent data suggests that excessive speed may also contribute to crash occurrence. In fact, Rios-Reboyras et al confirmed in their series of 33 patients, that 66% of ATVs causing injuries were 350cc or greater and some had homemade alterations to increase horsepower(5).
Rios-Reboyras et al identified the typical patient injured in an ATV crash as a male in his early twenties, driving without experience, without a helmet, at excessive speed and under the influence of alcohol. The lack of safety equipment clearly contributes to the severity of injuries.
Greene & Metzler noted that 72% of ATV crash victims in his series were not wearing a helmet, 24% were wearing shorts or a bathing suit, and 72% were wearing either tennis shoes or sandals. None were wearing leather protective gear. In their 1988 report, 26 crashes involved 3-wheelers and 6 involved 4-wheelers.
The most definitive work on the subject of ATV use was published in 1999 by Rodgers and was based on a national probability survey performed by the CPSC. While the survey has limitations, the data are of interest:
• The South and Midwest are over-represented in ATV use• The majority(60%) of ATV-owning households are in low density areas• The median income and education of ATV households are higher than the US norms• 80% of ATV drivers are between the ages of 16 – 50, 15% are less than 16 years of age.• Males drivers predominate(66%)• Wheelies/jumping – 25%• Hilly/difficult terrain – 60%• Carry passengers – 50%• Helmet use – 50% but only 35% always use helmets • Protective clothing – 70%, but boots 50%• Non-recreational use – 75%, mostly farming and ranching• Formal training – 11%• Significant number bought outside dealer franchisesystem(42%)• Owner modifications approach 50%• The number of children ATV drivers under age 16 has declined, but almost all children under age 16 ride ATVs intended for adults(95%)
In 1989, there were approximately 2.75 million ATVs in use; in 1997, there were 4 million. Based on ATV-related injuries and deaths, the injury rate per 10,000 ATVs dropped from 256 to 149 and the death rate from 0.93 to 0.65. This was a reduction of 42% in the injury rate and 30% in the death rate. This improvement in injury and death rates was attributed to impacting 3 ATV driver sub-populations: children, inexperienced drivers, and drivers of 3-wheeled ATVs. However, recent studies on the subject confirm that the problem is again worsening(6).
Panam J Trauma
6 Marzo 2004
There are now 7 million ATVs in use and injuries are on the increase. In 2001, there were 111,000 injuries requiring ED treatment and 547 deaths were recorded in 2000. Children are 4.5 times more likely to be involved in an ATV mishap and are over-represented among those killed or injured.
CONCLUSIONS
ATV crashes can result in disabling, life-threatening injuries. There has been significant improvement in ATV-related injuries and deaths but the problem is still with us. The lapse of the CPSC decree, the sale of bigger and more powerful off-road vehicles, and the appeal to risk-taking behavior of our youth suggests that we will continue to care for victims of ATV crashes in the years to come. Ongoing efforts to address the preventable risk factors of rider inexperience, alcohol use, excessive speed, and riding without safety equipment, appear indicated.
The machines that screams are made of…Yamaha ATV Promotional Brochure – 2003
BIBLIOGRAPHY
1. Dolan MA, Knapp JF, Andres J: Three wheel and four wheel all-terrain vehicle injuries in children. Pediatrics. 84:604-698, 1989.
2. Rodgers GB: The characteristics and use patterns of all-terrain vehicle drivers in the United States. Accident Analysis & Prevention 31:409-419, 1999.
3. Golladay ES, Slezak JW, Mollit DL et al: The three wheeler– a menace to the preadolescent child. J Trauma, 25:232-233, 1985.
4. Greene MA, Metzler MH: Trauma associated with three and four wheeled all-terrain vehicles. J Trauma 28:391-394, 1988.
5. Rios-Reboyras LA, Grovis JE, Ramirez N et al: Musculoskeletal trauma in four-wheeled all-terrain vehicles. Orthopedics 25:1079-1082, 2002.
6. Scutchfield SB: All-terrain vehicles: injuries and prevention. Clin Orthop 409:62-71, 2003.
Panam J Trauma 2004, 11:1
7
DEFINING STABILITY - THE REAL PROBLEMMichael Rhodes, MD, FACS.
Chairman, Department of Surgery, Christiana Care Health System, Wilmington, Delaware
Nonoperative management of blunt torso injuries that had previously required surgery has markedly changed therapeutic strategy for many trauma patients. A non-operative approach has been successfully used on most solid organs in the abdomen including kidney, spleen, liver, pancreas, and adrenal glands. A delayed as well as nonoperative strategy has also been used for thoracic aortic injury. Candidates for nonoperative management are expected to be “stable” before this approach is considered. However, a definition of “stable” is necessary to utilize this approach.
The following guidelines are useful in defining stability:
• There is no absolute definition of stability.• Stability is a clinical determination based on a variety
of physiologic, anatomic, and situational observations.• The variables in defining stability for nonoperative
management include blood pressure, pulse, abdominal distension, age, coagulopathy, organ injured, associated injuries and, to some extent, the blood requirement.
• Persistent or recurring hypotension accompanied by other physical signs of intra-abdominal or retroperitoneal hemorrhage (abdominal distension, pallor, tachycardia) is the classic clinical picture of “instability” and should prompt laparotomy, especially with an abdominal US demonstrating free intra-abdominal fluid.
• In general, the amount of free fluid on CT scan or US does not directly correlate with the likelihood of successful nonoperative management. However, massive free fluid seen on a CT scan increases the likelihood of operative requirement.
• A blush on CT scan does not define instability, but does increase the likelihood that hemodynamic instability may occur.
• A patient with a distended abdomen who has received massive fluid resuscitation in a short period (e.g., 6L in 2 hours) with a previous flat abdomen or a negative abdominal CT scan frequently represents bowel edema and may prompt a non-therapeutic laparotomy (although decompression of abdominal compartment syndrome may occur). This scenario commonly occurs with hemorrhage from pelvic fractures, massive facial/head injury, or mangled extremities.
• Interventional vascular embolization for hemorrhage control may convert an unstable patient to stable without operative intervention.
• A hemodynamically stable patient with a high-grade splenic injury (>grade II) should be considered for laparotomy with any of the following: 1) moderate or severe head injury, 2) advanced age (>65), 3) refractory coagulopathy 4) flail chest.
• A hemodynamically stable patient with a high-grade liver injury should have attempted nonoperative (or interventional radiological) management even in the presence of the high risk factors listed above for splenic injury.
• A hemodynamically stable patient with a high grade renal injury should be considered for nonoperative (or interventional radiological) management even in the presence of the high risk factors listed above, except for massive extravasation of contrast.
• Severe abdominal tenderness either early or late in any hemodynamically stable patient with known solid organ injury should prompt either laparoscopy or laparotomy to rule out hollow viscus injury.
• When nonoperative (with or without radiological interventional therapy) treatment of the liver fails,
Panam J Trauma
8 Marzo 2004
high consideration should be given to inviting a second attending surgeon to participate in the laparotomy.
• Failure to clear blood lactate or base deficit suggests incomplete resuscitation, ongoing ischemia, or sepsis, and by itself does not define instability prompting laparotomy in a patient being managed nonoperativly.
• Failure of nonoperative management of splenic and renal injuries in a closely monitored setting is usually easily controlled at laparotomy.
• Failure of nonoperative management of liver injuries (with or without radiologic interventional therapy) usually predicts a significant morbidity and mortality.
• Except in children, the amount of blood transfused does not precisely define stability in the absence of hypotension.
BIBLIOGRAPHY
1. Gett RM, McMahon D: Cut to cure? Blunt hepatic trauma. ANZ J Surg. 73 Supplement 1:A115, May 2003.
2. Strong RW: Operative versus non-operative management of blunt liver trauma. ANZ J Surg 73 Supplement 1:A113, May 2003.
3. Malhotra AK, Fabian TC, Croce MA, et al: Blunt hepatic injury: a paradigm shift from operative to nonoperative management in the 1990s. Ann Surg 231:804-13, 2000.
4. Richardson JD, Franklin GA, Lukan JK, et al: Evolution in the management of hepatic trauma: a 25-year perspective. Ann Surg 232:324-30, 2000.
5. Holland, AJ, Davey, RB, Sparnon AL Chapman M, LeQuesne, GW: Traumatic pancreatitis: long-term review of initial non-operative management in children. J Paediatr Child Health. 35(1):78-81, February 1999.
6. Carrillo, EH, Platz A, Miller, FB, Richardson, JD, Polk, HC Jr. Non-operative management of blunt hepatic trauma. Br J Surg. 85:461-8, April 1998.
7. Matthews LA, Smith EM, Spirnak JP: Nonoperative treatment of major blunt renal lacerations with urinary extravasation. J Urol 157:2056-8, 1997.
8. Powell M, Courcoulas A, Gardner M, et al: Management of blunt splenic trauma: significant differences between adults and children. Surgery 122:654-60, 1997.
9. Pachter HL, Knudson MM, Esrig B, et al: Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 40:31-8, 1996.
10. Smith JS, Cooney RN, Mucha P: Nonoperative management of the ruptured spleen: a revalidation of criteria. Surgery 120:745-50, discussion 750-1, 1996.
11. Boone DC, Federle M, Billiar TR, et al: Evolution of management of major hepatic trauma: identification of patterns of injury. J Trauma 39:344-50, 1995.
12. Croce MA, Fabian TC, Menke PG, et al: Nonoperative management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients. Ann Surg 221:744-53, discussion 753-5, 1995.
13. Morrell DG, Chang FC, Helmer SD: Changing trends in the management of splenic injury. Am J Surg 170:686-9, 1995.
14. Pachter HL, Hofstetter ST: The current status of nonoperative management of adult blunt hepatic injuries. Am J Surg 169:442-54, 1995.
15. Sclafani SJA, Shaftan GW, Scalea TM, et al: Nonoperative salvage of computed tomography-diagnosed splenic injuries: utilization of angiography for triage and embolization for hemostasis. J Trauma 39:818-25,discussion 826-7, 1995.
16. Sutyak JP, Chiu WC, D’Amelio LF, et al: Computed tomography is inaccurate in estimating the severity of adult splenic injury. J Trauma 39:514-8, 1995.
17. Cheng DL, Lazan D, Stone N: Conservative management of type III renal trauma. J Trauma 36:491-4, 1994.
18. Gates JD: Delayed hemorrhage with free rupture complicating the nonsurgical management of blunt hepatic trauma: a case report and review of the literature. J Trauma 36:572-5. Review, 1994.
19. Meredith JW, Young JS, Bowling J, et al: Nonoperative management of blunt hepatic trauma: the exception or the rule? J Trauma 36:529-34, discussion 534-5, 1994.
20. Husmann DA, Gilling PJ, Perry MO, et al: Major renal lacerations with a devitalized fragment following blunt abdominal trauma: comparison between nonoperative (expectant) versus surgical management. J Urol 150:1774-7, 1993.
21. Croce MA, Fabian TC, Kudsk KA, et al: AAST organ injury scale: correlation of CT-graded liver injuries and operative findings. J Trauma 31:806-12, 1991.
22. Cogbill TH, Moore EE, Jurkovich JJ, et al: Nonoperative management of blunt septic trauma: a multicenter experience. J Trauma 29:1312-7, 1989.
23. Schiffman MA: Nonoperative management of blunt abdominal trauma in pediatrics. Emerg Med Clin North Am 7:519-35, 1989.
Panam J Trauma 2004, 11:1
9
DELAYED LAPAROTOMY - WHAT NOW?David Feliciano, MD, FACS.
Chief of Surgery, Grady Memorial Hospital. Professor of Surgery, Emory University School of Medicine Atlanta, Georgia
One major consequence of the expanding percentage of patients undergoing nonoperative management of solid organ injuries is the decreasing number of operations in which resection or repair is performed. In particular, this is a troublesome problem for the current generation of surgical residents where much of their elective operative experience includes laparoscopic procedures rather than laparotomies.
REASONS FOR FAILURE OF NONOPERATIVE MANAGEMENT
The first reason for failure of nonoperative management is underrecognition of the magnitude of injury on the initial spiral CT scan. Underestimation of the depth of a laceration or the size of a hematoma, failure to recognize intraparenchymal extravasation of intravenous contrast, and overlooking the presence of blood in the pelvis have occurred in all major trauma centers over the past 15 years.1-3 The use of multidetector CT scanners may eliminate many of these problems in the future.4
The second reason for failure is poor judgment of the attending surgeon. Patients with profound hypotension (systolic BP < 70 mm) in the field or in the emergency center, repeated episodes of hypotension in the emergency center or CT scanner despite fluid resuscitation, or the need for 2-4 units of RBC transfusion in the first 24 hours after admission are unlikely to have successful nonoperative management. Adult patients with AAST OIS Grade IV ruptures of the spleen and a “large” hemoperitoneum will fail nonoperative management alone (without angioembolization) 80-90% of the time.5 And, it should be restated that 2/3 of the patients who required operative
intervention after failure of nonoperative management of a blunt hepatic injury in Pachter’s multi-institutional review had Grade IV or V injuries.6 All of us can only hope that the 70% preventable or potentially preventable record of deaths in the EAST multi-institutional study of nonoperative management of splenic injuries by A. Pietzman et al will never be repeated.7
INDICATIONS FOR AND OUTCOME OF DELAYED LAPAROTOMY
Splenic Injuries
In-hospital signs of failure of nonoperative management of the spleen include the following:8
1. ↓ Hematocrit, tachycardia, ± hypotension in the first48 hr of observation2. >2 units packed red blood cell transfusion needed in patient with isolated splenic injury3. ↑ Abdominal pain and tenderness4. Changes on emergency abdominal computed tomography
• New extravasation of intravenous contrast into a parenchymal laceration or outside the spleen• Significant increase in size of original hemoperitoneum• Significant expansion or new rupture of subcapsular hematoma
Angioembolization would be appropriate in any of these instances, if the patient’s hemodynamic status can be maintained while the interventional angiography team returns to the hospital.
Panam J Trauma
10 Marzo 2004
Delayed Laparotomy - What Now?
11Vol. 11 Number 1
Another approach has been to perform splenic arteriography in all patients after the contrast-enhanced spiral CT has been performed. In the study by Shanmuganathan et al,9 five of 78 patients (6%) failed nonoperative management after both of these studies were performed. Two of these patients had no evidence of contrast extravasation on the original two studies; two had vascular lesions (1 extravasation, 1 pseudoaneurysm) that were not embolized as there was no “focal vascular injury” on the arteriogram; and the remaining patient had embolization of a pseudoaneurysm and areas of extravasation shortly after admission. All five of these patients had a splenectomy performed.
In the pre-embolization period, the study by Cogbill et al10 is of particular interest. Nonoperative management was performed in 112 patients (40 < 16 years old; 72 adults) at six referral trauma centers. Failure of nonoperative therapy occurred in one child (2%) and in 12 adults (17%) and was due to ongoing hemorrhage in 12 patients and delay recognition of a pancreatic injury in one. Splenic salvage (splenorrhaphy) was accomplished in seven of the 12 patients (58%) undergoing delayed operation for ongoing hemorrhage. While splenorrhaphy is performed infrequently in modern trauma centers, extensive descriptions of operative techniques are available in the surgical literature.8,11
Other than hemorrhage or delayed recognition of other intra-abdominal injuries, the other indication for a delayed operation is the presence of a posttraumatic splenic cyst. In the report by Pachter et al12 in 1993, the authors recommended that cysts > 5 cm in diameter should undergo some form of therapy. While the authors discussed the likelihood that percutaneous drainage would be worthwhile in most patients in the future, they performed open resection of the cyst-bearing position of the spleen with successful splenic preservation in all seven instances. In the modern era, a laparoscopic approach would be appropriate s/p failed aspiration, recognizing that there will be significant inflammation in the left upper quadrant.
HEPATIC INJURIES
Failure of nonoperative management of hepatic injuries has been reported to occur in 1-18% patients, but has
averaged 2-5% when larger patient series are reviewed.13 In the review by Carrillo et al13, a large number of complications including some that might require a delayed operation were described:
Early
• Recurrent or persistent bleeding• Pulmonary complications (atelectasis, pneumonia)• Initial unrecognized associated injuries• Liver infection (perihepatic sepsis, liver abscess)• Hyperpyrexia and systemic inflammatory response• Extrahepatic biliary ductal disruption and biliary
fistulas• Jaundice and adynamic ileus Late
• Intrahepatic vascular fistulas (i.e., hemobilia, bilhemia)
• Biliary ductal strictures• Persistent biliary fistulas • Subcapsular hematomas• Posttraumatic liver cyst
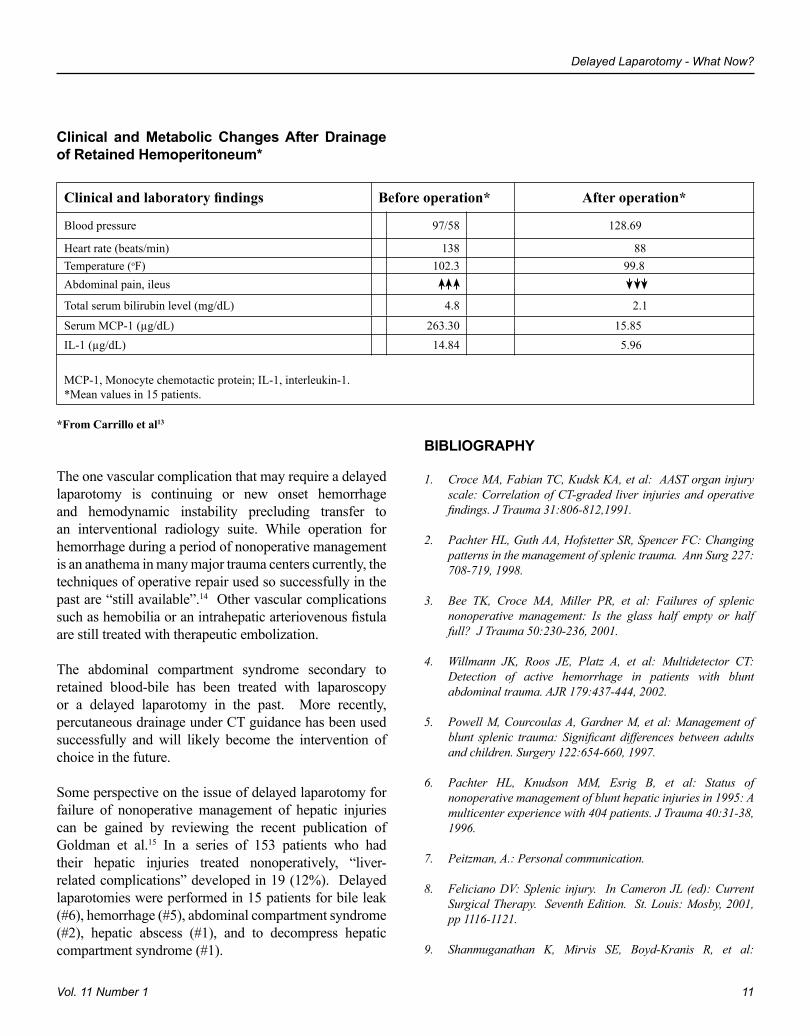
As with the previously described failures of nonoperative management of splenic injuries, many of the problems listed above are managed by the interventional radiologist. Therefore, delayed laparotomy will be necessary in only 10-15% of patients with failure of nonoperative management of a hepatic injury. Biliary complications that require intervention include a perihepatic or intrahepatic abscess, biliary fistula, posttraumatic cysts, toxicity syndrome of retained intraperitoneal blood and bile, missed extrahepatic ductal injury, and late stricture of extrahepatic duct. Indications for delayed operation include failure of radiological intervention of any of these entities, especially missed extrahepatic ductal injury or late ductal stricture, or failure of laparoscopic drainage of retained intraperitoneal bile. Carrillo et al13 have emphasized early laparoscopy to remove large peritoneal blood and bile collections and have shown dramatic clinical improvement in such situations:
Panam J Trauma
10 Marzo 2004
Delayed Laparotomy - What Now?
11Vol. 11 Number 1
BIBLIOGRAPHY
1. Croce MA, Fabian TC, Kudsk KA, et al: AAST organ injury scale: Correlation of CT-graded liver injuries and operative findings. J Trauma 31:806-812,1991.
2. Pachter HL, Guth AA, Hofstetter SR, Spencer FC: Changing patterns in the management of splenic trauma. Ann Surg 227:708-719, 1998.
3. Bee TK, Croce MA, Miller PR, et al: Failures of splenic nonoperative management: Is the glass half empty or half full? J Trauma 50:230-236, 2001.
4. Willmann JK, Roos JE, Platz A, et al: Multidetector CT: Detection of active hemorrhage in patients with blunt abdominal trauma. AJR 179:437-444, 2002.
5. Powell M, Courcoulas A, Gardner M, et al: Management of blunt splenic trauma: Significant differences between adults and children. Surgery 122:654-660, 1997.
6. Pachter HL, Knudson MM, Esrig B, et al: Status of nonoperative management of blunt hepatic injuries in 1995: A multicenter experience with 404 patients. J Trauma 40:31-38, 1996.
7. Peitzman, A.: Personal communication.
8. Feliciano DV: Splenic injury. In Cameron JL (ed): Current Surgical Therapy. Seventh Edition. St. Louis: Mosby, 2001, pp 1116-1121.
9. Shanmuganathan K, Mirvis SE, Boyd-Kranis R, et al:
Clinical and Metabolic Changes After Drainage of Retained Hemoperitoneum*
Clinical and laboratory findings Before operation* After operation*
Blood pressure 97/58 128.69
Heart rate (beats/min) 138 88Temperature (oF) 102.3 99.8Abdominal pain, ileus
Total serum bilirubin level (mg/dL) 4.8 2.1
Serum MCP-1 (µg/dL) 263.30 15.85IL-1 (µg/dL) 14.84 5.96
MCP-1, Monocyte chemotactic protein; IL-1, interleukin-1.*Mean values in 15 patients.
*From Carrillo et al13
The one vascular complication that may require a delayed laparotomy is continuing or new onset hemorrhage and hemodynamic instability precluding transfer to an interventional radiology suite. While operation for hemorrhage during a period of nonoperative management is an anathema in many major trauma centers currently, the techniques of operative repair used so successfully in the past are “still available”.14 Other vascular complications such as hemobilia or an intrahepatic arteriovenous fistula are still treated with therapeutic embolization.
The abdominal compartment syndrome secondary to retained blood-bile has been treated with laparoscopy or a delayed laparotomy in the past. More recently, percutaneous drainage under CT guidance has been used successfully and will likely become the intervention of choice in the future.
Some perspective on the issue of delayed laparotomy for failure of nonoperative management of hepatic injuries can be gained by reviewing the recent publication of Goldman et al.15 In a series of 153 patients who had their hepatic injuries treated nonoperatively, “liver-related complications” developed in 19 (12%). Delayed laparotomies were performed in 15 patients for bile leak (#6), hemorrhage (#5), abdominal compartment syndrome (#2), hepatic abscess (#1), and to decompress hepatic compartment syndrome (#1).
Panam J Trauma
12 Marzo 2004
Nonsurgical management of blunt splenic injury: Use of CT criteria to select patients for splenic arteriography and potential endovascular therapy. Radiology 217:75-82, 2000.
10. Cogbill TH, Moore EE, Jurkovich GJ, et al: Nonoperative management of blunt splenic trauma: A multicenter experience. J Trauma 29:1312-1317, 1989.
11. Feliciano DV, Spjut-Patrinely V, Burch JM, et al: Splenorrhaphy. The alternative. Ann Surg 211:569-582, 1990.
12. Pachter HL, Hofstetter SR, Elkowitz A, et al: Traumatic cysts of the spleen -- the role of cystectomy and splenic preservation:
Experience with seven consecutive patients. J Trauma. 35:430-436, 1993.
13. Carrillo EH, Wohltmann C, Richardson JD, Polk HC Jr: Evolution in the treatment of complex blunt liver injuries. Curr Prob Surg 38:1-60, 2001.
14. Feliciano DV, Pachter HL: Hepatic trauma revisited. Curr Prob Surg 26:453-524, 1989.
15. Goldman R, Zilkoski M, Mullins R, et al: Delayed celiotomy for the treatment of bile leak, compartment syndrome, and other hazards of nonoperative management of blunt liver injury. Am J Surg 185:492-497, 2003.
Panam J Trauma 2004, 11:1
13
INTESTINAL FISTULAS: TECHNICAL TIPS FOR SUCCESSFUL CLOSUREGlen Tinkoff, MD, FACS.
Director, Trauma Services Christiana Care Health System. Wilmington, Delaware
A fistula is a passage from an organ to an epithelial surface or from one organ to another formed by disease or injury. Although several potential anatomic sites are subject to fistula formation after penetrating trauma, postoperative intestinal fistulas are one of the most challenging complications for a general surgeon to manage. Although often the result of well-intentioned surgical intervention, a postoperative intestinal fistula usually represents a technical failure, with potential catastrophic consequences for the patient. Only a well-thought-out and principled approach to diagnosis and management of this humbling postoperative complication will afford the patient the opportunity for full recovery with intestinal continuity.
ETIOLOGY
Any circumstance that leads to a full-thickness defect in the bowel wall and interferes with normal healing may lead to fistula formation. Although certain systemic abnormalities may be factors (e.g., diabetes, sepsis, malignancy, steroids, chemotherapy, malnutrition, renal failure), most fistulas (85%) are caused by technical failures. These surgical mishaps include direct bowel injury from dissection or foreign body, anastomotic failure, and mesenteric devascularization.
Although little published data are available specific to the development of intestinal fistulas in the penetrating trauma patient, these same factors are involved. Furthermore, the widely accepted damage-control techniques for the resuscitation and recovery of the
critically injured penetrating trauma victim, including planned dehiscence, have a significant rate of fistula occurrence of 10% to 50%. These fistulas are usually caused by the application of nonabsorbable mesh or gauze material directly onto the bowel during management of the open wound. However, even with protection of the underlying bowel, fistulas can still occur.
DIAGNOSIS AND STABILIZATION
Intestinal fistulas that occur during the postoperative course of the trauma patient with a penetrating abdominal injury usually appear late in the first week after initial laparotomy. The patient develops fever and a persistent ileus. Enteric contents may eventually appear on the wound dressing, or an intra-abdominal abscess may develop. Patients requiring planned dehiscence and management of an open abdominal wound as a damage-control measure may display an obvious external fistula. It is tempting to address such a fistula primarily; however, direct suture repair is often futile and can lead to additional intestinal injury.
At the time of fistula presentation, the patient will often display profound metabolic dyscrasia, with clinical signs of sepsis, fluid and electrolyte disturbances, and malnutrition. Such a patient must undergo intravenous volume resuscitation guided by hemodynamic monitoring and repletion of electrolytes. Institution of nutritional support should follow. In most instances, this support should be via total parenteral nutrition. Nitrogen balance and visceral protein markers (e.g., albumin, transferrin, prealbumin) should be assessed routinely. Early computed tomographic (CT) imaging with percutaneous drainage of the collections and broad-spectrum antibiotic coverage are valuable adjuncts to
Panam J Trauma
14 Marzo 2004
Intestinal Fistulas: Technical Tips for Successful Closure
15Vol. 11 Number 1
early management. Surgical drainage and debridement should be performed as indicated.
CONTROL OF FISTULA DRAINAGE AND LOCAL WOUND CARE
Fistula drainage must be controlled, collected, and quantified to attain optimal outcome for these difficult-to-manage patients. High-output fistulas (> 500 mL/day) and fistulas associated with large, open wounds can be particularly challenging in this regard. Early in the course of the patient with a developing fistula, simple ostomy bagging should be avoided, as skin closure can occur over the newly forming tract, leading to underlying abscess formation. Insertion of a soft, sump-type drain into the forming fistula tract with applied suction, when possible, is optimal to control and collect the drainage. External drainage associated with large, open wounds does not allow for simple drain insertions. Techniques that protect the underlying granulating wound bed while allowing closed suction drainage (such as the VacPac system) or a large wound drainage bag can be applied. H2 blockers and octreotide (a somatostatin analogue) can be utilized as pharmacologic adjuncts to reduce fistula output. In instances in which fistula output must be controlled completely, such as to manage a septic wound, proximal diversion can be considered if feasible.
With all techniques for fistula control, meticulous local skin care needs to be maintained to prevent the maceration and breakdown of the integument from exposure to digestive enzymes. The enterostomal therapy nurse is a valuable member of the healthcare team and should be consulted early in the patient’s course. Preparations such as Stomahesive, DuoDERM, or karaya paste should be used routinely for skin protection.
RADIOLOGIC INVESTIGATION/DETERMINATION OF SPONTANEOUS CLOSURE
After stabilization, fistulography with water-soluble contrast material should be performed to define the anatomy and characteristics of the fistula tract. Fistula length, width, and complexity, bowel continuity, lateral versus end location, associated abscess cavities, condition
of the adjacent bowel, and presence of distal obstruction can be ascertained. CT imaging should be used liberally to address any potential underlying collections, which may prolong the duration of recovery.
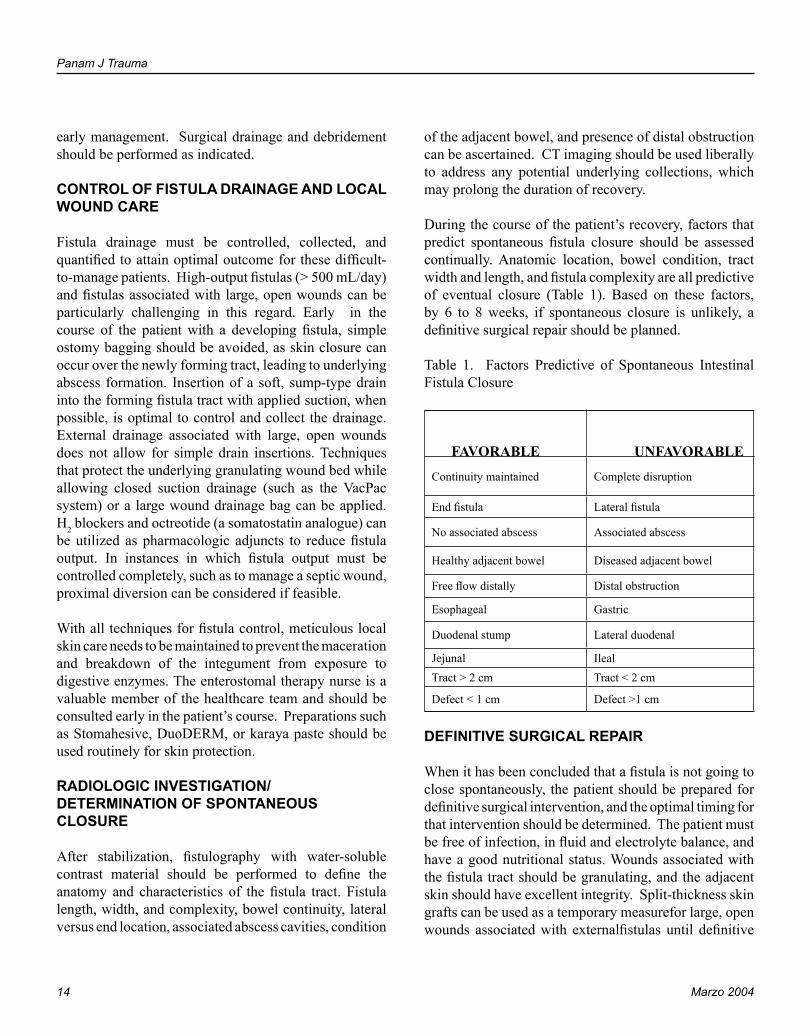
During the course of the patient’s recovery, factors that predict spontaneous fistula closure should be assessed continually. Anatomic location, bowel condition, tract width and length, and fistula complexity are all predictive of eventual closure (Table 1). Based on these factors, by 6 to 8 weeks, if spontaneous closure is unlikely, a definitive surgical repair should be planned.
Table 1. Factors Predictive of Spontaneous Intestinal Fistula Closure
UNFAVORABLE
Continuity maintained Complete disruption
End fistula Lateral fistula
No associated abscess Associated abscess
Healthy adjacent bowel Diseased adjacent bowel
Free flow distally Distal obstruction
Esophageal Gastric
Duodenal stump Lateral duodenal
Jejunal IlealTract > 2 cm Tract < 2 cm
Defect < 1 cm Defect >1 cm
DEFINITIVE SURGICAL REPAIR
When it has been concluded that a fistula is not going to close spontaneously, the patient should be prepared for definitive surgical intervention, and the optimal timing for that intervention should be determined. The patient must be free of infection, in fluid and electrolyte balance, and have a good nutritional status. Wounds associated with the fistula tract should be granulating, and the adjacent skin should have excellent integrity. Split-thickness skin grafts can be used as a temporary measurefor large, open wounds associated with externalfistulas until definitive
FAVORABLE

