Embed Size (px)
Citation preview

Pain measurement tools for clinical practiceand researchSTEPHEN A. FLAHERTY, CRNA, MSRiver Forest, Illinois
An important component of effectivepostoperative pain management is a measureof the patient's pain intensity. This articleexamines three unidimensional painmeasurement instruments and onemultidimensional pain measurementinstrument used in daily practice andclinical research. The strengths andweaknesses of the numerical rating scale,verbal descriptor scale, visual analogue scale,and the McGill Pain Questionnaire arediscussed. Issues of validity and reliability,important in clinical research, are alsopresented.
Key words: McGill Pain Questionnaire,pain measurement, postoperativeperiod, visual analogue scale.
IntroductionAn important component of effective postopera-tive pain management is a measure of the patient'spain intensity. The personal nature of pain com-plicates its measurement and necessitates relianceon instruments which equate subjective feedbackwith objective data. This article examines painmeasurement instruments routinely used in theevaluation of acute postoperative pain in the adultpopulation.*
Three unidimensional pain measurement in-struments (those measuring only one dimension of
pain) are discussed. One multidimensional painmeasurement instrument, capable of measuringseveral facets of the pain experience, is also exam-ined. The numerical rating scale (NRS), the verbaldescriptor scale (VDS), and the visual analoguescale (VAS) comprise the unidimensional instru-ments; while the McGill Pain Questionnaire(MPQ) is the multidimensional instrument. Thefirst two instruments find common use in dailypractice; the latter two instruments, in clinicalresearch.
Issues in pain measurementBoth the clinician and the pain researcher face
three distinct challenges when attempting to mea-sure pain. First, the pain experience must beviewed from the perspective of the patient. This ismade difficult by both the patient and the clini-cian/researcher who brings his or her own uniqueperceptions and responses to the pain experience.What the patient describes is filtered through the
* For a discussion of pain assessment in children refer to:Schecter NL, Berde CB, Yaster M, eds. Pain in Infants, Children and
Adolescents. Baltimore, Maryland: Williams & Wilkins. 1992.The reader is also referred to:
Acute Pain Management Guideline Panel. Acute Pain Management:Operative or Medical Procedures and Trauma. Clinical Practice Guideline.AHCPR Pub. No. 92-0032. Rockville, Maryland: Agency for HealthCare Policy and Research, U.S. Department of Health and HumanServices. Feb. 1992.
Jacox A. Carr DB, Payne R, et al. Management of Cancer Pain. Clini-cal Practice Guideline. No. 9 AHCPR Publication No. 94-0592, Rockville,Maryland. Agency for Health Care Policy and Research, U.S. Depart-ment of Health and Human Services, Public Health Service, March1994.
April 1996/ Vol. 64/No. 2 133
clinician's/researcher's understanding of painbased on his or her own prior experience. For ex-ample, the patient's description of pain in his bro-ken leg is interpreted by the clinician/researcherthrough reference to a personal, usually different,suffering of pain-perhaps hurting a toe gettingout of the shower. The clinician/researcher mustalways be aware of this unavoidable bias, as some-thing is always lost in translation.
Next, both clinical and personal factors candramatically influence the patient's perception ofand response to pain. The type of pain, its dura-tion, and its etiology, as well as any prior experi-ence with the therapy employed in its manage-ment, are all clinical factors influencing themeasurement of pain. Patient characteristics suchas education level, nature of physical illness, gen-der, presence of affective disorders, visual ability,and ethnic background all have been shown to in-fluence pain measurement in specific popula-tions. 3-7
Finally, only a limited number of pain mea-surement instruments are available that are quan-tifiable, reliable, and valid. Many researchers useordinal measure Likert scales or interval measurevisual analogue scales in an attempt to measureand quantify pain intensity. The major limitationof these unidimensional instruments is their ques-tionable ability to measure the multidimensionalaspects of pain.7 Each instrument possesses advan-tages and disadvantages when used either in dailypractice or clinical research, which are discussedin this article.
Unidimensional instrument: Numerical ratingscale
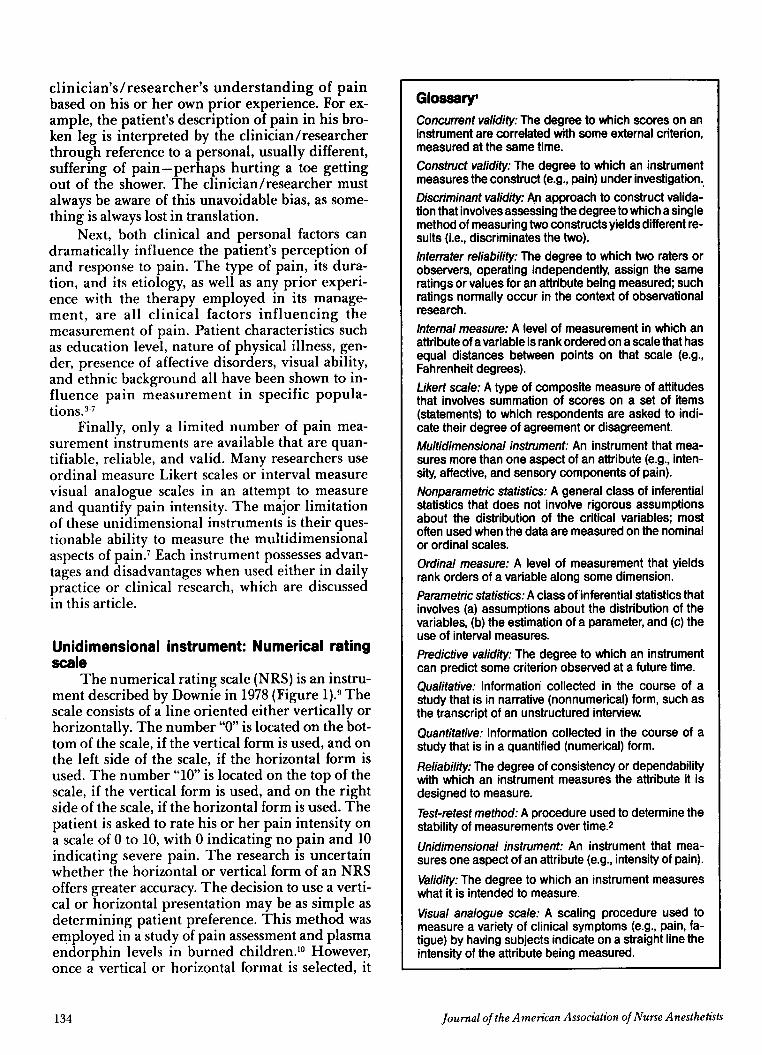
The numerical rating scale (NRS) is an instru-ment described by Downie in 1978 (Figure 1).9 Thescale consists of a line oriented either vertically orhorizontally. The number "0" is located on the bot-tom of the scale, if the vertical form is used, and onthe left side of the scale, if the horizontal form isused. The number "10" is located on the top of thescale, if the vertical form is used, and on the rightside of the scale, if the horizontal form is used. Thepatient is asked to rate his or her pain intensity ona scale of 0 to 10, with 0 indicating no pain and 10indicating severe pain. The research is uncertainwhether the horizontal or vertical form of an NRSoffers greater accuracy. The decision to use a verti-cal or horizontal presentation may be as simple asdetermining patient preference. This method wasemployed in a study of pain assessment and plasmaendorphin levels in burned children. 0 However,once a vertical or horizontal format is selected, it
GlossaryConcurrent validity: The degree to which scores on aninstrument are correlated with some external criterion,measured at the same time.Construct validity: The degree to which an instrumentmeasures the construct (e.g., pain) under investigation.Discriminant validity: An approach to construct valida-tion that involves assessing the degree to which a singlemethod of measuring two constructs yields different re-sults (i.e., discriminates the two).Interrater reliability: The degree to which two raters orobservers, operating independently, assign the sameratings or values for an attribute being measured; suchratings normally occur in the context of observationalresearch.Internal measure: A level of measurement in which anattribute of a variable is rank ordered on a scale that hasequal distances between points on that scale (e.g.,Fahrenheit degrees).Likert scale: A type of composite measure of attitudesthat involves summation of scores on a set of items(statements) to which respondents are asked to indi-cate their degree of agreement or disagreement.Multidimensional instrument: An instrument that mea-sures more than one aspect of an attribute (e.g., inten-sity, affective, and sensory components of pain).Nonparametric statistics: A general class of inferentialstatistics that does not involve rigorous assumptionsabout the distribution of the critical variables; mostoften used when the data are measured on the nominalor ordinal scales.Ordinal measure: A level of measurement that yieldsrank orders of a variable along some dimension.Parametric statistics: A class of inferential statistics thatinvolves (a) assumptions about the distribution of thevariables, (b) the estimation of a parameter, and (c) theuse of interval measures.Predictive validity: The degree to which an instrumentcan predict some criterion observed at a future time.Qualitative: Information collected in the course of astudy that is in narrative (nonnumerical) form, such asthe transcript of an unstructured interview.Quantitative: Information collected in the course of astudy that is in a quantified (numerical) form.Reliability: The degree of consistency or dependabilitywith which an instrument measures the attribute it isdesigned to measure.Test-retest method: A procedure used to determine thestability of measurements over time. 2
Unidimensional instrument: An instrument that mea-sures one aspect of an attribute (e.g., intensity of pain).Validity: The degree to which an instrument measureswhat it is intended to measure.Visual analogue scale: A scaling procedure used tomeasure a variety of clinical symptoms (e.g., pain, fa-tigue) by having subjects indicate on a straight line theintensity of the attribute being measured.
