Embed Size (px)
Citation preview


1 | P a g e
Consultant
Dr. Shagufta Zareen Pak One Health Alliance-VBD-2016-17
End Assessment Report
Mapping the use of Mobile Technology for Public Health Programs in
Punjab – Pakistan
Focusing Infectious Diseases
Nov-Dec 2016

2 | P a g e
TABLE OF CONTENTS ACKNOWLEDGEMENT ............................................................................................................................................ 4
EXECUTIVE SUMMARY ........................................................................................................................................... 5
LIST OF ACRONYMS ................................................................................................................................................ 8
List Of Graphs ............................................................................................................................ 8
List Of Figures ............................................................................................................................ 8
List Of Tables ............................................................................................................................. 8
Section-1 INRTODUCTION ...................................................................................................................................... 9
1.1 Background ..................................................................................................................................... 9
1.2 Study Rationale ............................................................................................................................. 10
1.3 Study Objectives ........................................................................................................................... 11
1.4 Methodology ................................................................................................................................ 11
1.5 Expected Outcome ........................................................................................................................ 12
SECTION-2 INTERNATIONAL BEST PRACTICES IN Mhealth ............................................................................ 13
2.1 Options For Use Of Mobile Technology For Public Health .......................................................... 13
2.2 International Mhealth Models Operating In LMICS. ................................................................... 15
2.3 Pre-Requisites Of Optimal Mhealth Projects ............................................................................... 18
SECTION-3 USE OF MOBILES IN PUBLIC HEALTH IN PUNJAB ......................................................................... 20
3.1 A Brief About Punjab Province ..................................................................................................... 20
3.1.1 Health Indicators In Punjab ............................................................................................. 21
3.2 Mhealth Status In Punjab, Pakistan ............................................................................................. 22
3.2.1 M-Health Apps For Field Monitoring And Evaluation ........................................................ 23
3.2.2 M-Health Project For Infectious Diseases ........................................................................... 27
3.2.3 Mhealth Project For Drug Quality Assurance ..................................................................... 28
3.2.4 Mhealth Project For Cancer Patients .................................................................................. 29
SECTIO.N-4 SURVEY FINDINGS AND DISCUSSION ............................................................................................... 30
4.1 Survey Design ................................................................................................................................ 30
4.2 Survey Coverage ........................................................................................................................... 30
4.3 Sample Size ................................................................................................................................... 30
4.4 Data Collection Tool ..................................................................................................................... 31
4.5 Data Analysis Methods ................................................................................................................. 31
4.6 General Observations ................................................................................................................... 31
4.7 Discussion ..................................................................................................................................... 35
4.8 M-Health SWOT Analysis .............................................................................................................. 38
SECTION-5 RECOMMENDATIONS & WAY FORWARD .................................................................................... 40
CONCLUSION ........................................................................................................................................................ 41

3 | P a g e
REFERENCES ......................................................................................................................................................... 42
ANNEXURES .......................................................................................................................................................... 44
Annexure-I: Projects / Program Surveyed For Data Collection ............................................................... 44
Annexure-Ii: Data Collection Tool (Questionnaire) .................................................................................. 45
Annexure-Iii Analytical Report Of Mhealth Projects, Punjab .................................................................. 48
Annexure-Iv: List Of Officials Interviewed ................................................................................................ 61

4 | P a g e
ACKNOWLEDGEMENT Due to time and resource constraints, the preparation of this report would not have been possible without the cooperation of senior managers who spared enough time out of their busy schedule to provide the required information. Though most of the projects were in the nascent stage but the technical and administrative heads of almost all the projects cooperated with the author in a best possible way. I highly appreciate the support provided by Dr. Munir Ahmad, Additional Director, EPI Program Punjab, Mr. Shehzad Anwar, Program Manager Dengue, PITB, Mr. Arsalan Manzoor, Program Manager DSS, Dr.Farrukh Sultan, Additional Director Dengue Control Cell, Dr. Bashir Bashir, Additional Director Malaria Control Program, Dr. Mehmood Salahuddin, IRMNCH, Mr. Imran Durrani IRMNCH, Mr. Manzar Abbas, Incharge Software Cell SKM &RH, Dr.Saba Senior Manager Organization Management Heartfile, Dr. Amir MS Mian Munshi Hospital, Dr. Shehnaz MS DHQ Sheikhupura, Dr. Afzal Acting MS DHQ Nankana and Dr. Zaka ur Rehman Chief Drug Officer Punjab. I am grateful to Mr. Gul Shehzad, Data Analyst, POHA, who helped me a lot in analyzing the data collected during this study. Special thanks go to Dr. S. M. Mursalin, CEO POHA, who provided all technical guidance and support to me in the preparation of this report. I must say formal thanks to Pak One Health Alliance that provided me a chance to work on this interesting subject and enabled me to conduct this first ever study on mHealth situation in Punjab.
Dr. Shagufta Zareen
POHA Consultant, Punjab 9th Jan, 2017

5 | P a g e
EXECUTIVE SUMMARY In the last two decades, healthcare system has been under drastic revolution to widen the scope of health surveillance and provision of healthcare services to the public. Social welfare states have been at the forefront in this health initiative. The ubiquitous availability of Information and Telecommunication technology everywhere in the world has introduced a trend of using the same for easy access to health care services. Use of ICTs in the health sector has resulted in coining new terms like eHealth and mHealth. Apple was a company that ruled the mobile phone market by launching smart phones with a large number of apps for its users. These apps, available in apple store, can be downloaded free and range from health and fitness to the professional apps for healthcare workers to facilitate them in the performance of their jobs. Now almost all governments, in developed and developing countries, are following this trend rigorously by officially launching health apps on smart phones used by healthcare workers only. This. new trend of using wireless technology including mobile phones, patient monitoring devices, personal digital assistants (PDAs) etc. in the health sector is commonly referred as mHealth or mobile health. mHealth is being used to investigate outbreak of track the trends of infectious diseases for creating disease early warning system, maintenance of medical records, health education for patients, upgradation of professional medical skills and facilitation of healthcare delivery. The smart phones based simple and easy to use tools have been used to improve disease prevention, surveillance, clinical care and performance management. This is widely used practice all over the world. mHealth has particularly made is easier for the health managers to provide healthcare services in the remote areas of the country where healthcare infrastructure is either not available or weak and dilapidated it is. The mHealth platform is particularly useful in collection, transmission and timely analysis of digital data. Since no manual procedures like maintenance of data on registers or diaries and transmission through post or courier are involved. Therefore, data travels faster and reach point of analysis from point of collection within no time. It helps us in making evidence based health policy and implementation. Furthermore, monitoring and evaluation of health workers according to the job description assigned to them is also easier through mHealth projects. Therefore, such apps are widely used in both rich and poor settings of the world. It has also proved to be an excellent method to measure the performance of health workers, which is otherwise very difficult in medical field, to evaluate the quality of work done by health practitioners. Pakistan is not left behind in following this new approach in the health sector. The worst outbreak of Dengue Haemorrhagic Fever (DHF) in 2011 that led to more than 300 deaths in few. months and affected more than 20000 patients in Punjab proved to be a turning point in the health sector by introducing the use of mHealth to control dengue fever outbreak in future in all cities of Punjab.

6 | P a g e
Initially smart phone app was created for tracking dengue fever only and it was used by all stakeholder departments including health, environment, water and sanitation, agriculture etc. Due to the success of dengue tracking system by controlling dengue outbreak in Punjab in following years, android phones were used for other infectious diseases, hospital based apps, monitoring and evaluation and drug quality monitoring in Punjab. Due to strong political support and administrative leadership, Punjab spearheaded the trend of launching android apps for health sector in Pakistan. This baseline exercise was carried out to assess the current status of mHealth projects and identify the measures for optimal mHealth in Punjab by comparing it with International Best Practices. Quantitative cum Qualitative approach was used by using a structured questionnaire to get baseline information which was further corroborated by conducting semi-structure interviews of the heads of the respective mHealth projects and Health policy makers. Since there is no focal person or organization in Punjab that is particularly working on mHealth. Therefore, snowball approach was used to get sample of 9 mHealth projects including 7 from public sector and 2 from private sector in Punjab. The data obtained in the filled questionnaires indicate that smart phone user’s qualification varies from under- graduation to post-graduation in different projects. 90% of the surveyed projects were fully launched and only project that was in the pilot phase was from Private sector and created by Shaukat Khanum Hospital. More than 50% users were trained from less than 1 week and only 10% were trained for 4 weeks for using mHealth apps. Majority of the respondents (30%) were using smart phone app known as Hospital watch while other mHealth projects were represented by only one member each project in the data. Most of the surveyed mHealth projects (77%) are owned and supported by Govt. of Punjab. Therefore, mHealth projects were technically designed by Punjab Information Technology Board and implemented by respective projects. This led to a sense of alienation between designers and implementers and lack of ownership of the projects was observed. It was also noticed that some mHealth projects like Hospital Watch was termed as un-necessary workload thrust upon the project administrator, rather than contributing to the efficiency of the healthcare system. Such gulf needs to be bridged and misunderstandings are required to be urgently removed for better performance of the system. On the whole, mHealth projects were considered to be integral part of the healthcare system that should be properly embedded in the routine health information system. Many respondents recommended to widen the scale of operation of these projects from some divisions to the provincial level by making it more user-friendly. Now the digital platform is ranked as integral part, not adds on to the healthcare system. Since mHealth is only one time cost at the time of lunching it with later nominal maintenance cost. Thus it is getting more popular in provision of quality healthcare services at far off areas than in-person services to the suffering population.

7 | P a g e
Therefore, it is highly recommended to enhance the number and use of mHealth projects for all categories of health services. However, the users, health customers, community representatives, program administrators should be taken in the loop while designing Smart phone health apps. There is also a need to establish standard protocols, rules and procedures for creation and governance of such projects.
8 | P a g e
LIST OF ACRONYMS
BHU Basic Health Unit
BISP Benazir Income Support Program
CDC Community Development Corporation
CRVS Civil Registration and Vital Statistics
DHIS District Health Information System
DHQ District Head Quarter
DOH Department of Health
EDO Executive District Officer
EWEC Early Women Early Child
GDP Gross Domestic Product
I.C.T Information and Communication Technology
LHW Lady Health Worker
LHS Lady Health Supervisor
MNO Mobile Network Operator
MICS Multiple Indicator Cluster Survey
MIS Management Information System
MNCH Maternal and Child Health Care Program
MPA Member of Provincial Assembly
MS Medical Superintendent
NGO Non-Governmental Organizations
NHIS National Health Information System
PHC Primary Health Care
PITB Punjab Information Technology Board
PSPU .PITB
Policy and Strategic Planning Unit Punjab Information Technology Board
RHC Rural Health Centre
RHIS Routine Health Information System
RDT Rapid Diagnostic Test
SMU Special Monitoring Unit
SDGs Sustainable Development Goals
THQ Tehsil Head Quarter
UHC Universal Health Coverage
WHO World Health Organization
LIST OF GRAPHS Graph 1: Mobile phone apps used by the projects Graph 2: Current status of mHealth Apps Graph 3: Technical stakeholder of mHealth Apps Graph 4:Training period of Smart phone users Graph 5: Academic qualification of the mHealth app users
LIST OF FIGURES Figure 1: Mobile phone subscription per 100 inhabitants Figure 2: The Map of Punjab
LIST OF TABLES Table 1:Types of information collected by various project using android phones

