Embed Size (px)
Citation preview

11/25/2014
1
Palliative Care in Long Term Care
Leading Age New York DNS/DSW Annual Conference & Exposition
Nov. 21, 2014
Angela Katrichis, LMSW
The Community Hospice, Albany, NY
Inpatient Palliative Care Team at Ellis Medicine
George J. Giokas, M.D.
Director for Palliative Care, The Community Hospice, Albany, NY
Inpatient Palliative Care Team at Elis Medicine
Learning Objectives
• The learner will be able to identify 2 palliative care models applicable to long term care
• The learner will be able to name 3 recommended processes for advance care planning
• The learner will reflect on their values and preferences for their own end of life care
The presenters have no financial disclosures
Outline
• Define Palliative Care
• Palliative Care Models in LTC
• Clinical course of dementia patients
• Advance Care Planning
• Communication Skills
• MOLST
Your Work
1. Nursing
2. Social Work
3. Administrative
4. Other
Years of Clinical Experience
1. < 5 years
2. 5‐15
3. 16–30
4. Much too long
Favorite Spot on New Year’s Eve
A. Times Square
B. Secluded cabin in the woods
C. A cabana on the beach
11/25/2014
2
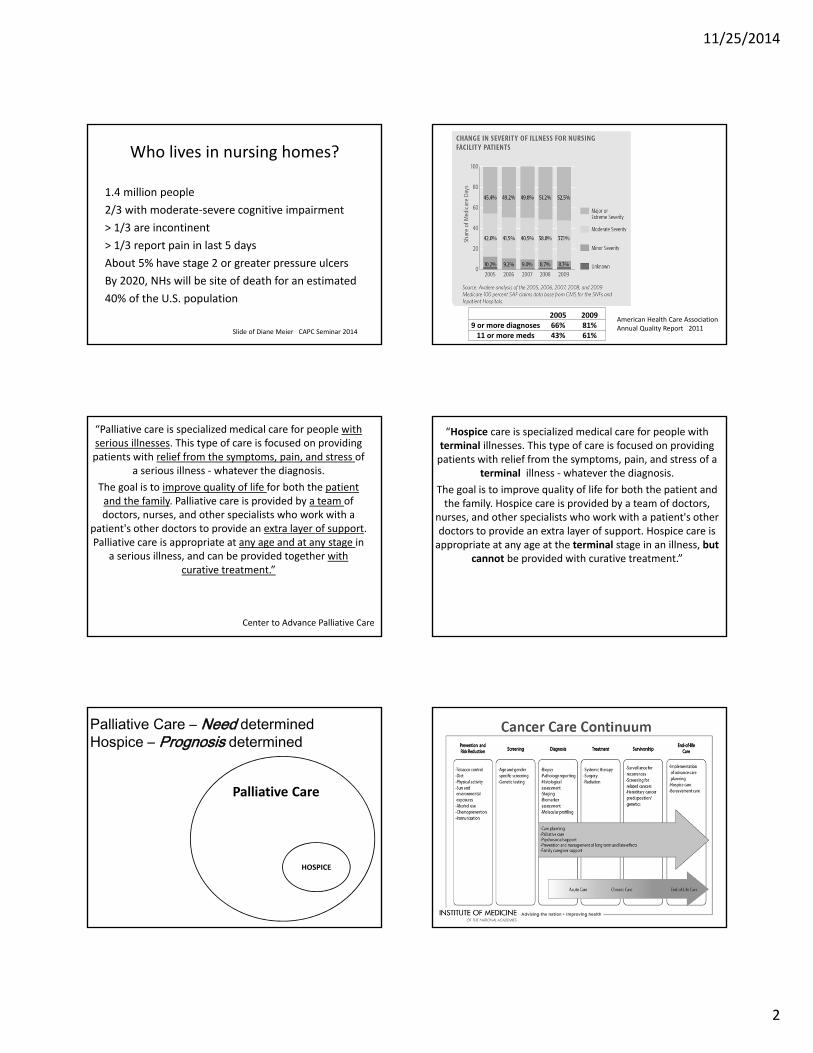
Who lives in nursing homes?
1.4 million people
2/3 with moderate‐severe cognitive impairment
> 1/3 are incontinent
> 1/3 report pain in last 5 days
About 5% have stage 2 or greater pressure ulcers
By 2020, NHs will be site of death for an estimated
40% of the U.S. population
Slide of Diane Meier CAPC Seminar 2014
2005 20099 or more diagnoses 66% 81%11 or more meds 43% 61%
American Health Care AssociationAnnual Quality Report 2011
“Palliative care is specialized medical care for people with serious illnesses. This type of care is focused on providing patients with relief from the symptoms, pain, and stress of
a serious illness ‐ whatever the diagnosis.