Panam J Trauma
14 Marzo 2004
Intestinal Fistulas: Technical Tips for Successful Closure
15Vol. 11 Number 1
surgical repair can be performe.
Several less invasive maneuvers have been described to attain fistula closure without the need for another laparotomy. Recently, tissue adhesives have been directly or endoscopically applied to simple fistula tracts with some success. However, this technique is not appropriate for complex fistulas or for those associated with large, open wounds. For these situations, direct closure of the fistulas with mucosal and serosal closure using sutures or a sutureless bio-fragmentable ring covered by a split-thickness skin graft can be considered. The use of tissue adhesives placed over a cadaveric acellular dermal patch (AlloDerm) and applied to fistula sites within open wounds has also been described.
However, most patients a repeat laparotomy will be necessary to re-establish intestinal continuity. This procedure should be undertaken only when signs of the prior obliterative peritonitis are resolved, which can be determined by physical examination, by the observation of a “pinchable” split-thickness skin graft over the open wound. The patient’s abdomen should be soft and pliable. Digital examination of the fistula, if possible, or the presence of a “pinchable” skin graft used for temporary closure allows accurate assessment of the pliability and softness of the intra-abdominal contents and the readiness of the fistula for surgical closure.
Reoperation for fistula closure is tedious and time-consuming and requires meticulous technique and hemostasis. These operations should usually be performed early in the day, with ample time allotted and experienced assistance. Prophylactic antibiotics should be administered to the patient. The abdominal wall, including the fistula site, should be thoroughly prepared, and the open draining area should be covered with gauze secured in place with a large transparent adhesive drape.
If at all possible, the abdomen should be entered in an area free of prior entry. Upon entering the abdomen, care must be taken not to reinjure underlying bowel. Once the peritoneal cavity is entered, dissection is performed under the abdominal scar, usually midline and then onto both flanks. During the course of dissection, identifiable loops of small bowel are sought and are used to guide the adhesiolysis toward discernible anatomic locations,
such as the ligament of Treitz and terminal ileum, as well as toward the fistulous segment. The entire length of small intestine should be dissected and the fistula site resected, leaving two healthy ends of small bowel for reanastomosis. Hand- sewn single-layer anastomosis is personally preferred. The anastomosis is protected with an omental patch or a tissue adhesive. The peritoneal cavity is copiously irrigated. In rare instances when dissection is impossible, an intestinal bypass can be created.
Often, abdominal wall closure requires reconstructive techniques. These techniques include rectus component separation or muscle flaps. Defects can also be managed with cadaveric acellular dermal patches (AlloDerm) as primary repair or onlay. Synthetic patches are less preferable because of the presence of open bowel. Subcutaneous drains are used if skin and subcutaneous tissue are undermined to attain closure.
A prolonged postoperative course should be anticipated, marked by prolonged ileus and significant pain control issues. The patient should be assessed continually to prevent wound breakdown, bowel obstruction, and intra-abdominal sepsis. Intravenous nutritional support should be maintained during this critical period to optimize recovery. Rehabilitative therapies are often required before the patient can regain full independent status.
BIBLIOGRAPHY
1. Berry SM, Fischer JE: Enterocutaneous fistula. Curr Probl Surg 81:469-566, 1994
2. Duvicnian, GA, et al: Postoperative abdominal wall defects wth enterocutaneous fisutlas. Am J Surg 172:223, 1996
3. Edmunds LH, Williams GM, Welch CE: External fistulas arising from the gastrointestinal tract. Ann Surg 152:4445, 1960
4. Fazio VW (ed): Alimentary Tract Fistulas. World J of Surg 7:445, 1983
5. Girard, S, Sideman, M, Spain, PA. A novel approach to the problem of intestinal fistulization in patients with open peritoneal cavities. Am J Surg 184:166, 2003
6. Maguid MM, Campos AC (eds): Surgical Management of
Panam J Trauma
16 Marzo 2004
Gastrointestinal Fistulas. Surg Clin North Am Volume 76, October 1996.
7. Lee, JT: Reoperative care of postoperative external fistulas: stomach, pancreas, intestine. In McQuarrie, DE, Humphrey, EW, Lee, JT: Reoperative General Surgery, 2nd edition, St. Louis, MO, Mosby pps 432-462.
8. Orringer JS, Mendeloff EN, Eckhauser FE: Management of wounds in patient with complex enterocutaneous fistulas. Surg Gynecol Obstet 165:79-80, 1987.
9. Rubelowsky J, Machiedo GW: Reoperative versus conservative management for gastrointestinal fistulas. Surg Clin North Am 71:147-157, 1991.
10. Sarfeh IJ, Jaleowatz, JG. Surgical treatment of enteric “bud” fistulas in contaminated wounds. Arch Surg 127:1027, 1992.
11. Shand, A, Pendlebury, J: Endoscopic injection of human fibrin sealant – a novel method for closure of resistant intestinal fistula. Gut 140 (sup 1):105A, 1999.
12. Sitges-Serra A, Jaurrieta E, Sitges-Creus A: Management of postoperative enterocutaneous fistulas: the roles of parenteral nutrition and surgery. Br J Surg 69:147-150, 1982.
13. Soeters PB, Ebeid AM, Fischer JE: Review of 404 patients with gastrointestinal Fistulas. Impact of parenteral nutrition. Ann Surg 190:189-202, 1979.
Panam J Trauma 2004, 11:1
17
KIDS AND COMPLICATIONS - WHAT YOU NEED TO KNOWDavid P. Mooney, MD, FACS.
Assistant Professor of Surgery, Director, Trauma Program Children’s Hospital Boston, Boston, Massachusetts
Trauma remains the number one cause of morbidity and mortality among children, each year claiming more lives than all other causes combined. The number of children dying from injury, however, is decreasing each year, as are the number of children admitted to hospitals for the care of an injury. While children may still present to the nearest hospital for emergency care, when stable they are often transferred to a regional pediatric center for admission. Unstable children may not tolerate transfer and their care falls upon the center of first presentation. Diminished frequency of exposure, but to the most critically injured children places an increasing burden on providers at non-pediatric trauma facilities to remain current with pediatric trauma care. Critical analysis of the incidence of complications among injured children finds that the percentage of children suffering a complication after injury is no different than has been noted for adults. Fortunately, most complications do not result in long-term sequelae, but significant problems persist.
Airway complications continue to plague injured children. Up to 1/3 of children who die of a traumatic brain injury die from a secondary brain injury from lack or loss of their airway, and not from their primary injury [1]. Airway problems abound in the pre-hospital arena, where, in many jurisdictions, the infrequency of pediatric intubation makes it nearly impossible for individual practioners to maintain their skills. A shift in focus toward airway management and not intubation has followed publication of two studies that demonstrated
no improvement in survival for intubated children over those who received bag-valve-mask ventilation [2] [3].
It is normal for children to become sleepy after even minor traumatic brain injury. Often children are intubated prior to transportation to a pediatric trauma center secondary to fears of lost airway en route. The risks of loss of airway control must be carefully weighed against the risks of intubation prior to this maneuver. Much of the difficulty with pediatric airway management involves differences in pediatric airway anatomy and the variety of equipment sizes necessary to care for injured children. Organization systems have simplified the equipment selection process, but have not been fully integrated across the spectrum of care.
Variation in pediatric body weights may lead to inappropriate fluid management. Children require heightened attention to the infusion rate per kilogram of body weight and to the volume of fluid boluses. Excessive fluid administration may lead to pulmonary edema and has been reported to cause secondary abdominal compartment syndrome. Sadly, a common error still involves the use of weight in pounds versus kilograms. This may quickly lead to an erroneous doubling of fluid and medication doses.
Injured children may require sedation for radiologic or other procedures, such as fracture reduction. This situation places the patient at significant risk for airway complications, especially if the procedure is performed by personnel without sufficient training in pediatric sedation or is performed distant from the Emergency Department [4]. With the advent of rapid CT scanning techniques, sedation for diagnostic procedures may often be achieved through parental comforting. Sedatives used