9 | P a g e
SECTION-1 INRTODUCTION 1.1 Background
The advances in the information and communication technology over the past few decades has revolutionized all fields of our lives. The utilization of modern gadgets like mobiles and laptops have also transformed the traditional healthcare system of developed countries at a faster pace and developing countries at a slower speed. The use of different forms of information and communication technology devices in healthcare system is called eHealth or telehealth. Mobile Health or mHealth is defined as the “use of mobile devices such as mobile phones, patient monitoring devices, personal digital assistants (PDAs) and other wireless devices for medical and public health practices”. The accelerated penetration of electronic devices into the market has fuelled interest in mHealth. In general terms, mHealth is the application of mobile computing, medical sensors and communication technologies for healthcare. mHealth capitalizes on the success of mobile and other wireless technology to deliver and monitor the health services. The rapid ICT diffusion into the health system is particularly helpful in provision of services to remote areas where health facilities and infrastructure is patchy. The use of mobiles and wireless technology has increased rapidly not only in the developed countries but also in the poorer settings of the world. The international subscription of mobile devises has increased from 2.2 billion to 7 billion from 2005 to 2015. The increase of mobile technology has concomitantly increased the use of improvement of healthcare delivery, health services and health outcome. The figure no 1 shows the accelerated use of mobiles in South-East Asia.
Figure 3: Mobile phone subscription per 100 inhabitants

10 | P a g e
Pakistan being a 6th most populous nation with 190m population is ranked as a developing country where 65% people are living in rural areas. Due to insufficient health infrastructure and workforce, the healthcare needs of the people in distant areas are not properly addressed. The expansion of Information and Communication Technology (ICT) in health care has provided an unprecedented opportunity to Pakistan to provide health care services to the people in remote areas. Wide range of functions including storage, transmission and retrieval of digital data are being performed through the use of intelligent handsets called Smart phones. Remote diagnostic monitoring, information dissemination, public education and alerts system are being managed by using Smart Phones. Since Communicable diseases are taking a heavy toll on the health budget of Pakistan. Therefore, mHealth has the potential to help Pakistan to combat communicable diseases. Due to the potential of mobile Health to offer cost effective solution to many health related problems, Pakistan has taken several initiatives in this regard. There are many diseases that are being monitored with the help of Smart phones provided to health care professionals and supporting staff. After a worst episode of dengue outbreak in Punjab in 2011, Punjab took a lead in this regard by turning towards mHealth and developing android based application for dengue fever only. This experiment proved successful in controlling future dengue outbreaks in Punjab. Later, Punjab spearheaded in developing a long list of applications for other communicable disease surveillance programs. The vaccination programs, infant and maternal mortality has also been reduced by sharing health information to community health workers through Smart Phones.
1.2 Study Rationale Pakistan is in the nascent phase of using wireless technology for provision of quality healthcare services in different areas of Pakistan. Currently, various health programs and projects are using Android based applications to ensure their targets. However, all these projects are either scattered or that data is not being used for evidence base decision making of that particular disease. The purpose of this baseline study is to conduct baseline survey of ..majority of health projects in public and private sector that are using Smart phones to monitor the health care services. Moreover, the findings of this survey will be shared with a group of health professionals and IT professionals, in provincial consultative meeting, to get suggestions in the improvement of current applications. Since vector borne diseases take a heavy death toll in Pakistan, therefore, the recommendations in the final report will be helpful in designing an application that is useful for launching mobile application for integrated disease surveillance program like Vector Borne Diseases.

11 | P a g e
1.3 Study Objectives The study objectives are:
To conduct baseline survey of currently implemented mHealth projects in Public sector in Punjab and the barriers in the smooth working of those projects
To identify the measures for improvement in existing mHealth projects for enhancing the rate of data collection and reporting.
To recommend sustainable mHealth initiatives for priority diseases
To suggest measures to enhance epidemiological capacity at provincial level
To promote risk awareness for vector borne diseases among health professionals and policy makers
1.4 Methodology The multipronged strategy involving both qualitative and quantitative methods was used to meet the intended study objectives. This included following steps.
Literature review and inference from international best practices for mobile Health projects to evaluate mHealth initiatives in Punjab.
Preliminary Meetings with health professionals, focal persons from health Departments, Directorate General of Health and other relevant stakeholders to generate understanding about the work, modalities, contents of questionnaire and expected outcomes.
Development of a standard structured questionnaires for the assessment survey for use at strategic and operational levels (Questionnaire is attached).
Un-structured Interviews of mobile health system managers, ICT Experts, Provincial/District staff, stakeholders engaged and other relevant key personnel were conducted.
Selected health facilities were visited to document existing situation for commodity data collection, consolidation, analysis and feedback.
Provincial consultative meeting with key professionals/Stakeholders was held to understand current status, policies, practices, issues and future prospects in Punjab
Development of work document after taking into account the suggestions by the relevant professionals and recommendations for mHealth approach to combat prioritized vector borne diseases.
12 | P a g e
1.5 Expected Outcome The projects that are using android based application are scattered in different parts of Pakistan. There is no centralized office that is monitoring these projects. Therefore, the data collected in these projects is fragmented and does not yield tangible results that are helpful in solid mHealth decision making. It leads to health decision making based on political demands rather than on evidences. The current assessment study of mobile health projects is an attempt to compile data of ongoing mHealth activities in the country and compare them international best mHealth practices. The purpose of this exercise is to develop a system where at least some mobile health applications and practices can be incorporated into our national system to combat vector borne diseases.

13 | P a g e
SECTION-2 INTERNATIONAL BEST PRACTICES IN MHEALTH The impetus for using wireless technology came from the increasing use of cellular phones in both poor and rich settings of the world. With increase in the number of mobile phones, the active mobile broadband subscription has also rapidly increased to cover 86% inhabitants of developed countries and 39% in the developing countries. This rapid global inclination towards mobile technology has provided an opportunity to achieve the goal of “Universal Health Coverage” (UHC) by replacing traditional health services with mHealth. UHC is a part of the “post-2015” agenda which is geared to meet the Sustainable Development Goals (SDGs) adopted by the United National General Assembly in September 2015. The Goal No. 3 of SDGs is to “Achieve Universal Health Coverage” to provide high quality health services to all people with no financial hurdles. The most comprehensive approach to achieve this goal in a coherent manner is to provide people centred and people monitored services through the use of ICTs in health sector. There is a trend not only in the developing but also in developed countries to discontinue using fixed telephone lines and moving towards mobile technology. Since providing health services to remote and underserved communities with mobile phone is far easier than in-person services. Therefore, the use of mHealth is much in vogue in developing as well as developed world. mHealth applications have been applied in a wide range of settings including facilitation of care delivery, medical records charting, patient and health worker education, disease prevention and patient self-management. These simple tools can improve disease surveillance, clinical care, prevention, and standardized management.
It has been observed that maximum utilization of mHealth is in the high-income countries as compared to low-income countries. One reason of that may be the capacity issue of low-income countries to develop and maintain the technology to implement mHealth programs without financial support from donor or mobile network operators (MNOs).
2.1 Options for Use of Mobile Technology for Public Health World Health Organization has categorized following different types of mHealth programs that are commonly being practiced in the world to provide health services or collecting health information or are meant to collect public health information. The region of America is reported to have maximum countries with at least one mHealth program in each categories and South East Asia region has the least percentage of it.
2.1.1 Accessing or providing health services In this category, either the individuals can directly get access to health services through their wireless technology or individuals are approached by health service providers by sending messages in the form of text, voice or multimedia for provision of some health services.
14 | P a g e
1) Health Call Centres/Health care telephone helplines. The individuals seek health care advice or pre-recorded health related messages from a trained worker calling a telephonic helpline through their mobile phone or fixed lines. This is the oldest and most common global use of mobile technology for health services.
2) Emergency toll-free telephone services
Free telephone hotlines manned by trained worker and linked to response system are also available to tackle health emergencies. This is the oldest and most common global use of mobile technology for health services.
3) Treatment adherence Health facilities/services send reminder messages to patients to ensure timely usage of medication
by them. This is common for reminding to take antiretroviral drugs for HIV in low and middle income countries.
4) Appointment reminders
Health services/facilities send reminder messages to patients to make or attend a medical appointment. This app has significantly reduced non-attended appointments. This is the 2nd common use of mHealth apps in the world.
5) Mobile telehealth Healthcare professionals communicate with each other or with patients by using wireless technology.
6) Emergency management systems
This system is designed to manage disasters and other emergency conditions using mHealth applications. This is the communication between health workers to give inter-sectoral response in some emergency conditions
2.1.2 Accessing or providing health information
Health monitoring or surveillance is done in this category to provide health information to the consumers or health workers.
1) Community mobilization campaigns
Health promotion campaigns are organized by mobilizing the communities by health services providers by using ICTs. The purpose is to raise awareness among target groups for certain health related issues. This is the 2nd common use of mHealth apps in the world.
2) Access to medical information
Healthcare professionals get access to health sciences literature, database, resources and tools on their mobiles.
3) Clinical decision support systems Health practitioners get patient and their disease related information on their smart phones for review and clinical decision making. The android phones are used to add to the knowledge of health care professionals on different subjects
4) Electronic patient information
Electronic data of patients and their lab reports enable the health practitioners to review the patients clinical status and make decisions accordingly.
5) mLearning
It is access to online educational resources

15 | P a g e
2.1.3 Collecting Health Information
Smart phones apps are used to collect patient and disease related data from vast and dispersed areas in no time.
1) Health surveys
Health survey are conducted using ICTs to collect and manage real time data. 2) Surveillance
Public health surveillance is managed using mHealth approach for routine, emergency and targeted data collection and management.
3) Patient monitoring
Receiving patient data for monitoring and evaluation by using mobile apps. It has been observed that this app is used more commonly in the European region which may be due to policy focus on research across Europe by the European Commission.
The role of mHealth has been re-cognized internationally as well as in the UN Commodity Commission Report. In that report, the use of ICTs best practices was recommended to ensure supply chain management of essential commodities to save lives of women and children in remote and under-developed countries of the world.
2.2 International mHealth Models Operating in LMICS. Based on the commodity commission recommendations, following five models have been identified to elaborate best international mHealth practices along with financial sustainability.
2.2.1 For Demand Generation and Awareness
Village Reach Program Under this category, Village Reach Program is a best case study. This is a program launched in Malawi which offers free Maternal, New-born and Child Health (MNCH) hotline known in the local language as “Chipatala Cha Pa Foni (CCPF). By calling on this hotline, the user seeks direct information, advisory service about health promotion of maternal and child health which otherwise may be beyond the reach of the health system. Hotline callers also have an option to be enrolled in a SMS-based tips and reminder service to receive. special health messages about maternal or child health. Though currently this program relies on a support of donor and MNO for call and text services. However, due to the high success rate of the program with 500 calls/month and high client satisfaction rate (77%), Village Reach plans to extend its service area from free hotline to emergency transportation of the patients by attracting telecommunication companies, transporters and enterprises. The payment for these services will be made either by the callers themselves or by the community groups and Ministry of Health to sustain the health outcomes. Though government provides trained health workforce but Village Reach is not relying on the government as a sole financer for the program to ensure its sustainability in future. A multi-layer implementation plan and monitoring and Evaluation system is also there in the program.