The goal is to improve quality of life for both the patient and the family. Palliative care is provided by a team of doctors, nurses, and other specialists who work with a
patient's other doctors to provide an extra layer of support. Palliative care is appropriate at any age and at any stage in
a serious illness, and can be provided together with curative treatment.”
Center to Advance Palliative Care
“Hospice care is specialized medical care for people withterminal illnesses. This type of care is focused on providing patients with relief from the symptoms, pain, and stress of a
terminal illness ‐ whatever the diagnosis.
The goal is to improve quality of life for both the patient and the family. Hospice care is provided by a team of doctors,
nurses, and other specialists who work with a patient's other doctors to provide an extra layer of support. Hospice care is appropriate at any age at the terminal stage in an illness, but
cannot be provided with curative treatment.”
Palliative Care – Need determinedHospice – Prognosis determined
Palliative Care
HOSPICE
11/25/2014
3
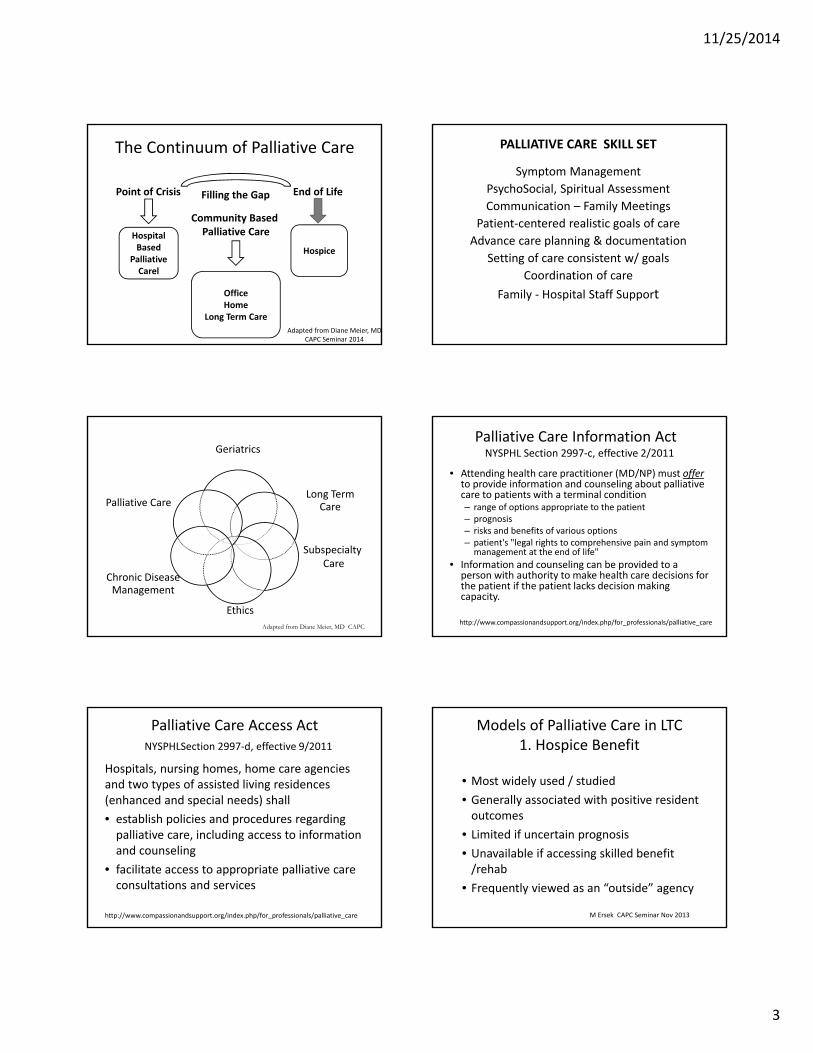
The Continuum of Palliative Care
Hospital Based
Palliative Carel
Hospice
Point of Crisis End of Life
OfficeHome
Long Term Care
Filling the Gap
Community Based Palliative Care
Adapted from Diane Meier, MDCAPC Seminar 2014
Symptom Management
PsychoSocial, Spiritual Assessment
Communication – Family Meetings
Patient‐centered realistic goals of care
Advance care planning & documentation
Setting of care consistent w/ goals
Coordination of care
Family ‐ Hospital Staff Support
PALLIATIVE CARE SKILL SET
Ethics
Geriatrics
Long Term Care
Chronic Disease Management
Palliative Care
Adapted from Diane Meier, MD CAPC
Subspecialty Care
Palliative Care Information ActNYSPHL Section 2997‐c, effective 2/2011
• Attending health care practitioner (MD/NP) must offerto provide information and counseling about palliative care to patients with a terminal condition – range of options appropriate to the patient – prognosis – risks and benefits of various options – patient's "legal rights to comprehensive pain and symptom management at the end of life"
• Information and counseling can be provided to a person with authority to make health care decisions for the patient if the patient lacks decision making capacity.