Journal of the American Association of Nurse Anesthetists
°
134
should not be changed during the course of thestudy.
Although the NRS was originally publishedas a line with a scale of 0 to 10, multiple versions ofthis scale currently exist. This multiplicity of scalesis the result of attempts to improve:
1. Ease of administration and scoring.2. Rates of correct response.3. Sensitivity of the scales.4. Ability to detect treatment effects.' 0
Some clinicians use a 0 to 5 scale, while othersuse a 0 to 10 scale. Visual cues may or may not beincluded. The latter type of scale is used as a mea-sure of pain intensity at the author's institution inthe postanesthesia care unit and in other patientcare areas.
The NRS has several practical advantages overother pain measuring scales. The scale is simple toadminister, easy to score, and readily administeredin either written or verbal form." The scale can beused with non-English speaking patients throughthe appropriate substitution of the anchor wordsin the patient's native language. The majority ofpatients understand this scale, and it can be usedto measure both the intensity of acute pain and theefficacy of analgesic therapy. Its chief disadvan-tage is its use at extremes of age. Impaired cogni-tion is sometimes found in the elderly, and theinability of the very young to differentiate wordsand numbers may prohibit use of the NRS.
Unidimensional instrument: Verbal rating scale/verbal descriptor scale
Keele first devised the verbal rating scale/verbal descriptor scale (VDS) and established its
Figure 1A format of the numerical rating scale (NRS)
10
9
8
7
65
4
3
2
10
NRS
April 1996/ Vol. 64/No. 2
Downie WW, Leatham PA,(Reprinted with permission fromRhind PA, et al. Page 378.9)
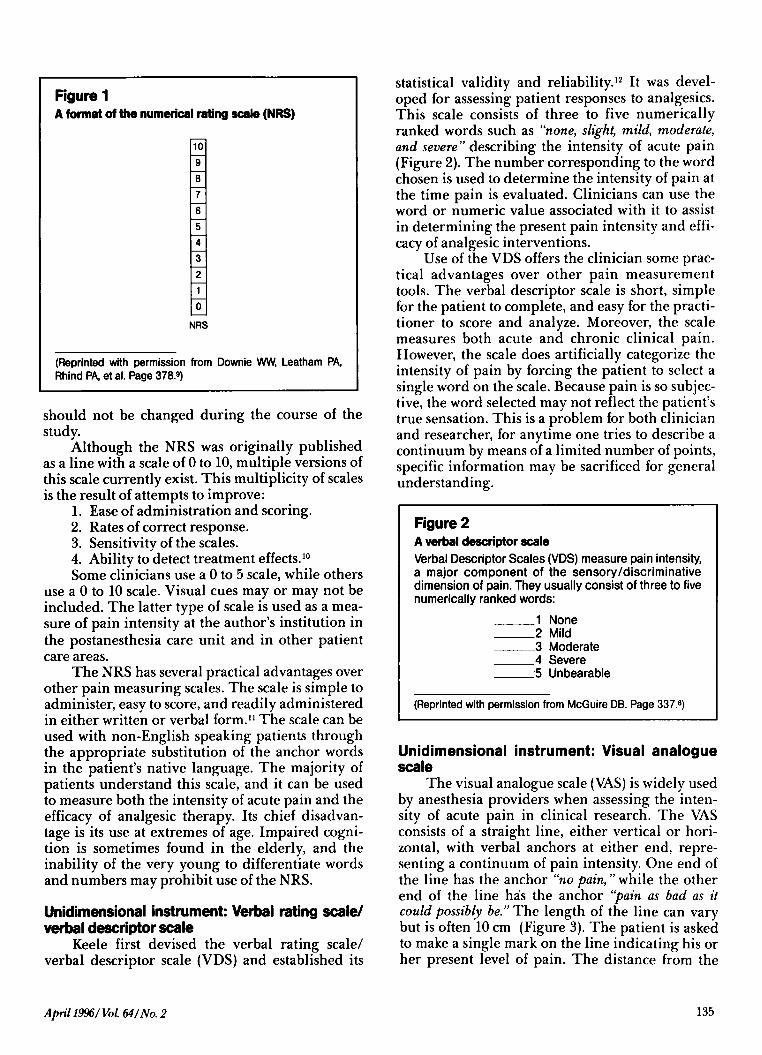
statistical validity and reliability.12 It was devel-oped for assessing patient responses to analgesics.This scale consists of three to five numericallyranked words such as "none, slight, mild, moderate,and severe" describing the intensity of acute pain(Figure 2). The number corresponding to the wordchosen is used to determine the intensity of pain atthe time pain is evaluated. Clinicians can use theword or numeric value associated with it to assistin determining the present pain intensity and effi-cacy of analgesic interventions.
Use of the VDS offers the clinician some prac-tical advantages over other pain measurementtools. The verbal descriptor scale is short, simplefor the patient to complete, and easy for the practi-tioner to score and analyze. Moreover, the scalemeasures both acute and chronic clinical pain.However, the scale does artificially categorize theintensity of pain by forcing the patient to select asingle word on the scale. Because pain is so subjec-tive, the word selected may not reflect the patient'strue sensation. This is a problem for both clinicianand researcher, for anytime one tries to describe acontinuum by means of a limited number of points,specific information may be sacrificed for generalunderstanding.