16 | P a g e
2.2.2 Performance and Accountability Switchboard: Switchboard is a free calling network for Health workers in Ghana and Liberia are enrolled. Initial financing for this model was provided by donors but now it is becoming a commercial entity with the involvement of Private sector. It is a simple model with few players where health professionals including doctors, nurses and community health workers join the closed health worker networks to get free calls and texts to other health workers. The service fee is paid by them by calling people outside the network. The funding for Switchboard comes from MNO that is benefitted by the additional revenue gains and a network that may have further future services. For instance, in Ghana and Liberia, health workers made 4 million calls to their colleagues. Simultaneously, the health workers paid $1.5 million for calling their family and friends who were not in the network. Switch board is now expanding to Tanzania by creating largest network of health workers with 9000 health practitioners.
2.2.3 Quality Monitoring
Sproxil. Sproxil is a social enterprise that provides SMS based drugs verification to monitor the quality of drugs in India, Nigeria, East Africa and Ghana. Sproxil enables the users to verify the drugs authenticity, if original or counterfeit, by texting the one time use code on drugs packages. In this model, not only the end user get a direct access to the original and quality drugs but Pharmaceutical manufacturers are also benefitted by mitigating their loss of revenue due to counterfeit drugs. Sproxil has multiple pharmaceutical clients to make its services cheaper to the end users. Thus it is financially sustained by the revenues generated due to its drug authentication services. Sproxil also get ethical supports from the respective governments that want to reduce the hazards posed by counterfeit drugs to the consumers. Sproxil plans to expand its services by using market intelligence and advisory consulting. The organization also intend to move from anti-counterfeiting to monetizing the data obtained from the service users.
2.2.4 Supply Chain Awareness:
SMS for life This is an S.MS services for stock level tracking of essential medicines like Anti-malarial drugs as well as Malaria rapid diagnostic tests (RTD) to align with National diagnostic policy. (Plus one) This model provides SMS between health facilities that uses anti-malarial medicines and district managers who made those medicines available in the districts to reduce shortfalls or stock outs. This system started with efficient partnership of Information Technology and process knowledge provided by Novartis, Communication expert from Vodafone, a mapping person from Google and a project manager from IBM. However, it was soon realized that Governments are the key stakeholders in this chain. The government is the only player that can ensure funding and staff to support the project by receiving stock information to avoid stock outs in emergencies. Without the support of the government, the whole system will collapse and cannot proceed further.
17 | P a g e
SMS for life has performed remarkably in Tanzania where stock-outs were reduced from 79% to less than 26%; at the beginning of the pilot. In Ghana, after successfully piloting it in 6 districts, the program is about to expand to whole country by coordinating with the Ghana Health Service. The same is a case with Kenya where its successfully piloting is now being extend to whole country with the Division of Malaria Control in Cameroon, not only the program is being introduced at national scale but patient surveillance data on the use of RDTs is also being collected. Magpi (former EpiSurveyor) This is a mobile phone application by the DELIVER PROJECT of USAID for control of Malaria. This application had been launched in seven countries (Ghana, Malawi, Mozambique, Nigeria, Tanzania, Zambia, and Zimbabwe) since 2009. Vigilant monitoring, evaluation and timely responding to the emergencies of Malaria was a challenge hindering the successful implementation of Malaria Programs in all these countries. Therefore, a mobile phase activity “End use Verification” was designed. This software focused on two aspects: I) Ensure availability of enough stocks of artemisinin-based combination therapy (ACT),
recommended by World Health Organization (WHO) for treatment of Malaria, at the health facility level.
II) Case Management of Malaria on an established protocol.
Since ACTs are needed within 24 hours of the onset of symptoms of Malaria, otherwise, disease progress to severe malaria which can be fatal. Therefore, the purpose of “End-use activity” was a rigorous monitoring and supervision to ensure malaria supply chain, availability of sufficient stocks of ACTs to control malaria wherever it arises. It also ensures snapshots of how malaria is treated after being diagnosed by training respective manpower of health professionals. The information provided by End-use activity is quickly analysed by a software “Episurveyor” installed in the mobile phones. It’s a simple software that allows the user to create surveys through an online interface, to send the data collected at health facilities to a remote server where it can be accessed online. Thus it reduced the time in .data collection and analysis of indicators. It also enabled the decision makers to control malaria by timely tackling the barriers in the supply chain and case management in the region.
ILS Gateway This is a mobile health application to ensure steady supply of essential medicines in Tanzania. It tracks the stocks of 20 essential medicines, along with family planning and malaria products at health facility level. The health workers use their personal mobile phones to text the stocks of required medicines/information to a toll free short code. The dash board displays the latest information received through text messages to enable the logistics decision making.
The ILS Gateway is a mobile alert and reporting system designed to support and strengthen the Integrated Logistics System (ILS) by: a) Expanding and ensuring the accessibility of logistics data
b) Utilizing the use of logistics data for supply chain decision making

18 | P a g e
This mobile phone-based reporting system reinforces and strengthens the existing paper-based logistics system that is used to report on essential health products. ILS Gateway is constantly being evaluated and improved with routine Monitoring and Evaluation.
.2.2.5 Financial barriers in the Treatment Bearing financial cost of the treatment is a huge obstacle in accessing quality healthcare services. Changamka: In order to provide affordable health care to poor patients, Changamka program is launched. This is a program with partnership of MNO, Safaricom that has a largest database of subscribers and mobile money. Three basic components of the program are savings, voucher and mirco-insurance programs. a) Savings program is for in-patients and out-patients services for maternal health b) Voucher program assists poor women to use government subsidies for health care.
When users are unable to pay for their health care, donors come to their rescue. For this purpose, Community health workers identify eligible women and assign them a telephonic registration women. Women can use that number on phones to redeem vouchers at health facilities. Thus paper vouchers are replaced by mobile vouchers.
c) Micro-insurance
The funding for Changamka comes from government subsidies for poor women and revenues generated from end-users. Initially the savings program was for out-patients only. However, Changamka found that health care is not predictable and in-patients should also be included in these services. Changamka has diversified the role of insurance companies from managing funds and pay providers to manage savings as well. When health savings reach a threshold, they are converted to premiums to become income of an insurance company. The health facilities are also benefitted by dealing with increased patient load with less administrative costs and faster payments for their services.
2.3 Pre-Requisites of Optimal mHealth Projects In the desk review of literature, following key areas have been identified for successful incorporation of any form of ICTs into the national health system to yield universal coverage of preventive, primary and clinical care to all.
2.3.1 Institutional and Stakeholder Leadership Strong commitment by Political and Bureaucratic leadership is a pre-requisite to allow integration of Information Technology into the health system. This determination will ensure that health sector policymakers and implementers will comprehend and utilize electronic health information system. It will also promote a professional culture to embrace the innovative solution for emerging and existing health issues. Strong leadership will ensure cross-sector coordination for better coordination of health care.
19 | P a g e
2.3.2 Regulatory and Legal Framework There is a need for regulatory and legal framework to standardize the collection, integration and analysis of data and utilization of that in the evidence based decision making at various level. Since it is very difficult to qualitatively measure the performance of health professionals, therefore, the electronic health system will also be used to ensure accountability, transparency, neutrality and work friendly.
2.3.3 Civil Registration and Vital Statistics (CRVS)
CRVS should also be focused as a key area to be focused to get long term effects on not only health systems but also on policy making for social security, education and other sectors of civil service. Allotting unique IDs to the citizens in CRVS will be helpful in tracking each citizen’s health record irrespective of their migration within or out of city. Integration of data of CRVS with health information systems should be a central component in devising strategies for women’s, children’s and Adolescents’ health for achievement of post 2015 Sustainable Development Goals.
2.3.4 Routine Health Information System (RHIS) RHIS should also be strengthened while introducing innovation in the existing health system. Harmonizing and standardizing multiple initiatives and assimilation of them into the existing ones is a basic component to achieve desired outcomes in health sector.
2.3.5 Quality and Coverage
In order to enhance the quality and coverage of healthcare, the environment should be created where both healthcare users (Patients) and healthcare providers (Health workers) are satisfied with the quality of health services. Use of wireless technology enable both to get access to each other and share the information of mutual interest. In order to ensure the quality of health coverage, health infrastructure should be improved and capacity building of health workers should be done. The use of ICTs in health sector will also resolve the long standing issue of equity and quality and enhance the level of monitoring and evaluation of various health initiatives. Thus government will be able to ensure high-quality and affordable health care by reducing the time, cost and number of visits required for a patient to reach a healthcare providers.
2.3.6 Stakeholders’ engagement
Meaningful engagement of all stakeholders including health professionals, workers, medical and para-medical staff, communities, citizens, ICT department, policy makers and implementers is required to achieve the objectives of universal health for all. For instance, active engagement by citizens is required to update their electronic health records etc. The use of electronic health information will also empower the citizens to use health services efficiently.

20 | P a g e
SECTION-3 USE OF MOBILES IN PUBLIC HEALTH IN PUNJAB 3.1 A Brief about Punjab Province
The name of Punjab is derived from Persian words “Punj” means five and “Ab” means water. It is due to the five tributaries of Indus River named as Ravi, Sutlej, Jhelum, Chenab and Beas flowing through the plains of Punjab. Therefore, it is called a land of five rivers. However, it also contains deserts like Thar and Cholistan.
Figure 4: The map of Punjab Geographically, Punjab is located at the north-western end of Indian plate. It is bordered by Sindh to the south, Baluchistan to the southwest, India (Punjab and Rajasthan) to the east, Khyber Pakhtunkhwa to the west, AJK (Azad Jammu and Kashmir) to the north east and Islamabad to the north. It is the only province that borders all other provinces of Pakistan. Punjab has been a hub of 4000 years old Indus Valley Civilization. Due to its peculiar geography, it has historically served as a gateway to the subcontinent for invaders.

21 | P a g e
Punjab has a tropical wet and dry climate. It experiences hot summer (Apr to June), mild winter (Oct to Mar) and rainy season (July to Sep).
The area of. Punjab is 79,284 sq. miles which makes it area wise the 2nd largest province of Pakistan after Baluchistan. With estimated population of 101 M, Punjab is the most populous province of Pakistan with relatively high human development index at 0.670 as compared to other provinces of Pakistan. Literacy rate in Punjab is 61% and huge network of Public and Private universities exist there. In addition to the Services and manufacturing sector, Agriculture sector dominates in the economy of Punjab due to the presence of the worlds’ largest canal irrigation system. Punjab is also perceived to be the most industrialized province of Pakistan. Industrial sector is contributing up to 24% of provincial Gross Domestic Product Its one of the most urbanized region of South Asia with almost 40% people living in urban areas. Despite all its development, Unemployment still exists there. Unemployment rate in Punjab is 7% in the adults of age group 15-24years. The unemployment is more in urban areas (8%) than in rural areas (6%).
There are 74 medical and dental colleges in Punjab of which only 23 belong to Public sector and rest are being managed by private sector. Medical and dental colleges along with their affiliated teaching hospitals are being managed by specialized healthcare and medical education department. There are large number of primary and secondary health care centres including 2520 Basic health units, 316 Rural health centres, 123 Tehsil Headquarters and 26 District head quarter hospitals which are being managed by Primary and Secondary Healthcare department in Punjab. Both department of health are administratively headed by their respective secretaries. It has been noticed that 57% of the population in Punjab has reported to have nearest health facility belonging to Public sector but still privately run health institutions are catering to a vast majority of population in Punjab. Though most of the private hospitals are located in urban or semi-urban areas and are being run on commercial basis by charging exorbitant fees irrespective of the social status of the patients but they are enjoying good reputation for the quality of the services they are providing.
3.1.1 Health Indicators in Punjab According to Multiple Indicator Cluster Survey (MICS) conducted in Punjab in collaboration with UNICEF conducted in 2014, Under 5 mortality rate in Punjab is estimated to be 93 deaths per 1000 live births which is higher in rural areas with 105 deaths as compared to 69 deaths in urban areas. There is a considerable difference in child mortality due to mother's educational and economic status. Under-5 mortality for children whose mothers are illiterate or have only pre-school is high (124 deaths per thousand live births) and the rates decline as the mother’s educational level increases. Similarly, infant mortality rate is quite high with illiterate mothers as compared to children whose mothers have higher secondary education (96 versus 46 deaths per 1000 live births). Infant mortality rate (for children under 1year of age) is 75 deaths per 1000 live births. Among under 5 years’ children, 34% are moderately or severely