http://www.compassionandsupport.org/index.php/for_professionals/palliative_care
Palliative Care Access Act NYSPHLSection 2997‐d, effective 9/2011
Hospitals, nursing homes, home care agencies and two types of assisted living residences (enhanced and special needs) shall
• establish policies and procedures regarding palliative care, including access to information and counseling
• facilitate access to appropriate palliative care consultations and services
http://www.compassionandsupport.org/index.php/for_professionals/palliative_care
Models of Palliative Care in LTC1. Hospice Benefit
• Most widely used / studied
• Generally associated with positive resident outcomes
• Limited if uncertain prognosis
• Unavailable if accessing skilled benefit /rehab
• Frequently viewed as an “outside” agency
M Ersek CAPC Seminar Nov 2013
11/25/2014
4
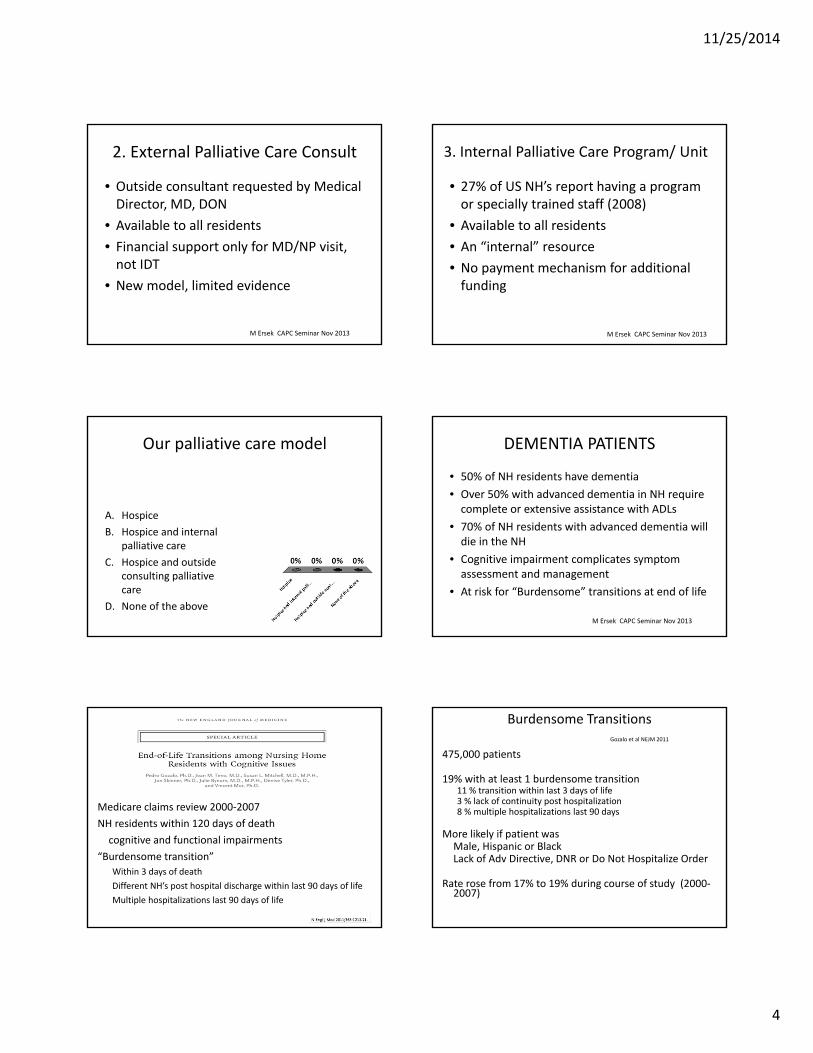
2. External Palliative Care Consult
• Outside consultant requested by Medical Director, MD, DON
• Available to all residents
• Financial support only for MD/NP visit, not IDT
• New model, limited evidence
M Ersek CAPC Seminar Nov 2013
3. Internal Palliative Care Program/ Unit
• 27% of US NH’s report having a program or specially trained staff (2008)
• Available to all residents
• An “internal” resource
• No payment mechanism for additional funding
M Ersek CAPC Seminar Nov 2013
Our palliative care model
A. Hospice
B. Hospice and internal palliative care
C. Hospice and outside consulting palliative care
D. None of the above
DEMENTIA PATIENTS
• 50% of NH residents have dementia
• Over 50% with advanced dementia in NH require complete or extensive assistance with ADLs
• 70% of NH residents with advanced dementia will die in the NH
• Cognitive impairment complicates symptom assessment and management
• At risk for “Burdensome” transitions at end of life
M Ersek CAPC Seminar Nov 2013
Medicare claims review 2000‐2007
NH residents within 120 days of death
cognitive and functional impairments
“Burdensome transition”
Within 3 days of death
Different NH’s post hospital discharge within last 90 days of life
Multiple hospitalizations last 90 days of life