Panam J Trauma
18 Marzo 2004
Kids and Complications - What you Need to Know
19Vol. 11 Number 1
for this purpose may become more effective after the procedure and lead to hypoventilation and hypoxia. Also, if the institution still uses enteral contrast material for abdominal CT scans, a practice dismissed over 15 years ago at Children’s Hospital Boston, the patient is at significant risk for vomiting and aspiration while sedated and supine.
Brain injury remains an unsolved problem and is responsible for the majority of trauma-related death and disability. The association between clinical management and brain injury outcome remains elusive, but for certain variables. Hypotension and hypoxemia have been associated with a worse outcome after traumatic brain injury [5].
Nonoperative management has become the standard of care for hemodynamically stable children with solid organ injuries. Somewhere between 0.1 and 6 % of these children will suffer from a bowel injury that requires laparotomy [6]. The differentiation between these two conditions is difficult and requires frequent observations over several hours. Secondary to nonoperative management the diagnosis of bowel injury may be delayed, but the clinical importance of a delay in diagnosis does not appear to be as significant as previously thought [7]. CT findings consistent with bowel injury, other than free air, may not correlate with the need for laparotomy, and many resolve without operation.
Orthopedic injuries remain the number one reason for hospitalization after injury in children. Complications, fortunately, are unusual. Volkman’s ischemic contracture may be associated with supracondylar humeral fracture and these fractures require both prompt surgical attention and special operative techniques to diminish this risk. The majority of the vascular compromise associated with orthopedic injury resolves on reduction of the fracture, which should be attempted prior to vascular diagnostic maneuvers. Pelvic fractures are associated with more significant long-term morbidity than previously realized and attention must be paid to the lingering effects of these injuries [8]. The short-term mortality, though, is much less than in adults and issues such as urethral disruption are rare in childhood.
One of the worst conceivable complications is a neurologically significant missed cervical spine injury. Cervical spine clearance is a clinical decision that may be assisted by, but not performed by, diagnostic imaging. Many different techniques have been proposed for clearing the cervical spine. Each technique, however, will have a certain percentage of false negative and positive studies that will commit the child to either another study, which may require sedation or general anesthesia, or to a prolonged period of time in a collar.
Venous thromboemboli and pulmonary emboli occur much less often in injured children than in adults. In a large series of injured children, the incidence of diagnosed venous thromboemboli and pulmonary emboli was 0.08% and 0.012% respectively [9]. Given that the major bleeding complication rate for subcutaneous heparin and low molecular weight heparin prophylaxis ranges from 1 to 4% in adults (Thomson MICROMEDEX, 2002), serious consideration should be given to whether these medications are appropriate in this situation. Select children, such as those with spinal cord injury, may be at higher risk of VTE and prophylaxis should be considered.
Post-traumatic stress disorder is the most common complication of childhood injury and may be the least often recognized. Psychologic sequelae after injury may occur in up to 1/3 of hospitalized children, and doesn’t appear to directly correlate with the severity or mechanism of their injury [10]. This unfortunate problem may become worse than the physical sequelae of the injury and may have permanent effects. Maneuvers such as parental presence at resuscitations, play therapists and avoidance of painful procedures that may not be necessary may help prevent this problem.
Complications occur as often in injured children as in injured adults. Careful attention to the differences between adult and pediatric trauma patients may avoid the most serious of these problems.
BIBLIOGRAPHY
Physicians’ Desk Reference
1. Chiaretti, A., et al., The impact of initial management on the
Panam J Trauma
18 Marzo 2004
Kids and Complications - What you Need to Know
19Vol. 11 Number 1
outcome of children with severe head injury. Childs Nervous System., 2002. 18(1-2): p. 54-60.
2. Cooper, A., et al., Prehospital endotracheal intubation for severe head injury in children: a reappraisal. Seminars in Pediatric Surgery., 2001. 10(1): p. 3-6.
3. Gausche, M., et al., Effect of out-of-hospital pediatric endotracheal intubation on survival and neurological outcome: a controlled clinical trial.[comment][erratum appears in JAMA 2000 Jun 28;283(24):3204]. Jama., 2000. 283(6): p. 783-90.
4. Sedik, H., Use of intravenous methohexital as a sedative in pediatric emergency departments. Archives of Pediatrics & Adolescent Medicine., 2001. 155(6): p. 665-8.
5. Dearden, N.M., Mechanisms and prevention of secondary brain damage during intensive care. Clinical Neuropathology., 1998. 17(4): p. 221-8.
6. Morse, M.A. and V.F. Garcia, Selective nonoperative
management of pediatric blunt splenic trauma: risk for missed associated injuries. Journal of Pediatric Surgery., 1994. 29(1): p. 23-7.
7. Bensard, D.D., et al., Small bowel injury in children after blunt abdominal trauma: is diagnostic delay important? Journal of Trauma-Injury Infection & Critical Care., 1996. 41(3): p. 476-83.
8. Upperman, J.S., et al., Early functional outcome in children with pelvic fractures. Journal of Pediatric Surgery., 2000. 35(6): p. 1002-5.
9. Vavilala, M.S., et al., Risk factors for venous thromboembolism in pediatric trauma. Journal of Trauma-Injury Infection & Critical Care., 2002. 52(5): p. 922-7.
10. Daviss, W.B., et al., Acute stress disorder symptomatology during hospitalization for pediatric injury. Journal of the American Academy of Child & Adolescent Psychiatry., 2000. 39(5): p. 569-75.
Panam J Trauma 2004, 11:1
20
NonOperative Management of Gunshot Wounds
21Vol. 11 Number 1
NONOPERATIVE MANAGEMENT OF GUNSHOT WOUNDSThomas M. Scalea, MD, FACS.
Physician-in-Chief, R Adams Cowley Shock Trauma Center Francis X. Kelly / MBNA Professor of Trauma Surgery.Director, Program in Trauma, University of Maryland School of Medicine Baltimore, Maryland
Nonoperative management has become the norm in most patients with blunt torso trauma. Blunt trauma applies diffuse force and may be applied to a number of body cavities. There are no clear entrance or exit wounds. Thus, investigation must cast a relative wide net. Fortunately, the injuries most commonly caused by blunt trauma to the chest and abdomen are reliably identified with standard imaging techniques such as the combination of plain x-ray and CT scanning. This allows for grading of injury as well as identification, and allows rational planning for nonoperative management.
In the case of penetrating trauma, the zone of injury is much more focused. Entrance and exit wounds identify areas of concern, but it is important to remember that bullets may not travel in a straight line. In addition, the concussive effects of blast injury from high velocity missiles increases the potential zone of injury. Unfortunately, diagnostic testing is not as robust as it is for blunt force trauma. Thus, suspicion for injury is based on proximity following gunshot wounds. The imperfect diagnostic techniques in the past made surgeons believe that exploration was often necessary to either exclude or identify all injuries.
The notion that exploration is necessary to exclude injury began to be questioned nearly 15 years ago in the diagnosis of peripheral vascular trauma. Up until then, screening angiography was felt to be necessary to exclude injury in patients whose missile past in proximity to a major blood vessel. This was an invasive
and costly screening exam, particularly in patients without hard or soft signs of vascular injury. This highest yield of screening angiography for reported was 6%.1 Frykberg et al has clearly demonstrated that careful physical examination reliably excludes vascular injury.2 Most trauma centers have abandoned the use of pure proximity angiography now rely on a combination of physical examination and measurement of ankle brachial indices.
This concept of serial physical examination has been extended to other areas such as penetrating neck injury. Injury to Zones 1 and 3 of the neck require evaluation for the potential of vascular as well as aerodigestive injury. Physical examination may miss injury in these areas particularly in Zone 1. However, Zone 2 of the neck is much more assessable for careful physical examination. Early reports suggested that physical exam was inadequate in determining the presence of vascular injury in the neck.3 Other recent work suggests serial exams are reliable.4 In addition, Demetriades and his colleagues have investigated a large number of penetrating neck injuries.5 None of the 160 patients without clinical signs of vascular injury had vascular injuries requiring treatment. The authors believe that physical examination is reliable for identifying in patients with penetrating injury to the neck that requires further diagnostic study. It is important to note that in this prospective study, a careful physical exam was performed according written protocol and the result recorded. Patients were observed overnight to prevent missed injury.
Nonoperative management techniques have been extended to the torso as well. A single physical examination of the abdomen is often inadequate to make the diagnosis of intra-abdominal injury. Small bowel

Panam J Trauma 2004, 11:1
20
NonOperative Management of Gunshot Wounds
21Vol. 11 Number 1
injuries may not be manifested on physical exam, initially. Patients who sustain gunshot wounds may themselves be intoxicated or in some other way not be reliable. Other more objective diagnostic testing is generally utilized. Many clinicians believe that virtually all patients with transabdominal gunshot wounds have injuries requiring operation. Thus, conventional wisdom is to determine the presence of absence of transabdominal trajectory and explore all patients with proven or suspected transabdominal gunshot wounds. Adjunctive techniques such as diagnostic peritoneal lavage can be utilized to determine the presence of transabdominal trajectory.
More recently, a more selective approach has been proposed. Serial physical exams are an acceptable manner to evaluate patients with anterior abdominal stab wounds. Serial exams have successfully been employed in patients with gunshot wounds.6 Recently, Valmahos et al reviewed over 1,800 patients with abdominal gunshot wounds over an eight-year period.7 These patients were managed by protocol. Those that did not have peritonitis were hemodynamically stable and had reliable clinical exam were observed. Only 4% of those followed developed symptoms and required delayed laparotomy. Only 0.3% suffered complications potentially related to the delay in laparotomy. Thirty-eight percent of the patients who would have previously undergone diagnostic abdominal exploration were successfully managed nonoperatively.
This strategy requires personnel and hospital resources be available to carefully follow patients. Other investigative techniques can help evaluate the possibility of intra-abdominal injury. In the 1980s, CT scanning revolutionized the nonoperative management of blunt trauma. In 1986, triple contrast CT scanning was first described, demonstrating the utility of CT in patients with penetrating trauma.8 In this study, however, CT was used only to image the retroperitoneum. The possibility of intra-abdominal injuries was evaluated through diagnostic peritoneal lavage. More recently, focused ultrasound exam has been used to evaluate patients with blunt trauma. Both of these techniques have recently been evaluated in patients with penetrating trauma. In a series of 75 consecutive patients, Udobi et al evaluated ultrasound in patients with trajectories around the abdomen who did not meet criteria for mandatory
laparotomy.9 A positive ultrasound exam reliably predicted the presence of abdominal injury requiring surgical repair. A negative ultrasound, however, was associated with a significant rate of intra-abdominal injury. Triple contrast CT scan has been evaluated as well and has been shown to be sensitive and reliable at predicting the need for operative repair.10 CT scanning is an expensive technology, but saves the cost and resource needs required for in-hospital observation.
The area of the torso that is fraught with the most difficulty in diagnosing injury requiring operation is the thoracoabdomen. Recent data has demonstrated that many gunshot wounds to the liver can be managed nonoperatively.11 In the case of a diaphragmatic injury, the concern about a biliary pleural fistula exists. Minimally invasive repair via thoracoscopy is an option. On the left side of the thoracoabdomen, diagnosing diaphragmatic injury can be quite difficult. While there is no data that evaluates the natural history of a missed left diaphragmatic injury, most clinicians believe that these should be repaired if diagnosed. CT scanning shows some promise in the diagnosis of penetrating injury to the diaphragm, but it is not yet definitive. Simple observation is acceptable, but diaphragmatic injuries may be symptomatic for months or years. Laparoscopy may not be able to fully evaluate the abdomen for injuries, but should be able to perform directed exploration well.12 In this setting, laparoscopy or thoracoscopy is probably the most reliable way of making the diagnosis.
Nonoperative management of penetrating trauma has become far more common. It is important to remember, however, that observation must be reserved for hemodynamically stable patients with reliable physical exam. The rate of negative or non-therapeutic laparotomy should be kept at the absolute minimum necessary. However, this must be weighed against the potentially devastating complication of missed injury.
BIBLIOGRAPHY
1. Trooskin SJ, Sclafani SJA, Winfield J, Duncan AO, Scalea TM, Vieux E, Atweh N. The management of vascular injuries of the extremity associated with civilian firearms. Surg Gynecol Obstet 35:350-354, 1993.
2. Frykberg ER, Crump JM, Dennis JW, et al. Nonoperative