22 | P a g e
underweight, 33 percent are moderately or severely stunted (i.e. too short for their age) and 18 percent are moderately or severely wasted (i.e. too thin for their height).
In the age group 15-49 years, total Fertility Rate (TFR) is estimated at 3.5 children per woman which is slightly higher in rural areas 3.7 compared to urban 3.0. Among women with a live birth in the last two years, 79 percent receive antenatal care at least once during their pregnancy from a skilled personal which can be a medical doctor, nurse, midwife or Lady Health Visitor (LHV). Around 61% birth deliveries are conducted in a health facility with 43% in private and 18% in public health facility. By the age of 2 years, 56% children are fully immunized as per official schedule of Expanded Program of Immunization (EPI). According to the data of National Health Information System (NHIS), the caseload for patients with communicable diseases is significantly higher (58%) compared to 42% patients with non-communicable diseases during 2015 in Punjab. The same was a trend during previous years. The top infectious diseases reported through this system were acute ARI with 13.6% of all visits. Other significant infections were scabies, diarrhoea, dermatitis, worm infestation, malaria, tuberculosis viral
hepatitis, pneumonia and enteric fever. 3.2 mHealth Status in Punjab, Pakistan Currently a number of mHealth applications are being used in Public and Private Health sector in Punjab. Surprisingly, public sector is far ahead of private sector in this regard. The main reason of that is the strong political support for getting such applications designed by the efficient and professional sound staff members of Punjab Information Technology Board (PITB). There is only one health project IRMNCH that has developed some in-house applications to perform its various functions. Otherwise, rest of all mHealth apps in Public sector in Punjab have been designed by PITB. Punjab Information Technology Board is one of the most proactive institution that uses its indigenous expertise in Information Technology to develop high efficient mobile app for many Government departments. Health department was one of the first government representatives that started using professional expertise of PITB. In order to develop mHealth apps, PITB first conducts all relevant stakeholders into confidence and prepare a mobile app after consulting respective health professionals including Entomologist, Environment Inspectors. The mock-up app is designed and tested. It is confirmed only when field staff approves it. Majority of mHealth apps are developed in-house by PITB with no extra payment except their own salaries. Following are the different types of mHealth projects currently being implemented in the public health sector of Punjab

23 | P a g e
3.2.1 m-Health apps for field monitoring and evaluation Some mHealth projects are used to monitor the attendance, performance and quality of work performed by the public health managers and workers.
3.2.1.1 Integrated Reproductive Maternal New-born Child Health and Nutrition Program
This is a public health program with largest network of 46000 Lady Health workers (LHWs) and 1850 Lady Health Supervisors (LHSs) that are providing promotive, preventive, curative and rehabilitative services at community level in 36 districts of Punjab. The objective of this program is to improve access to Reproductive health, Child health and Nutrition services in Punjab through improving contraceptive prevalence rate, increasing skilled birth attendance, increasing institutional deliveries, increasing coverage of complete immunization program and increasing the percentage of children suffering from diarrhoea treated with ORS and Zinc. This program has 70% coverage (37% in Urban and 85% in rural areas) and is contributing to bridge a gap between far off health facilities and communities. The program strengthens the health system at grass root level by strengthening services for provision of qualified and comprehensive Emergency Obstetric and New-born care (EmONC). It also implements woman focused approach by using the 1000days plus model for nutrition that starts from contraception to the first 24 months of child’s life. This program has increased the demand for preventive and primary healthcare services for a targeted group (Women and children) through socially acceptable strategies. In order to improve the patient satisfaction from the community services, this program has designed a system with performance based incentives as well as accountability mechanism. For this purpose, e-reporting and e-monitoring system has been introduced.
Lady Health Supervisor (LHS) Android APP For Lady Health Supervisors, an android based App has been designed by PITB which monitors
Daily attendance
Monitoring of LHW
CMW mentoring
Verify LHWs house
Figure 5: Snapshot of LHS mHealth app

24 | P a g e
Delivery Reporting (in-house developed) Currently IRMNCH & NP working on Real Time Delivery Report and Daily Status Report from Health Facility (BHUs and RHCs) through SMS short code 9697. This application has been developed in-house by IRMNCH.
Figure 6: Snapshot of district MIS dashboard
Neonatal and maternal death e-surveillance (NMDS) (in-house developed) This is also in-house developed app where LHSs are reporting neonatal and maternal death from community through SMS short code 9697. Standard Office Procedure (SOP):
Figure 7: SOP for sms based reporting by LHS

25 | P a g e
ONLINE MIS LHW Program MIS L.HW MIS is supported by TRF+ and it contain monthly report of LHW and LHS.
Figure 8: Monthly Performance evaluation report of LHW and LHS
Verbal Autopsy (in-house developed) Verbal Autopsy is a very important app developed in-house for reporting maternal and neonatal deaths from all 36 districts of Punjab.
. Figure 9: Verbal autopsy report for maternal and neonatal deaths in Punjab

26 | P a g e
IRMNCH MIS This app is used to generate following reports
24/7 BHUs and RHCs health facility
Online Payroll of District Staff
Real Time Delivery Reporting 3.2.1.2) E-VACC
Since Pakistan is one of the only 3 countries in the world, after Nigeria and Afghanistan, where Polio still exists while Measles rate is also quite high here. Therefore, PITB has created another application E-VACC I &II for Smart phones. The purpose of this app is to get geo-tagged photos of the houses visited by each vaccinators/day to ensure the children less than 2 years of age to be vaccinated at their door steps. Almost 4000 vaccinators were equipped with 4000 smart phone and were properly trained to use that application in their field visits. This application is also used to ensure the attendance of the vaccinator along with monitoring of their performance. After successfully launching Phase-I&II of E-VACC program, now the department in the process of launching E-VACC-III where the vaccinator supervisor will be provided with a chip enabling him/her to scan the vaccination card of the baby to see how many vaccination has been completed.
3.2.1.3) Hospital Watch
Public sector healthcare system in Punjab is comprising of huge set- up of 17 teaching/tertiary care hospitals, 115 secondary health care hospitals and about 3500 primary health care facilities (Basic health units and rural health centres). Govt. is spending 2.8% of total GDP for the health of population of 92 million. However, large number of population is not catered in these public health facilities resulting in out of pocket expenses on health care. It is assumed that lack of monitoring and evaluation system on the performance of Public Health Professionals is the main reason behind this low-performance of public health sector. In order to address the growing dissatisfaction with the existing health services and meet the demand of better healthcare, a mobile app “Hospital Watch” has been launched in Apr, 2015.
This mobile app enables the user to monitor hospitals Emergencies, Paediatrics, Obstetrics and Gynaecology wards in 21 District Head Quarters (DHQs) and 101 Tehsil Head Quarters (THQs) across Punjab. The user of this application are District Coordination Officers (DCOs), Executive District Officers Health (EDOH), Assistant Commissioners (ACs), Director General Health Office (DG), Medical Superintendent (MS) and the Members of Provincial Assembly (MPAs). PITB in collaboration with Policy and Strategic Planning Unit (PSPU) and Special Monitoring Unit (S.MU) has imparted training to the user to properly use this mHealth application. However, the prime user of Hospital Watch is MS of the respective hospital who is required to report data on the given fields of this application at least 20days/month. Similarly, EDOH is required to visit each health facility in his/her district at least once a month. The android based application has been installed on smart phones of the users. The main objective of this application is to provide quality healthcare to the masses in Public hospitals, irrespective of their social and economic status. Therefore, frequent surprise visits to the respective health facility supports in documenting the reported parameters.

27 | P a g e
The data submitted by the users through Hospital Watch application is recorded on the dashboard. The real-time data pertaining to attendance, medication, utility and patient’s perception about his/her treatment in the hospital is received. The data is automatically analysed and shared with the health managers at various level. It is expected that information gathered through the usage of this application can be used to measure the performance of District, Tehsil and Administrative health professionals.
3.2.2 m-Health project for infectious diseases Dengue Activity Tracking system Lahore and its surroundings in Punjab were hit by a worst dengue outbreak in 2011 when more than 20000 patients were affected and more than 300 deaths were officially reported. In order to take preventive measures for any future dengue outbreaks, Govt. of Punjab took special initiative by developing Dengue Activity Tracking System 2012 and is operational till today. A proactive approach was adopted to stop prevailing of dengue carrier larvae and mosquitoes by tracking and eradicating their breeding sources and immediately reporting that on dengue app to the concerned authorities. A monitoring mechanism “Dengue Activity Tracking System” requires to log all field activities related to prevention and eradication of the dengue carriers in real time. The reporting on this system is made on portal through GPS enabled android based mobile application. For this purpose, more than 1900 smart phones have been provided to the field officials that can be entomologists, CDC Supervisors, environment inspectors, vaccinators etc. The dengue app covers multiple activities ranging from Larviciding, Dengue patient tagging, OVI taps, tracing adult mosquitoes, Dewatering, FIshseed, Debris removal, Disease surveillance of graveyards, junkayards, abandoned buildings, nurseries, pools etc and conducting dengue awareness workshops in the schools. Each field official is required to perform its designated function and take geo-tagged photographs of that activity in order to monitor not only the performance of that official but also to show that same to the concerned district authorities on dashboard. Field officials are also mandated to identify and remove the larvae breeding hotspots and take two separate geo-tagged “Before” and “After” photographs of that. Spatial-temporal analysis (SaTScan) to identify intersecting areas with dengue larvae breeding hotspots. In addition to this, data entry operators have been deployed in 145 hospitals (Teaching hospitals, District Head Quarter and Tehsil Head Quarter) in Punjab for reporting suspected or confirmed dengue affected patients via “Dengue Patient Reporting System”.
Since, mobile phones capture longitude and latitude along with photographs. Therefore, data submitted by android phones is used to develop real time data streams on Google maps after verifying the data on GPS coordinates. The consolidated online dashboard is also accessible to all stakeholders including district health authorities and higher authorities in the Department of Health. This system is operational in 36 districts of Punjab as well as Islamabad Capital Territory (ICT). Almost 25 government departments are involved in dengue tracking activities. More than 2800 mobile users are added in database. On the whole, this mobile app serves as disease early warning system with geographical illustrations.

28 | P a g e
3.2.3 mHealth project for drug quality assurance Drug Inspection and Monitoring In order to provide affordable and good quality drugs to the population generally and hospitals specially, Govt. of Punjab has launched drug inspection, monitoring and evaluation (DIME) system. The purpose of this Smart phone app is to ensure transparency and keep a checks and balance system on the drugs through drug inspectors. DIME app was launched in 2013 to facilitate the drug inspectors in carrying out their designated functions like inspecting the medical stores selling drugs, record drug contraventions and take corrective measures against the offenders. Through this app, the drug inspectors monitor the registered and unregistered pharmacies, check the available of standard drugs and ensure the compliance of relevant drug laws. DIME is a two stage activity that involves first tagging the drug store to be visited. Tagging involves uploading the picture of the stores, its name, license number and the registration status. The tagged information is verified followed by actual visit of the store. The data uploaded by drug inspectors is compiled in a central data base and displayed at the central web dashboard. Since DIME is a geo-tagged app, so it also facilitates concerned authorities to monitor the performance of drug inspectors.
. Figure 10: Reporting in DIME Figure 11: Snapshot of DIME
3.2.3 mHealth Projects FOR Financial Barriers
Heartfile Health Financing Heartfile is a non-profit organization that focuses on policy analysis and innovative solutions for provision of improved healthcare systems in Pakistan. One glaring example of that is Heartfile Health Financing. Out of pocket expenditure on healthcare are quite high in Pakistan while 60% Pakistanis are employed in non-formal sectors of economy. According to a survey, two third of the households in Pakistan reported to have been affected by one or more health shocks resulting in catastrophic spending on health during the last 3

29 | P a g e
years. In this context, Heartfile has launched Heartfile Health Financing program which is mHealth application that aims to protect the poor people of Pakistan from “catastrophic” expenditure on healthcare. The word “catastrophic” means taking loan or using critical savings or selling personal assets to meet out of pocket healthcare payments. mHealth application is available on website and can be downloaded any android phone. On this application, the demand for health funds is created by the registered health service provider including clinicians, pharmacies, laboratories, rehabilitation centres. The demand is processed in fairly transparent manner with multiple checks to ascertain the eligibility and verify the request/demand. Subsequently, authorize cash transfer for the cost of healthcare is done. For this purpose, Heartfile has also generated “Health equity fund” to seek donations as a means of resourcing cash transfers to poor. To make this project more transparent and efficient, the donors have been given a right to track each transaction of their donations as well as a right to instruct demand specific use of their funds. Thus donors also act as Auditors of the funds of Heartfile Health Financing which makes its unique application with unprecedented advantages. This project is funded by Rockefeller Foundation and is a featured commitment of the Clinton Global Initiative.
3.2.4 mHealth project for cancer patients
Shaukat Khanum Cancer hospital and Research Centre (SKMH &RC) Lahore is known as one of the biggest and state of the art hospital that is established by a charitable organization in Lahore. This hospital aims at acting a model institution for treating the patients suffering from cancer through the application of modern methods of curative methods of curative and palliative therapy. Though cancer patients are being treated in other hospitals of Punjab as well. However, there is no regular data analysis of all such patients in different wards of different hospitals. Management Information System (MIS) department of Shaukat Khanum Memorial (SKM) has developed an android based application to get all such data collected from all hospitals in Punjab through Punjab Cancer Registry. This application has been installed on the personal Smart Phones of different health professionals and medical and paramedical staff. This is user friendly app and the user were trained for almost 4 weeks to use this app and to enter data in the required fields. This mobile app is being used at health facility level to get clinical information collected at one centre. The project has been piloted at HF and is yet to be fully launched. The app will enable the clinicians to review any medical information of a specific patient and make medical decisions accordingly and instantly.