Figure 2A verbal descriptor scaleVerbal Descriptor Scales (VDS) measure pain intensity,a major component of the sensory/discriminativedimension of pain. They usually consist of three to fivenumerically ranked words:
1 None2 Mild3 Moderate4 Severe5 Unbearable
(Reprinted with permission from McGuire DB. Page 337.8)
Unidimensional instrument: Visual analoguescale
The visual analogue scale (VAS) is widely usedby anesthesia providers when assessing the inten-sity of acute pain in clinical research. The VASconsists of a straight line, either vertical or hori-zontal, with verbal anchors at either end, repre-senting a continuum of pain intensity. One end ofthe line has the anchor "no pain, " while the otherend of the line has the anchor "pain as bad as itcould possibly be." The length of the line can varybut is often 10 cm (Figure 3). The patient is askedto make a single mark on the line indicating his orher present level of pain. The distance from the
135
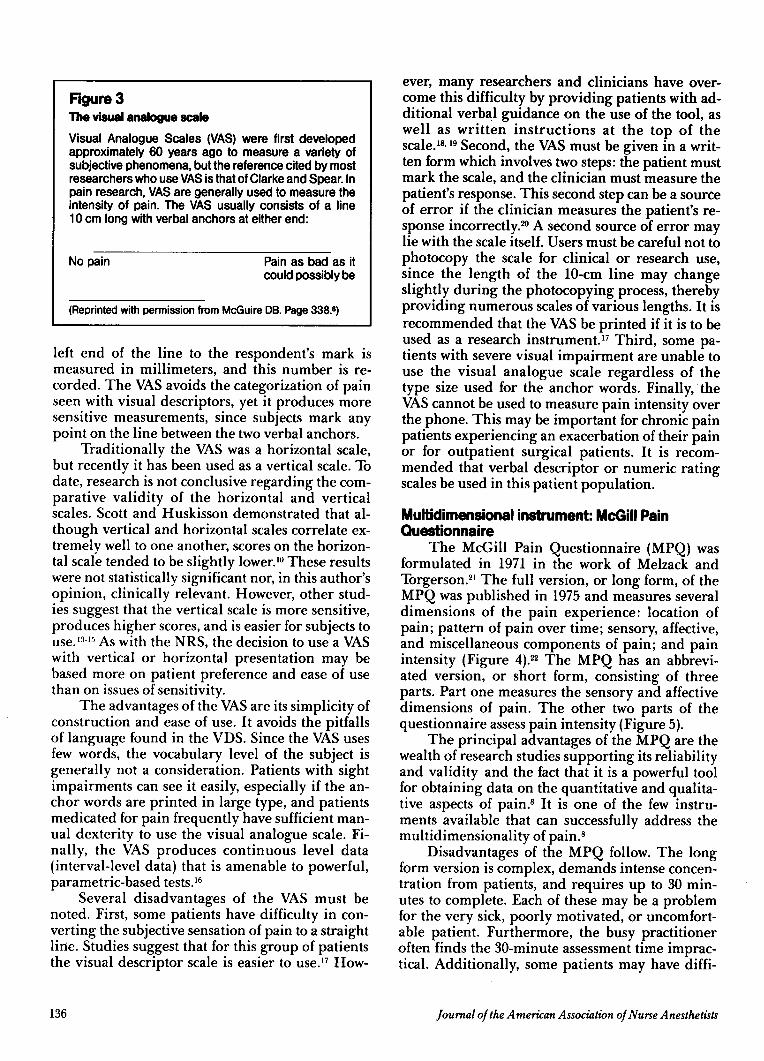
Figure 3The visual analogue scaleVisual Analogue Scales (VAS) were first developedapproximately 60 years ago to measure a variety ofsubjective phenomena, but the reference cited by mostresearchers who use VAS is that of Clarke and Spear. Inpain research, VAS are generally used to measure theintensity of pain. The VAS usually consists of a line10 cm long with verbal anchors at either end:
No pain Pain as bad as itcould possibly be
(Reprinted with permission from McGuire DB. Page 338.8)
left end of the line to the respondent's mark ismeasured in millimeters, and this number is re-corded. The VAS avoids the categorization of painseen with visual descriptors, yet it produces moresensitive measurements, since subjects mark anypoint on the line between the two verbal anchors.
Traditionally the VAS was a horizontal scale,but recently it has been used as a vertical scale. Todate, research is not conclusive regarding the com-parative validity of the horizontal and verticalscales. Scott and Huskisson demonstrated that al-though vertical and horizontal scales correlate ex-tremely well to one another, scores on the horizon-tal scale tended to be slightly lower.'0 These resultswere not statistically significant nor, in this author'sopinion, clinically relevant. However, other stud-ies suggest that the vertical scale is more sensitive,produces higher scores, and is easier for subjects touse. 13"- 1 As with the NRS, the decision to use a VASwith vertical or horizontal presentation may bebased more on patient preference and ease of usethan on issues of sensitivity.
The advantages of the VAS are its simplicity ofconstruction and ease of use. It avoids the pitfallsof language found in the VDS. Since the VAS usesfew words, the vocabulary level of the subject isgenerally not a consideration. Patients with sightimpairments can see it easily, especially if the an-chor words are printed in large type, and patientsmedicated for pain frequently have sufficient man-ual dexterity to use the visual analogue scale. Fi-nally, the VAS produces continuous level data(interval-level data) that is amenable to powerful,parametric-based tests.' 6
Several disadvantages of the VAS must benoted. First, some patients have difficulty in con-verting the subjective sensation of pain to a straightline. Studies suggest that for this group of patientsthe visual descriptor scale is easier to use. 17 How-
136
ever, many researchers and clinicians have over-come this difficulty by providing patients with ad-ditional verbal guidance on the use of the tool, aswell as written instructions at the top of thescale.',19 Second, the VAS must be given in a writ-ten form which involves two steps: the patient mustmark the scale, and the clinician must measure thepatient's response. This second step can be a sourceof error if the clinician measures the patient's re-sponse incorrectly.20 A second source of error maylie with the scale itself. Users must be careful not tophotocopy the scale for clinical or research use,since the length of the 10-cm line may changeslightly during the photocopying process, therebyproviding numerous scales of various lengths. It isrecommended that the VAS be printed if it is to beused as a research instrument. 17 Third, some pa-tients with severe visual impairment are unable touse the visual analogue scale regardless of thetype size used for the anchor words. Finally, theVAS cannot be used to measure pain intensity overthe phone. This may be important for chronic painpatients experiencing an exacerbation of their painor for outpatient surgical patients. It is recom-mended that verbal descriptor or numeric ratingscales be used in this patient population.
Multidimensional instrument: McGill PainQuestionnaire
The McGill Pain Questionnaire (MPQ) wasformulated in 1971 in the work of Melzack andTorgerson. 21 The full version, or long form, of theMPQ was published in 1975 and measures severaldimensions of the pain experience: location ofpain; pattern of pain over time; sensory, affective,and miscellaneous components of pain; and painintensity (Figure 4). 22 The MPQ has an abbrevi-ated version, or short form, consisting of threeparts. Part one measures the sensory and affectivedimensions of pain. The other two parts of thequestionnaire assess pain intensity (Figure 5).