Panam J Trauma
22 Marzo 2004
observation of clinically occult arterial injuries: a prospective evaluation. Surg 109:85-96, 1991.
3. Sclafani SJA, Cavaliere G, Atweh N, Duncan AO, Scalea TM. The role of angiography in penetrating neck trauma. J Trauma 31:557-563, 1991.
4. Atteberry LR, Dennis JW, Menawat SS, Frykberg ER. Physical examination alone is safe and accurate for evaluation of vascular injuries in penetrating zone II neck trauma. J Am Coll Surg 179:657-662, 1994.
5. Demetriades D, Theodorou D, Cornwell EE, et al. Evaluation of penetrating injuries of the neck: a prospective study of 223 patients. World J Surg 21:41-47, 1997.
6. Demetriades D, Velmahos G, Cornwell EE et al. Selective nonoperative management of gunshot wounds to the anterior abdomen. Arch of Surg 132:178-183, 1987.
7. Velmahos G, Demetriades D, Toutouzas KG, et al. Selective nonoperative management in 1856 patients with abdominal gunshot wounds: should routine laparotomy still be the
standard of care? Ann of Surg 234:395-402, 2001.
8. Philips TF, Sclafani SJA, Goldstein AS, Scalea TM, Shaftan GW. Use of the contrast-enhanced CT enema in the management of penetrating trauma to the flank and back. J Trauma 26:593-601, 1986.
9. Udobi K, Rodriguez A, Chiu WC, Scalea TM. The role of ultrasonography in penetrating abdominal trauma: a prospective clinical study. J Trauma 50:475-479, 2001.
10. Chiu WC, Shanmuganathan K, Mirvis S, Scalea TM. Determining the need for laparotomy in penetrating torso trauma: a prospective study using triple contrast abdominopelvic computed tomography. J Trauma 51:860-869, 2001.
11. Demetriades D, Gomez H, Chahwan S et al. Gunshot wounds to the liver: the role of selective nonoperative management. J Am Coll Surg 188:343-348, 1999.
12. Ivatury RR, Simon RJ, Stahl WM. A critical evaluation of laparoscopy in penetrating abdominal trauma. J Trauma 34:822-828, 1993.
Panam J Trauma 2004, 11:1
23
NURSE CLINICIANS - WHAT IS THEIR ROLE?Kathleen D. Martin, MSN, RN, CCRN.
Managing Consultant, Martin Trauma Associates Narberth, Pennsylvania
The need for nurse practitioners and advanced practice nurses has expanded over the last decade as a result of changing economics and the unpredictable healthcare environment. There has been expansion of the number of nurse practitioners, changes in legal parameters of advanced practice nurses and the need for additional clinical expertise at the bedside as the 80 hour resident work week becomes reality. There have also been alterations occurring in the hospital settings, including increased acuity of hospitalized patients, demands of managed care to reduce length of stay and to better coordinate patient care, and decreases in the number of medical residency programs. The role of the advanced practice nurse in the trauma setting has been tried successfully in both the urban, community and rural settings.
The first nurse practitioners were pediatric nurse practitioners who began in Colorado in 1965. The educational program developed in response to the need for health care in rural areas. Since that time numerous specialties have evolved including family practice, pediatrics, gynecology, psychiatry, acute care, critical care and public health. A nurse practitioner (NP) is a registered nurse with advanced academic and clinical experience, which enables him or her to diagnose and manage most common and many chronic illnesses, either independently or as part of a health care team. A nurse practitioner provides some care previously offered only by physicians and in most states has the ability to prescribe medications. Working in collaboration with a physician, a nurse practitioner provides high-quality, cost-effective and individualized care for the lifespan of
patient’s special needs.
There are over 50,000 nurse practitioners authorized to practice in the United States. Nurse practitioners are only one type of Advanced Practice Nurses. Advance Practice Nurses (APNs) include nurse anesthetists, clinical nurse specialists, certified nurse midwives, and nurse practitioners. All APNs require advance education beyond the Bachelor of Science in Nursing (BSN), usually at the Master of Science in Nursing (MSN) level. Course work for preparation as an advanced practice nurses includes clinical experience in advanced health assessment, physiology, pathophysiology, pharmacology, research, professional role development, nursing theory, health promotion, disease prevention, healthcare policy, diagnostic reasoning, and clinical decision making. Additionally, they must have at least 500 clinical practicum hours to sit for the national ACNP certification exam.
CLINICAL PRACTICE
Acute care hospital settings are using NPs and APNs in ICUs, step down units, and other patients care areas, and some units are even managed by advanced practice nurses. The addition of NPs to a service improves patient and family satisfaction as well as communication and overall patient care. In many hospitals, resident coverage may be limited, and the ACNP is responsible for managing all aspects of patients’ care either independently or in collaboration with attending physicians, but must have an RN license before being accepted into an NP or APN educational program. The major difference between an advanced practice nurse and a physician’s assistant is that the PAs work under the supervision of a physician. The Board of Registered Nursing has established guidelines
for procedures which are performed by acute care nurse practitioners. Some of those clinical responsibilities may include:
• obtain medical histories• perform physical examinations• first assist in the OR• chest tube or central line removal• suturing• suture removal• debridment• prescribe medications • prescribe treatments• patient and family education• staff education• ventilator management• x-ray ordering and interpretation• lab ordering and interpretation• EKG ordering and interpretation• nutritional feedings intervention• discharge planning • working closely with families
Additional responsibilities which may be considered in a trauma center setting include:
• resuscitation• post-operative/injury pain management• jugular bulb oxygenation monitoring and catheter
placement• ICP monitor placement• implementation of clinical management guidelines• tracking of compliance with clinical management
guidelines• professional billing
It is the Position of the American College of Nurse Practitioners that
• Access to highly educated nurse practitioners as quality providers and skilled caregivers is the right of every resident in the United States.
• Residents of the United States must have access to quality, cost effective health care services. These services must be delivered safely with an emphasis on prevention of illness and a state of complete
physical, mental and social well being, not merely the absence of disease or infirmity.
• Standards of didactic instruction and clinical practice must be based on accountability and outcome based research.
• Nurse practitioner education must be specific to area of practice.
• The Criteria for Evaluation of Nurse Practitioner Programs (NONPF, 1997) developed through the joint deliberation of the National Task Force on Quality Nurse Practitioner Education comprised of many organizations should be adopted by all NP Educational Programs.
• Curricula of NP Educational Programs should be based on the Curriculum Guidelines and Programs Standards for Nurse Practitioner Education (NONPF, 1995).
• Faculty practice is essential to retain and build upon clinical excellence within nurse practitioner faculties. NP Faculty must be provided the opportunity to act as clinical preceptors, mentors and role models for NP students and new graduates.
• The active exchange of information relative to student preparation, clinical experiences and curriculum development between NP preceptors, mentors, graduate NPs and faculty of NP programs is essential for highest quality NP education
• NP students must be sufficiently experienced, academically and clinically educated, and ethically ready to assume the responsibilities of being an NP student upon entrance into the NP program.
• All undergraduate nursing education programs should continually evaluate their programs to assure the highest standards of professional nursing as a strong foundation for NP Programs, and should implement changes as indicated after review of available data and program self assessment.
Clinical research and practice-based research for continual improvement of NP care delivery and health care delivery in process and outcomes must be supported and encouraged by NP programs of preparation.
Source: Division of Nursing, HRSA, PHS, Rockville, MD http://bhpr.hrsa.gov/healthworkforce/rnsurvey/rnss1.htm
Panam J Trauma
24 Marzo 2004
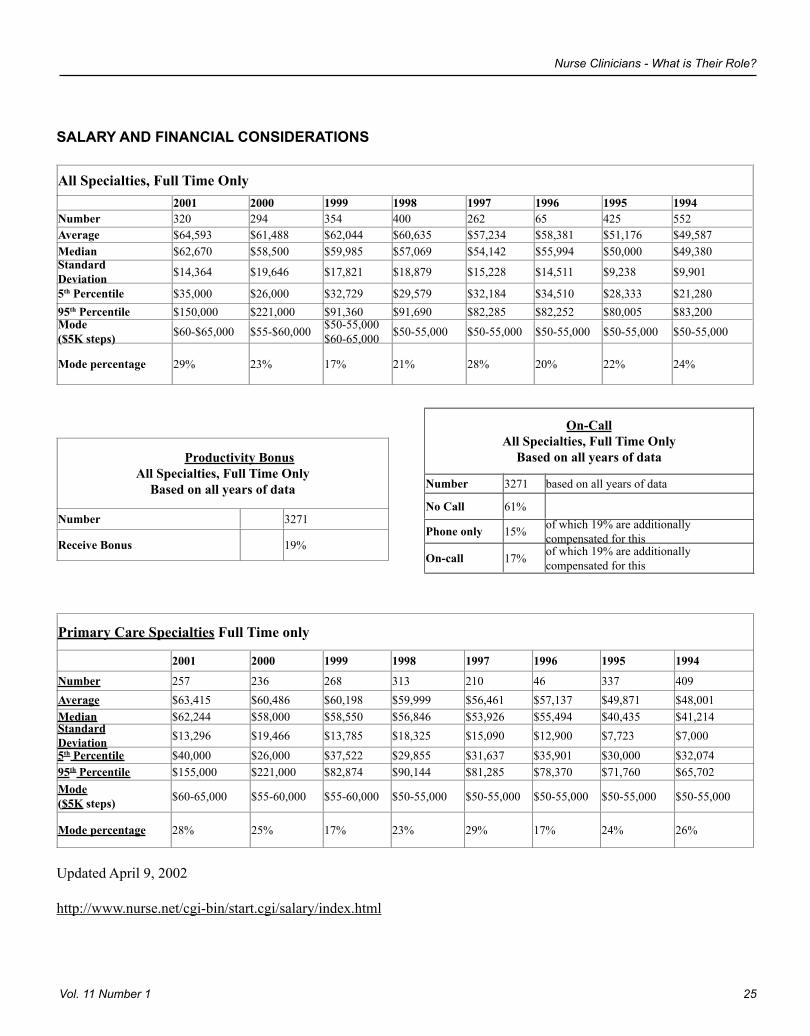
SALARY AND FINANCIAL CONSIDERATIONS
All Specialties, Full Time Only2001 2000 1999 1998 1997 1996 1995 1994
Number 320 294 354 400 262 65 425 552Average $64,593 $61,488 $62,044 $60,635 $57,234 $58,381 $51,176 $49,587Median $62,670 $58,500 $59,985 $57,069 $54,142 $55,994 $50,000 $49,380StandardDeviation $14,364 $19,646 $17,821 $18,879 $15,228 $14,511 $9,238 $9,901
5th Percentile $35,000 $26,000 $32,729 $29,579 $32,184 $34,510 $28,333 $21,28095th Percentile $150,000 $221,000 $91,360 $91,690 $82,285 $82,252 $80,005 $83,200Mode($5K steps) $60-$65,000 $55-$60,000 $50-55,000
$60-65,000 $50-55,000 $50-55,000 $50-55,000 $50-55,000 $50-55,000
Mode percentage 29% 23% 17% 21% 28% 20% 22% 24%
Productivity Bonus All Specialties, Full Time Only
Based on all years of data
Number 3271
Receive Bonus 19%
Primary Care Specialties Full Time only
2001 2000 1999 1998 1997 1996 1995 1994
Number 257 236 268 313 210 46 337 409Average $63,415 $60,486 $60,198 $59,999 $56,461 $57,137 $49,871 $48,001 Median $62,244 $58,000 $58,550 $56,846 $53,926 $55,494 $40,435 $41,214 StandardDeviation $13,296 $19,466 $13,785 $18,325 $15,090 $12,900 $7,723 $7,000 5th Percentile $40,000 $26,000 $37,522 $29,855 $31,637 $35,901 $30,000 $32,074 95th Percentile $155,000 $221,000 $82,874 $90,144 $81,285 $78,370 $71,760 $65,702 Mode($5K steps) $60-65,000 $55-60,000 $55-60,000 $50-55,000 $50-55,000 $50-55,000 $50-55,000 $50-55,000
Mode percentage 28% 25% 17% 23% 29% 17% 24% 26%
Updated April 9, 2002
http://www.nurse.net/cgi-bin/start.cgi/salary/index.html
On-Call All Specialties, Full Time Only
Based on all years of data
Number 3271 based on all years of data
No Call 61%
Phone only 15% of which 19% are additionally compensated for this
On-call 17% of which 19% are additionally compensated for this
Nurse Clinicians - What is Their Role?
25Vol. 11 Number 1
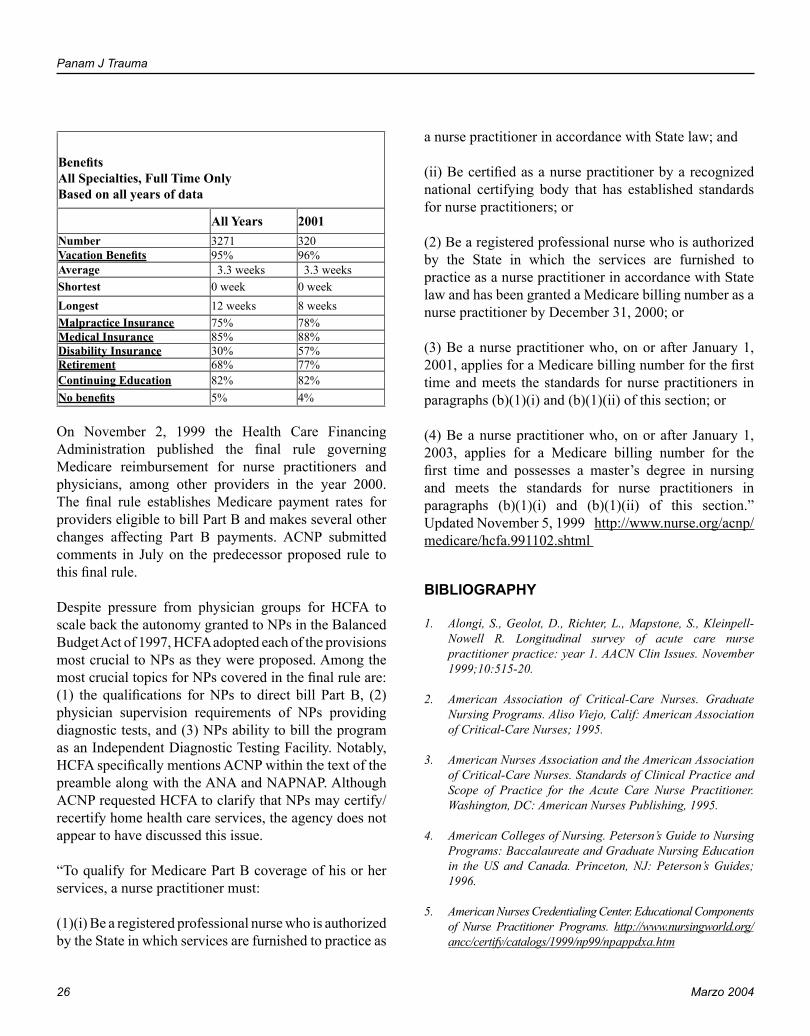
Panam J Trauma
26 Marzo 2004
Nurse Clinicians - What is Their Role?
27Vol. 11 Number 1
BenefitsAll Specialties, Full Time OnlyBased on all years of data
All Years 2001Number 3271 320Vacation Benefits 95% 96%Average 3.3 weeks 3.3 weeksShortest 0 week 0 weekLongest 12 weeks 8 weeksMalpractice Insurance 75% 78%Medical Insurance 85% 88%Disability Insurance 30% 57%Retirement 68% 77%Continuing Education 82% 82%No benefits 5% 4%
On November 2, 1999 the Health Care Financing Administration published the final rule governing Medicare reimbursement for nurse practitioners and physicians, among other providers in the year 2000. The final rule establishes Medicare payment rates for providers eligible to bill Part B and makes several other changes affecting Part B payments. ACNP submitted comments in July on the predecessor proposed rule to this final rule.
Despite pressure from physician groups for HCFA to scale back the autonomy granted to NPs in the Balanced Budget Act of 1997, HCFA adopted each of the provisions most crucial to NPs as they were proposed. Among the most crucial topics for NPs covered in the final rule are: (1) the qualifications for NPs to direct bill Part B, (2) physician supervision requirements of NPs providing diagnostic tests, and (3) NPs ability to bill the program as an Independent Diagnostic Testing Facility. Notably, HCFA specifically mentions ACNP within the text of the preamble along with the ANA and NAPNAP. Although ACNP requested HCFA to clarify that NPs may certify/recertify home health care services, the agency does not appear to have discussed this issue.
“To qualify for Medicare Part B coverage of his or her services, a nurse practitioner must:
(1)(i) Be a registered professional nurse who is authorized by the State in which services are furnished to practice as
a nurse practitioner in accordance with State law; and
(ii) Be certified as a nurse practitioner by a recognized national certifying body that has established standards for nurse practitioners; or
(2) Be a registered professional nurse who is authorized by the State in which the services are furnished to practice as a nurse practitioner in accordance with State law and has been granted a Medicare billing number as a nurse practitioner by December 31, 2000; or
(3) Be a nurse practitioner who, on or after January 1, 2001, applies for a Medicare billing number for the first time and meets the standards for nurse practitioners in paragraphs (b)(1)(i) and (b)(1)(ii) of this section; or
(4) Be a nurse practitioner who, on or after January 1, 2003, applies for a Medicare billing number for the first time and possesses a master’s degree in nursing and meets the standards for nurse practitioners in paragraphs (b)(1)(i) and (b)(1)(ii) of this section.” Updated November 5, 1999 http://www.nurse.org/acnp/medicare/hcfa.991102.shtml
BIBLIOGRAPHY
1. Alongi, S., Geolot, D., Richter, L., Mapstone, S., Kleinpell-Nowell R. Longitudinal survey of acute care nurse practitioner practice: year 1. AACN Clin Issues. November 1999;10:515-20.
2. American Association of Critical-Care Nurses. Graduate Nursing Programs. Aliso Viejo, Calif: American Association of Critical-Care Nurses; 1995.
3. American Nurses Association and the American Association of Critical-Care Nurses. Standards of Clinical Practice and Scope of Practice for the Acute Care Nurse Practitioner. Washington, DC: American Nurses Publishing, 1995.
4. American Colleges of Nursing. Peterson’s Guide to Nursing Programs: Baccalaureate and Graduate Nursing Education in the US and Canada. Princeton, NJ: Peterson’s Guides; 1996.
5. American Nurses Credentialing Center. Educational Components of Nurse Practitioner Programs. http://www.nursingworld.org/ancc/certify/catalogs/1999/np99/npappdxa.htm
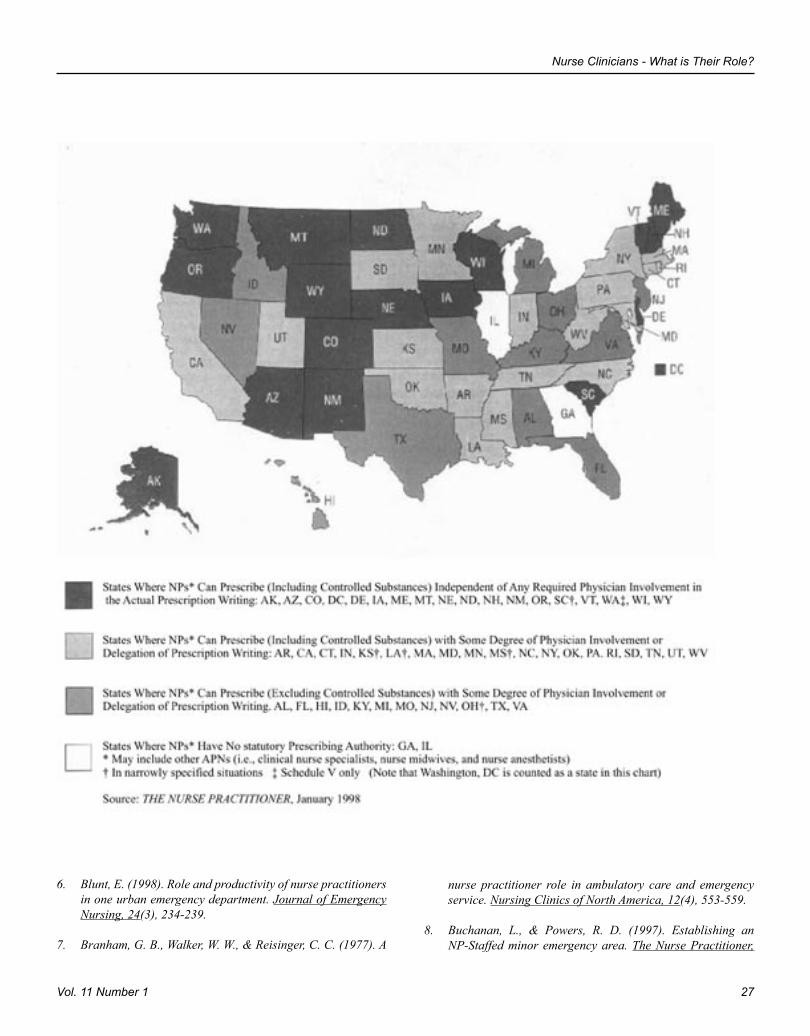
Panam J Trauma
26 Marzo 2004
Nurse Clinicians - What is Their Role?
27Vol. 11 Number 1
6. Blunt, E. (1998). Role and productivity of nurse practitioners in one urban emergency department. Journal of Emergency Nursing, 24(3), 234-239.
7. Branham, G. B., Walker, W. W., & Reisinger, C. C. (1977). A
nurse practitioner role in ambulatory care and emergency service. Nursing Clinics of North America, 12(4), 553-559.
8. Buchanan, L., & Powers, R. D. (1997). Establishing an NP-Staffed minor emergency area. The Nurse Practitioner,
Panam J Trauma
28 Marzo 2004
Nurse Clinicians - What is Their Role?
29Vol. 11 Number 1
22(4), 175-178, 183-187.
9. Cairo, M. J. (1996). Emergency physicians’ attitudes toward the emergency nurse practitioner role: Validation versus rejection. Journal of the American Academy of Nurse Practitioners, 8(9), 411-417.
10. Chang, E., Daly, J., Hawkins, A., McGirr, J., Fielding, K., Hemmings, L., O’Donoghue, A., & Dennis, M. (1999). An evaluation of the nurse practitioner role in amajor rural emergency department. Journal of Advanced Nursing, 30, 260-268.
11. Cole, F. L., & Ramirez, E. G. (1997). The emergency nurse practitioner: An educational model. Journal of Emergency Nursing, 23(2), 112-115.
12. Cole, F. L., Ramirez, E. G., & Mickanin, J. (1999). ED nurse practitioners’ employment by a physician group versus hospital: Pros and cons. Journal of Emergency Nursing, 25(3), 183-186.
13. Cole, F. L., Ramirez, E., G., & Mickanin, J. (1998). Skill station models for teaching incision and drainage of abscesses, felons, and paronychia to emergency nurse practitioners. Journal of Emergency Nursing, 24(5), 455-456.
14. Cole, F.L. & Ramirez, E. (1999). Evaluating an emergency nurse practitioner program for its relevance to the role. Journal of Emergency Nursing, 25(6), 547-550.
15. Cole, F.L. & Ramirez, E. (2000). Activities and procedures performed by nurse practitioners in emergency care settings. Journal of Emergency Nursing, 26, 455-463.
16. Cole, F.L. & Ramirez, E. (2000). Assessing critical thinking of applicants to the Master of Science in Nursing emergency nurse practitioner option with clinical case scenario-based interviewing. Journal of Emergency Nursing, 26, 609-611.
17. Cole, F.L. & Ramirez, E. (2000). Nurse practitioner autonomy in a clinical setting. Emergency Nurse, 7(9), 26-30.
18. Covington, C., & Sellers, F. (1992). Implementation of a nurse practitioner-staffed fast track. Journal of Emergency Nursing, 18(2), 124-131.
19. Curry, J. L. (1994). Nurse practitioners in the emergency department: Current issues. Journal of Emergency Nursing, 20(3), 207-12.
20. Dolan, B., Dale, J., & Morley, V. (1997). Nurse practitioners: the role in A&E and primary care. Nursing Standard, 11, 33-38.
21. Edgerton, M. T., & Edlich, R. F. (1979). Physician and patient
acceptance of emergency nurse practitioners. Journal of American College of Emergency Physicians, 8(19), 357-359.
22. Fincke, M. K. (1975). A new dimension in emergency nursing. Journal of Emergency Nursing, 1(5), 45-52.
23. Geolot, D., Alongi, S., & Edlich, R. F. (1977). Emergency nurse practitioner: An answer to an emergency care crisis in rural hospitals. Journal of American College of Emergency Physicians, 6(8), 355-357.
24. Graham, M.C. & Dellinger, R.W. (2001). Emergency department patients within the scope of nurse practitioner pracitce. The American Journal for Nurse Practitioners, 5(3), 29, 30, 35, 36, 39-42.
25. Hayden, M. L., Davies, L. R., & Clore, E. R. (1982). Facilitators and inhibitors of the emergency nurse practitioner role. Nursing Research, 31(5), 294-299.
26. Ingersoll G. Evaluation of the advanced practice nurse role in acute and specialty care. Crit Care Nurs Clin North Am. 1995;7:25-34.
27. Johnson, E. (1996). A nurse practitioner’s experience in bush Alaska. Journal of Emergency Nursing, 22(6), 509-10.
28. Kindig D, Libby D. How will graduate medical education reform affect specialties and geographic areas? JAMA. 1994;272:37-42.
29. Kleinpell, R. The acute care nurse practitioner: a new career opportunity for critical care curses. Crit Care Nurse. 1997;17:66-69.
30. Kleinpell-Nowell, R. Longitudinal survey of acute-care nurse practitioner practice: year 2. AACN Clinical Issues. August 2001;12:447-452.
31. Parinello, K. Advanced practice nursing. Crit Care Nurse Clinical North Am. 1995;7:9-16.
32. Powers, M. J., Jalowiec, A., & Reichelt, P. A. (1984). Nurse practitioner and physician care compared for nonurgent emergency room patients. Nurse Practitioner, 9(2), 39, 42-52.
33. Ramirez, E. G. (1996). A personal perspective: Nurse practitioner in the emergency department. Journal of Emergency Nursing, 22(6), 538-540.
34. Rhee, K. J., & Dermyer, A. L. (1994). Patient satisfaction with a nurse practitioner in a university emergency service. Annals of Emergency Medicine, 26(2), 131-132.
35. Roglieri, J. L. (1975). Multiple expanded roles for nurses in
Panam J Trauma
28 Marzo 2004
Nurse Clinicians - What is Their Role?
29Vol. 11 Number 1
urban emergency rooms. ‘Emergency room nurse-practitioner.’ Archives of Internal Medicine, 135(10), 1401-1404.
36. Shea, S. S. (1997). The ED nurse practitioner: Pearls and pitfalls of role transition and development. Journal of Emergency Nursing, 23(3), 235-237.
37. Spisso, J., O’Callaghan, C., McKennan, M., & Holcroft, J. W. (1989). Improved quality of care and reduction of housestaff workload using trauma nurse practitioners. The Journal of Trauma, 30(6), 660-663.
38. Stafford Hardy, V. G. (1978). The emergency nurse practitioner: The role and training of an emerging health professional. Journal of American College of Emergency Physicians, 7(10), 372-376.
39. Stuchlak, P.J., Brown, J., & Cydulka, R.K. (1995). Using nurse practitioners and physician assistants in the emergency department. Critical Decisions in Emergency Medicine, 10(1), 1-10.
40. Tye, C. C. (1997). The emergency nurse practitioner role in
major accident and emergency departments: Professional issues and the research agenda. Journal of Advanced Nursing, 26(2), 364-370.
41. Walrath, J. M., Levitt, M. K., & Styka, M. A. (1984). Innovative ED nurse practitioner group practice. Journal of Emergency Nursing, 10(5), 239-241.
42. Widhalm, S. A., & Anderson, L. A. (1982). Emergency nurse practitioners: motivators, barriers, and autonomy in role performance. Journal of Emergency Nursing, 8(2), 67-74.
43. Wilson, C., Farrell, M., & Bove, S. (1994). Emergency department nurse practitioners: The AtlantiCare medical center program in review. Journal of Emergency Nursing, 20(3), 195-198.
44. Wright, S. W., Erwin, T. L., Blanton, D. M., & Covington, C. M. (1992). Fast track in the emergency department: A one-year experience with nurse practitioners. The Journal of Emergency Medicine, 10, 367-373.
45. http://sonser4.nur.uth.tmc.edu/ecnps/bibliogr.htm
Panam J Trauma 2004, 11:1
30
Penetrating Cardiac Trauma
31Vol. 11 Number 1
PENETRATING CARDIAC TRAUMA Ricardo Ferrada, MD, MsP, FACS.
Professor of Surgery Universidad del Valle Cali, Colombia, South America
The real incidence of cardiac wounds is much higher than described in clinical series. It is estimated that 75- 85% of cardiac wounds result in mortality either in situ or during transportation. Over a one year period (1992) in Cali, Colombia, all patients with cardiac wounds, alive and deceased, were studied. Our sources included clinical records of all public and private hospitals, and the city’s coroner registry. We were able to study 637 victims of cardiac wounds. Of this number, 254 or 39.9% died on the scene, allowing 383 or 60.1% for transportation. Of these, 166 or 43.3% died during transport, allowing 217 for surgical treatment. Finally 136 were discaharged after successful surgical intervention. This means that the survival rate among the patients arriving alive was 62.7% on the average. However the real survival rate for the entire group was 21.3%. The blunt cardiac trauma incidence is more difficult to assess due to the large number of blunt thoracic trauma with no clinical profile for cardiac contusion. Regarding the cardiac wound due to blunt trauma, in our study we found 69 victims with two survivors, both with atrial injuries. We found no survivors reported with ventricle injuries due to blunt trauma.
The overpressure in the pericardial space produces an increase in ventricular, atrial and central venous pressure which decreases the right and left ventricular ability to fill decreasing the ejection fraction, cardiac output and stroke volume. Energy demand on myocardium increases, resulting in oxygen debt and hypoxemia. If the pericardium is not opened surgically and the pressure released, cardiac arrest and death comes within minutes.Precordial area. Pericardium, the heart and great vessels
outline projected to the anterior chest wall lie from 2nd intercostal space 2 cm on both sides to 5th intercostal space 2 cm right and 8 cms left. However as stab wounds can produces an injury as deep as the length of the weapon, a danger zone has been established bigger than anatomic outlines. On the other side, it is important to define the path of the injury. For instance, a stab wound located in the 3rd left intercostal space midclavicular line, can be heart directed or left subclavian directed according to its angle. In the same way, a 5th intercostal space wound can be heart or abdominal directed. Epigastrium stab wounds, which are very common, if cefalad directed, can easily reach the heart. In fact there are reports of cardiac injuries with a remote entrance eg. midaxillary line, left hypocondrium. Accordingly, our danger zone for stab wounds includes not only the precordium, but the superior mediastinum and epigastrium.
Gunshot wounds can reach the pericardium from virtually any location. In particular, the management of transmediastinal wounds implies investigating and ruling out accordingly cardiac, esophageal and great vessels injuries.
MANAGEMENT
Emergency cardiopulmonary bypass is almost never necessary. Most of the patients will be saved with a simple suture under general anesthesia. Accordingly, the most important clue in a prehospital setting is transport as soon as possible to the nearest hospital with surgical facilities. Transportation to a more distant facility with heart-lung machine implies treatment delay which could result in much higher mortality.