Burdensome TransitionsGozalo et al NEJM 2011
475,000 patients
19% with at least 1 burdensome transition11 % transition within last 3 days of life3 % lack of continuity post hospitalization8 % multiple hospitalizations last 90 days
More likely if patient was Male, Hispanic or BlackLack of Adv Directive, DNR or Do Not Hospitalize Order
Rate rose from 17% to 19% during course of study (2000‐2007)

11/25/2014
5
Burdensome TransitionsGozalo et al NEJM 2011
Comparing regions with high rate of burdensome transitions to those with low rate, residents in high rate regions were more likely…
• to be admitted to ICU last 30 days of life
• to have feeding tube inserted
• to have stage IV decubitus ulcer
• to be referred to hospice in last 3 days of life
ICU Use During Terminal Hospitalization Medicare Patients 2010
40% of COPD pts in ICU w/in 1 month of death
22% of dementia patients in ICU
w/in 1 month of death
40% of patients referred to Hospice w/in 3 days of death had ICU stay that preceded
referralTeno JAMA 2013
20% of all deaths in the US occur in the ICUor shortly after an ICU stay
Angus CritCareMed 2004
Prospective cohort of NH residents with advanced dementia and their families (HCA) Feb 2003 – Aug 2007 22 Boston area NHs
Facility administrators identified residents > = 60 y.o. LOS > 30 daysStage 7 Global Deterioration Scale
unable to recognize family, minimal verbal, total functional dependence, incontinent, unable to ambulate independently
Funded by the National Institutes of Health, National Institute on Aging
Complications & MortalityMitchell, Teno NEJM Oct 2009
54% died w/in the 18 months of the studyMI, Stroke, PE uncommon sentinel event before death
40% hospitalized, ED transfer, IV Rxs, or TF
OccurrenceAdj 6 month mortality
All patients in study 24%
41% Pneumonia 47%
53% Febrile episode 45%
86% Eating Problem 37%
11/25/2014
6
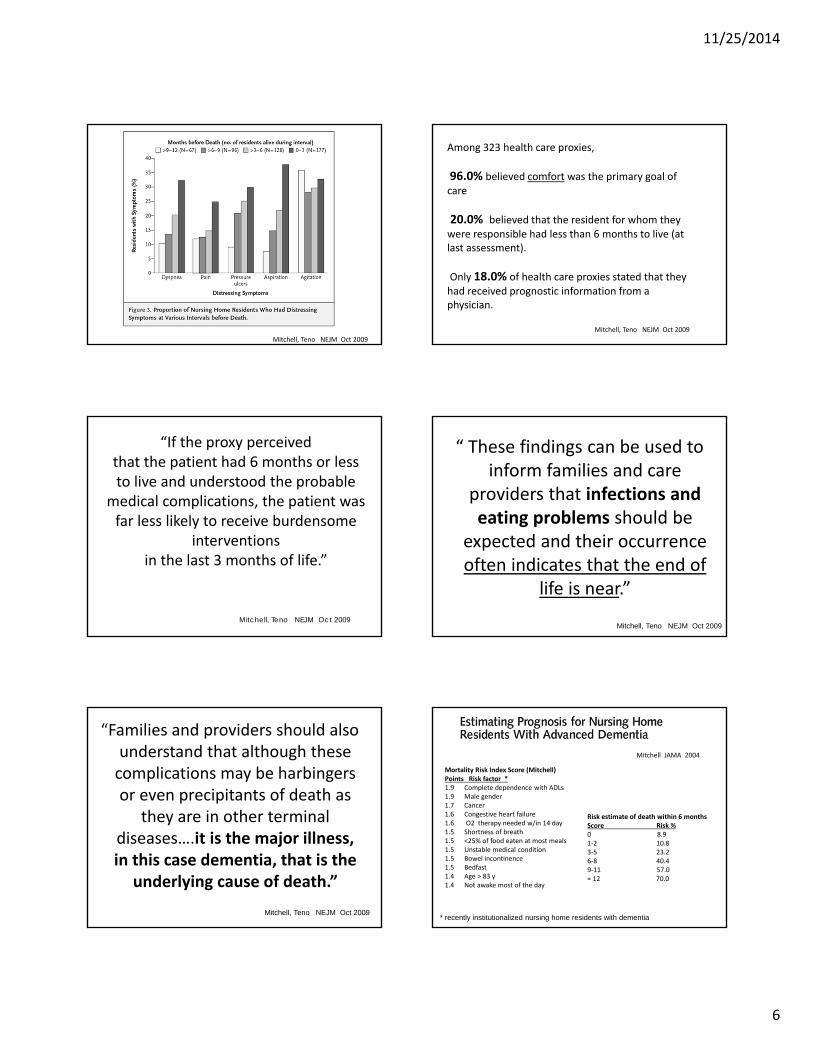
Mitchell, Teno NEJM Oct 2009
Among 323 health care proxies,
96.0% believed comfort was the primary goal of care
20.0% believed that the resident for whom they were responsible had less than 6 months to live (at last assessment).