30 | P a g e
SECTIO.N-4 SURVEY FINDINGS AND DISCUSSION 4.1 Survey Design The cross sectional quantitative cum qualitative baseline study was conducted. The study comprised consultation and compilation of both secondary and primary data sources. The questionnaire was considered to be most feasible primary data source to collect basic information about the infrastructure and type of mHealth initiative taken by different projects in Punjab. Due to the wide geographical area, scattered health institutions and time limitations, this questionnaire was the easiest method to collect huge information from large number of respondents. However, to augment the validity and reliability of the data, face to face semi structured and unstructured interviews were also conducted. Face to face interviews were also conducted of few senior administrative and technical coordinators who have either designed mHealth application or are administrative head of the projects/programs that are using those apps. Focus group discussion was also held during provincial meeting to “Review the mHealth applications in Punjab” conducted by WHO on 9th Feb, 2017. The extensive discussion held during the meeting enabled to enrich the report with the information provided by seasoned provincial and district health experts from Public as well as Private sector. The secondary source of data included the PC-1 and official notifications of few of the projects containing the details of the inception of those projects. However, for the sake of privacy policy of those institutions, only those points are being documented here that are publicly shared by their heads in the focus group discussion as well as during interviews.
4.2 Survey Coverage More than 12 programs/ organizations were selected on the basis of snow ball sampling and contacted .in Punjab for this study but only 9 agreed to respond. Thus electronic analysis of the data received from only 9 projects (Annex-1) has been done and discussed in this report. All participants in this study were highly qualified, senior level managers or head of the respective health facility. Lahore is a provincial capital with a population of 5.143 million as per 1998. The headquarters of 7 Public and one private project using android apps are located in Lahore and data collected from all 36 districts of Punjab is also being analysed in Lahore. So Lahore occupied a focal position in this study. In addition to Lahore, mHealth situation of 2 additional districts including Sheikhupura and Nankana was also studied.
4.3 Sample Size Despite the time and resources constrains, a sample of 11 projects was approached to get the data for this baseline survey. However, 9 institutions agreed to respond. There was no point of choice of projects but all the known institutions using smart phone apps for collection of data were contacted. To make this exercise comprehensive, institutes belonging to both public and private sector were included. The reason for inclusion of private sector

31 | P a g e
hospitals/Projects was the assumption that usually private sector/projects are more organized than public sector due to more resources at their disposal. Therefore, they must have a well-established mHealth system. Since tertiary hospitals are currently not using mHealth apps on a wider scale. Therefore, the data was collected only from secondary health institutions. (Annexure-I)
4.4 Data Collection Tool The main data collection instrument was developed in the form of a questionnaire (Annexure-II) which contained mostly structured, close ended question, but a provision of overall comments was also made. Prior to administering questionnaire, telephonic contacts were made with all the respondents to explain them the context and purpose of this study. Semi structured and unstructured interviews of the study participants also helped the interviewees to seek support from the interviewer in filling out the questionnaire (List of interviewees in Annexure-IV). Secondary source of data, i.e, PC-1 and official notifications on data collection and transmission on respective smart phone apps was also studied to get more insight into mHealth applications of the project. Then the data were entered in for the purpose of analysis.
4.5 Data Analysis Methods
The data obtained from the questionnaires filled out by the respondents was coded, entered and analysed by Statistical Package for Social Science (SPSS) version 17. For this a specialized data entry screen for all the variables included in the questionnaire was developed in SPSS. Graphic presentation of the analysed data was interpreted. The information from interviews and documents also corroborated the findings from questionnaires.
4.6 General Observations Almost 10 institutions and projects were contacted to get the data on the respective mHealth apps. However, one institution had stopped using that app while the concerned authority was not around, so only 9 participants responded to the researcher. Among all the participants, 7 were representing public sector and 2 were from Private sector. Overall, all the respondents were using 7 mobile apps to get the required data as shown in the graph below. Three respondents were using one app “Hospital Watch” while among others, one respondent was selected from each projects using 6 different mHealth Apps.
32 | P a g e
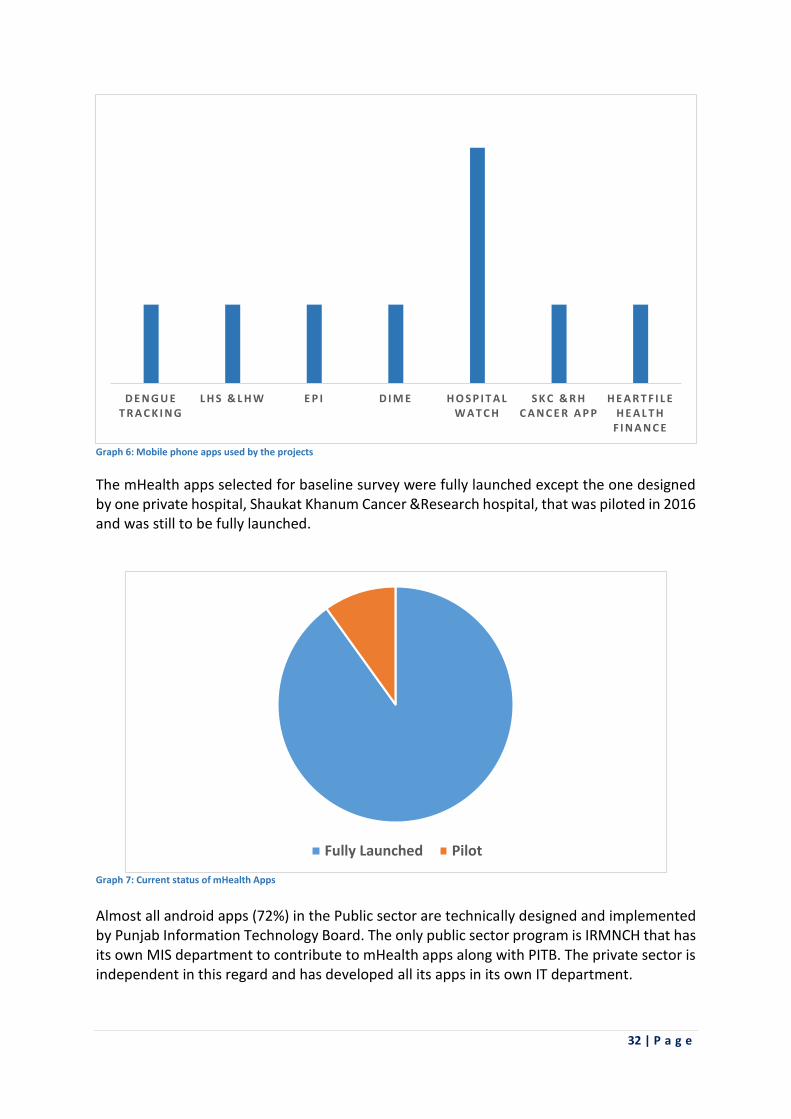
Graph 6: Mobile phone apps used by the projects
The mHealth apps selected for baseline survey were fully launched except the one designed by one private hospital, Shaukat Khanum Cancer &Research hospital, that was piloted in 2016 and was still to be fully launched.
Graph 7: Current status of mHealth Apps
Almost all android apps (72%) in the Public sector are technically designed and implemented by Punjab Information Technology Board. The only public sector program is IRMNCH that has its own MIS department to contribute to mHealth apps along with PITB. The private sector is independent in this regard and has developed all its apps in its own IT department.
D E N G U E T R A C K I N G
L H S & L H W E P I D I M E H O S P I T A L W A T C H
S K C & R H C A N C E R A P P
H E A R T F I L E H E A L T H
F I N A N C E
Fully Launched Pilot

33 | P a g e
Graph 8: Technical stakeholder of mHealth Apps
The Smart phone users were properly trained for a training period spanning less than 1week to almost 4 weeks. Majority of the institutions (50%) have less than 1week training period, around 20% have 2 weeks training while only one institution has trained its users over the period of 4 weeks. There was only one application designed by private NGO, Heartfile, that has no specific training period for the users.
. Graph 9:Training period of Smart phone users
The users academic qualification varies in different projects from under-graduation,i.e, intermediate to post-graduation. It was not necessary for the users to have a medical background but all of them had studied science or biology at secondary or higher secondary school level. There is almost equal percentage of users in each of the 3 category of qualification as shown in the graph no 6.
0% 10% 20% 30% 40% 50% 60% 70% 80%
PITB
IRMNCH
SKC&RH
Heartfile
0%
10%
20%
30%
40%
50%
60%
<1wk 2Wk 4Wk Unspecified

34 | P a g e
. Graph 10: Academic qualification of the mHealth app users
All projects/programs are using mHealth apps to collect variety of information. The functions of the respective institutions are mentioned below while detailed tabulated analysis is attached (Annexure-III).
S# mHealth app Type of Information Collected
1 Heartfile health financing
Demographics and Poverty profiling of the end beneficiary is done on a validated Poverty Scoring card.
2 Cancer app Clinical record keeping
3
Dengue tracking app Geo-tagged information is collected about the Incidence of Positive/negative Larvae and the residence/workplace-Location-Containment Activities
4 Hospital Watch
Recording the availability of doctors and patient’s treatment satisfaction
7 IRMNCH
Monitoring the attendance of LHSs, LHWs and their job performance
8 EPI
1. Vaccination of < 2 years’ children 2. Attendance of vaccinators
9 Chief Drugs Controller, Punjab Office
Tagging and verification of drug stores, record drug, contraventions / Violations
Table 2:Types of information collected by various project using android phones
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
Post grad Grad Undergrad