Panam J Trauma 2004, 11:1
30
Penetrating Cardiac Trauma
31Vol. 11 Number 1
Pericardiocentesis. In the past, pericardiocentesis was advocated as an initial treatment, even in hospitals with surgeons available. However several authors have demonstrated that the best outcome is achieved with immediate thoracotomy. This is due to the clotting of the blood in the pericardial sac, which produces false negative results and makes the pericardiocentesis needle procedure useless as a test or treatment. In some cases there are clots and some liquid blood, which can allow improvement of hemodynamics with the procedure. Hence, pericardiocentesis must be reserved for the patient with pericardial tamponade, hemodynamically unstable, with no surgical facility available; and only as a temporary measure. It must also be remembered that the procedure is dangerous. Coronary tearing and arrhytmias can occur, particularly in these semi-conscious restless patients.
As previously noted most of the patients with cardiac wounds die at the scene shortly after the trauma. In our experience the patients arriving alive to the hospital are one third of the entire group, but this number depends on the type of trauma and the transportation system.
It has been described that patients with penetrating cardiac injury are seen with one of two distinct clinical syndromes: pericardial tamponade or hemorrhagic shock. However, the classic Beck triad (muffled heart sounds, distended neck veins and hypotension) is present only in 10% to 40% of cases of cardiac tamponade. According to our experience and that of others, symptomatic cardiac wounds ranks between 45% to 55%.
Consequently there are a number of patients, with no other signs besides the anterior thoracic wound. It has also been described that these stable patients may have a clot in the wound or they have a very small wound which eventually can be sealed without treatment. However there is neither literature about this condition nor a specific group of physical signs for assuming the injury is an innocent one. On the other hand there are patients dying suddenly despite a previous stable condition. For these reasons, in the presence of a precordial wound it must be assumed that there is an important cardiac injury until proven otherwise. It does not matter if the patient is stable or not.
For practical purposes, patients can be classified as:
• Agonal those with deep hemodynamic compromise. In these cases an immediate thoracotomy must be performed, and the speed of the team define the results.
• Unstables, those with any change in their hemodynamic condition. In these cases ABC is carried out. If recovery is not complete, thoracotomy is warranted.
• Stables, those who have no other signs besides the wound in the precordial area. In these cases studies and procedures can be performed in order to rule out a cardiac wound.
The studies and procedures are:
• Chest X Ray and EKG are not useful because of their unspecific findings. However, X-Rays are very useful in determining thoracic problems: pneumothorax, hemothorax; which must be treated at this moment.
• Local wound exploration. Thoracic wound exploration has been criticized by some authors. However it has been our experience and that of others, that cautious exploration in stable patients, particularly in stab wounds, is very useful in determining the injury direction, which in turn decides the final procedure. This can be made with the finger or instrument. When in doubt, local anesthesia and enlargement of the wound is made. Under direct inspection the surgeon can determine the penetration. If penetration can not be determined, it must be assumed.
• Echocardiogram. Echocardiogram (ECHO) has been advocated as an initial test in stable patients. After the studies from Rozycki and associates, the enthusiasm for its use is almost universal, including at our hospital. However in patients with hemothorax, chest tubes and emphysema, the test can be equivocal or false negative. Accordingly, in stables patients without these problems the echocardiography will miss no significant injury and if available, must be the first test. When there is a doubtful result, a pericardial window is warranted.
Panam J Trauma
32 Marzo 2004
Penetrating Cardiac Trauma
33Vol. 11 Number 1
• Pericardial window. For many years, the pericardial window has been utilized as a diagnostic test in patients with penetrating precordial wounds hemodynamically stables, which are a majority in our experience. The ECHO has narrowed its indication because it is non invasive and the sensitivity is similar to a pericardial window. However when the machine or the experience is lacking, which is common in Latin America, then the pericardial window is a useful test for these patients. During a 6-year period ending December 1988 at the University Hospital in Cali, Colombia, we received 863 patients with penetrating precordial wounds. Of this number 261 or 30.2% were unstable or with signs of tamponade and were underwent an immediate thoracotomy; and 602 or 69.8% were stable with no other signs except the precordial wound. Of these latter patients, which were a majority, 517 underwent a pericardial window. These results were confirmed in a later study with 1101 pericardial windows. The test sensitivity is 100%, and the specificity is more than 99% if the pericardial wound is considered true positive.
• Thoracoscopy. Thoracoscopy has been utilized in precordial trauma as a diagnostic tool. The advantage of this method is the possibility of evaluating thoracic injuries other than cardiac, like pleural effusion or diaphragm wounds and for evacuation of clotted hemothorax.
OPERATIVE MANAGEMENT
Incision
The type of incision is very important because when correctly chosen it can make the procedure easier, but when a mistake at this point is made, the consequences can be catasthrophic. Many patients arrive unstable or agonal, which makes the correct incision determinant of the final result. On the other hand, before the thoracotomy is made, the surgeon does not know what structure is compromised. Many of the patients with precordial wounds have injuries other than cardiac, and others have no injuries at all.
The incision utilized most of the time is the submammary
anterolateral because it can be made with basic instruments; it is very fast; and tt allows management of most of the thoracic viscera including the heart.
However there are some considerations for selecting the incision
1. Location of the wound on the thorax. Left anterolateral is preferable in left wounds and right anterior in right wounds. If multiple stabs are present, and the patient is stable, we prefer to verify the penetration, by exploring the wounds. If both, left and right penetration are found, then left thoracotomy is preferred, because most structures can be accessed through the left side. Gunshot wounds are not explored because they are erratic and it is often difficult to follow their paths. If only right penetrating wounds are found, then right anterolateral is performed.
2. Suspected structures injured.
a. In higher anterior mediastinal wounds, in which no lung injuries are suspected, median sternotomy is advisable. Pulmonary artery and aortic arch are faster and more easily accessible through this incision.
b. When anterolateral incision is made, and if the surgeon finds an injury in the opposite side; it is not wise to repair it through the same incision. Luxation of the heart or maneuvers under heavy pressure can result in cardiac arrest, which in turn has a very high mortality. For these reasons in this case it is preferable to perform another anterolateral incision on the opposite side. If the structure is not easily accessed through this new incision, then a cross sternotomy is made. Cross sternotomy is not made initially because of its postoperative morbidity.
During a two-year period, we performed 242 urgent thoracotomies at the University Hospital in Cali, Colombia. The viscera injured were:
Lung 122Heart 112Internal M vessels 33Intercostal vessels (posterior) 30Pulmonary vessels 8Aorta 3Others 22
Panam J Trauma
32 Marzo 2004
Penetrating Cardiac Trauma
33Vol. 11 Number 1
The type of thoracotomy in these cases were:
Left anterolateral 154Right anterolateral 65Left and right anterolateral 11Median sternotomy 8Left and right with transverse sternotomy 4
Surgical Technique
Once inside the thoracic cavity, the surgeon must make three maneuvers almost simultaneously:
1. If the patient arrives in agonal condition, the correct position of the endotracheal tube must be assessed. This is a crucial step lasting one or two seconds, by verifying the lungs’ movements with the anesthesiologist insuflations. Even in experienced hands the esophageal intubation is possible. Under resuscitation thoracotomy the anesthesiologist has no time to verify the correct position of the tube, which usually is made by auscultation of the thorax. Auscultation is not possible in this setting due to the speed of the maneuvers and because at the same time the surgeons prepare the area with yodophores. Esophageal intubation results in a severe hypoxemia and due to previous agonal condition, non-reversible cardiac arrest follows.
2. Hemorrhage control. As previously noted a number of these patients have injuries other than cardiac. Lung clamp or vascular clamp to pulmonary hilium are important adjunct maneuvers. When the hemorrhage is exanguinating, the heart is empty and it is flaccid on palpation. In these cases the aorta must be occluded, which is a very easy maneuver. However, unless the surgeon is very experienced, it is wiser to do it with fingers, not with a clamp at this moment. Clamping without direct inspection can result in esophagus or aortic small branches injury. For this reason the surgeon should not intend to palpate the aorta, because it is also empty. Instead the fingers are put against the vertebral bodies as a temporary occlusion. Once identified, the surgeon must ask the assistant to do it. This allows the surgeon to do other maneuvers, but more importantly avoids tremors in his hands due to the effort. In these cases it is very
important that the surgeon be calm, mentally and physically.
3. Pericardial sac opening. When pericardial tamponade is released, hemodynamics improve, but usually tachicardia persists. It is wiser not to suture the myocardium at this moment, because of increased difficulty. Instead, put a finger on the wound thus avoiding blood loss, and wait for a few minutes until the cardiac rythm becomes normal. Besides the IV fluids, the anesthesiologist can help with a temporary vagal maneuver which makes the suture a lot easier.
Myocardial suture. Most of our patients are young and interrupted simple sutures without pledgets are well tolerated. Patients older than 50, and or with previous hypertension have friable myocardium. Hence Teflon or pericardium felt pads are used. In those particular patients, all caution should be taken to avoid myocardium tearing by following the heart movements.
Non absorbable suture eg. silk or tycron with a non traumatic needle is used. Polipropylene can be used also, however the author’s preference are the former because it has no memory and consequently the knots are faster and safer. It is a lot easier to use two needle holders, one for the surgeon and the other for the assistant who receives the needle at the moment of suturing.
The entire wall is sutured in right ventricular wounds, and in the left part of it. Atrial wounds are clamped with a Satinsky forceps and sutured with a running suture. Wounds closer to coronary artery are sutured underrruning the vessel in order to avoid its closure. Wound of the coronary vessel can result in significant ischemia, arrhytimias and death. However most of them produce minimal effects in spite of the elevated ST segment. Accordingly, if proximal coronary artery is wounded, repair is intended with 6-0 or 7-0 tycron or polipropilene, separated suture. If it is technically impossible, then the artery is ligated under EKG monitoring. A 10-minute surveillance is recommended for arrhytmias or hemodynamic descompensation. If this is not tolerated, then the suture is removed and gentle digital compression is made until the bypass is initiated.
Panam J Trauma
34 Marzo 2004
Pericardium Closure
In median sternotomy, the pericardium can be left open. In left anterior thoracotomy however, the open pericardial sac can result in heart luxation which produces cava veins occlusion, heart failure and death. Accordingly in left anterior or anterolateral thoracotomy the pericardial sac is closed with an interrupted suture, avoiding the lower one or two stitches. This avoids fluid accumulation and reduces the postpericardiotomy syndrome.
One particular problem not found in the articles on the subject is the heart dilatation during the procedure. When it is increasing, it has to be assumed as acute cardiac failure and the surgeon must make a manual massage. Others techniques like clamping the cava veins leads to cardiac arrest in our experience. If after the procedure the heart is far larger than the pericardial sac, then a prostetic material can be used for enlarge the sac. We have used the IV fluids in the same way and the same concept as the “abdominal compartment syndrome”. If available, the advantage of PTFE or Dacron prothesis is the patient does not necessarily have to go again to the OR.
BIBLIOGRAPHY
1. Kulsherestha P., Iyer K.S., Sampath K.A., et al: Cardiac injuries-A clinical and autopsy profile. J Trauma 1990; 30: 203-207.
2. Ferrada R., Currea D., Manzano J: Epidemiologia del trauma cardiaco. Abstract, VII Panamerican Trauma Society Meeting. 1994.
3. Demetriades D. Cardiac wounds. Experience with 70 patients. Ann Surg 1986; 203: 315-317.
4. Ivatury RR, Rohman M, Steichen FM et al. Penetrating cardiac injuries: Twenty-year experience. Am Surg 1987; 53: 310-317.
5. Ordoñez C., Florez G., Ferrada R.: Trauma cardiaco penetrante. Resumenes (Abstract) Congreso Avances en Cirugia. Sociedad Colombiana de Cirugia. Bogota, Colombia, 1990.
6. Ferrada R, García A. Torso Penetrating Trauma. Adv Trauma and Critical Care 1993; 8: 85-116.
7. Rozycki GS, Feliciano DV Ochsner G et al. The role of ultrasound in patients with possible penetrating cardiac wounds: a prospective multicenter study. J Trauma 1999; 46: 543-552.
8. Ferrada R. Comment in Fulda G, Brathwaite CE, Rodriguez A, et al. Blunt traumatic rupture of the heart and the pericardium: A ten-year experience (1979-1989). J Trauma 1991; 31: 173.
9. Currea D, Ferrada R, García A. Experience with 1101 Pericardial windows at the Hospital Universitario, Cali, Colombia. Abstract X Congress Panamerican Trauma Society. Miami, USA, XI, 1997.
10. Ferrada R, Mejia W. Toracotomia de resuscitacion. S Am J Thoracic Surg; 2001; 7: 64 –79.
11. Yugueros P., Sarmiento J., Ferrada R.: Sindrome Postpericardiotomia. Revista Colombiana de Cirugia. 1993;8:90-100.
Panam J Trauma 2004, 11:1
35
PROPHYLAXIS IN THE ICU: WHAT WORKS AND WHAT DOESN’TMichael D. Pasquale, MD, FACS, FCCM.
Associate Professor, Penn State University.Chief, Division of Trauma/Surgical Critical Care. Vice Chairman, Department of Surgery, Lehigh Valley Hospital Allentown, Pennsylvania
VENOUS THROMBOEMBOLISM PROPHYLAXIS
It has been shown that among hospitalized patients, those sustaining major trauma have the highest risk of developing venous thromboembolism (VTE). Without prophylaxis, this population of patients has a DVT risk that exceeds 50% and PE is the third most common cause of death in those patients that survive beyond one day. Despite the routine use of thromboprophylaxis, a recent study in trauma patients reported the incidence of DVT to be 28%. Specific risk factors that have been associated with an increased incidence of thromboembolism include spinal cord injury, lower extremity or pelvic fracture, the need for a prolonged surgical procedure, advanced age, venous injury or indwelling femoral venous line, prolonged immobility, and increased hospital length of stay.
Mechanical Prophylaxis
The best evidence for the use of intermittent pneumatic compression devices (IPC) comes from a trial in 149 trauma patients without lower extremity fracture who were randomized to receive either thigh-high sequential compression devices or venous foot pumps. In this study patients were evaluated by venous duplex on day 8 and DVT was detected in 6.5% of the IPC group and in 21% of the foot pump group (p<.009). Two other studied by Knudson et al. showed that IPC appeared to be effective in patients with head injuries however, a number of other studies have reported no benefit of IPC compared with no prophylaxis. Problems with IPC include its
inability to be used in approximately one third of trauma patients and poor compliance with proper use. Based on the available data, venous foot pumps cannot be recommended for VTE prophylaxis in trauma patients while IPC may be beneficial in patients with intracranial bleeds and as initial prophylaxis for patients at high risk for bleeding, until anticoagulation can be started.
Low Dose Unfractionated Heparin
Currently, low dose unfractionated heparin is not particularly effective in trauma patients. Evidence against its routine use in high-risk patients comes from a large trial comparing LDUH to LMWH and a meta-analysis that demonstrated that LDUH was no better than no prophylaxis.
Low Molecular Weight Heparin
LMWH has been shown to be superior to LDUH in a prospective, double-blind, randomized trial by Geerts et al. In this study of 344 major trauma patients without intracranial bleeding the risk reductions for DVT and proximal DVT with LMWH over LDUH were 30% and 58% respectively (p<.01). The greater protection of LMWH applied to both the higher-risk patients with lower extremity fractures and to the lower-risk patients without leg fractures.
Combined Mechanical and Pharmacologic Methods
While it is acknowledged that combinations of mechanical and pharmacologic methods of prophylaxis may confirm additive protection agains VTE, data in trauma is currently lacking and thus no recommendation

Panam J Trauma
36 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
37Vol. 11 Number 1
can be made regarding this type of therapy.
Screening
The high risk for VTE in trauma and the limited effectiveness of most prophylaxis has led to the recommendation that high-risk patients be screened for asymptomatic DVT using duplex ultrasonography. It should be noted that duplex scanning will fail to detect even proximal DVT in a significant proportion of trauma patients and the use of duplex scanning may not prevent PE. At least 25% of trauma patients are unable to have a complete ultrasound study of their proximal deep venous system because of local injuries, pain, or poor patient compliance. Cost of duplex scanning and the possibility of delaying prophylaxis are other limitations that must be considered. With appropriate use of prophylaxis, there is little or no incremental value of routine duplex screening however, selective screening may be beneficial in high-risk patients in whom early prophylaxis is not possible.
Prophylactic Vena Cava Filter
There are currently no randomized trials of the prophylactic use of IVC filters in any patient population and no evidence that IVC filter insertion is of benefit when added to the most effective prophylaxis modality appropriate for the patient’s clinical condition. Several studies and a recent meta-analysis of prospective studies found no difference in rates of PE in paitents with and without prophylactic filters while it is recognized that IVC filters may be associated with short and long-term complications. Additionally, it has been suggested that there may be an increased incidence of thrombosis at the insertion site. In an analysis by Spain et al. it was concluded that routine screening or prophylactic IVC filter insertion would not prevent any deaths or otherwise benefit trauma patients.
The routine use of VTE prophylaxis in trauma patients is now the standard of care and as such, all trauma units should develop a management guideline for VTE prevention based on individual patient risk factors. It is important to select an effective method of prophylaxis and to start as soon as possible. The use of LMWH, once bleeding has been controlled is the most efficacious and simplest option for the majority of moderate and high
risk patients. Contraindications to LMWH prophylaxis include: intracranial hemorrhage, uncontrolled bleeding , uncorrected coagulopathy, and incomplete spinal cord injury with paraspinal hematoma. Most trauma patients can be started on LMWH within 36 hours of injury, although brief delays are appropriate when necessary to establish the presence of hemodynamic stability. For patients with contraindications to LMWH, mechanical modalities should be considered in spite of their limited protection. If mechanical devices are used they should be started as early as possible after admission, applied to both legs, and used for close to 24 hours per day. After an initial period of mechanical prophylaxis, and once hemostasis is achieved, these patients can usually be started on a regimen of LMWH. The optimal duration of prophylaxis is not known, but it is generally recommended that it should continue appropriate for the patient’s risk, until hospital discharge, including the period of post-trauma rehabilitation. If the hospital stay is in excess of 2 weeks, and if there is an ongoing risk for VTE, continuing inpatient prophylaxis with oral anticoagulants should be considered provided there is no longer a major risk of bleeding or further surgical intervention planned. In patients at high risk for VTE who have received suboptimal prophylaxis, consideration should be given to screening with duplex ultrasound. IVC filters cannot be recommended for primary prophylaxis at this time.
STRICT GLYCEMIC CONTROL
Stress induced hyperglycemia associated with insulin resistance is a prevalent condition in the critically ill surgical patient population, even in those who have not previously had diabetes. This “stress diabetes” is a result of the hypermetabolism often associated with critical illness and is characterized by significant alterations in carbohydrate metabolism. Physiologically, nondiabetic patients with protracted critical illnesses demonstrate high serum levels of insulin-like growth factor-binding protein 1, which reflects an impaired response of hepatocytes to insulin, so-called “insulin resistance”. It is widely recognized that hyperglycemia in the setting of diabetes mellitus leads to increased infectious complications via an impairment of host immune defenses and it has been suggested that pronounced hyperglycemia may lead to complications

Panam J Trauma
36 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
37Vol. 11 Number 1
in non-diabetic critically ill patients as well. It has been shown that critically ill patients who require more than 5 days of intensive care have a 20% risk of death and substantial morbidity. Contributing factors include critical illness polyneuropathy with skeletal muscle wasting which leads to prolonged mechanical ventilation and increased susceptibility to infection and multiple organ dysfunction syndrome. Previous studies have shown that aggressive efforts to tightly control serum glucose in the diabetic population during the peri-operative period will lead to a decrease in infectious complications. With this as a background, others have undertaken studies to determine whether “tight control” of blood glucose during critical illness will decrease mortality and morbidity in surgical patients.
Van den Berghe et al. hypothesized that hyperglycemia or relative insulin deficiency during critical illness predisposes patients to complications such as severe infections, polyneruopathy, multiple-organ failure, and death. The authors performed a prospective, randomized, controlled trial at one center to determine whether normalization of blood glucose levels with intensive insulin therapy reduces mortality and morbidity among critically ill patients. In this study adult patients receiving mechanical ventilation admitted to a primarily surgical intensive care unit were randomly assigned to receive either intensive or conventional insulin therapy. In the conventional treatment group, a continuous infusion of insulin with the use of a pump was started only if the blood glucose level exceeded 215 mg/dL and the infusion was adjusted to maintain the level at a value between 180 and 200 mg/dL. In the intensive treatment group, an insulin infusion was started if the blood glucose level exceeded 110 mg per deciliter, and the infusion was adjusted to maintain normoglycemia (80 to 110 mg/dL). The primary outcome measure was death from any cause during intensive care. Secondary outcome measures were in-hospital death; the number of days in the intensive care unit and the need for prolonged intensive care (more than 14 days) or readmission; the need for ventilatory support, renal replacement therapy, or inotropic or vasopressor support; critical-illness polyneuropathy; markers of inflammation (the C-reactive protein level, white-cell count, and body temperature); bloodstream infection and use of antibiotics for more than 10 days; transfusion requirements; and hyperbilirubinemia.
A total of 1548 patients were enrolled in the study. The clinical and demographic characteristics of the treatment groups were similar at randomization and there were no significant differences in the rates of preexisting diabetes and hyperglycemia at the time of admission, the mean intake of nonprotein calories, and the mean nitrogen intake. In the intensive treatment group the morning blood glucose level was maintained at a mean value of 103+19 mg per deciliter (5.7+1.1 mmol per liter). In the conventional treatment group, the morning blood glucose level was maintained at a mean value of 153+33 mg per deciliter (8.5+1.8 mmol per liter). Hypoglycemia (defined as a blood glucose level of 40 mg per deciliter (2.2 mmol per liter) or less) occurred in 39 patients in the intensive treatment group and in 6 patients in the conventional treatment group. In two patients who received intensive insulin therapy, hypoglycemia was associated with sweating and agitation, but there were no instances of hemodynamic deterioration or convulsions.
Thirty five patients in the intensive treatment group (4.6 percent) died during intensive care, as compared with 63 patients (8.0 percent) in the conventional treatment group, representing an apparent risk reduction in mortality of 42 percent. Intensive insulin therapy also reduced in-hospital mortality with the greatest reduction seen in deaths due to multiple-organ failure with a septic focus. The numbers of deaths during the first five days of intensive care were similar in the two treatment groups. The proportion of patients who required intensive care for more than five days was similar in the two groups (27 percent in the intensive treatment group and 31 percent in the conventional treatment group, P=0.1). The observed reduction in mortality with intensive insulin therapy occurred exclusively in this long stay cohort (10.6 percent mortality in the intensive treatment group vs. 20.2 percent in the conventional treatment group, P=0.005).
In a multivariate logistic-regression model, the independent determinants of mortality were an APACHE II score of 9 or higher for the first 24 hours of intensive care, greater age, indication for admission other than cardiac surgery, tertiary referral, and conventional insulin treatment, but not a history of diabetes or hyperglycemia at the time of admission to the intensive care unit. Additionally, a history of diabetes or

Panam J Trauma
38 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
39Vol. 11 Number 1
hyperglycemia at the time of admission did not affect measures of morbidity. Intensive insulin therapy reduced the duration of intensive care but not the overall length of stay in the hospital. Significantly fewer patients in the intensive treatment group required prolonged ventilatory support and renal replacement therapy, whereas the proportion of patients who needed inotropic or vasopressor support was similar in the two groups. The number of patients who had hyperbilirubinemia was also significantly smaller in the intensive treatment group. Intensive insulin treatment also reduced the episodes of septicemia by 46%. Markers of inflammation were less frequently abnormal in the intensive treatment group than in the conventional treatment group (P<.02). The patients who received intensive insulin therapy were less likely to require prolonged use of antibiotics than were the patients who received conventional treatment, an effect that was largely attributable to the lower rate of bacteremia in the intensive treatment group. Among patients with bacteremia, those treated with intensive insulin therapy had a lower mortality rate than those treated conventionally (12.5 percent vs. 29.5 percent), although this difference was not statistically significant. Among the patients who were screened, those receiving intensive insulin therapy were less likely to have critical illness polyneruopathy than were those receiving conventional treatment, and the cases that did develop resolved more rapidly. The number of patients who received red-cell transfusions did not differ significantly between the two groups, however, the median number of transfusions in the intensive treatment group was only half that in the conventional treatment group.In a separate study recently presented at the American College of Surgeons, Committee on Trauma meeting, Fox et al. hypothesized that strict glycemic control would decrease rates of blood borne infections in SICU patients. In this study consecutive adult patients admitted to the SICU requiring treatment of hyperglycemia (serum glucose > 150mg%) were randomized to receive standard therapy or strict glucose control. The strict glucose control group received continuous regular insulin infusion therapy using a target serum glucose (SG) range of 80-120mg%. Standard therapy patients likewise were managed by continuous regular insulin infusion using a target SG range of 180-220mg%. Outcomes measures included SG values, insulin dose, incidence of blood borne infections and length of stay
in the ICU. Infection rates were calculated as CDC-defined infections per 1000 patient ICU-days (PID) and compared between groups. Blood borne infections are defined as: bacteremia (2/2 blood cultures with growth of same organism), catheter infection (> 15 colonies from the distal 1 cm protion of the intra-vascular catheter), and catheter-related sepsis (CRS) (catheter tip infection plus a 2/2 positive blood cultures for same organism within 2 days of each other).
A total of 65 patients completed the study, (strict control = 36, and standard control = 29). Mean age (58 yrs), APACHE II scores (16), length of stay (20 days) and percent diabetes (25%) were not different between groups. Mean daily serum glucose values were significantly less for the strict control group vs standard control group, (127+37 mg% vs 182+58 mg%, p<.05). The incidence of bacteremia was reduced to 3.5 per 1,000 PID in the strict control group, down from 31 per 1,000 PID in the standard control group, p<.001. Episodes of catheter-related sepsis, likewise were reduced from 20 per 1,000 PID in the standard group to 1.7 per 1,000 PID in the strict group. A significant increase in patients experiencing hypoglycemic events (serum glucose <60mg%) was observed in the strict control group vs the standard control group, 30% vs 8% respectively, p<.01. In all cases hypoglycemia was rapidly reversed with glucose infusion with out associated complications.
Since the introduction of mechanical ventilation, few intensive care interventions have improved survival. Treatment of sepsis with activated protein C results in a 20% reduction in mortality at 28 days. Glycemic control is a preventive approach that is more broadly applicable to critically ill patients and that reduced mortality in the ICU by more that 40%. Intensive insulin therapy also reduced the use of intensive care resources and the risk of complications that are common among patients requiring intensive care, including episodes of septicemia and a corresponding need for prolonged antibiotic therapy. The higher risk in the conventional treatment group may reflect the deleterious effects of hyperglycemia on macrophage or neutrophil function or insulin-induced trophic effects on mucosal and skin barriers. Intensive insulin treatment also prevented acute renal failure and reduced the number of transfusions required in critically ill patients. The reduced need for mechanical ventilation