The principal advantages of the MPQ are thewealth of research studies supporting its reliabilityand validity and the fact that it is a powerful toolfor obtaining data on the quantitative and qualita-tive aspects of pain.8 It is one of the few instru-ments available that can successfully address themultidimensionality of pain. 8
Disadvantages of the MPQ follow. The longform version is complex, demands intense concen-tration from patients, and requires up to 30 min-utes to complete. Each of these may be a problemfor the very sick, poorly motivated, or uncomfort-able patient. Furthermore, the busy practitioneroften finds the 30-minute assessment time imprac-tical. Additionally, some patients may have diffi-
Journal of the American Association of Nurse Anesthetists
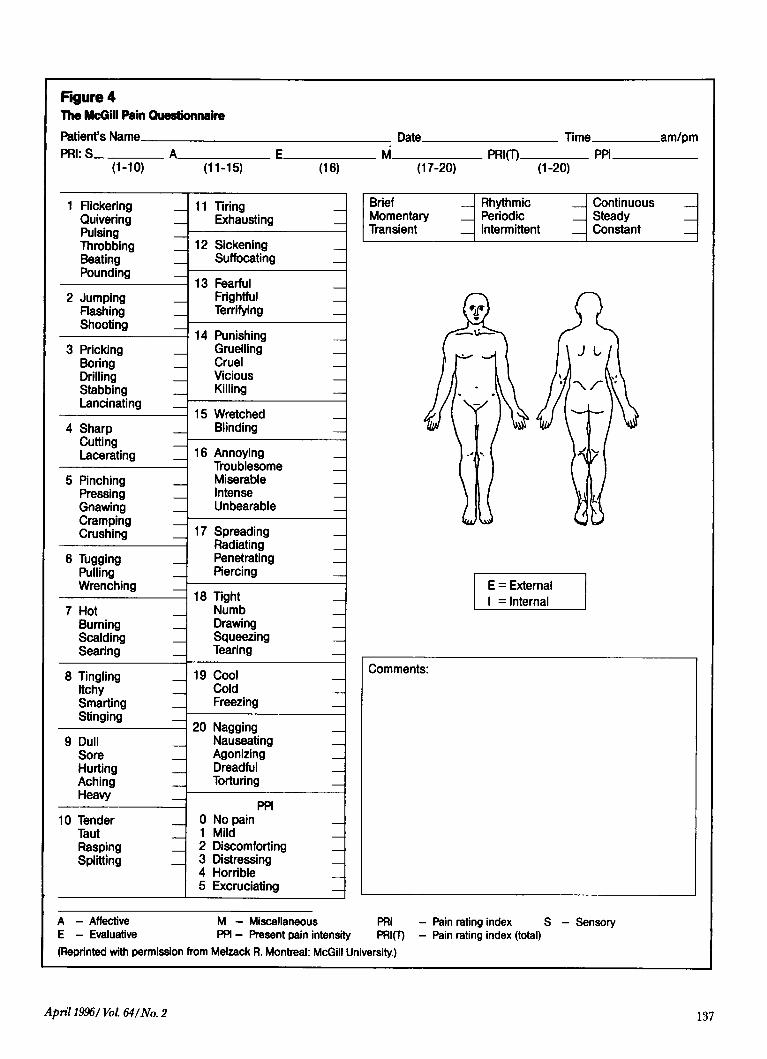
Figure 4The McGill Pain QuestionnairePatient's NamePRI: S
(1-10)
DateA_ E
(11-15) (16)M
(17-20)
Time am/pmPRI(T) PPI
(1-20)
1 FlickeringQuiveringPulsingThrobbingBeatingPounding
2 JumpingFlashingShooting
3 PrickingBoring _DrillingStabbingLancinating
4 SharpCuttingLacerating
5 PinchingPressingGnawingCrampingCrushing
6 TuggingPullingWrenching
7 HotBurningScaldingSearing
8 TinglingItchySmartingStinging
9 DullSoreHurtingAchingHeavy
10 TenderTautRaspingSplitting
11 TiringExhausting _
12 SickeningSuffocating
13 FearfulFrightfulTerrifying
14 PunishingGruellingCruelViciousKilling
15 WretchedBlinding
16 AnnoyingTroublesomeMiserableIntenseUnbearable
17 SpreadingRadiatingPenetratingPiercing
18 TightNumbDrawingSqueezingTearing
19 CoolColdFreezing
20 NaggingNauseatingAgonizingDreadfulTorturing
PPI0 No pain1 Mild2 Discomforting3 Distressing4 Horrible5 Excruciating
Brief _ Rhythmic _ ContinuousMomentary _ Periodic _ SteadyTransient Intermittent Constant
E = ExternalI = Internal
A - Affective M - Miscellaneous PRIE - Evaluative PPI - Present pain intensity PRI(T
(Reprinted with permission from Melzack R. Montreal: McGill University.)
- Pain rating index) - Pain rating index (total)
April 1996/1Vol 64/No. 2
Comments:
S - Sensory
I
137
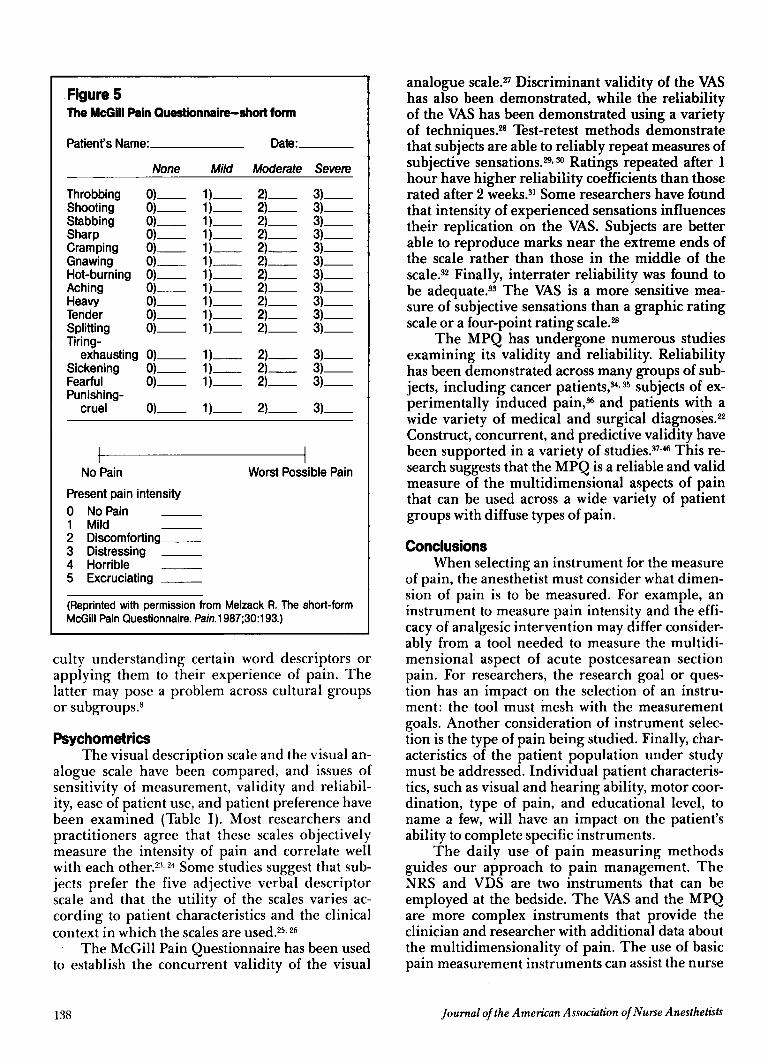
Figure 5The McGill Pain Questionnaire-short form
Patient's Name: Date:
None Mild Moderate Severe
Throbbing 0) 1) 2) 3)Shooting 0) 1) 2) 3)Stabbing 0) 1) 2) 3)Sharp 0) 1) 2) 3)Cramping 0) 1) 2) 3)Gnawing 0) 1) 2) 3)Hot-burning 0) 1) 2) 3)Aching 0) 1) 2) 3)Heavy 0) 1) 2) 3)Tender 0) 1) 2) 3)Splitting 0) 1) 2) 3)Tiring-
exhausting 0) 1) 2) 3)Sickening 0) 1) 2) 3)Fearful 0) 1) 2) 3)Punishing-
cruel 0) 1) 2) 3)
No Pain Worst Possible PainPresent pain intensity0 No Pain _1 Mild2 Discomforting3 Distressing4 Horrible5 Excruciating
(Reprinted with permission from Melzack R. The short-formMcGill Pain Questionnaire. Pain. 1987;30:193.)