Only 18.0% of health care proxies stated that they had received prognostic information from a physician.
Mitchell, Teno NEJM Oct 2009
“If the proxy perceivedthat the patient had 6 months or less to live and understood the probable
medical complications, the patient was far less likely to receive burdensome
interventions in the last 3 months of life.”
Mitchell, Teno NEJM Oct 2009
“ These findings can be used to inform families and care
providers that infections and eating problems should be
expected and their occurrence often indicates that the end of
life is near.”
Mitchell, Teno NEJM Oct 2009
“Families and providers should also understand that although these complications may be harbingers or even precipitants of death as
they are in other terminal diseases….it is the major illness, in this case dementia, that is the
underlying cause of death.”
Mitchell, Teno NEJM Oct 2009
Mortality Risk Index Score (Mitchell)Points Risk factor *1.9 Complete dependence with ADLs1.9 Male gender1.7 Cancer1.6 Congestive heart failure1.6 O2 therapy needed w/in 14 day1.5 Shortness of breath1.5 <25% of food eaten at most meals1.5 Unstable medical condition1.5 Bowel incontinence1.5 Bedfast1.4 Age > 83 y1.4 Not awake most of the day
Risk estimate of death within 6 monthsScore Risk %0 8.9 1‐2 10.8 3‐5 23.26‐8 40.49‐11 57.0= 12 70.0
Mitchell JAMA 2004
* recently institutionalized nursing home residents with dementia
11/25/2014
7
Advance Care
Planning
Advance care planning (ACP) An ongoing process of discussing and clarifying the current state of a person’s goals, values and preferences for future medical care.
Advance Directive (AD) General term referring to a written document for future medical care in the event that a person loses capacity to make health care decisions.
– Health care proxy, Living Will
Medical OrderOrders signed by a physician immediately applicable for a seriously ill individual. DNR/DNI, POLST paradigm MOLST, MOST, POST, COLST, SMOST, SPOST, TOPP
The Conversation Project
National Quality Forum Preferred Practices
• Designated surrogate/decision maker in every patient in primary, acute, long‐term care, palliative and hospice care.
• Document goals of care, treatments and settings of care at first assessment and update as conditions change.
• Convert goals into transferable medical orders (POLST)
• Make advance directives available across care
• Develop health care and community collaborations to promote advance care planning for all individuals
Institute of Medicine Dying in America 2014 “It’s too early until it’s too late”
40 % of all adult medical inpatients lack decision making capacity
44‐69 % of LTC residents lack capacity
The “vast majority” of critically ill patients lack decision making capacity
Most hospitalized patients at end of life will receive care from MDs who do not know them
Institute of Medicine Dying in America 2014
Medical Decision‐Making Capacity
Capacity is the ability to:take in information, understand its meaning and make an informed decision using the information
Capacity can vary with time & condition
Capacity is task‐specificchoosing a health care agent vs ability to make complex medical decisions
Adv Care Planning in Long Term Care
3 LTC facilities in Ontario, Canada 182 residents
Almost all had completed an AD within 3 months of death
Most changed to comfort based, but not until days before death
Staff concerned that intense treatments in days before death with not in the resident’s best interest.
Staff attributed the delay in transition to a comfort goal to family members
Staff were reluctant to transition to comfort measures until imminent death was certain.
Cable‐Williams Open Journal of Nursing 2014

11/25/2014
8
• Staff members understood Advance Care Planning as getting an AD signed
“Well, we have to have the directive—right from the first—because the staff has to know what they’re supposed to do, you know. You can’t be trying to figure whether they’re a transfer or a DNR when they are crashing in front of you. It has to be on the chart. Because who knows if
you’re going to be able to find anyone to ask if it isn’t there.”