Panam J Trauma
38 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
39Vol. 11 Number 1
in patients who received intensive insulin therapy is explained in part by the reduced rate of critical-illness polyneuropathy, though a direct anabolic effect of insulin on respiratory muscles.
In conclusion, the use of exogenous insulin to maintain blood glucose at a level no higher than 110-120 mg per deciliter reduces morbidity and mortality among critically ill patients in the surgical intensive care unit, regardless of whether they have a history of diabetes.
STRESS ULCER PROPHYLAXIS
Critically ill patients commonly develop proximal gastrointestinal tract problems as a result of severe physiologic stress. Among the abnormalities observed in such patients are stress-related mucosal disease, gastrointestinal motility disturbances, and mucosal edema related to hypoalbuminemia. Stress-related mucosal disease refers to the development of specific, discrete, gastric mucosal lesions in response to severe stress in other organ systems. Seventy-five percent to 100% of critically ill patients demonstrate evidence of mucosal damage within 24 hours of admission to the ICU. Two types of stress-related mucosal disease occur. The first is stress-related injury, which consists of superficial erosions that usually are diffuse. Patients with such lesions generally have a low risk of clinically important bleeding. The second stress-related mucosal disease consists of stress ulcers, deeper lesions that tend to be more focal and have a greater risk of clinically important bleeding. Although sequelae are rare three different kinds of stress-related mucosal bleeding may occur in the ICU. Occult bleeding is defined as a guaiac-positive gastric aspirate or guaiac-positive stool. Overt bleeding refers to hematememsis, hematochezia, or melena. Clinically important bleeding is overt bleeding complicated by hemodynamic changes or by the need for transfusion, defined as the presence of hypotension, tachycardia, or orthostasis or as a drop in hemoglobin of > 2 g/dl. The rate of overt bleeding is estimated to be approximately 5% in clinically ill patients, however most overt bleeding is not clinically relevant. Only when bleeding is associated with alterations in physiology, such as hypotension or tachycardia, or results in anemia or the need for transfusion is it considered clinically important. Clinically important bleeding occurs only in
approximately 1% to 4% of critically ill patients.
Pathophysiology of gastrointestinal ulceration is incompletely understood. A mucosal lesion results from a defective gastric mucosal barrier that is unable to counter the damaging effects of hydrogen ions. In the setting of a very low intraluminal gastric pH, hypoperfusion and acidosis combine to decrease gastric blood flow. The decrease in gastric blood flow, coupled with a low intraluminal gastric pH, are the major factors in stress-related mucosal disease and stress-related mucosal bleeding. Decreased blood flow (ischemia), followed by reperfusion may augment injury. Several studies have concluded that abnormal gastrointestinal motility is common in critically ill patients. The prevalence of abnormalities in gastric emptying in such patients has been estimated to be as high as 50%. Delayed gastric emptying affects the ability to provide enteral nutrition and may affect the pharmacokinetics of orally administered drugs. These disturbances in motility also may influence decisions regarding the route of delivery of treatment for stress-related mucosal disease. Another possible consequence of critical illness is an acute decrease in serum proteins, exacerbated by inadequate nutritional repletion. Marked hypoalbuminemia may result in gastrointestinal mucosal edema, which inhibits the absorption of amino acids and peptides necessary to restore tissue and serum proteins. Furthermore, mucosal edema may inhibit the absorption of orally administered medications and so may influence medication decisions.
In the absence of an effective mucosal barrier or repair process, exposure to gastric acid causes gastrointestinal mucosal injury and represents the most important factor in stress-related mucosal disease. The hypersecretion of acid is unusual in critically ill patients; acid secretion is, in fact, often diminished in this patient population. However, even small amounts of acid can cause significant injury. Because the presence of acid is a prerequisite for mucosal injury, the inhibition of acid secretion is the primary goal of any therapeutic approach for the treatment or prevention of stress-related mucosal disease. Clinical trials have shown clearly that maintaining intragastric pH above 3.5 to 5.0 can prevent injury. The rationale for the use of antisecretory therapy is based on three factors: the formation of clots, the lysis of clots, and mucosal healing. The aggregation of

Panam J Trauma
40 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
41Vol. 11 Number 1
platelets is impaired in the presence of gastric acidity; clotting is optimized at a pH of 5.0 to 7.0. Pepsin results in the lysis of clots; the presence of pepsin may make clots unstable and also may cause mucosal injury. This enzyme becomes inactive at a pH of > 4.5. Furthermore, mucosal healing is impaired in the presence of gastric acid. Maintaining a gastric pH of > 5.0 neutralizes 99% of acid.
The primary objective of acid-suppressive therapy is to prevent stress-related mucosal disease by raising intragastric pH to > 4. Maintaining the pH at > 4 renders pepsin inactive and inhibits fibrinolysis. Raising the pH merely to 4 will prove inadequate for patients with acute upper gastrointestinal bleeding or those at risk for rebleeding after successful hemostasis. In such patients, an intragastric pH of > 6 must be achieved and maintained to prevent the dissolution of blood clots. Intragastric pH studies have demonstrated that, whereas agents that produce a gastric pH of 4 may have the ability to prevent stress-related mucosal disease, only agents that can achieve a pH of > 6 seem to be able to maintain clots after bleeding has occurred.
Several studies have identified the risk factors for stress-related mucosal disease as being the need for prolonged mechanical ventilation (>48 hours) and coagulopathy. Shock (hypotension) was nearly statistically significant with an odds ration of 3.7 (p=.08). Other risk factors that were not statistically significant include sepsis, liver failure, renal failure, enteral feeding, and glucocorticoids. These data indicate that patients in the ICU without mechanical ventilation, coagulopathy, or possibly shock may not benefit from prophylaxis. Data from Cook et al. in 1994, showed that, among 847 patients with risk factors, 31 (3.7%) experienced clinically important bleeding. Among 1405 patients without risk factors, only 2 (.1%) had clinically important bleeding. The authors concluded that prophylaxis with acid-suppressing medications does not seem to be warranted in patients at low risk for clinically important bleeding (patients not receiving mechanical ventilation or without significant coagulopathy) because prophylaxis would need to be given to >900 such patients to prevent a single episode of bleeding. In contrast, prophylaxis in high-risk patients receiving prolonged mechanical ventilation or with significant coagulopathy would need to be given
to only 30 patients to prevent one episode of bleeding. This suggests that prophylaxis with acid suppression is clinically meaningful and is a reasonable approach in high-risk patients.
In order to evaluate the best method of prophylaxis, Cook et al. published a meta-analysis in 1996, of 57 randomized controlled trials, involving 7218 patients. In this analysis, the ability of histamine-2-receptor antagonists (H2RAs) to reduce the prevalence of overt and clinically important bleeding was compared with that of antacids or placebo. The pooled comparative data indicated that acid suppression with H2RAs provided a significant clinical benefit with regard to overt bleeding. Far more relevant was the finding that the prevalence of clinically important bleeding in patients receiving H2RAs was significantly less than that in patients taking placebo or antacids. The findings of this meta-analysis suggested that acid suppression with H2RAs reduced the likelihood of clinically important bleeding in the ICU by 50%.
It has been shown that in patients with moderate to severe gastroesophageal reflux disease that the oral and intravenous proton pump inhibitors (PPIs) are more potent acid suppressants than the H2RAs. Compared with the latter agents, PPIs raise the intragastric pH higher and maintain the elevated pH for longer periods of time. Two studies by Phillips et al. and Lasky et al. investigated the use of PPIs for stress ulcer prophylaxis in 60 and 75 mechanically ventilated patients respectively. These studies showed that intragastric pH was raised from 3.3 and 3.5 to 5.6 and 6.7 respectively, and that clinically significant bleeding did not occur in any patient treated with a PPI. These studies involved low numbers of patients and did not have a comparison group. A third study by Levy et al. prospectively randomized mechanically ventilated patients to receive either an IV H2RA or a PPI. This study showed that 11 of 35 patients (31%) treated with the H2RA developed clinically significant bleeding as compared with 2 of 32 patients (6%) of those treated with the PPI. Again, this study had a low sample size and was not blinded. Additionally, patients in the H2RA group had more risk factors for bleeding than those in the PPI group and there was a much higher than expected bleeding rate in the H2RA group of patients. A major problem with the three
Panam J Trauma
40 Marzo 2004
Prophylaxis in the ICU: What Works and What Doesn’t
41Vol. 11 Number 1
trials cited above was the use of a different definition of clinically important bleeding than that in the benchmark studies by Cook et al. Although PPIs have been shown to increase intragastric pH to a greater degree than H2RAs, the available data does not support their use as a first line agent to prevent stress ulceration.
In conclusion, it appears as though the main risk factor for the development of stress injury to the gastric mucosa is impaired supply of oxygenated blood to the mucosa. This inadequate mucosal oxygenation results in low tissue pH and ATP, increased lactate production, release of oxygen radicals, and impaired synthesis of protective prostaglandins causing reduced production of bicarbonate and mucous. This condition is then further exacerbated by gastric acid production with subsequent mucosal injury. Thus, the most effective stress ulcer prophylaxis is achieved by general intensive care measures. It is preferred to restrict specific pharmacologic prophylaxis to patients running a high risk of developing stress bleeding. Two strong independent risk factors for bleeding that have been identified are prolonged mechanical ventilation (> 48 hours) and the presence of coagulopathy. Other factors including sepsis, hypotension, renal failure, hepatic failure, GCS < 7, severe burns, tetraplegia, and MODS have conflicting data as to whether or not they are risk factors and therefore may be given consideration for prophylaxis. When pharmacologic therapy is necessary, the best agent for stress ulcer prophylaxis would ideally be inexpensive, effective, easily administered, and without significant side effects. At this time the preferred agent would appear to be a H2RA.
BIBLIOGRAPHY
1. Geerts WH, Code KI, Jay RM, et al. A prospective study of venous thromboembolism after major trauma. NEJM 1994;331:1601-1606.
2. Meissner MH, Chandler WL, Elliott JS. Venous thromboembolism in trauma: A local manifestation of systemic hypercoagulability? J Trauma 2003;54:224-231.
3. Geerts WH, Jay RM, Code KI, et al. A comparison of low-dose heparin with low-molecular weight heparin as prophylaxis against venous thromboembolism after major trauma. NEJM 1996;335:701-707.
4. Elliot CG, Dudney TM, Egger M, et al. Calt-thigh sequential pneumatic compression compared with plantar venous pneumatic compression to prevent deep-vein thrombosis after non-lower extremity trauma. J Trauma 1999;47:25-32.
5. Knudson MM, lweis FR, Clinton A, et al. Prevention of venous thromboembolism in trauma patients. J Trauma 1994;37:480-487.
6. Knudson MM, Morabito D, Paiement GD, et al. use of low molecular weight heparin in preventing thromboembolism in trauma patients. J Trauma 1996;41:446-459.
7. Pasquale MD, Fabian TC, and the EAST Ad Hoc Committee on Practice Management Guideline Development. Practice management guidelines for trauma from the Eastern Association for the Surgery of Trauma. J Trauma 1998;44:941-957.
8. Rogers FB, Cipolle MD, Velmahos G, et al. Practice management guidelines for the prevention of venous thromboembolism in trauma patients: The EAST Practice Management Guidelines Work Group. J Trauma 2002;53:142-164.
9. Cipolle MD, Wojcik R, Seislove E, et al. The role of surveillance duplex scanning in preventing venous thromboembolism in trauma patients. J Trauma 2002;52:453-462.
10. Spain DA, Richardson JD, Polk HC, et al. Venous thromboembolism in the high-risk trauma patient: Do risks justify aggressive screening and prophylaxis? J Trauma 1997;42:463-469.
11. Girard P, Stern J-B, Parent F. Medical literature and vena cava filters: So far so weak. Chest 2002;122:963-967.
12. Wojcik R, Cipolle MD, Fearen I, et al. Long-term follow-up of trauma patients with a vena caval filter. J Trauma 2000;49:839-843.
13. Velmahos GC, Kern J, Chan LS, et al. Prevention of venous thromboembolism after injury: An evidence-based report-part I: Analysis of risk factors and evaluation of the role of vena caval filters. J Trauma 2000;49:132-139.
14. Velmahos GC, Kern J, Chan LS, et al. Prevention of venous thromboembolism after injury: An evidence-based report-part II: Analysis of risk factors and evaluation of the role of vena caval filters. J Trauma 2000;49:140-144.
15. Geerts WH, et al. Prevention of venous thromboembolism. Seventh ACCP Consensus Conference on Antithrombotic Therapy. Chest 2003; in press.
Panam J Trauma
42 Marzo 2004
16. Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. NEJM 2001;345(19):1359-1365.
17. Fox S, Swan K, Murawski D, et al. Strict glycemic control reduces the incidence of bacteremia in critically ill surgical patients. Presented at the 81st Annual Meeting of the Committee on Trauma. Chicago, Ill. March 13, 2003
18. Mizock BA. Alterations in carbohydrate metabolism during stress: A review of the literature. Am J Med 1995;98:75-84.
19. Pomposelli JJ, Baxter JK, Babineau TJ, et al. Early postoperative glucose control predicts nosocomial infection rate in diabetic patients. JPEN 1998;22:77-81.
20. Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. NEJM 1994;330:377-381.
21. Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer
prophylaxis in critically ill patients: Resolving discordant meta-analyses. JAMA 1996;275:308-314.
22. Phillips JO, Metzler MH, Plamieri TL, et al. A prospective study of simplified imeprazole suspension for the prophylaxis of stress-related mucosal damage. Crit Care Med 1996;24:1793-1800.
23. Lasky MR, Metzler MH, Phillips JO, et al. A prospective study of omeprazole suspension to prevent clinically significant gastrointestinal bleeding from stress ulcers in mechanically ventilated trauma patients. J Trauma 1998;44:527-533.
24. Cash BD. Evidence-based medicine as it applies to acid suppression in the hospitalized patient. Crit Care Med 2002;30:S373-S378.
25. Fennerty MB. Pathophysiology of the upper gastrointestinal tract in the critically ill patient: Rationale for the therapeutic benefits of acid suppression. Crit Care Med 2002;30:S351-S355.
Panam J Trauma 2004, 11:1
43
SOLID ORGANS - ARE THEY ALL THE SAME?J. Wayne Meredith, MD, FACS.
Chairman, American College of Surgeons Committee on Trauma, Director, Division of Surgical Sciences, Professor and Chairman, Department of General Surgery, Wake Forest University Medical School, Winston-Salem, North Carolina
For the general surgeon, the management of blunt trauma solid organ injuries takes up a significant amount of time and interest. The most common injuries and the most common causes for operation following blunt trauma are solid organs - the liver, spleen, and kidneys. These organs differ in location, anatomy and blood supply, the natural history of the course of an injury, and the function of the organ, all of which determine the indications for operation or operative management and the treatment options.
The liver is a large anterior organ, mostly protected by the rib cage but also housed between the rib cage and vertebral column, allowing the liver to be prone to fractures by compression between these structures. In addition, its large size makes it the most commonly injured solid organ by penetrating trauma.
The spleen is located deep in the left upper quadrant. With age, the spleen becomes more delicate and prone to fracture and more susceptible to lower energy impacts.
The kidneys are located in a relatively well-protected position in the loin area, protected by the transverse processes of the spine and the lower and posterior ribs.
The anatomy and blood supply for the solid organs are different. Seventy percent of the liver blood supply comes from the portal venous system, which is a low-pressure system. Only 20% of the liver blood supply is provided at arterial pressures. This contributes to
the natural history of bleeding from the liver, which is described below. The hepatic veins coalesce superiorly to join the retro- and suprahepatic portion of the inferior vena cava. Therefore, injuries of the liver on the diaphragmatic surface are more likely to involve large hepatic veins and injuries of the liver on the portal surface are more likely to involve hepatic artery or portal venous structures. These considerations are important in choosing between options for operative management.
The blood supply to the spleen and kidney are arterial, i.e. at arterial pressure. Classically, a large splenic artery, which 85% of the time bifurcates into two branches of superior and inferior, supplies the spleen. In approximately 15% of spleens, there is a middle splenic artery. The splenic artery generally divides prior to entering the substance of the spleen and is therefore a favorable anatomic configuration for managing certain injuries with hemisplenectomy when the injury is confined to either the superior or the inferior portions of the spleen. The large veins and large arteries are on the hilar surface of the spleen, making superficial cracks on the lateral aspect of the spleen more easily controlled by pressure or other nonspecific techniques. Whereas, injuries in the hilar surface of the spleen more commonly require definitive management, either by ligation of the vessel of removal of that portion or the entire spleen.
The anatomy of the kidney includes both arterial and venous supply and outflow, which arrive at the hilum. There are commonly multiple or accessory renal artery branches, which may be avulsed leading to an ischemic area of the kidney, which is interpreted as a parenchymal injury or laceration. The kidney is surrounded by a dense, thick capsule and incorporated in Gerota’s