culty understanding certain word descriptors orapplying them to their experience of pain. Thelatter may pose a problem across cultural groupsor subgroups.8
PsychometricsThe visual description scale and the visual an-
alogue scale have been compared, and issues ofsensitivity of measurement, validity and reliabil-ity, ease of patient use, and patient preference havebeen examined (Table I). Most researchers andpractitioners agree that these scales objectivelymeasure the intensity of pain and correlate wellwith each other.23, 24 Some studies suggest that sub-jects prefer the five adjective verbal descriptorscale and that the utility of the scales varies ac-cording to patient characteristics and the clinicalcontext in which the scales are used.25, 26
The McGill Pain Questionnaire has been usedto establish the concurrent validity of the visual
138
analogue scale.2 Discriminant validity of the VAShas also been demonstrated, while the reliabilityof the VAS has been demonstrated using a varietyof techniques.28 Test-retest methods demonstratethat subjects are able to reliably repeat measures ofsubjective sensations. 29' 3° Ratings repeated after 1hour have higher reliability coefficients than thoserated after 2 weeks.31 Some researchers have foundthat intensity of experienced sensations influencestheir replication on the VAS. Subjects are betterable to reproduce marks near the extreme ends ofthe scale rather than those in the middle of thescale.32 Finally, interrater reliability was found tobe adequate.33 The VAS is a more sensitive mea-sure of subjective sensations than a graphic ratingscale or a four-point rating scale.28
The MPQ has undergone numerous studiesexamining its validity and reliability. Reliabilityhas been demonstrated across many groups of sub-jects, including cancer patients, 34,35 subjects of ex-perimentally induced pain,36 and patients with awide variety of medical and surgical diagnoses. 2
Construct, concurrent, and predictive validity havebeen supported in a variety of studies.37- 6 This re-search suggests that the MPQ is a reliable and validmeasure of the multidimensional aspects of painthat can be used across a wide variety of patientgroups with diffuse types of pain.
ConclusionsWhen selecting an instrument for the measure
of pain, the anesthetist must consider what dimen-sion of pain is to be measured. For example, aninstrument to measure pain intensity and the effi-cacy of analgesic intervention may differ consider-ably from a tool needed to measure the multidi-mensional aspect of acute postcesarean sectionpain. For researchers, the research goal or ques-tion has an impact on the selection of an instru-ment: the tool must mesh with the measurementgoals. Another consideration of instrument selec-tion is the type of pain being studied. Finally, char-acteristics of the patient population under studymust be addressed. Individual patient characteris-tics, such as visual and hearing ability, motor coor-dination, type of pain, and educational level, toname a few, will have an impact on the patient'sability to complete specific instruments.
The daily use of pain measuring methodsguides our approach to pain management. TheNRS and VDS are two instruments that can beemployed at the bedside. The VAS and the MPQare more complex instruments that provide theclinician and researcher with additional data aboutthe multidimensionality of pain. The use of basicpain measurement instruments can assist the nurse
Journal of the American Association of Nurse Anesthetists
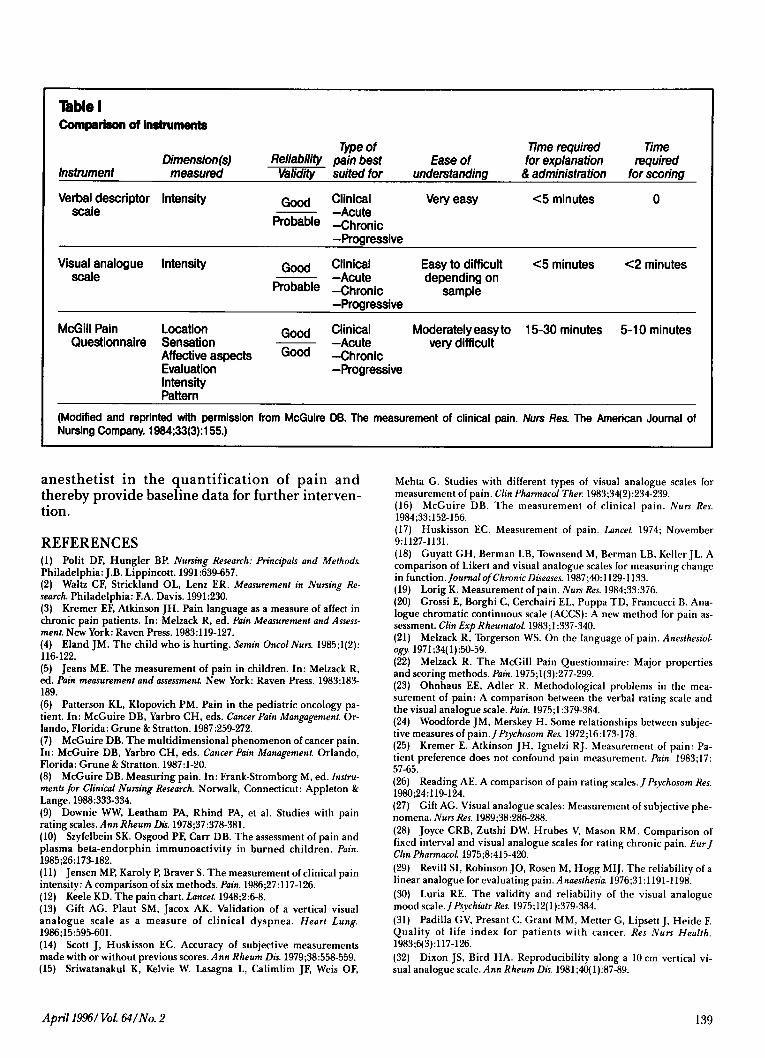
Table IComparison of instruments
Type ofReliability pain best Ease of
Time requiredfor explanation
Timerequired
Instrument measured Validity suited for understanding & administration for scoring
Verbal descriptor Intensity Good Clinical Very easy <5 minutes 0scale -Acute
Probable -Chronic-Progressive
Visual analogue Intensity Good Clinical Easy to difficult <5 minutes <2 minutesscale -Acute depending on
Probable -Chronic sample-Progressive
McGill Pain Location Good Clinical Moderately easy to 15-30 minutes 5-10 minutesQuestionnaire Sensation -Acute very difficult
Affective aspects Good -ChronicEvaluation -ProgressiveIntensityPattern
(Modified and reprinted with permission from McGuire DB. The measurement of clinical pain. Nurs Res. The American Journal ofNursing Company. 1984;33(3):155.)
anesthetist in the quantification of pain andthereby provide baseline data for further interven-tion.