Cable‐Williams Open Journal of Nursing 2014
• Discussions about changes in ADs often occurred when residents had been deemed palliative by their physicians within a day or two of death
• Staff members reported that family members usually do not want to talk about their family members’ decline or think about palliative care.
• However, one family member said, “I ask a lot of questions. If you don’t ask questions they will think you are not ready to hear it.”
Cable‐Williams Open Journal of Nursing 2014
“Its always too early until its too late”The Conversations Project
“…the staff have to recognize when the time is right. We wait until they’re true end‐of‐life, within hours, and if we’re lucky we get days.”
RNs in that facility were reluctant to discuss changes in ADs to comfort directed care. One nurse stated this was because “they feel that the minute they do that, everyone—you know, will stop caring for them.”
Cable‐Williams Open Journal of Nursing 2014
A Sense of Home
Staff believed that the AD should allow residents to die at the LTC facility, as this had become their home.
“It would be my worst nightmare to think they ended up dying all alone up at the hospital when we could have been with
them right here.”Cable‐Williams Open Journal of Nursing 2014
Not “Giving Up”
“I think [families] struggle with saying ‘no, we don’t want them to go to hospital.’
They have a sense that they are abandoning their mother or father, and
that they really should be doing everything they can, even though it’s
futile”
“You never want to be the one who gives up on somebody!”
Cable‐Williams Open Journal of Nursing 2014
Does this sound/feel familiar?
11/25/2014
9
Other BarriersNothing more can be done
End‐of‐life decisions should have clear answers. I must always have something to say
Residents and families generally do not want to discuss issues related to death and dying
I’ll take away hope if I raise end of life issues
If I get close to residents who die, I cannot be effective in my work.
Weiner and Cole, Palliative and Supportive Care, 2004
Principles of Good Communication
Start with the resident’s agenda
Stay with the resident and move the conversation forward one step at a time
Track both the emotion and the cognitive data you get from the resident
Articulate empathy explicitly
Slide of James Tulsky, MDCAPC 2014
NURSE Responding to Emotion
Name “Some people would be angry…”
Understand “It must be hard going through this alone”
Respect “I am so impressed by your commitment to your mother”
Support “I’ll be with you throughout all of this”
Explore “Tell me more…”Slide of James Tulsky, MDCAPC 2014
Key Points in End of Life Discussions
Is everybody on the same page regarding the resident’s condition & prognosis?
Focus on the resident’s GOALS, then address treatments
Weissman, Quill, & Arnold Fast Fact # 226 www.mcw.edu/eperc
Bring the resident’s “voice” into the room
Explore resident’s recollection of family member’s experiences with EOL treatments
Respond with empathy not just facts
Weissman, Quill, & Arnold Fast Fact # 226 www.mcw.edu/eperc
Key Points in End of Life Discussions
Don’t saddle the family with the guilt of decision – make a recommendation based on your best professional judgment
Emphasize what you ARE doing… you never stop care, you only stop treatments
Respect the resident’s & family’s need for time & support
Weissman, Quill, & Arnold Fast Fact # 226 www.mcw.edu/eperc
Key Points in End of Life Discussions

11/25/2014
10
Chronic disease or functional decline
Advancing chronic illness
Multiple co-morbidities, with increasing frailty
Death with dignity
Maintain & maximize health and
independence
Healthy and independent
Adapted from Pat Bomba, MD Compassion and Supportand Bud Hammes, PhD Gundersen Health System
1st Steps“Who”
Next StepsWhat Matters Most
Last StepsEOL
Interventions
Who would make medical decisions
for you?
What medical care you would want if you had a severe brain injury and were unlikely
to recover?
Why ???
Respecting ChoicesGundersen Lutheran Medical Foundation
1st STEPS
1st StepsHealth Care Proxy – “the Who ?”
The person(s) you appoint to decide about your medical care when you do not have the capacity to do so.
Only the patient can name a HC Agent
Different than a “Power of Attorney”
2 witnesses required for completionP Bomba compassionandsupport.org
Who would you choose?
At least 18 years old
Knows what is important to you
Able to separate his/her own wishesfrom your own
Thinks clearly in emotional situationsP Bomba compassionandsupport.org
NOT a Health Care AgentDurable Power of Attorney
Authorized for Disclosure of Protected Health Information (HIPAA)
Emergency Contact
Dialysis Centers 94 pts – only 3 had Surrogate Decsion‐maker.