Panam J Trauma
44 Marzo 2004
Solid Organs - Are They All the Same?
45Vol. 11 Number 1
fascia, which firmly contains hemorrhage. Therefore, low-pressure sources of bleeding will generally be self-limited and only those injuries, which either transgress these capsules or are large arterial sources of bleeding, will bleed persistently.
The natural history of injuries of the solid organs is quite different. Liver injuries in general, once they stop bleeding, will not reinstitute bleeding. Whereas, the spleen, because of its thin pulp, flimsy capsule, and intraperitoneal location, more often presents delayed bleeding or delayed recognition of rupture. Intrahepatic arteries may be contained by the pulp of the spleen for some period of time and ultimately rupture through the parenchyma of the spleen or the peritoneal cavity producing hemorrhage which is brisk and resulting in hemodynamic derangement of the patient and requiring an urgent operation. On the other hand, liver injuries that fail operative management generally do not fail in this catastrophic manner. The typical history would be the recognition of persistent, gradual drop in hematocrit or hemoglobin and the requirement of transfusion or fluid boluses in a patient who is hemodynamically rather stable, ultimately prompting either arteriography or re-operation. The other two common causes of failure for liver laceration are bile leak requiring either operation or percutaneous drainage or rupture of pseudoaneurysm of the hepatic artery branch into an adjacent injury of the bile duct, leading to hematobilia. This condition is best managed by angio-embolization.
The function of the various solid organs impact profoundly on the surgical options and indications for surgery. The spleen is a single organ and not essential for life. Its primary function is hematologic and immunologic. Loss of the spleen earlier in life results in a higher risk of subsequent overwhelming post splenectomy infection. The loss of the function of the spleen mandates vaccination of patients who are treated with splenectomy.
The liver on the other hand is a single, indispensable organ and cannot be routinely removed, which is an extremely important option in hemorrhage control of both the spleen and the kidney. The kidney is a paired organ and may be removed for massive bleeding or repaired. The two functional nuances of kidney injuries have
to do with urine leak, which can often be managed by percutaneous drainage or by percutaneous nephrostomy but may require direct operative repair. The other function of the kidney relates to its production of renin, which stimulates the conversion of angiotensinogen into angiotensin. Occasionally patients with renal artery injury will develop renovascular hypertension and require follow-up and management of that condition.
In general, the natural history of the liver is that once bleeding has stopped it will generally stay stopped. Failed nonoperative management of the liver is generally not catastrophic or sudden as in ruptured splenic hematoma or renal hematoma. In general, indications for operating on splenic injuries and nonoperative management of splenic injuries have been well studied. Splenic injuries are graded 1 through 5. The failure rate of nonoperative management of splenic injuries for those grades is: Grade 1 - 5%; Grade 2 - 10%; Grade 3- 20%; Grade 4- 33%; and Grade 5 - 75%. Therefore, the grade of the injury itself is much more influential in the decision to operate on a patient. In fact, in general, Grade 4 and 5 injuries should be managed operatively and Grade I and 2 injuries can generally be managed nonoperatively. The Grade 3 injuries are a source of controversy. It is my personal recommendation that Grade 3 injuries in the polytrauma patient or in patients who have exhibited any evidence of hemodynamic instability, including persistent tachycardia, should have operative repair of their spleen. Those Grade 3 injuries in patients whose injuries are isolated to the spleen, for example those who have fallen off a horse or a direct blow to the left flank, have an 80% chance of success with nonoperative management. The difference in the management for those patients is the return to normal daily function without a laparotomy incision within a few days to weeks compared to the recovery time of a laparotomy. On the other hand, the patient with multiple injuries, for instance bilateral femur fracture or spinal cord injury, the 1 in 5 risk of subsequent bleeding in those patients is less well tolerated and the impact of laparotomy on the time course of the recovery in the context of multiple or severe fractures, head injury, spinal cord injury, etc. is much less. For most of these patients, a laparotomy incision is not the limiting facture to determine when they are able to return to a productive life style.
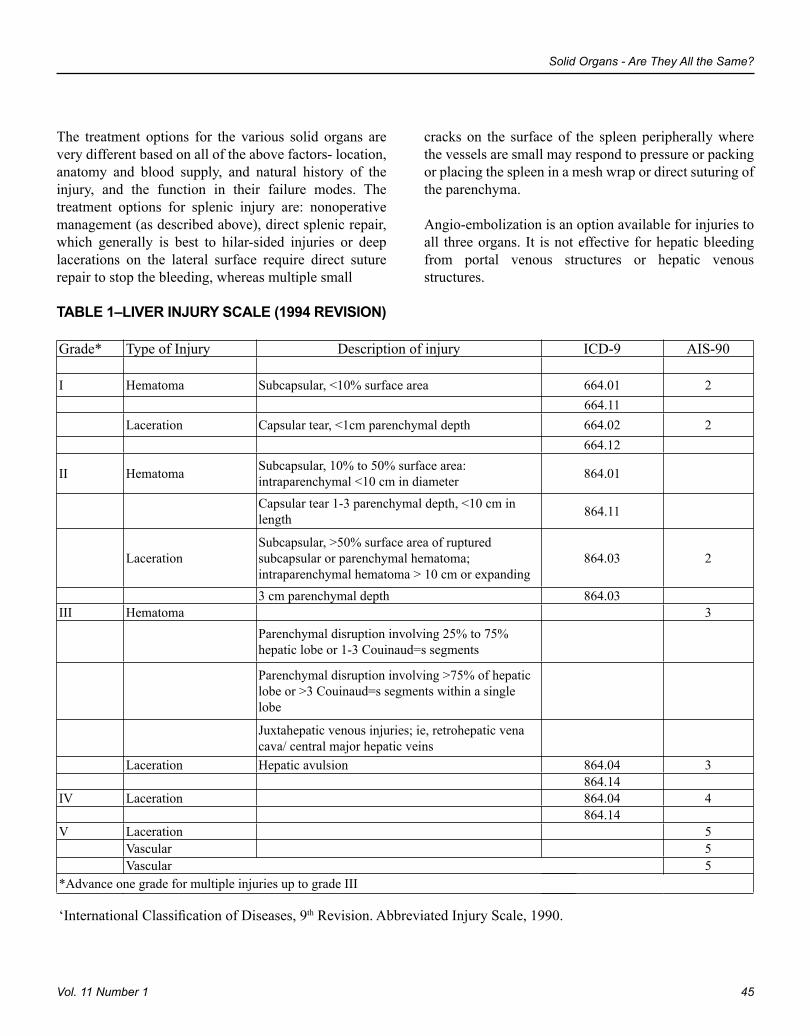
Panam J Trauma
44 Marzo 2004
Solid Organs - Are They All the Same?
45Vol. 11 Number 1
The treatment options for the various solid organs are very different based on all of the above factors- location, anatomy and blood supply, and natural history of the injury, and the function in their failure modes. The treatment options for splenic injury are: nonoperative management (as described above), direct splenic repair, which generally is best to hilar-sided injuries or deep lacerations on the lateral surface require direct suture repair to stop the bleeding, whereas multiple small
TABLE 1–LIVER INJURY SCALE (1994 REVISION)
Grade* Type of Injury Description of injury ICD-9 AIS-90
I Hematoma Subcapsular, <10% surface area 664.01 2 664.11 Laceration Capsular tear, <1cm parenchymal depth 664.02 2 664.12
II Hematoma Subcapsular, 10% to 50% surface area: intraparenchymal <10 cm in diameter 864.01
Capsular tear 1-3 parenchymal depth, <10 cm in length 864.11
LacerationSubcapsular, >50% surface area of ruptured subcapsular or parenchymal hematoma; intraparenchymal hematoma > 10 cm or expanding
864.03 2
3 cm parenchymal depth 864.03III Hematoma 3
Parenchymal disruption involving 25% to 75% hepatic lobe or 1-3 Couinaud=s segments
Parenchymal disruption involving >75% of hepatic lobe or >3 Couinaud=s segments within a single lobe
Juxtahepatic venous injuries; ie, retrohepatic vena cava/ central major hepatic veins
Laceration Hepatic avulsion 864.04 3 864.14IV Laceration 864.04 4 864.14V Laceration 5
Vascular 5Vascular 5
*Advance one grade for multiple injuries up to grade III
‘International Classification of Diseases, 9th Revision. Abbreviated Injury Scale, 1990.
cracks on the surface of the spleen peripherally where the vessels are small may respond to pressure or packing or placing the spleen in a mesh wrap or direct suturing of the parenchyma.
Angio-embolization is an option available for injuries to all three organs. It is not effective for hepatic bleeding from portal venous structures or hepatic venous structures.
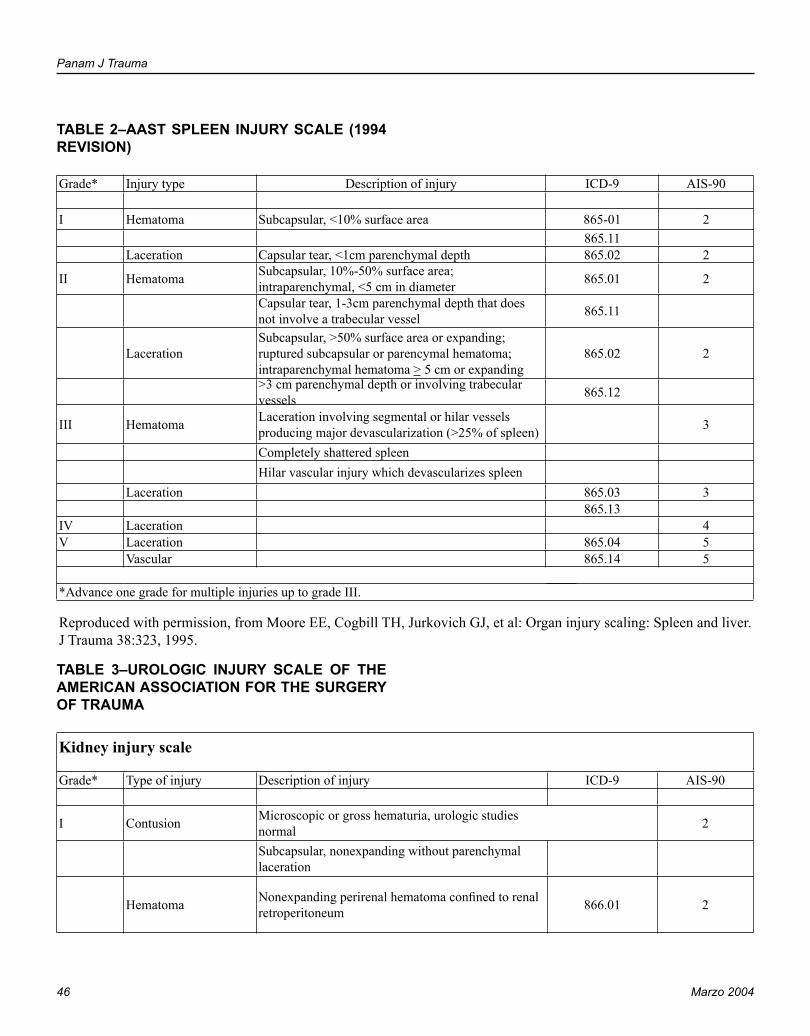
Panam J Trauma
46 Marzo 2004
Solid Organs - Are They All the Same?
47Vol. 11 Number 1
TABLE 2–AAST SPLEEN INJURY SCALE (1994 REVISION)
Grade* Injury type Description of injury ICD-9 AIS-90
I Hematoma Subcapsular, <10% surface area 865-01 2 865.11 Laceration Capsular tear, <1cm parenchymal depth 865.02 2
II Hematoma Subcapsular, 10%-50% surface area; intraparenchymal, <5 cm in diameter 865.01 2
Capsular tear, 1-3cm parenchymal depth that does not involve a trabecular vessel 865.11
LacerationSubcapsular, >50% surface area or expanding; ruptured subcapsular or parencymal hematoma; intraparenchymal hematoma > 5 cm or expanding
865.02 2
>3 cm parenchymal depth or involving trabecular vessels 865.12
III Hematoma Laceration involving segmental or hilar vessels producing major devascularization (>25% of spleen) 3
Completely shattered spleen Hilar vascular injury which devascularizes spleen Laceration 865.03 3 865.13IV Laceration 4V Laceration 865.04 5
Vascular 865.14 5
*Advance one grade for multiple injuries up to grade III.
Reproduced with permission, from Moore EE, Cogbill TH, Jurkovich GJ, et al: Organ injury scaling: Spleen and liver. J Trauma 38:323, 1995.
TABLE 3–UROLOGIC INJURY SCALE OF THE AMERICAN ASSOCIATION FOR THE SURGERY OF TRAUMA
Kidney injury scale
Grade* Type of injury Description of injury ICD-9 AIS-90
I Contusion Microscopic or gross hematuria, urologic studies normal 2
Subcapsular, nonexpanding without parenchymal laceration
Hematoma Nonexpanding perirenal hematoma confined to renal retroperitoneum 866.01 2
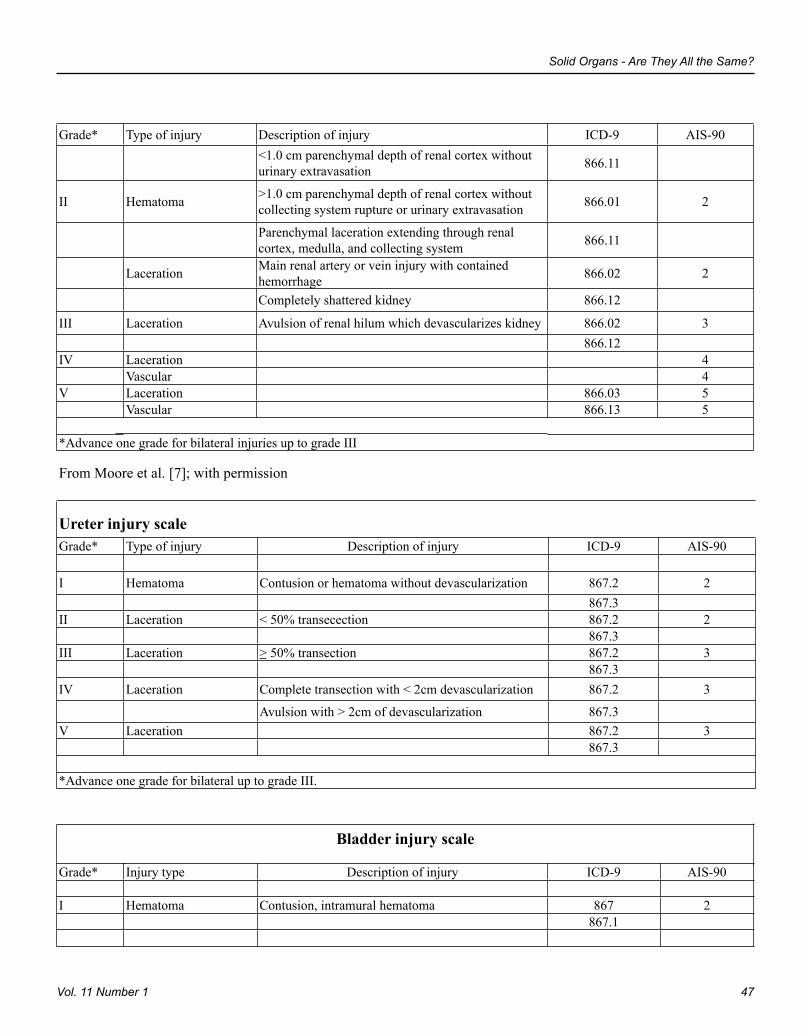
Panam J Trauma
46 Marzo 2004
Solid Organs - Are They All the Same?
47Vol. 11 Number 1
Grade* Type of injury Description of injury ICD-9 AIS-90
<1.0 cm parenchymal depth of renal cortex without urinary extravasation 866.11
II Hematoma >1.0 cm parenchymal depth of renal cortex without collecting system rupture or urinary extravasation 866.01 2
Parenchymal laceration extending through renal cortex, medulla, and collecting system 866.11
Laceration Main renal artery or vein injury with contained hemorrhage 866.02 2
Completely shattered kidney 866.12
III Laceration Avulsion of renal hilum which devascularizes kidney 866.02 3 866.12IV Laceration 4 Vascular 4V Laceration 866.03 5
Vascular 866.13 5
*Advance one grade for bilateral injuries up to grade III
From Moore et al. [7]; with permission
Ureter injury scaleGrade* Type of injury Description of injury ICD-9 AIS-90
I Hematoma Contusion or hematoma without devascularization 867.2 2 867.3II Laceration < 50% transecection 867.2 2 867.3III Laceration > 50% transection 867.2 3 867.3IV Laceration Complete transection with < 2cm devascularization 867.2 3
Avulsion with > 2cm of devascularization 867.3V Laceration 867.2 3
867.3
*Advance one grade for bilateral up to grade III.
Bladder injury scale
Grade* Injury type Description of injury ICD-9 AIS-90
I Hematoma Contusion, intramural hematoma 867 2 867.1
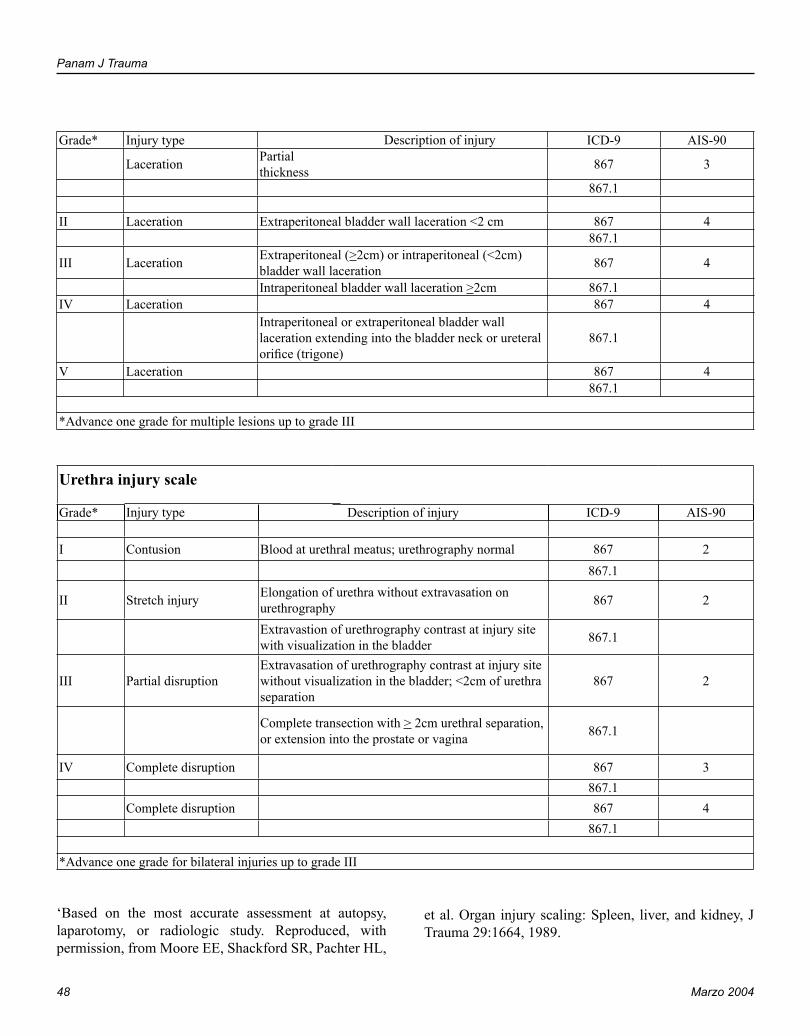
Panam J Trauma
48 Marzo 2004
Solid Organs - Are They All the Same?
49Vol. 11 Number 1
Grade* Injury type Description of injury ICD-9 AIS-90
Laceration Partial thickness 867 3
867.1
II Laceration Extraperitoneal bladder wall laceration <2 cm 867 4 867.1
III Laceration Extraperitoneal (>2cm) or intraperitoneal (<2cm) bladder wall laceration 867 4
Intraperitoneal bladder wall laceration >2cm 867.1IV Laceration 867 4
Intraperitoneal or extraperitoneal bladder wall laceration extending into the bladder neck or ureteral orifice (trigone)
867.1
V Laceration 867 4 867.1
*Advance one grade for multiple lesions up to grade III
Urethra injury scale
Grade* Injury type Description of injury ICD-9 AIS-90
I Contusion Blood at urethral meatus; urethrography normal 867 2 867.1
II Stretch injury Elongation of urethra without extravasation on urethrography 867 2
Extravastion of urethrography contrast at injury site with visualization in the bladder 867.1
III Partial disruptionExtravasation of urethrography contrast at injury site without visualization in the bladder; <2cm of urethra separation
867 2
Complete transection with > 2cm urethral separation, or extension into the prostate or vagina 867.1
IV Complete disruption 867 3 867.1Complete disruption 867 4
867.1
*Advance one grade for bilateral injuries up to grade III
‘Based on the most accurate assessment at autopsy, laparotomy, or radiologic study. Reproduced, with permission, from Moore EE, Shackford SR, Pachter HL,
et al. Organ injury scaling: Spleen, liver, and kidney, J Trauma 29:1664, 1989.
Panam J Trauma
48 Marzo 2004
Solid Organs - Are They All the Same?
49Vol. 11 Number 1
BIBLIOGRAPHY
1. Malhotra AK, Fabian TC, Croce MA, et al. Blunt hepatic injury: A paradigm shift from operative to nonoperative management in the 1990s. Ann Surg 2000;231(6):804-811, discussion 812-813.
2. Meredith JW, Young JS, Bowling J, Roboussin D. Nonoperative management of blunt hepatic trauma: The exception or the rule? J Trauma 1994;36(4):529-534; discussion 534-535.
3. Peitzman AB, Heil B, Rivera L, et al. Blunt splenic injury in adults: Multi-institutional study of the Eastern Association for the Surgery of Trauma. J Trauma 2000; 49(2): 177-187; discussion 187-188.
4. Bee TK, Croce MA, Miller PR, et al. Failures of splenic
nonoperative management: Is the glass half-empty or half full? J Trauma. 2001;50(2):230-236
5. Davis KA, FabiaN TC, Croce MA, et al. Improved success in nonoperative management of blunt splenic injuries: Embolization of splenic artery pseudoaneurysms. J Trauma. 1998; 44:1008-1015.
6. Schurr MJ, Fabian TC, Gavant M, et al. Management of blunt splenic trauma: Computed tomographic Contrast blush predicts failure of nonoperative management. J Trauma 1995; 39:507-513.
7. Croce MA, Fabian TC, Menke PG et al. Nonoperative Management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients: Results of a prospective trial. Ann Surg 1995;221(6):744-755.
Panam J Trauma 2004, 11:1
50
Surgical Simulation in Trauma Care
51Vol. 11 Number 1
SURGICAL SIMULATION IN TRAUMA CARELenworth M. Jacobs, MD, MPH, FACS.
Professor of Surgery, Professor and Chairman, Department of Traumatology and Emergency Medicine. University of Connecticut School of Medicine Director, EMS/Trauma Program Hartford Hospital
The ability of surgeons to competently and effectively manage operative penetrating torso trauma depends upon their total caseload and frequency of exposure to these types of injuries. However, residents and practicing surgeons have limited experience with operative trauma for a number of reasons. The incidence of penetrating trauma has been decreasing throughout the United States and currently represents approximately 15% of trauma admissions nationwide. Non-operative management for blunt injuries has become increasingly common, with less than 25% of all trauma patients requiring an immediate operation of any type. Both changes have decreased the number of operative trauma cases for the average surgeon and surgical resident. Military conflicts, which previously were a fertile training ground for surgeons, more recently result in decreasing numbers of wounded American soldiers. The last conflict involving major casualties was the Vietnam War, in which more than 58,000 soldiers perished and many more were injured in combat. The consequences of declining exposure to trauma surgery are a decrease in surgeons’ confidence for managing penetrating injuries and the potential for an increase in morbidity and mortality.
Surgical simulators have become increasingly sophisticated and complex in the last decade. The use of 3-D imaging with computer simulation has allowed the surgical user to interact with a computer simulation in such a way that the operator develops both cognitive as well as hand and eye coordination skills. In the last year, there has been increasing use and sophistication
of HAPTICS in both laparoscopy and other computer simulation. This technique has begun to explore giving resistances to the various instruments which simulate the passage of a needle through tissue or the path of a knife through skin or other tissues. These techniques are becoming increasingly realistic.
In the endoscopic arena, there are now simulators for bronchoscopy and colonoscopy which are extremely lifelike. In bronchoscopy not only does the user place the scope into a mannequin and obtains real images, but these images have the ability to give educational outputs such as anatomic labeling of various structures. It also allows the user to perform biopsies of various tissues. The device allows enable the user to give drugs to mitigate cough reflexes or pain. The results of these interventions and treatments are given a score which is maintained in the computer database for objective evaluations. The same kind of technology is in place for colonoscopy. It includes extremely lifelike sounds which are emitted from the mannequin when a pain-eliciting move is created with the scope. It is even more interesting to use the scope to observe the interior service of the anal sphincter. These views are extremely lifelike. The user is left with the distinct impression that he or she has performed a real bronchoscopy or colonoscopy in a real patient.
Even as these devices become more and more realistic and lifelike with increasing attention paid to tissue tensions, the models do not fully capture the realistic operating room auditory and tactile cues of operating upon real tissue. The other ‘simulation’ is to utilize the large animal model with real injuries which are derived from a real human environment. The Advance Trauma Operative Management Course (ATOM) has been

Panam J Trauma 2004, 11:1
50
Surgical Simulation in Trauma Care
51Vol. 11 Number 1
developed to take advantage of penetrating injuries in a large swine and in so doing simulate the same injury in the human.
The purpose of the ATOM course is to educate surgeons on the surgical management of penetrating injuries, to improve their self-confidence in managing these injuries, and to assure their technical competence in the surgical repair of penetrating injuries. The intended audience is senior surgical residents, trauma fellows, military surgeons, and fully trained general surgeons who are infrequently called upon to treat penetrating injuries. A.T.O.M. is a tightly structured educational experience with a rigorous evaluative component. It is designed to be completely reproducible.
The didactic portion of the course is comprised of six 30-minute lectures covering the basic principles of the trauma laparotomy and damage control, management of abdominal and thoracic injuries, as well as injuries to the heart and major vessels. These lectures, supported with power point presentations, contain uniform content and illustrations, which can be given in a reproducible fashion by different instructors.
The surgical laboratory exercises consist of scenarios of penetrating trauma to the small bowel, bladder, duodenum, kidney, ureter, spleen, diaphragm, stomach, pancreas, liver, inferior vena cava, and heart. Participants are blind to the number or types of injuries. As with the lectures the operative scenarios adhere to uniform content. Following the presentation of case scenarios by the instructor, participants are expected to assess the history of the traumatic event, evaluate appropriate investigations, and then perform the appropriate surgery based on the identification of injuries. The human operative environment is reproduced as closely as possible with the use of a 50-kilogram swine. This animal was chosen because its abdominal cavity approximates the size of an average adult human. Anatomic differences between the swine and human are reviewed at the start of the operative laboratory. The injuries are created in a consistent manner so that each course participant has a similar learning experience.
For the affective domain, an instrument to measure self-efficacy was developed with items reflecting the skills
taught in the course. Self-efficacy refers to peoples’ judgments of their capabilities to achieve successful performance. Persons with high levels of confidence for a particular task readily and successfully perform the task while those low in self-efficacy avoid or abandon the task. The self-efficacy questionnaire requires that the participant rate his/her confidence in performing twenty-five surgical tasks. The participant used a scale of one to five to rate his/her confidence. A score of one indicated very little self-confidence. A score of five indicated quite a lot of self-confidence. The highest possible total score is 125. The participant’s total score was then divided by 25 (the number of items) to approximate each participants overall confidence level.
The self-efficacy instrument was also evaluated for content validity by the national expert panel. In addition, further support of validity was assessed through a process commonly referred to as “known groups”. For this, the instrument was administered to groups that would be expected to score differently, from low to high, on confidence for performing the surgical procedures. The groups included anesthesiologists, emergency department physicians, junior surgical residents, senior surgical residents, trauma fellows, surgical attendings, and expert traumatologists. Anesthesiologists and emergency physicians while having knowledge of surgical techniques would not be expected to be competent in performing complex trauma surgery and would therefore understandably have lower self-confidence in performing such procedures.
For the psychomotor domain, an operative performance evaluation was designed. The participants were evaluated based on a preset series of critical behaviors for each injury. The critical behaviors are those actions required to perform essential skills. These are identification of the injury, formulation of a treatment plan, and successful repair of the injury. The participants were judged on a 3-point scale reflecting the degree of assistance required to complete the task. One point was awarded if one could not successfully complete the task, two points if he/she required some assistance in completing the task, and three points if he/she completed the task independently. The maximum number of points for the entire exercise is 81. To ensure consistent use of the operative performance evaluation, instructors were briefed regarding the critical