REFERENCES(1) Polit DF, Hungler BP. Nursing Research: Principals and Methods.Philadelphia: J.B. Lippincott. 1991:639-657.(2) Waltz CF, Strickland OL, Lenz ER. Measurement in Nursing Re-search. Philadelphia: F.A. Davis. 1991:230.(3) Kremer EF, Atkinson JH. Pain language as a measure of affect inchronic pain patients. In: Melzack R, ed. Pain Measurement and Assess-ment. New York: Raven Press. 1983:119-127.(4) Eland JM. The child who is hurting. Semin Oncol Nurs. 1985;1(2):116-122.(5) Jeans ME. The measurement of pain in children. In: Melzack R,ed. Pain measurement and assessment. New York: Raven Press. 1983:183-189.(6) Patterson KL, Klopovich PM. Pain in the pediatric oncology pa-tient. In: McGuire DB, Yarbro CH, eds. Cancer Pain Mangagement. Or-lando, Florida: Grune & Stratton. 1987:259-272.(7) McGuire DB. The multidimensional phenomenon of cancer pain.In: McGuire DB, Yarbro CH, eds. Cancer Pain Management. Orlando,Florida: Grune & Stratton. 1987:1-20.(8) McGuire DB. Measuring pain. In: Frank-Stromborg M, ed. Instru-ments for Clinical Nursing Research. Norwalk, Connecticut: Appleton &Lange. 1988:333-334.(9) Downie WW, Leatham PA, Rhind PA, et al. Studies with painrating scales. Ann Rheum Dis. 1978;37:378-381.(10) Szyfelbein SK. Osgood PF, Carr DB. The assessment of pain andplasma beta-endorphin immunoactivity in burned children. Pain.1985;26:173-182.(11) Jensen MP, Karoly P, Braver S. The measurement of clinical painintensity: A comparison of six methods. Pain. 1986;27:117-126.(12) Keele KD. The pain chart. Lancet. 1948;2:6-8.(13) Gift AG, Plaut SM, Jacox AK. Validation of a vertical visualanalogue scale as a measure of clinical dyspnea. Heart Lung.1986;15:595-601.(14) Scott J, Huskisson EC. Accuracy of subjective measurementsmade with or without previous scores. Ann Rheum Dis. 1979;38:558-559.(15) Sriwatanakul K, Kelvie W. Lasagna L, Calimlim JF, Weis OF,
Mehta G. Studies with different types of visual analogue scales formeasurement of pain. Clin Pharmacol Ther. 1983;34(2):234-239.(16) McGuire DB. The measurement of clinical pain. Nurs Res.1984;33;152-156.(17) Huskisson EC. Measurement of pain. Lancet. 1974; November9:1127-1131.(18) Guyatt GH, Berman LB, Townsend M, Berman LB, Keller JL. Acomparison of Likert and visual analogue scales for measuring changein function. Journal ofChronic Diseases. 1987;40:1129-1133.(19) Lorig K. Measurement of pain. Nurs Res. 1984;33:376.(20) Grossi E, Borghi C, Cerchairi EL, Puppa TD, Francucci B. Ana-logue chromatic continuous scale (ACCS): A new method for pain as-sessment. Clin Exp Rheumatol. 1983;1:337-340.(21) Melzack R, Torgerson WS. On the language of pain. Anesthesiol-ogy. 1971;34(1):50-59.(22) Melzack R. The McGill Pain Questionnaire: Major propertiesand scoring methods. Pain. 1975;1(3):277-299.(23) Ohnhaus EE, Adler R. Methodological problems in the mea-surement of pain: A comparison between the verbal rating scale andthe visual analogue scale. Pain. 1975;1:379-384.(24) Woodforde JM, Merskey H. Some relationships between subjec-tive measures of pain. Psychosom Res. 1972;16:173-178.(25) Kremer E. Atkinson JH, Ignelzi RJ. Measurement of pain: Pa-tient preference does not confound pain measurement. Pain. 1983;17:57-65.(26) Reading AE. A comparison of pain rating scales. JPsychosom Res.1980;24:119-124.(27) Gift AG. Visual analogue scales: Measurement of subjective phe-nomena. Nurs Res. 1989;38:286-288.(28) Joyce CRB, Zutshi DW. Hrubes V, Mason RM. Comparison offixed interval and visual analogue scales for rating chronic pain. EurJClin Pharmacol. 1975;8:415-420.(29) Revill SI, Robinson JO, Rosen M, Hogg MIJ. The reliability of alinear analogue for evaluating pain. Anaesthesia. 1976;31:1191-1198.(30) Luria RE. The validity and reliability of the visual analoguemood scale.JPsychiatr Res. 1975;12(1):379-384.(31) Padilla GV, Presant C, Grant MM, Metter G, Lipsett J, Heide FQuality of life index for patients with cancer. Res Nurs Health.1983;6(3):117-126.(32) Dixon JS, Bird HA. Reproducibility along a 10 cm vertical vi-sual analogue scale. Ann Rheum Dis. 1981;40(1):87-89.
April 1996/ Vol. 64/No. 2
Dimension(s)
139

(33) Litte JC, McPhail NI. Measures of depressive mood at monthlyintervals. Br] Psychiatry. 1973;122:447-452.(34) Graham C, Bond SS, Gerkovich MM, et al. Use of the McGillPain Questionnaire in the assessment of cancer pain: Replicability andconsistency. Pain. 1980;8(3):377-387.(35) McGuire DB. Assessment of pain in cancer inpatients using theMcGill Pain Questionnaire. Oncol Nurs Forum. 1984;11(6):32-37.(36) Klepac RK, Dowling J, Rokke P, et al. Interview vs. paper andpencil administration of the McGill Pain Questionnaire. Pain.1981;11:241-246.(37) Byrne M, Troy A, Bradley LA, et al. Cross-validation of thefactor structures of the McGill Pain Questionnaire. Pain. 1982;13:193-202.(38) Prieto EJ, Hopson L, Bradley LA, et al. The language of lowback pain: Factor structure of the McGill Pain Questionnaire. Pain.1980;8:11-19.(39) Reading AE. The internal structure of the McGill Pain Ques-tionnaire in dysmenorrhea patients. Pain. 1979;7:353-358.(40) Kremer E, Atkinson JH. Pain measurement: Construct validityof the affective dimension of the McGill Pain Questionnaire withchronic benign pain patients. Pain. 1981;11:93-100.(41) Burckhardt CS. The use of the McGill Pain Questionnaire inassessing arthritis pain. Pain. 1984;19:305-314.(42) Prieto EJ, Geisinger KF. Factor-analytic studies of the McGillPain Questionnaire. In: Melzack R, ed. Pain Measurement and Assess-ment. New York: Raven Press. 1983;63-70.(43) Buren JV, Kleinknecht RA. An evaluation of the McGill Pain
Questionnaire for use in dental pain assessment. Pain. 1979;6:23-33.(44) Klepac RK, Dowling J, Gauge G, et al. Sensitivity of the McGillPain Questionnaire to intensity and quality of laboratory pain. Pain.1981;10:199-207.(45) Hunter M, Philips C. The experience of headache-An assess-ment of the qualities of tension headache pain. Pain. 1981;10:209-219.(46) Reading AE. The McGill Pain Questionnaire: An appraisal. In:Melzack R, ed. Pain Measurement and Assessment. New York: RavenPress. 1983:55-61.
AUTHORStephen A. Flaherty, CRNA, MS, is a graduate of the Anesthesia
Nurse Practitioner Program, Rush University, Chicago, Illinois. Hecurrently practices at Rush-Presbyterian-St. Luke's Medical Center inChicago. Active at both the state and national level, Mr. Flaherty serveson the Illinois Association of Nurse Anesthetists Board of Directorsand has served on the AANA Practice Committee (1993-1994 and1994-1995). In addition to clinical and didactic teaching assignments inthe Nurse Anesthesia Program at Rush, Mr. Flaherty is also a doctoralcandidate in the Rush University College of Nursing.
ACKNOWLEDGMENTSThe author would like to thank Judith Paice, RN, PhD, and Mark
Lindhorst for their advice and support in preparation of thismanuscript.
Journal of the American Association of Nurse Anesthetists140
-
INTRODUCING ULTANETM (SEVOFUlRAN
AN IDEAL PROFILE
^-INHALATION ANEST
FASTER ADJUSTMENT OF ANESTHETIC DEPTH
Provides lower solubility than isoflurane orhalothane, for more rapid uptake, elimination,and adjustment of anesthetic depth 1, 2
HEMODYNAMICALLY STABLE
No changes in heart rate at doses up to 2.0 MAC 3-5
BETTER RECOVERY PROFILE
IN MOST RECOVERY EVENTS
More rapid attainment of most recovery parametersthan isoflurane and halothane 3, 6,7
Please see brief summary of Prescribing Information on the last page of this advertisement.
I
~'-,u1
NEW for Inhalation Anesthesia
YIULTANE.sevoflurane
Rapid Recovery, Predictable Control
REFERENCES
1. Yasuda N, Lockhart SH, Eger El, et al. Comparison of kinetics of sevoflurane and isoflurane in humans. Anesth Analg. 1991;72:316-324.
2. Eger El II. New inhaled anesthetics. Anesthesiology. 1994;80:906-922.
3. Data on file, Abbott Laboratories.
4. Ebert TJ, Muzi M, Lopatka CW. Effects of sevoflurane on hemodynamics and sympathetic neural activity in humans: a comparison to isoflurane.Anesthesiology. 1994;81:A133.