35 | P a g e
4.7 Discussion The smart phones are a buzz word that was introduced in late 1990’s and soon became not only a fashion symbol but also affected all walks of lives of common man with its multiple apps. Though there is no exact definition of smart phone but it can be defined as “a mobile phone handset with advanced hardware and software capabilities and enable it to perform complex functions similar to those of laptop computers”. The role of smart phones has gradually evolved not only for communication purposes but also for its supporting apps for its consumers. One category of such apps is in the “Health and Fitness category” to target health consumers. Such apps are helpful in promoting the health of individuals and community. Due to the popularity of such apps among the customers, the number of health related apps on the Apple App stores had reached 13000 by 2012. Soon the governments, leading health organizations and health professionals started paying heed to the rapidly changing role of ICTs and android phones to provide health services to remote populations and underserved communities. In the name of eHealth and mHealth, smart phones made health system robust and economically viable in areas with insufficient health infrastructure. Now the use of android phones in health has emerged as a modern tool to replace traditional health services due to the ubiquitous availability of mobile communication technology in almost all parts of the world. According to one study, 89% residents and 98% of faculty members in the US owned smart phones. The same is a scenario in the developing countries where there is a growing trend of discontinuing fixed telephone lines. The use of mobile phones is on rise because they are easy to purchase and carry, with multiple other supporting functions like video calling, SMS and other apps. Gradually, android phones have caught the world attention for performing health related functions by collecting and transmission of data to gauge the satisfactory performance of health services. The smart phones can collect, store and transfer data to a remote database or export data directly to a computer. Thus it is easier to analyse the data for evidence based decision making. The cheap rates and effective monitoring for provision of mobile health than in-person health services is a motivation behind this mHealth evolution turning into revolution. The smart phones in health or mHealth are used for multitude of health functions ranging from healthcare delivery, patient and health workers education, disease surveillance, disease management and electronic medical record keeping. These tools are particularly being used worldwide for improvement in the Maternal, neonatal and Child healthcare services (MNCH). For instance, Tanzania has launched the mobile technology in the RCH where pregnant women are sent reminder SMS to attend their ante-natal visits. Another mHealth intervention of this category is Text for baby. This project was launched in the US in 2010 for free cell phone SMS to pregnant women and new-born babies mothers thrice a week with information about having a healthy pregnancy and a healthy baby. The free text messages provide information on issues related to breastfeeding, immunizations, labour and delivery, prenatal care, exercise and fitness etc. 96% of its 281000 enrolees of this

36 | P a g e
project by Jan 2012, have indicated success of the project by reporting satisfaction over its services and recommending it to their friends as well. Internationally, the role of mHealth has been recognized and being considered as an integral component of health care system. The ICTs tools are incorporated into routine health information system to strengthen the District Health Information System (DHIS) and reporting epidemics and routine surveillance. Similarly, in Solomon Island, DHIS 2 has been installed to collect not only routine and individual patients data but also allow data entry from smart phones with optimized web input. DHIS 2 supports Web-API to get access to all functions of a software thought a web interface. Thus data entry and reporting interface can be customized on mobiles or computers. Since mHealth was taking off globally, Pakistan also joined this bandwagon soon after the worst dengue outbreak in Punjab. Due to the sporadic cases, the surveillance system and vector control program of dengue fever was weak that resulted in medical emergency in Punjab generally and Lahore especially when more than 20000 patients and 321 deaths were reported in the monsoon season of 2011. Later, the change of season and the multifaceted strategy of health department enabled the government to control the outbreak. However, that incidence also proved a turning point in the health sector by introducing the use of mobile phones in reporting and managing dengue fever in Punjab with an application “dengue tracking system”. This system enabled the health department to control dengue fever in future with its multipronged strategy with the help of this mobile app. This led to a development of number of other mHealth apps either for surveillance for other diseases or for management and performance evaluation. The majority of these apps are designed by government organizations and only few are introduced by private sector at limited scale. The detail of the mHealth applications included in this baseline survey are discussed below. Due to strong political support and administrative leadership, mHealth projects are widely popular in healthcare system of Punjab. The financial funding for these projects/programs either come from donor or from the government of Punjab and are embedded in the respective PC-1. All the smart phones apps in Public sector are either designed by PITB or MIS cell of the concerned program. Therefore, free of cost technical expertise is always available. Moreover, recently PITB has also started providing free internet access at public places including hospital in Punjab. Thus internet connectivity that was reported as an operational issue by some projects during the survey, will not be an obstacle in data collection in future. Since purchase of smart phones is a onetime expenditure and the users are usually the health workers already working in the government sector. It means there is no recruitment of new staff members solely for data collection and transmission through smart phones. Therefore, there is no immediate chance of discontinuation of any of these projects due to lack of financial or technical support. However, capacity of the users especially health workers and data entry operators of the mobile data is an issue that needs to be taken into account as pointed out by one surveyed organization in the questionnaire and shared by many other respondents during interviews. Though academic qualification of users range from under graduation to post graduation but they have not been properly trained in typing and transmitting medical data. No checks and

37 | P a g e
balance system has been observed to maintain quality of data and improve the quality of healthcare in future. mHealth is an exciting innovation that is filling an important gap in the surveillance and management of existing health program. It enables fast data travel from the point of collection to point of use which is usually in the form of dashboard of email. It has been observed during the survey that there needs to establish a regular system of data analysis at the point of data collection as well. So that appropriate action could be taken at early stage, instead of being notified by the higher authorities after analysing and communicating the relevant medical emergencies. Since PITB is the agency that takes initiative in designing and launching the mHealth app while the implementing organization is some health program or project. Thus, lack of ownership of the respective smart phone apps was observed during interviews. The interviewees considered such apps to be thrust upon them and had increased their already enormous workload. This was especially true for “Hospital watch” where the highest ranking administrator, usually Medical Superintendent of the health facility, was required to send data at regular interval. Since MS is a very busy person, so this app was criticised almost all the respondents. They thought users are not taken into confidence while designing any mHealth apps. Similarly, the users were also not much aware of the utility of other mHealth apps. They collected required data like robots and sent it to the concerned authorities with any iota of ownership and contribution in the improvement of respective app. This alienation has further increased due to none of the survey ever conducted by the government for opinion of the users and implementers to improve the android apps. This is especially true for government initiated health apps and is a global observation. The only android app improved over the period of time is dengue tracking system. This improvement is more due to the individual efforts of the users or concerned administrators. Such concrete efforts for improvement is missing in case of other health related apps. Such misunderstanding or grievances needs to be addressed at priority basis to enhance the effectiveness of smart phone health apps in Public hospital. Few private organizations have taken initiative to contribute to mHealth in Punjab. Heartfile and Shaukat Khanum Cancer & Research hospitals are two highly respected names in the health community in Pakistan. Though currently Heartfile has introduced its health app in few cities of Punjab and Sindh but keeping in view the importance and success, Heartfile intends to widen its scope to all over the country. Huge out of pocket financial expenditure on health is a big obstacle for poor people in getting access to quality medical treatment. Heartfile has tried to bridge this gap with Heartfile health financing app many years ago. Currently the government has also stepped in the field of health financing by introducing health insurance program for poor people. However, no smart phone health app has been designed for this program yet and it is still using manual data of beneficiaries that was already prepared for distribution of funds by Benazir Income Support Program (BISP).

38 | P a g e
Despite all the operational issues and other obstacles, all respondents recommended to expand the coverage of existing android apps. For instance, E-Vacc program has a plan to launch E-Vacc-III in next few months where vaccination incharge will have a micro-chip to check and monitor the vaccination schedule of any child without his/her manual vaccination card. Similarly, Chief Drug controller Punjab has suggested to use DIME for all districts of Punjab. Heartfile intends to use its app for all regions of Pakistan. The only mHealth tool that was criticised was Hospital Watch which was recommended either to be ended or designate its users other than MS of the hospitals.
4.8 m-Health SWOT Analysis
A brief SWOT analysis of mHealth is shared as under:
Strengths
Mobile apps are used to get access to real time data using GPS system.
Faster access to data is ensured within few minutes as opposed to days and weeks for manual collection of data and preparation of reports.
Updated information is available with health managers.
Timely provision of information is a pre-requisite for evidence based decision making for formulation of health policies as well as treatment of diseases.
Visibility of data ensures accountability of the data collectors and other concerned health professionals for their designated jobs.
Evidence based data enables to justify the funding from donor with better reporting.
mHealth is used not only for collection and transmission of data from health centres but also provide feedback to the health facilities.
Use of smart phone apps in priority disease surveillance is very effective.
There is a positive impact on the reporting environment of health departments.
Reduced expenditure on the fuel, wear &tear of vehicles for only data collection.
Weaknesses. • Financial resources and capacity of IT departments of the health projects/programs
have been recognized as a concern. • Lack of coordination between health professionals using the ICT intervention and the
institutions designing the mHealth application is identified as a barrier obstructing the upgrading of some android based application.
• Since Most of the applications are government centric, therefore, there is a lack of ownership of these apps by the program for which it is created.
• The capacity of the health projects to analyse the data collected and utilize that analysis regularly for improvement in the health system is low.
• Neutral facilitation for group discussion by engaging all stakeholders for emergence of shared action plans for improving health services is ignored.
• Reliance on unreliable mobile handsets and internet connection is a point to be pondered.
• Screen size and (lack of) a keyboard limit the endurance of even the most dedicated field worker.

39 | P a g e
Opportunities.
In order to deliver better healthcare in the 21st Century, contribution of mHealth needs to be considered as an integral component of health system by making legal regulations for it. The standard protocol and legal modes needs to be established to make a workable system of checks and balance to govern mHealth. Regulations about mHealth have a capacity to affect mHealth programs. For instance, security regulations about mobile communication technology may impede the development of mHealth programs about sharing personal health information.
Development of policies and incentives for the health workers to use mHealth efficiently and effectively.
The traditional methods of data collection also needs to be evaluated to check the duplication and quality of data collection and communication.
Effective use of ICTs can educate, empower and connect vulnerable populations to health services in low-income settings for a variety of health services ranging from maternal, neonatal health, immunization, and chronic health
Threat Using mobile technology all the time has its own hazards to physical and mental health of human beings.

40 | P a g e
SECTION-5 RECOMMENDATIONS & WAY FORWARD After going through all research tools including questionnaire and interviews, following recommendations are made in respect of mHealth in Punjab.
There should be regulations and standard protocols to guide and govern rising trend of mHealth.
Privacy, security and confidentiality of personal and health record of health consumers must be ensured while sharing this information only for improvement in the health of the customers.
The smart phone provided to the users must be secure, password protected and maintained with reliable antivirus to prevent the leakage of health record of the patients.
Enormous resources were used to install DHIS that is already working in all 36 districts of Punjab and covering a number of communicable and non-communicable diseases. There is a need to strengthen DHIS and integrate it with the concerned mHealth apps. It may serve as a system to check the quality of digital data.
Vector borne diseases are taking a heavy toll in Punjab and the procedure to control the outbreak of all these diseases are same. Currently only one vector borne disease, DHF has been successfully controlled by using Smart phone app. There is a need to integrate all vector borne diseases prevalent in Punjab including Malaria, Leishmania, Chikungunya etc in this app to create a robust mHealth tool to deal with all these medical ailments.
The ultimate goal of healthcare system is to serve the public. Therefore, public representatives should be taken on-board while designed any mHealth apps. Similarly, the input from the users of the respective app should also be obtained to make it more people centric and user friendly.
The authorities at data collection and entry points should be trained to analyse the data at their end along with empowerment to take appropriate actions.