Panam J Trauma
52 Marzo 2004
Surgical Simulation in Trauma Care
53Vol. 11 Number 1
behaviors that the participant was required to perform. A list of these behaviors was conveniently located in the laboratory for easy reference. The operative performance evaluation was assessed for content validity by the national expert panel. In addition, interrater agreement was assessed when two instructors simultaneously and independently rated 12 participants.
DISCUSSION
Surgical education has traditionally relied on the experiential model. The surgical trainees have been expected to spend a substantial number of hours in the clinical environment where they see and evaluate clinical patients and perform a large number of operative procedures. The learning process is developed by an experienced mentor precepting the trainee through all aspects of the nonoperative and operative experience. As the number of procedures increases, the level of competence increases until the preceptor determines that the trainee is ready for independent and autonomous practice.
In the trauma environment where there are frequently multiple organ systems and multiple body cavities that have been injured. The decision-making is complex and difficult. It takes many clinical events to become confident in managing injuries that cause multiple body systems to fail simultaneously. Currently, obtaining experience with sufficient cases is difficult as the number of hours worked per week by the surgical trainee has decreased from approximately 120 hours to 80 hours a week In order to obtain the same amount of experience, in a true experimental model, it would be logical to lengthen the number of years in surgical training. However, the constraints on reimbursement for extra years of training placed by the federal government is such that extending the number of years of surgical education is unlikely.
In addition, to the reduced working hours, surgical residents are faced with an increased number of operations that must be learned. The adoption of minimally invasive procedures requires the resident to become competent in these as well as the traditional invasive operations. Thus, again the experiential learning model is severely challenged and creates a situation where surgeons are
now being required to demonstrate competency with decreasing real life experience.
Coinciding with the decrease in working hours, and the increase in the number of procedures to learn, there is increased scrutiny of surgeons’ operative experience and competency. There is also a corresponding increase in regulations required for credentialing surgeons to perform specific procedures and demonstrate competence in the psychomotor as well as the cognitive domain. In addition, registries that make public record of morbidity and mortality rates of individual surgeons are becoming commonplace.
All of these factors, the reduced working hours, the increased number of procedures to learn, and new regulatory requirements, have made it necessary for surgical educators to look at other medical specialties and industries to see how they have managed similar challenges.
Programs have been developed in ophthalmology, gynecology and laparoscopy to teach operative skills with simulation models. The trauma literature also reflects this trend with reports of simulated models of trauma patients for practice of resuscitation and operative skills. To this end there have been revisions to the Advanced Trauma Life Support course (ATLS) format to include more interactive and life-like situations. These changes to the ATLS format have produced improved clinical performance both initially and at 2 years after the course. This format of interactive lectures together with patient simulation exercises used in the revised ATLS is similar to the format that was used in the A.T.O.M. course. However, the experience of managing a live animal cannot be matched.
Like medicine, the aviation industry has been faced with increased public and regulatory scrutiny. As aircraft have become more sophisticated, demands on the pilots have dramatically increased. In order to provide pilots with the training necessary to fly modern aircraft and deal with complex problems, simulated models have been implemented. These models provide the trainees auditory, visual, and tactile cues that drive cognitive processes and psychomotor behaviors. The use of simulated models in the aviation industry is now the
Panam J Trauma
52 Marzo 2004
Surgical Simulation in Trauma Care
53Vol. 11 Number 1
accepted standard of ensuring that the pilot is competent to fly and manage the complexities of the modern aviation environment. Similarly, surgical education must find a way to deal with its challenges. A.T.O.M. is a step in that direction.
This course makes use of simulation to create life-like situations in order to train surgeons to perform operative procedures competently. In order to maximally prepare the participant for a realistic experience, the human operating room environment is reconstructed completely in the animal laboratory. The auditory cues from the anesthesia and EKG machines as well as prompts from the anesthesiologist such as when the animal becomes hypotensive, induce the real stresses experienced in the operating room. Similarly, the experience of having to listen to a history of the event and evaluate appropriate investigations and then perform an exploratory laparotomy without knowing how many or what type of injuries are present recreates the human operative experience. The experience is enhanced as the injuries become more severe and hemorrhage in the abdominal cavity is obvious. The injury to the inferior vena cava produces massive hemorrhage which requires immediate control or the animal will exsanguinate. Most students report that the visual, auditory, and actual experience during the operation so mimic the human environment that they have no difficulty in believing that this is a similar experience to the human penetrating trauma event.
Difficulties assessing the psychomotor skills of surgical trainees have been described and there is a substantial challenge to fairness and objectively determining competence. The course also promotes a collegial dialogue between surgeons and provides a new and effective method of continuing surgical education. Participants have reported using the knowledge and skills gained from A.T.O.M. in actual trauma cases with good results.
BIBLIOGRAPHY
1. National Trauma Data Bank Report 2001.
2. Rotondo MF, McGonigal MD, Schwab CW, Kauder DR, Angood PB. On the nature of things still going bang in the night: An analysis of residency training in trauma. J Trauma
1993;35:550-555.
3. Hawkins ML, Wynn JJ, Schmacht DC, Medeiros RS, Gadacz TR. Non-operative management of liver and/or splenic injuries: Effect on resident surgical experience. Am Surg 1998;64:552-557.
4. Lukan JK, Carrillo EH, Franklin GA, Spain DA, Miller FB, Richardson JD. Impact of recent trends of noninvasive trauma evaluation and non-operative management in surgical resident education. J Trauma 2001;50:1015-1019.
5. Barnes RW, Whiteside MF, Eisner JA, Lang NP, Campbell GS. The Good Ol’ Days is now: Trends in operative experience of general surgical residents over 25 years. Am Surg 1988;54:395-401.
6. Combat Area Casualty File, December 1998, Center for Electronic Records, National Archives and Records Administration, Washington, DC.
7. Bandura, A. Social Foundations of Thought and Action, A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall; 1986.
8. Jacobs L, et al. EAST Issues Seminar: The education of the trauma surgeon in the 21st century. J Trauma 31:1122, 1991.
9. Sinclair MJ, Peifer JW, Haleblian R, Luxenberg MN, Green K, Hull DS. Computer-simulated eye surgery. A novel teaching method for residents and practitioners. Ophthalmology 1995;102:517-521.
10. Lentz GM, Mandel LS, Lee D, Gardella C, Melville J, Goff BA. Testing surgical skills of obstetric and gynecologic residents in a bench laboratory setting: validity and reliability. Am J Obstet Gynecol 2001;184:1462-1468.
11. Levy JS. Virtual reality hysteroscopy. J Am Assoc Gynecol Laparosc 1996;3:S25-26.
12. Smith CD, Farrell TM, McNatt SS, Metreveli RE. Assessing laparoscopic manipulative skills. Am J Surg 2001;181:547-550.
13. Larsson A. Intracorporeal suturing and knot tying in surgical simulation. Stud Health Technol Inform 2001;81:266-271
14. Devarajan V, Scott D, Jones D, et al. Bimanual hepatic workstation for laparoscopic surgery simulation. Stud Health Technol Inform 2001;81:126-128.
15. Oppenheimer P, Weghorst S, Williams L, et al. Laparoscopic surgical simulator and port placement study. Stud Health Technol Inform 2000;70:233-235.
Panam J Trauma
54 Marzo 2004
16. Tseng CS, Lee YY, Chan YP, Wu SS, Chiu AW. A PC-based surgical simulator for laparoscopic surgery. Stud Health Technol Inform 1998;50:155-160
17. Jacobs LM, Lorenzo C, Brautigam RT. Definitive Surgical Trauma Care Live Porcine Session: A technique for training in trauma surgery. Conn Med 2001;65:265-268
18. McLellan BA. Early experience with simulated trauma resuscitation. Can J Surg 1999;42:205-210
19. Marshall RL, Smith JS, Gorman PJ, Krummel TM, Haluck RS, Cooney RN. Use of a human patient simulator in the development of resident trauma management skills. J Trauma 2001;51:17-21
20. Knudson MM, Sisley AC. Training residents using simulation
technology: Experience with ultrasound for trauma. J Trauma 2000;48:659-665
21. Ali J, Gana TJ, Howard M. Trauma mannequin assessment of management skills of surgical residents after Advanced Trauma Life Support training. J Surg Res 2000;93:197-200
22. Ali J, Adam R, Pierre I, Bedaysie H, Josa D, Winn J. Comparison of performance 2 years after the old and new (Interactive) ATLS courses. J Surg Res 2001;97:71-75
23. Trunkey DD, Botney R . Assessing competency: A tale of two professions. J Am Coll Surg 192:385, 2001
24. Darzi A, Datta V, Mackay S. The challenge of objective assessment of surgical skill. Am J Surg 181:484, 2001
Panam J Trauma 2004, 11:1
55
THE BLUSHING CT SCAN - WHOSE VENUE?Stuart E. Mirvis, MD, FACR.
Professor of Radiology Chief, Trauma and Emergency Radiology Section, Department of Radiology University of Maryland School of Medicine Baltimore, Maryland
INTRODUCTION Vascular injuries are frequently recognized during intravenously enhanced CT scans of patients sustaining both penetrating and blunt abdominal-pelvic trauma. While such lesions were occasionally recognized using conventional CT technology, the increased use of single and particularly multi-detector row CT has made this a commonly place finding. This increased sensitivity for recognition of vascular injury is the result of increased spatial resolution made possible by thin-slice thickness and higher intra-arterial contrast levels achieved within the organ parenchyma at the time of the scan made possible by bolus tracking technology. The finding of a vascular injury has direct implications on patient management over and above information regarding parenchmal disruption and physical examination findings alone.
THE CT APPEARANCE OF VASCULAR INJURY
The presence of high-density intra-vascular contrast permits direct and specific visualization of vessels. If the contrast material achieves peak density within the arteries at the time the image is acquired they will have very high density. Vascular lesions can appear as pseudoaneurysms, dissection of contrast within the organ parenchyma, or free extravasation of contrast into a low-pressure space such as the peritoneal cavity, gastric or bowel lumen, lesser sac. Iodinated blood can also be seen to dissect within tissue planes with the solid organs, body wall, retroperitoneum, and mesentery.
• Pseudoaneurysms appear has rounded collections of contrast that “wash-out” near completely on delayed imaging
• Extravasated contrast remains contained within a closed space such as an organ, appears irregular in shape, and persists within the tissue on delayed imaging
• Free bleeding usually appears as a linear collection of contrast that is communicating with a low-pressure space adjacent to the site of hemorrhage that shows expansion (a wider area of extravasation) on delayed images. This type of bleeding is the most rapid and has significant implications for urgent treatment.
• Arterio-venous malfomation: These usually result from penetrating injury and are frequently visualized on CT due to the improved “temporal resolution” of current multi-slice CT units. Early filling of adjacent veins adjacent to the arterial injury can be appreciated on the CT images. Reformation of data into volume rendered views can improve appreciation of the vascular anatomy for bothh AVMs and pseudoaneurysms.
Extravasated contrast is typically surrounded by lower density hematoma from previously extravasation of non-opacified blood. The hematoma typically has a density of 70-90 Hounesfield Units (HU) depending both on the hematocrit and degree of clot retraction. Liquid blood that is also often present around sites of injury typically has a density of 30-45 HU depending on these same factors. The density of blood may however decrease further with admixture of more watery fluids such as urine, bile, or intestinal content. If multiple sites of blood are present

Panam J Trauma
56 Marzo 2004
The Blushing CT Scan - Whose Venue?
57Vol. 11 Number 1
within the peritoneal cavity, the collection with the highest CT density is usually in closest proximity to the source of bleeding (the “sentinel” clot sign).
The location of the vascular blush and the type of vascular injury demonstrated has direct implications for treatment. A study by Yao et al including four major trauma centers reported an 18% incidence of contrast extravasation in various locations (104/565)
Pelvis
Active arterial hemorrhage is frequently demonstrated in patients with major pelvic fractures as a dense blush surrounded by lower density hematoma. Usually in this setting there is abundant extraperitoneal blood loss. Using single slice helical scanning, CT was 90% accurate in identifying active pelvic bleeding when compared to angiography. Pelvic arteriography is indicated to manage bleeding by endovascular occlusion. The prior CT can demonstrate that, in fact, active bleeding is present and the side involved. In turn, this information can indicate the need from arteriography and save time in reaching the most active bleeding site. In any case both sides of the pelvic arterial system need to be evaluated angiographically to look for injured, but not actively bleeding vessels.
Splenic Injury
Management of splenic injury has undergone some evolution in recent years with use of non-operative management becoming more common in hemodynamically stable patients. This approach requires appreciation of the extent of anatomic disruption and on-going physical findings. While the anatomic grade of injury does correlate strongly with likelihood of failure of non-operative treated, data developed since the mid 1990’s indicate that the presence of an arterial blush (pseudoaneurysm or intraprenchymal extravasation) is a far more powerful indicator of failure of non-operative management without intervention (p< 0.0001) compared to patients with spleen injury without a contrast blush. In our practice, patients with splenic vascular lesions undergo emergent arteriography and embolization that has been shown to improve successful non-operative outcome in these patients. In most cases the embolization
of performed using coils placed in the proximal splenic artery. The action lowers perfusion pressure but permits retained splenic function via collaterals. Some infarction of peripheral splenic tissue is not uncommon (63%) with this approach, but is usually not of clinical significance. Our angiography group has also performed selective distal splenic arterial branch embolization if the lesion is quite focal. This approach is more time-consuming and requires greater skill. While the vascular lesion is well occluded, distal tissue embolization is 100% and typically involves a larger volume than proximal embolization. Complications are rare with both methods. We have had occasion patients re-bleed via collaterals after proximal embolization and these have had secondary embolization through the initial coils with subsequent success in most cases. Patients with CT grade 3 injuries and below without vascular blushes on CT do not have urgent angiography, but may have elective angiography depending on precise clinical circumstances. Grade 4 splenic injuries (maceration, major devascularization are typically studied acutely by angiography or undergo surgery.
Liver Injury
Liver injury can also produce vascular lesions from blunt and penetrating sources. In general, the extent the parenchyma disruption or grade of injury is a poor predictor of the success of non-operative treatment. Most patients with liver injuries will ultimately do well as long as they are hemodynamically stable at admission. The influence of vascular injuries in treatment of liver trauma is less clear than for splenic injury. Children with a CT blush and injury grade 3-5 have statistically greater transfusions requirements and mortality risk than those without a blush and similar degree of liver parenchymal injury. It is our policy to angiographically study all patients with liver trauma who have a clear vascular injury on CT and to embolize any verified vascular lesions. In prospective CT studies of liver trauma, the occurrence of injuries near the major hepatic veins was a significant predictor of delay bleeding and other complications (p < .01) compared to those without involvement of major hepatic veins.. The appearance of a laceration extending into the main hepatic veins, particularly near the confluence with the IVC may warrant venography including the IVC and major veins

Panam J Trauma
56 Marzo 2004
The Blushing CT Scan - Whose Venue?
57Vol. 11 Number 1
to exclude injuries that may be less apparent in these low pressure vessels on CT. On occasion, intravascular stents can treat disruptions of these vessels, but at least better surgical planning will be permitted, if elected) when there is prior knowledge of this type of hepatic injury. Lacerations of the liver into the portal region and pericholecystic region were not significant risk factors for failure of non-operative treatment. As expected, most hepatic vascular injuries arise from the hepatic arterial branches. These can be occluded with impunity when necessary as long as portal venous flow is verified as intact.
Renal Trauma
Active bleeding can accompany major blunt renal injuries, typically associated with significant parenchymal disruption. Pseudoaneurysms and A-V fistulas are usually the result of penetrating injury. The timing of the CT scan is important in distinguishing bleeding of renal origin from leakage of iodinated urine from the collecting system. A blush noted on the initial arterial phase of the scan indicates arterial bleeding since there is insufficient time for excretion of iodinated urine into the collecting system. Delayed imaging, at 1-2 minutes after injection will reveal urine leakage and may also show residual foci of arterial contrast leak. Usually sites of renal hemorrhage are at the margins or torn parenchyma or centered within large hematomas adjacent to the kidney.
Pseudoaneurysms can typically be easily distinguished from arterial bleeding because of rapid dilution of the contrast on delayed scanning within a pseudoaneurysm. In most cases in which the patient is hemodynamically stable, arteriographic treatment of vascular lesions is possible. The advantage of this approach is the maimum preservation of renal tissue by use of very selective embolization of injured arterial branches. In general, the procedure is straightforward technically and successful in most cases. In the experience at the author’s institution, delayed complications (infection or hypertension) from management of major renal injury by interventional means is rare.
A small note of caution: contrast material from an
extraperitoneal bladder rupture can track up the retroperitoneal space to surround the kidney(s). This appearance could be mistaken for active bleed or contrast leak of renal origin. Since the urine is not iodinated until a few minutes after injection, the study should not suggest arterial injury with bleeding during the initial arterial phase scan.
Mesentery and Bowel
Active bleeding is usually easily recognized in the mesentery and may occasionally be observed extending into the bowel lumen. In most cases, the bright arterial contrast is surrounded by a lower density hematoma that is confined within the leaves of the mesentery and dissects along the mesentery. Bleeding that is free into the peritoneal space will not be confined in this fashion and more likely would present with hemodynamic instability or shock. Intraluminal oral contrast can rarely interfere with recognition of active bleeding. The detection of active bowel and mesenteric bleeding by CT is an indication for surgery as the integrity of the bowel and its viability cannot be discerned using CT early in the patient’s course.
Body Wall and Retroperitoneum
Bleeding into the body wall and retroperitoneum is again typically easy to identify as a hematoma with a bright center of arterial contrast. The location of this bleeding in closed spaces is often self-limited (particularly in the body wall). Of course, large vessel injury and coagulapathy can alter this tendency. Bleeding from lumbar, external iliac branches, epigastric, and phrenic vessels are all amenable to embolization if bleeding persists, although delineation of bleeding branches may be time-consuming. Bleeding in the anterior pararenal space may arise from duodenum, pancreas, colon, or the mesenteric root. These locations are sentinels indicating injury to the adjacent organ and will often, in this location require exploration to characterize and repair visceral injury.
Venous Bleeding
Bleeding of venous origin has been rarely mentioned in the literature, but will become more common given the

Panam J Trauma
58 Marzo 2004
capability of new 4, 8 and 16 slice scanners. Recently, the author has diagnosed several cases of active venous bleeding in major vessels based on CT findings. While the contrast level in the venous system is less than the arterial system and the pressure is lower, major injuries will still permit visualization of extravasated contrast due to improved temporal resolution of these scanners. Thus far, major venous injuries have been manages surgically in our practice, but are also amenable to stent-graft placement in selected cases with favorable anatomy.
A final note of caution: Often follow-up CT is performed after endovascular treatment of vascular injuries, such as the liver or spleen particularly. During the embolization procedure a significant amount of contrast may be extravasated around the site of injury and can persist for several days. It is important that this possibility be takan into account so that on repeat CT, this contrast from the arteriogram is not mistaken for on-going bleeding. A few non-contrast images through the organ of interest will clarify this issue prior to performing a full contrast-CT study.
BIBLIOGRAPHY
1. Eubanks JW 3rd, Meier DE, Hicks BA, Joglar J, Guzzetta PC. Significance of ‘bllush’ on computed tomography scan in children with liver injury. J Pediatr Surg 2003;38(3):363-366.
2. Ochsner MG. Factors of failure for nonoperative management of blunt liver and splenic injuries. World J Surg 2001;25(11):1393-96.
3. Poletti PA, Wintermark M, Schnyder P, Becker CD. Traumatic injuries: role of imaging in the management of the polytrauma victim (conservative expectation). Eur Radiol
2002;12(5):969-78.
4. Davis KA, Fabian TC, Croce MA, et al. Improved success in nonoative management of blunt splenic injuries: embolization of splenic artery pseudoaneurysm. J Trauma 1998;44(6):1008-13.
5. Cox CS Jr. Geiger JD, Liu DC, Garver K. Pediatric blunt abdominal trauma: role of computed tomography vascular blush. J Pediatr Surg 1997;32(8):1196-2000.
6. Schurr MJ, Fabian TC, Gavant M. et al. Management of blunt splenic trauma: computed tomographic contrast blush predicts failure of nonoperative management. J Trauma 1995;39(3):507-12.
7. Yao DC, Jeffrey RB Jr., Mirvis SE, et al. Using contrast-enhanced helical CT to visualize arterial extravasation after blunt abdominal trauma: incidence and organ distribution. AJR Am J Roentgenol 2002 ;178(1):17-20.
8. Killeen KL, Shanmuganathan K, Boyd-Kranis R, Scalea TM, Mirvis SE. CT findings after embolization for splenic trauma. J Vasc Interv Radiol 2001;12(2):209-14.
9. Poletti PA, Mirvis SE, Shanmuganathan K, Killeen KL, Coldwell D. CT criteria for management of blunt liver trauma: correlation with angiographic and surgical findings. Radiology 2000;21(6):418-427.
10. Cerva DS Jr., Mirvis SE, Shanmuganathan K, Kelly IM, Pais SO. Detection of bleeding in patients with major pelvic fractures:value of contrast CT. AJR Am J Roentgenol 1996;166(1):131-135.
11. Shanmuganathan K, Mirvis SE, Reaney SM. Pictorial review: CT appearances of contrast medium extravasations associated with injury sustained from blunt abdominal trauma. Clin Radiol 1995;50(3):182-187.





