5. Malan TP Jr, DiNardo JA, Frink EJ Jr, Isner RJ, Brown EA. Cardiovascular effects of sevoflurane and isoflurane in volunteers. Anesthesiology.1994;81:A131.
6. Binstock WB, Berkowitz R, Eyrich K, Hannallah RS, Apfelbaum JL. A comparison of sevoflurane and halothane for induction and maintenance ofanesthesia in pediatric ASA I and II outpatients. Anesthesiology. 1994;81:A1313.
7. Loeb R, Wetchler BV, Schacher D, Gross J. Comparison of sevoflurane and isoflurane for anesthesia on adult outpatients. Anesthesiology.1994;81:A3.
a ULTANE.se v o fl u r a n e volatile liquid for inhalation
INDICATIONS AND USAGESevoflurane is indicated for induction and maintenance of general
anesthesia in adult and pediatric patients for inpatient and outpatientsurgery.CONTRAINDICATIONS
Sevoflurane can cause malignant hyperthermia; it should not beused in patients with known history of sensitivity to sevoflurane or toother halogenated agents.WARNINGS
Sevoflurane should be administered only by persons trained in theadministration of general anesthesia. Facilities for maintenance of apatent airway, artificial ventilation, oxygen enrichment, and circula-tory resuscitation must be immediately available. Since levels ofanesthesia may be altered rapidly, only vaporizers producingpredictable concentrations of sevoflurane should be used.
Compound A is produced when sevoflurane interacts with soda limeand Baralyme® (See DESCRIPTION). Its concentration in a circle ab-sorber system increases with increasing absorber temperature andincreasing sevoflurane concentrations and with decreasing fresh gasflow rates. Although Compound A is a dose-dependent nephrotoxin inrats, the mechanism of this renal toxicity is unknown and has not beenestablished in humans. Because of limited clinical experience withsevoflurane in low-flow systems, fresh gas flow rates below2 L/min in a circle absorber system are not recommended.
Because clinical experience in administering sevoflurane to patientswith renal insufficiency (creatinine >1.5 mg/dL) is limited, its safety inthese patients has not been established.
Malignant HyperthennrmiaIn susceptible individuals, potent inhalation anesthetic agents, in-
cluding sevoflurane, may trigger a skeletal muscle hypermetabolicstate leading to high oxygen demand and the clinical syndromeknown as malignant hyperthermia. In clinical trials, one case of ma-lignant hyperthermia was reported. In genetically susceptible pigs,sevoflurane induced malignant hyperthermia. The clinical syndromeis signaled by hypercapnia, and may include muscle rigidity, tachy-cardia, tachypnea, cyanosis, arrhythmias, and/or unstable bloodpressure. Some of these nonspecific signs may also appear duringlight anesthesia, acute hypoxia, hypercapnia, and hypovolemia.
Treatment of malignant hyperthermia includes discontinuation oftriggering agents, administration of intravenous dantrolene sodium,and application of supportive therapy. (Consult prescribing informa-tion for dantrolene sodium intravenous for additional information onpatient management.) Renal failure may appear later, and urine flowshould be monitored and sustained if possible.
Sevoflurane may present an increased risk in patients with knownsensitivity to volatile halogenated anesthetic agents.
PRECAUTIONSDuring the maintenance of anesthesia, increasing the concentration
of sevoflurane produces dose-dependent decreases in blood pres-sure. Due to sevoflurane's insolubility in blood, these hemodynamicchanges may occur more rapidly than with other volatile anesthetics.Excessive decreases in blood pressure or respiratory depression maybe related to depth of anesthesia and may be corrected by decreasingthe inspired concentration of sevoflurane.
The recovery from general anesthesia should be assessed carefullybefore a patient is discharged from the post-anesthesia care unit.
Drug InteractionsIn clinical trials, no significant adverse reactions occurred with
other drugs commonly used in the perioperative period, including:central nervous system depressants, autonomic drugs, skeletalmuscle relaxants, anti-infective agents, hormones and syntheticsubstitutes, blood derivatives, and cardiovascular drugs.
Intravenous Anesthetics:Sevoflurane administration is compatible with barbiturates, propofol,
and other commonly used intravenous anesthetics.
Benzodiazepines and Oioids:Benzodiazepines and opioids would be expected to decrease the
MAC of sevoflurane in the same manner as with other inhalationalanesthetics. Sevoflurane administration is compatible with benzodi-azepines and opioids as commonly used in surgical practice.
Nitrous Oxide:As with other halogenated volatile anesthetics, the anesthetic re-
quirement for sevoflurane is decreased when administered incombination with nitrous oxide. Using 50% N20, the MAC equivalentdose requirement is reduced approximately 50% in adults, and ap-proximately 25% in pediatric patients (see DOSAGE ANDADMINISTRATION).
Neuromuscular Blocking Agents:As is the case with other volatile anesthetics, sevoflurane increases
both the intensity and duration of neuromuscular blockade induced bynondepolarizing muscle relaxants. When used to supplement alfen-tanil-N20 anesthesia, sevoflurane and isoflurane equally potentiateneuromuscular block induced with pancuronium, vecuronium oratracurium. Therefore, during sevoflurane anesthesia, the dosage ad-justments for these muscle relaxants are similar to those requiredwith isoflurane.
Potentiation of neuromuscular blocking agents requires equilibra-tion of muscle with delivered partial pressure of sevoflurane.Reduced doses of neuromuscular blocking agents during induction ofanesthesia may result in delayed onset of conditions suitable for en-dotracheal intubation or inadequate muscle relaxation.
Among available nondepolarizing agents, only vecuronium,pancuronium and atracurium interactions have been studied duringsevoflurane anesthesia. In the absence of specific guidelines:
1. For endotracheal intubation, do not reduce the dose of nondepo-larizing muscle relaxants.
2. During maintenance of anesthesia, the required dose ofnondepolarizing muscle relaxants is likely to be reducedcompared to that during N20/opioid anesthesia. Administrationof supplemental doses of muscle relaxants should be guided bythe response to nerve stimulation.
The effect of sevoflurane on the duration of depolarizing neuromus-cular blockade induced by succinylcholine has not been studied.
Renal or Hepatic FunctionResults of evaluations of laboratory parameters (e.g., ALT, AST, al-
kaline phosphatase, and total bilirubin, etc.), as well as investigatorreported incidence of adverse events relating to liver function,demonstrate that sevoflurane can be administered to patients withnormal or mild-to-moderately impaired hepatic function. However,patients with severe hepatic dysfunction were not investigated.
Occasional cases of transient changes in postoperative hepaticfunction tests were reported with both sevoflurane and referenceagents. Sevoflurane was found to be comparable to isoflurane withregard to these changes in hepatic function.
Based on the incidence and magnitude of changes in serum creati-nine, in patients with exposure up to 9.6 MAC-hours of anesthesia,no evidence for increased risk of developing renal dysfunction wasfound.
Serum fluoride levels increased with duration and concentration ofexposure to sevoflurane. The highest measured serum fluoride levelwas 111 pM and a level of 29.5 pM was seen as late as 92 hours postexposure. A 25% reduction in maximum urine-concentrating abilityhas been seen following enflurane anesthesia with mean peak seruminorganic fluoride levels of 33.6 pM and values above 20 pM for 18hours. Elevated fluoride levels after sevoflurane were not associatedwith impairment of renal function, presumably because of its rapidelimination at the end of anesthesia.
Carcinogenesis, Mutagenesis, Impairment of FertilityStudies on carcinogenesis have not been performed. No mutagenic
effect was noted in the Ames test and no chromosomal aberrationswere induced in cultured mammalian cells.