After selecting SDM, 1/3 were not the Emergency Contact JPM 2013
Emergency Department 308 pts10% had AD (only ½ had given to their PCP)
95 % expected their emergency contact should be able to tell the medical team what their wishes were if they could not. Int PalCare Conf Montreal 2014
What happens if no Advance Directive & Patient is without capacity?
NYS Family HealthCare Decisions Act
1. Court‐appointed guardian2. Spouse (if not legally separated) or domestic
partner3. Son or daughter 18 or older4. Parent5. Adult sibling6. Close friend

11/25/2014
11
Living will – the “what” document
Outlines what care you would want in specific medical situations:
Permanently unconscious, Conscious but permanently confused,Terminal condition
Difficult to predict the future…
Your Advance Directive ?
1. Not on my “To Do” List
2. Thinking About It3. Completed4. Revised
Next Step – Declining Health
Documents are important, but even more so are
conversations about what matters
to prepare your family
What Matters Most ?
What are you hoping for?
What concerns you most about your condition or your treatments?
As your condition worsens, what trade‐offs are you willing to make?
Online “Starter Kit”
GET READY ‐ importance of advance care planning
GET SET ‐ ?’s for patient – values, goals Encourages subsequent conversation with family
GO – resources for advance directive completion
Care‐giver resources
http://theconversationproject.org/
11/25/2014
12
What makes life worth living?
As a patient I
A. Want to live as long as possible no matter what
B. Would accept some decrease in QOL
C. Would accept only a little decrease in QOL
D. QOL most important
As a patient I want
A. My doctors to make most of the decisions
B. My doctors to make some of the decisions
C. I want a say in every decision
How involved do you want YOUR loved ones to be?
1. Do exactly what I’ve said even if they’re a uncomfortable
2. Give them some leeway
3. Do mostly what brings them peace

11/25/2014
13
Last Steps – MOLSTMedical Orders for Life Sustaining Treatments
Generally for patients with serious health conditions – might die within the next year or nursing home resident
Choice to receive or refuse treatments – not “all or none”
A doctor’s order – active once signed by a doctor – home, assisted living, nursing home, hospital
Pat Bomba, MD
Does NOT include DNI
Does not cover additional Rx’s
Valid for 24 hours in hospital
POLST/MOLST
Communication
Documentation
System Responsiveness
Core Elements of MOLST
Actionable medical orders
Advanced, chronic progressive illness
Prognosis < 1 year, NH resident
Direction about resuscitation status
Limit or request all medical interventions
Susan Tolle, MD
8‐Step MOLST Protocol1. Prepare for discussion
• Understand the patient and family • Understand the patient’s condition and prognosis• Retrieve completed Advance Care Directives• Determine “Agent” (Spokesperson) or responsible party *
2. Determine what the patient and family know• re: condition, prognosis
3. Explore goals, hopes and expectations4. Suggest realistic goals 5. Respond empathetically6. Use MOLST to guide choices and have patient/family share
wishes• Shared medical decision‐making• Conflict resolution
7. Complete and sign MOLST8. Review and revise periodically
Developed for NYS MOLST, Bomba, 2005
11/25/2014
14
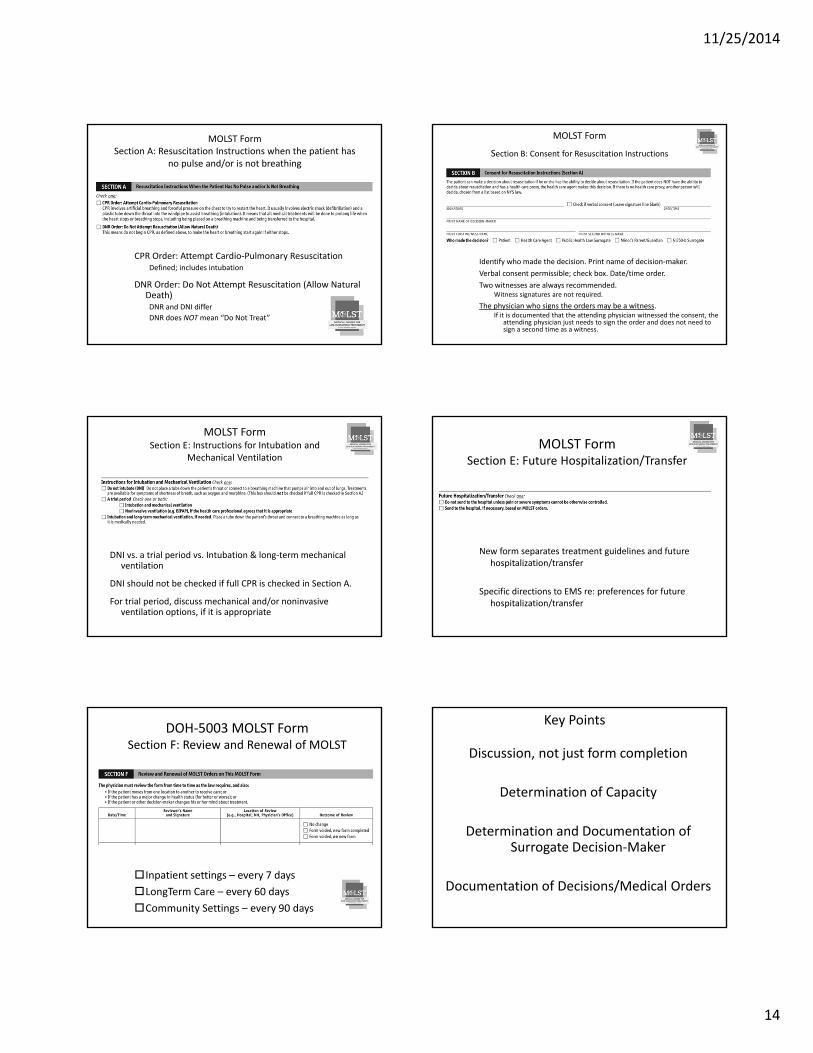
CPR Order: Attempt Cardio‐Pulmonary Resuscitation Defined; includes intubation