41 | P a g e
CONCLUSION This is the age of information technology. Sector is also advancing towards utilization of this technology. The biggest advantage of ICT is the availability of this technology in remote areas of the developing countries where health infrastructure is in the shabby state. The use of mobile technology in the form of eHealth or mHealth has enabled the health professionals to provide healthcare services to the public without any interruption. mHealth has proved an exciting innovation to bridge the existing gaps in the healthcare system of the developing countries as well as developed countries. Pakistan is not left behind in using the ICT as a new analytical tool for digital data. A number of smart phone based health apps have been introduced after successful experiment of dengue tracking system in 2012 in Punjab. The role of mHealth is fast increasing and being acknowledged by health professionals as well as Public. The wide acceptance and popularity of mHealth has enabled the government to launch user-centric apps after training the skilled workforce and finding new solution to the existing health problems of the public. The digital data collected by these smart phone apps is analysed by PITB and shared with all its stakeholders in the form of email and dashboard. The concerned authorities at district or provincial level, are expected to take necessary actions accordingly. Thus monitoring and evaluation of health projects is done simultaneously by higher authorities by looking at the digital findings and steps taken for tackling the upcoming health problems. Therefore, there has been substantial increase in the number and range of android health apps. Though universally it has been observed that most of mHealth projects are funded by donors and the projects usually do not move beyond Pilot stage. Even if launched, the mHealth programs come to an end when donor is gone or all money is spent. The financial hurdles and limited government ownership has proved to be a biggest hurdle in launching such programs at regional or national scale. This is not so in Pakistan. Due to strong political support and administrative leadership, all mHealth programs have been launched and are being governed by PITB and Department of Health. There is a need to integrate mHealth into routine healthcare delivery system to make it integral component, instead of treating it as a separate component of health system. It enables the governments to find comprehensive solution to many health problems by ending silo solutions. It will also end unreasonable data collection burden on staff and maintenance of manual registers and then transmission of that printed data through posts or courier. mHealth solutions to bridge the gaps in the health system best reflect the needs of health consumers for seeking health information and health professionals for management of healthcare system at district, provincial and national level. However, the process of embedding mHealth everywhere still has a long way to go in health system and require standard protocol and legal infrastructure to support it. The smart phones have ability to improve surveillance, clinical care, disease prevention and self-management. There is a requirement of using these tools under guidance and monitoring for the improvement of health care system with dedication, planning and monitoring.

42 | P a g e
REFERENCES
1) Ashraf et al. (2015) “Overview of a multi-stakeholder dialogue around Shared Services for Health: The Digital Health Opportunity in Bangladesh” Health Research Policy and Systems, 13:74, DOI 10.1186/s12961-015-0063-2
2) As mHealth Expands, a Call to Curb the Enthusiasm Accessed at: https://www.measureevaluation.org/news/as-mhealth-expands-a-.call-to-curb-the-enthusiasm
3) BinDhim F N. and Trevena L. (2015) “There’s an App for That; A Guide for Healthcare Practitioners and Researchers on Smartphone Technology” Online Journal of Public Health Informatics, 7(2):e218.
4) Burney A.,Abbas Z.,Mahmood N.,Arifeen Q. (2013)”Prospects for Mobile Health in Pakistan and Other Developing Countries” Advances in Internet of Things, 3:27-32
5) Githinji S, Kigen S, Memusi D, Nyandigisi A, Mbithi AM, et al. (2013) Reducing Stock-Outs of Life Saving Malaria Commodities Using Mobile Phone Text- Messaging: SMS for Life Study in Kenya. PLoS ONE 8(1): e54066. doi:10.1371/journal.pone.0054066
6) Heartfile Health Financing Accessed at: http://www.heartfilefinancing.org/HeartFilePage_0_752.aspx
7) Leal-Neto OB, Dimech GS, Libel M, Oliveira W and Ferreira JP. (2016) “Digital disease detection and participatory surveillance: overview and perspectives for Brazil” Rev Saude Publica.50:17.
8) Measure Evaluation “As mHealth Expands, a Call to Curb the Enthusiasm” Accessed at: https://www.measureevaluation.org/news/as-mhealth-expands-a-call-to-curb-the-enthusiasm
9) Multiple Indicator Cluster Survey, Bureaue of Statistics Punjab Accessed at : http://www.bos.gop.pk/mics
10) “Improving Monitoring and Supervision at the Health Facility Level Through End-Use Verification and Mobile Technology” Accessed at:http://deliver.jsi.com/dlvr_content/resources/allpubs/logisticsbriefs/MalLogHigh_ImpMonSupHFL.pdf
11) Integrated Reproductive Maternal Newborn Child Health and Nutrition Program Accessed at: http://www.irmnch.gop.pk/
12) mHealth Alliance and Vital Wave consulting (2013) “Sustainable Financing for Mobile Health (mHealth): Options and opportunities for mHealth financial models in low and middle-income countries ”Punjab information Technology Board https://www.pitb.gov.pk/
13) Routine Health Information Network (Apr 2-8, 2013) “Innovating Application of Mobile Technologies with Routine Health Information Systems” RHINO Forum Transcript
14) USAID/Deliver Project (Nov, 2010) “Improving Monitoring and Supervision at the Health Facility Level Through End-Use Verification and Mobile Technology”, Task Order 3.
15) “Using Mobile Technology to Achieve a Steady Supply of Essential Medicines” Accessed at: http://snisnet.net/mHealth_infographic_EssentialMeds_withJSIlogo_1.pdf
16) UN Commission on life saving commodities for women and children Accessed at: http://www.unfpa.org/publications/un-commission-life-saving-commodities-women-and-children
17) White, A., Thomas, D.S.K., Ezeanochie, N. and Bull, S. ( May 2016) “Health Worker mHealth Utilization: A Systematic Review” CIN: Computers, Informatics, Nursing,34:5,p 206–213, Wolters Kluwer Health, Inc

43 | P a g e
18) World Health Organization (2016) “Global diffusion of eHealth: making universal health coverage achievable. Report of the third global survey on eHealth”
a. ISBN 978-92-4-151178-0
.

44 | P a g e
ANNEXURES
Annexure-i: Projects / Program Surveyed for Data Collection
Sr. # Institution name Project Name
1 Heartfile Heartfile Health Financing
2 SKMCH&RC Cancer Mobile App
3 Punjab Information Technology Board Dengue Tracking System
4 DHQ Nankana Sahib Hospital Watch
5 DHQ Sheikhupura Hospital Watch
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Hospital Watch
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
IRMNCH & NP
8 Expanded Program on Immunization Expanded Program on immunization
9 Chief Drugs Controller Office, Punjab Drug Inspections Monitoring & Evaluation (DIME)

45 | P a g e
Annexure-ii: Data Collection Tool (Questionnaire)
Sr. No
Categories Description
1 Project Name
2 Location / Address
3 Institution/ Program name
4 Department
5
Application Developed by:
Company Name Team leader (If any) Individual developer
6
Application Development In house PITB DOH
Open Source Purchased Others
7
Smart Phones and application Funded by
Project Itself Donor DOH Other
8 Focal Person (Name)
Administration Coordinator Technical Coordinator
9 Scope (Local/District/ Field Community)
10
User Qualification (Community/LHW/Health Facility)
Post Graduate Graduate
Under Graduate Intermediate Any Other
11 Contact Person Name , Email and Cell No
12 Objective/ Purpose of this application
13
Being Used in Field by Health Center
LHS LHW Prog. Worker Others.
14 Type of Information Collected
15 Is location being captured?
Yes No Entry Time

46 | P a g e
Sr. No
Categories Description
16 Project Phase
Concept
Pilot
Fully Launched
Regularized Other
17 Technical/IT Support Team /Back stopping
Yes No Detail
18 If yes (State Mechanism)
19 Operational Issues
20 Future Prospects
21 Major Barriers (If any) to Implementation
22
Costs Involved:
Capital Cost
HR staff in the office & field
No of Smart Phones
No of data Analysts
IT Team Trainings held Other
23 Operational Cost / Month Recurrent Support available till
24 Types of Servers
Linux server Windows Server
Member Server SQL Server
Backup Server Application Server
Live Access Server Any other describe
25 Computer language Used
26 Any Training Given to the users of smart phone?
Yes No

47 | P a g e
27 If yes, then how long that training was and how frequently training is refresher?
Less than 1 week 2 weeks
3 weeks 4 weeks
28 How frequently user of smart phone is refresh?
Monthly Annually Other
29 Administrative Commitment
(PC1 & funding) Political Commitment
30 Where this data of this project is sent?
DOH(Primary) DOH( Tertiary)
DG Health Office MOH
31 How frequently data is sent to higher authority?
Daily Weakly
Monthly Yearly
32
Modes of Communication of data to higher ups?
Email What app
Dashboard Post
33 Is data analysis being done after all data collection?
Yes
No
34 Is this information being used for Policy Making?
Yes No
35 If yes, at which level of health system?
Overall Comments / Observations/Recommendation

48 | P a g e
Annexure-iii Analytical Report of mHealth Projects, Punjab
Baseline Survey for Use of Smart Phones / Applications for Public Health in Pakistan
Analysis of Reported Information
Institute / Program Approach
Sr. # Institute / Program Project Name
1 Heartfile Heartfile Health Financing
2 SKMCH&RC Mobile App
3 Punjab Information Technology Board Dengue Tracking System
4 DHQH Nankana Sahib Hospital Watch
5 P&S Health Care Department Hospital Watch
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore Hospital Watch
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
IRMNCH & NP
8 Expanded Program on Immunization Expanded Program on immunization
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Drug Inspections Monitoring & Evaluation (DIME)
Introductory Information
S# Institute / Program Department Company Name
Team leader (If any)
Individual developer
1 Heartfile Health Financing
Healthcare Technologies (SMC-Pvt) Ltd.
2 SKMCH&RC MIS
MIS Department of SKMCH & RC
3 Punjab Information Technology Board
E-Government Applications
PITB Saflain Haider (Director)
Shahzad Anwer (Program Manager)
4 DHQH Nankana Sahib Health
5 P&S Health Care Department PITB
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Health
7 Integrated Reproductive Maternal Newborn Child Health & Nutrition Program
Health Department Punjab
PITB TRF+ UNFPA
8 Expanded Program on Immunization
Health PITB
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
PITB

49 | P a g e
Administrative information
S# Institute / Program Administration Coordinator
Technical Coordinator
Scope
1 Heartfile Healthcare Technologies (SMC-Pvt) Ltd.
Field Community
2 SKMCH&RC Manzar Abbas Hyderi Local
3 Punjab Information Technology Board Shahzad Anwar Provincial
4 DHQH Nankana Sahib Dr. Muhammad Afzal, SMO
District
5 P&S Health Care Department MS DHQ Hospital SKP District
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Dr. Ahmed Bilal Bhatti District
7 Integrated Reproductive Maternal Newborn Child Health & Nutrition Program
Dr. Ambreen Fatima, MIS Incharge
Imran Durrani, Software Engineer
Field Community
8 Expanded Program on Immunization Dr. Muhammad Munir Ahmad
Field Community
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Program Coordinator PITB & Office of Chief Drugs Controller
PITB Paper free working structure
Funding Resource
S# Institute / Program
Application Development
Smart Phones & application Funded by Others
1 Heartfile Others Donor
USAID-HSSC & other Bilaterol donors
2 SKMCH&RC In house Project Itself
3 Punjab Information Technology Board PITB Project Itself Govt. of Punjab
4 DHQH Nankana Sahib PITB Other Govt. of Punjab
5 P&S Health Care Department . Other Govt. of Punjab
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
PITB Other Govt. of Punjab
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
PITB Donor PITB
8 Expanded Program on Immunization PITB DOH
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
PITB
..

50 | P a g e
User Qualification
S# Institute / Program User Qualification Any other
1 Heartfile Any Other
Trained Program staff (in-house) Doctors, Medical suppliers, Patients
2 SKMCH&RC Post Graduate
3 Punjab Information Technology Board
4 DHQH Nankana Sahib Graduate MBBS
5 P&.S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore Graduate MBBS
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Post Graduate
8 Expanded Program on Immunization Intermediate
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Post Graduate
Contact Information
S# Institute / Program Contact Person Name Email Cell No
1 Heartfile Ihtiramul Haq Khattaak [email protected] 0310-543981
2 SKMCH&RC Manzar Abbas [email protected] 0308-4435605
3 Punjab Information Technology Board
Shahzad [email protected]
0334-5408718
4 DHQH Nankana Sahib Dr. Muhammad Afzal [email protected] 0301-4196417
5 P&S Health Care Department Shahnaz Naeem [email protected] 0333-6477269
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Dr. Ahmed Bilal Bhatti [email protected] 0322-4787189
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Imran Durrani [email protected] 0345-2589994
8 Expanded Program on Immunization
Dr. Munir Ahmad [email protected]
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Mr. Moeen Akhtar Program Coordinator
[email protected] 0321-4463118

51 | P a g e
Objective / Purpose
S# Institute / Program Objective/ Purpose of this application
1 Heartfile
Protecting vulnerable population from catastrophic Healthcare expenditure
2 SKMCH&RC
3
Punjab Information Technology Board
To report & monitor the preventive activities being conducted by Field teams for vector borne diseases, Geo-tagging of HOTSPOTS, Confirmed Dengue Patients (residence & workplace), Early epidemic alerts
4 DHQH Nankana Sahib
5 P&S Health Care Department Monitoring, Supervision and Evaluation
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization Monitoring and tracking of vaccinators in field
9 Primary & Secondary Health Care Department, Govt. of Punjab Chief Drugs Controller, Punjab Office)
The system enables drug inspectors to monitor and check registered and unregistered pharmacies, the availability of standard drugs at these pharmacies and ensure the stores’ compliance with drug laws. Moreover, DIME is geo-tagging enabled and facilitates the higher authorities in checking whether the drug inspectors are visiting their concerned pharmacies regularly.
Used in Field by
S# Institute / Program Health Centre LHS LHW Prog. Worker Other
1 Heartfile Yes No No Yes Suppliers
2 SKMCH&RC Yes No No No
3
Punjab Information Technology Board
Health Teams, Allied Departments such as Environment, LG&CD, LWMC, TMA etc.
4 DHQH Nankana Sahib Yes Health Centre
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Yes
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Yes Yes Yes Yes
8 Expanded Program on Immunization Yes Vaccinators
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Drug Inspectors

52 | P a g e
Type of Information Collected
S# Institute / Program Type of Information Collected
1 Heartfile
Demographics and Poverty profiling of the end beneficiary is done on a validated Poverty Scoring card.
2 SKMCH&RC Clinical
3 Punjab Information Technology Board
When official’s geo tag the area following type of info is collected. -Incidence of Positive/negative Larvae-Confirmed Patient Residence/workplace-Location-Containment Activities
4 DHQH Nankana Sahib
5 P&S .Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Patient Satisfaction, Medicine & Doctor Availability
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization
1. Vaccination of < 2 years’ children 2. Attendance of vaccinators
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Tagging and verification of drug stores, record drug, contraventions / Violations
Location Access of Data Collector
S# Institute / Program Is location being captured? Entry Time
1 Heartfile Yes Entry time
2 SKMCH&RC Yes Entry time
3 Punjab Information Technology Board Yes
4 DHQH Nankana Sahib Yes
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Yes
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Yes
8 Expanded Program on Immunization Yes
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Yes
.

53 | P a g e
Status of Project
S# Institute / Program Project Phase
1 Heartfile Fully Launched
2 SKMCH&RC Pilot
3 Punjab Information Technology Board Regularized
4 DHQH Nankana Sahib Other
5 P&S Health Care Department Fully Launched
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore Other
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Fully Launched
8 Expanded Program on Immunization Fully Launched
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Fully Launched (in 9 divisional headquarters of Punjab)
Technical Support by
S#
Institute / Program
Technical/IT Support Team /Back stopping Details If yes (State Mechanism)
1 Heartfile No
Developer managed support
Online portal for reporting and logging support tickets
2 SKMCH&RC Yes In-house development
3 Punjab Information Technology Board Yes
Technical Support by PITB
Resolution to all technical quires being raised by field tea
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
No
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
We have in-house development MIS team
8
Expanded Program on Immunization Yes
PITB team collects and analyze the data of vaccination of children and attendance of vaccinators in field
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Yes
All the necessary development and operational support is
provided by PITB
.

54 | P a g e
Operational Issues Identified
S# Institute / Program Operational Issues
1 Heartfile Dependence on high bandwidth internet.
2 SKMCH&RC Carrying of Mobile / Tab for clinical staff
3 Punjab Information Technology Board
Departments not investing in upgrading the current tools
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization
Some of the vaccinators find difficult to use android phone so there working hours are increased
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Connectivity issues
Future Prospects
S# Institute / Program Future Prospects
1 Heartfile
(mMoney) mobile Money transaction across the platform; Primary Health; Care Financing; Health loans. Bring Your Own Device (BYOD) resourcing model.
2 SKMCH&RC
3 Punjab Information Technology Board
Similar technology can be used for tracking/monitoring of other diseases
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
To improve and strengthen the real-time data from health facilities and communities level
8 Expanded Program on Immunization E-VACC III
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Expansion of project on whole Punjab Basis

55 | P a g e
Major Barriers
S# Institute / Program Major Barriers (If any) to Implementation
1 Heartfile Cost implications for Enterprise level solution
2 SKMCH&RC
3 Punjab Information Technology Board
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization
Time taking and not user friendly for few of the vaccinators
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Funds for mobile sets and internet coverage in remote areas of Punjab
Resources (Physical / Human)
S#
Institute / Program HR staff in the office & field
No. of smart phones
No. of data analysis
IT team
Trainings held others
1 Heartfile 8 8 2
2 SKMCH&RC 30 2 3
3 Punjab Information Technology Board 500 15
4 DHQH Nankana Sahib 1
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
3 2 3
8 Expanded Program on Immunization 4000 4000
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Yes
Yes Yes Yes Yes

56 | P a g e
Types of Server
S#
Institute / Program
Operational Cost / Month
Linux server
Window server
Member server
SQL server
Backup server
Application server
Live Access server
Any other desire
1 Heartfile 1 1 1 1 1
2 SKMCH&RC 2 2 2 2 1
3 Punjab Information Technology Board
4 DHQH Nankana Sahib 1
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
1 1 1 SMS API
server
8 Expanded Program on Immunization
1
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Yes
Computer Language Used
S# Institute / Program Computer language Used
1 Heartfile Net Technology Framework
2 SKMCH&RC Android
3 Punjab Information Technology Board PHP, SQL, Ruby on Rails
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program PHP, .Net and JAVA
8 Expanded Program on Immunization Urdu
9 Primary & Secondary Health Care Department, Govt. of Punjab, (Chief Drugs Controller, Punjab Office)

57 | P a g e
Training Status
S#
Institute / Program Any Training Given
to the users of smart phone?
If yes, then how long that training was and how frequently
training is refresher?
1 Heartfile No
2 SKMCH&RC 4 weeks
3 Punjab Information Technology Board Yes 2 weeks
4 DHQH Nankana Sahib Yes Less than 1 week
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Yes Less than 1 week
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Yes 2 weeks
8 Expanded Program on Immunization Yes Less than 1 week
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Yes
Frequency of Refreshed
S#
Institute / Program How frequently user of smart
phone is refreshed? Unspecified
1 Heartfile
2 SKMCH&RC Other As needed
3 Punjab Information Technology Board Other As needed
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore Other
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization Other
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Annually

58 | P a g e
Administrative / Political Commitment
S#
Institute / Program Administrative Commitment
Political Commitment
1 Heartfile
2 SKMCH&RC
3 Punjab Information Technology Board
4 DHQH Nankana Sahib
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
8 Expanded Program on Immunization PC-1 Yes
9 Primary & Secondary Health Care Department, Govt. of Punjab; (Chief Drugs Controller, Punjab Office)
Data Sharing
S# Institute / Program
Where this data of this project is
sent?
How frequently data is sent to
higher authority?
Modes of Communication of data to higher ups?
1 Heartfile
2 SKMCH&RC
3 Punjab Information Technology Board
4 DHQH Nankana Sahib Daily Dashboard
5 P&S Health Care Department DOH(Primary) Daily Dashboard
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
DOH (Tertiary) Daily Dashboard
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
DG Health Office Monthly Email
8 Expanded Program on Immunization DG Health Office Daily
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Weekly Email

59 | P a g e
Analysis of Data Collection
S#
Institute / Program Is regular data analysis being done
after all data collection?
1 Heartfile
2 SKMCH&RC
3 Punjab Information Technology Board
4 DHQH Nankana Sahib Yes
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore Yes
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Yes
8 Expanded Program on Immunization Yes
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office) Yes
Is this information being used for Policy Making?
S# Institute / Program
Is this information being used for Policy Making?
If yes, at which level of health system?
1 Heartfile
2 SKMCH&RC
3
Punjab Information Technology Board
Secretary office, DG Health office and DCO’s used the information for decision making regarding the areas to be focused more for surveillance
4 DHQH Nankana Sahib At provincial level.
5 P&S Health Care Department
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
At provincial level.
7 Integrated Reproductive Maternal New-born Child Health & Nutrition Program
Yes
8 Expanded Program on Immunization Yes District and provincial level
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Yes Secretary Health, Chief Sec. CM Punjab Level

60 | P a g e
Overall Observations & Recommendation
S# Institute / Program Overall Comments / Observations/Recommendation
1 Heartfile Heartfile Health Financing has an extremely fast turnover and we also update our website and system in real time. This means that you can actually choose to help a patient who is in the hospital right now and will benefit from your donation in the next few days! Donors receive an email, SMS or letter every time any of your money is spent by Heartfile Health Financing. Donors can earmark their donation in terms of diseases, age, Gender and Geographical
2 SKMCH&RC This App supports clinicians and nursing staff to review any important medical information and to make quick clinical decisions for their patients using their mobiles and tabs.
3 Punjab Information Technology Board The project proves very useful and informative in controlling dengue across Punjab. More than 30,000 activities submitted every day through smart phones and more than 15 million verifiable activities with geo-tagged location since the launch of project. These activities helped in reducing the death rates and number of confirmed patients.
4 DHQH Nankana Sahib Only one patient data should be sent on daily basis as three patients data require much time.
5 P&S Health Care Department Work Load Increased while there is no visible effect
6 Govt. Mian Munshi DHQ Teaching Hospital Lahore
Only one patient data should be sent on daily basis as three patients data require much time.
7 Integrated Reproductive Maternal Newborn Child Health & Nutrition Program
8 Expanded Program on Immunization
After launching of EVACC I & E- VACC II there has been considerable improvement in Routine immunization coverage and attendance of vaccinators has also significantly improved in field.
9 Primary & Secondary Health Care Department, Govt. of Punjab (Chief Drugs Controller, Punjab Office)
Application proves very beneficial in controlling and eliminating the menace of fake drugs from Punjab and to monitor the field working of regulators. I recommend that this application should be operational on whole Punjab Basis.

61 | P a g e
Annexure-iv: List of Officials Interviewed
S. No Name Designation
1 Dr. Munir Ahmad Add. Director, EPI Program, DG Health Office, Punjab
2 Dr. Mehmood Salahuddin Acting Incharge, IRMNCH
3 Dr. Farrukh Sultan Add.Director (Dengue Control Cell)
4 Mr. Shahzad Anwa Program Manager dengue, PITB
5 Dr. Imran Bashir Incharge, Malaria Control Cell,
6 Mr. Arsalan Manzoor Disease Surveillance Program, PITB
7 Dr. Amir MS, Mian Munshi Hospital
8 Dr. Afzal MS, DHQ Nankana
9 Dr. Saba Heartfile.Senior Manager organization Management
10 Mr. Manzar Abbas Shaukat Khanum Hospital. Head of software development
11 Dr. Zaka-ur-Rehman Chief drug Punjab







![PAK-A-PUNCH & KEY BLANK REFERENCE - ABsupply.net · 2015-11-18 · pak-a-punch & key blank reference ... valet an1-an9282 x9/73vb pak-v1 v01 acces pak-90v 90deg ... [-p] pak-v1 v01](https://img.pdfslide.us/doc/110x75/5b3896967f8b9a5a518d9b59/pak-a-punch-key-blank-reference-2015-11-18-pak-a-punch-key-blank-reference.jpg)