Pregnancy Category B: Reproduction studies have been performed inrats and rabbits at doses up to 1 MAC (minimum alveolar concentra-tion) without CO2 absorbent and have revealed no evidence of im-paired fertility or harm to the fetus due to sevoflurane at 0.3 MAC, thehighest nontoxic dose. Developmental and reproductive toxicity stud-ies of sevoflurane in animals in the presence of strong alkalies (i.e.,degradation of sevoflurane and production of Compound A) have notbeen conducted. There are no adequate and well-controlledstudies in pregnant women. Because animal reproduction studies arenot always predictive of human response, sevoflurane should be usedduring pregnancy only if clearly needed.
Labor and Delivery: Sevoflurane has been used as part of generalanesthesia for elective cesarean section in 29 women. There were nountoward effects in mother or neonate. (See CLINICAL PHARMACOL-OGY, Clinical Trials.) The safety of sevoflurane in labor and deliveryhas not been demonstrated.
Nursing Mothers: The concentrations of sevoflurane in milk areprobably of no clinical importance 24 hours after anesthesia. Becauseof rapid washout, sevoflurane concentrations in milk are predicted tobe below those found with many other volatile anesthetics.
Geriatric Use: MAC decreases with increasing age. The averageconcentration of sevoflurane to achieve MAC in an 80 year old is ap-proximately 50% of that required in a 20 year old.
ADVERSE REACTIONSAdverse events are derived from controlled clinical trials conducted
in the United States, Canada, and Europe. The reference drugs wereisoflurane, enflurane, and propofol in adults and halothane in pediatricpatients. The studies were conducted using a variety of premedica-tions, other anesthetics, and surgical procedures of varying length.Most adverse events reported were mild and transient, and may re-flect the surgical procedures, patient characteristics (includingdisease) and/or medications administered.
Of the 5182 patients enrolled in the clinical trials, 2906 were exposedto sevoflurane, including 118 adults and 507 pediatric patients who un-derwent mask induction. Each patient was counted once for eachtype of adverse event. Adverse events reported in patients in clinicaltrials and considered to be possibly or probably related to sevofluraneare presented within each body system in order of decreasing fre-quency in the following listings. One case of malignant hyperthermiawas reported in pre-registration clinical trials.
Adverse Events During the Induction Period (from onset of anesthesiaby mask induction to surgical incision) Incidence >1%
Adult Patients (N = 118)Cardiovascular: Bradycardia 5%, Hypotension 4%, Tachycardia 2%Nervous System: Agitation 7%Respiratory System: Laryngospasm 8%, Airway obstruction 8%,
Breathholding 5%, Cough Increased 5%
Pediatric Patients (N = 507)Cardiovascular: Tachycardia 6%, Hypotension 4%Nervous System: Agitation 15%Respiratory System: Breathholding 5%, Cough Increased 5%,Laryngospasm 3%, Apnea 2%Digestive System: Increased salivation 2%
Adverse Events During Maintenance and Emergence Periods,Incidence >1% (N = 2906)
Body as a whole: Fever 1%, Shivering 6%, Hypothermia 1%,Movement 1%, Headache 1%Cardiovascular: Hypotension 11%, Hypertension 2%,Bradycardia 5%, Tachycardia 2%Nervous System: Somnolence 9%, Agitation 9%, Dizziness 4%,Increased salivation 4%
Digestive System: Nausea 25%, Vomiting 18%Respiratory System: Cough increased 11%, Breathholding 2%,Laryngospasm 2%
Adverse Events, All Patients in Clinical Trials (N =2906), AllAnesthetic Periods, Incidence < 1% (reported in 3 or more patients)
Body as a whole: Asthenia, PainCardiovascular Arrhythmia, Ventricular Extrasystoles, Supravdntri-cular Extrasystoles, Complete AV Block, Bigeminy, Hemorrhage,Inverted T Wave, Atrial Fibrillation, Atrial Arrhythmia, SecondDegree AV Block, Syncope, S-T DepressedNervous System: Crying, Nervousness, Confusion, Hypertonia, DryMouth, InsomniaRespiratory System: Sputum Increased, Apnea, Hypoxia, Wheezing,Bronchospasm, Hyperventilation, Pharyngitis, Hiccup, Hypoventila-tion, Dyspnea, StridorMetabolism and Nutrition: Increases in LDH, AST, ALT, BUN,Alkaline Phosphatase, Creatinine, Bilirubinemia, Glycosuria,Fluorosis, Albuminuria, Hypophosphatemia, Acidosis, HyperglycemiaHemic and Lymphatic System: Leucocytosis, ThrombocytopeniaSkin and Special Senses: Amblyopia, Pruritus, Taste Perversion,Rash, ConjunctivitisUrogenital: Urination Impaired, Urine Abnormality, Urinary Retention,OliguriaSee WARNINGS for information regarding malignant hyperthermia.Laboratory Findings: Transient elevations in glucose, liver function
tests, and white blood cell count may occur as with use of otheranesthetic agents.
OVERDOSAGEIn the event of overdosage, or what may appear to be overdosage,
the following action should be taken: discontinue administration ofsevoflurane, maintain a patent airway, initiate assisted or controlledventilation with oxygen, and maintain adequate cardiovascularfunction.
DOSAGE AND ADMINISTRATIONThe concentration of sevoflurane being delivered from a vaporizer
during anesthesia should be known. This may be accomplished byusing a vaporizer calibrated specifically for sevoflurane. The adminis-tration of general anesthesia must be individualized based on the pa-tient's response.
Pre-anesthetic Medication: No specific premedication is either in-dicated or contraindicated with sevoflurane. The decision as towhether or not to premedicate and the choice of premedication is leftto the discretion of the anesthesiologist.
Induction: Sevoflurane has a nonpungent odor and does not causerespiratory irritability; it is suitable for mask induction in pediatrics andadults.
Maintenance: Surgical levels of anesthesia can usually be achievedwith concentrations of 0.5 - 3% sevoflurane with or without theconcomitant use of nitrous oxide. Sevoflurane can be administeredwith any type of anesthesia circuit.
MAC Values For Adults And Pediatric Patients According To Age
Age of Patient Sevoflurane Sevoflurane in(years) in Oxygen 65% N20/35% 02
0-1 months # 3.3%1-<6 months 3.0%
6 months -<3 years 2.8% 2.0%@3-12 2.5%
25 2.6% 1.4%40 2.1% 1.1%60 1.7% 0.9%80 1.4% 0.7%
# Neonates are full-term gestational age. MAC in premature infantshas not been determined.
@ In 3- < 5 year old pediatric patients, 60% N20/40% 02 was used.
HOW SUPPUEDULTANE
TM (sevoflurane), Volatile Liquid for Inhalation, is packaged
in amber colored bottles containing 250 mL sevoflurane, List 4456,N D C#0074-4456-02.
SAFETY AND HANDLINGOccupational Caution
There is no specific work exposure limit established for sevoflurane.However, the National Institute for Occupational Safety and Healthhas recommended an 8 hour time-weighted average limit of 2 ppm forhalogenated anesthetic agents in general (0.5 ppm when coupled withexposure to N20).
STORAGEStore at controlled room temperature, 15° - 30°C (59" - 86°F).
Caution: Federal (USA) law prohibits dispensing without prescription.
Manufactured by: Abbott Laboratories, North Chicago, IL 60064, USAunder license from Maruishi Pharmaceutical Company LTD. 2-3-5,Fushimi-machi, Chuo-Ku, Osaka, Japan.
© Abbott 1994 Ref. 06-9230-R2-Rev. June, 1995 Printed in USAABBOTT LABORATORIES, NORTH CHICAGO, IL 60064, USA
95-3760-Jul., 95





