DNR Order: Do Not Attempt Resuscitation (Allow Natural Death)DNR and DNI differ
DNR does NOT mean “Do Not Treat”
MOLST FormSection A: Resuscitation Instructions when the patient has
no pulse and/or is not breathing
MOLST Form
Section B: Consent for Resuscitation Instructions
Identify who made the decision. Print name of decision‐maker.
Verbal consent permissible; check box. Date/time order.
Two witnesses are always recommended. Witness signatures are not required.
The physician who signs the orders may be a witness. If it is documented that the attending physician witnessed the consent, the
attending physician just needs to sign the order and does not need to sign a second time as a witness.
MOLST FormSection E: Instructions for Intubation and
Mechanical Ventilation
DNI vs. a trial period vs. Intubation & long‐term mechanical ventilation
DNI should not be checked if full CPR is checked in Section A.
For trial period, discuss mechanical and/or noninvasive ventilation options, if it is appropriate
MOLST FormSection E: Future Hospitalization/Transfer
New form separates treatment guidelines and future hospitalization/transfer
Specific directions to EMS re: preferences for future hospitalization/transfer
DOH‐5003 MOLST FormSection F: Review and Renewal of MOLST
Inpatient settings – every 7 days
LongTerm Care – every 60 days
Community Settings – every 90 days
Key Points
Discussion, not just form completion
Determination of Capacity
Determination and Documentation of Surrogate Decision‐Maker
Documentation of Decisions/Medical Orders
11/25/2014
15
Helpful Hits
Listen, do you want to know a secret?
You can’t always get what you want
Stop! In the name of love
Selected References
• Cable‐Williams, B.E., et al. Advance Directives in the Context of Uncertain Prognosis for Residents of Nursing Homes. Open Journal of Nursing, 2014, 4, 321‐329.
• Institute of Medicine. Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life. National Academies Press. 2014
• Gozalo, P;, et al. End‐of‐Life Transitions among Nursing Home Residents with Cognitive Issues. New England Journal of Medicine. 365;13. 2011
• Mitchell, S. et al. The Clinical Course of Advanced Dementia. New England Journal of Medicine. 361;16. 2009
• Mitchell, S. et al. Estimating Prognosis for Nursing Home Residents With Advanced Dementia. Journal of the American Medical Association. 291. 2004
Web Based Resources • Compassion an Support – Patient and professional resources for on advance care
planning, MOLST, pain management, feeding tubes, and others http://www.compassionandsupport.org/index.php/
• Deciding about Health Care ‐ A Guide for Patients and Families – NYS DOH guide on advance care planning and surrogate decision‐making standards. https://www.health.ny.gov/publications/1503/
• Center to Advance Palliative Care – Long Term Carehttp://www.capc.org/palliative‐care‐across‐the‐continuum/long‐term/
• American Geriatrics Society http://www.healthinaging.org/resources/resource:living‐with‐multiple‐health‐problems‐what‐older‐adults‐should‐know/
• The Conversation Project – advance care planning resourcehttp://theconversationproject.org/
• MOLST FAQs NYS DOHwww.health.ny.gov/professionals/patients/patient_rights/molst/frequently_asked_questions.html
• MOLST Checklists NYS DOH www.health.ny.gov/professionals/patients/patient_rights/molst/





























