Embed Size (px)
Citation preview

Pain Management in HPB tumor
A. Husni Tanra Hasanuddin University Faculty of Medicine
Anesthesiology Intensive Care and Pain Management Makassar
Presented in Makassar Hepatopancreaticobilliary surgery forum in Makassar October 26, 2019

Pain in Hepatobilliary Cancer
• 1.Parietal pain somatic nociceptive pain
• 2. Visceral pain from from organ surrounding the liver .
• 3. Bone metastase somatic nociceptive pain

PAIN MANAGEMENT
Before pain management we have to know:
1. Type of pain
2. Pain Assessment/Intensity of pain

Type of Pain
• 75 % of patients present mild to moderate abdominal and/or back pain in early stage ( visceral nociceptive pain)
• 80 % of patients with advanced stage will experience severe pain prior to death (invasion to the celiac plexus) severe neuropathic pain
• At the beginning oral (nonopioid + opioid transdermal)
may be helpful.
• But there is evidence that patients who undergo early
celiac plexus block experience improved QoL

Pain Assessment Pain assessment should be ongoing,
individualized, and documented.
Patients should be asked to describe their pain in terms of the following characteristics: location, radiation, mode of onset, character, temporal pattern, exacerbating and relieving factors, and intensity.
Should be measured along with temperature, pulse, blood pressure, and respiratory rate.

1.1 Visual Analog Scale (VAS)
/ No Pain
Worst Pain you can imagine
The VAS is most commonly a straight 100-mm line without demarcations. “no pain” at the left-most end and “worst pain” at the right-most end.

1.4. Numerical Rating Scale (NRS)
This is the current recommendation advice that pain intensity should be assessed on 11-point numerical rating scale (NRS) from 0 to 10. 0 indicates the absence of pain, while 10 represents the most intense pain It is designed to be used by those over the age of 9

Pedoman pengelolaan nyeri THREE STEP LADDER WHO, 1986
1
2
3
Severe pain
Moderate pain
Mild pain
World Health Organization. Cancer Pain Relief: With a Guide to Opioid Availability. World Health Organization; 1986.

Successive change
WHO method of cancer pain relief Three-step analgesic ladder
Strong opioids
Step III For moderate to severe pain,
Strong Opioid analgesics
± Non-opioid analgesics ± adjuvant analgesics
APAP/NSAIDs ± adjuvant analgesics
Step I Non-opioid analgesics
± adjuvant analgesics
APAP/NSAIDs ± adjuvant analgesics
For mild to moderate pain,
Mild Opioid analgesics
Codeine
Tramadol Tramadol+/APAP
Step II
± Non-opioid analgesics ± adjuvant analgesics
Pain
Pain
Pain
level
APAP (acetyl p aminophenol) =Acetaminophen=Paracetamol

Analgesics for cancer pain should be given1
By the mouth
By the clock
By the ladder
For the individual
With attention to detail
1.World Health Organization. Cancer Pain Relief: With a Guide to Opioid Availability. World Health Organization; 1996.

ANALGESIC DRUGS
NONOPIOIDS OPIOIDS ADJUVANTS
• Mild Opioid ( codeine & tramadol )
• Strong Opioid ( Morphine, Fetanyl,
oxycodon, hydromorphone )
• Paracetamol • NSAID (nonselective) • Coxib (selective NSAID)
• Steroid (dexamethason) • Antidepressant (tricyclic) • Gabapentinoid
(gabapentin& pregabaline) • Ketamine

Newly Proposed Analgesic Ladder
Nerve Block Epidurals
PCA pump Neurolytic block
Spinal stimulators Nonopioid
analgesics NSAIDs
Weak opioids
Strong opioids Methadone
Oral Administration
Transdermal Patch
Step 4
Step 3
Step 2
Step 1
NSAIDs (with or without adjuvants at each step) Chronic Pain Non Malignant Pain
Cancer Pain
Neurosurgical Procedures
Acute pain Chronic pain without control Acute crises of chronic pain

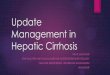
Pyramid of Pain Management in Cancer Pain
75-85%
10-15%
2-5%
1-5%
Nerve blocks
Epidural / intratechal
Intravenous
Interventions
Oral and Transdermal
Three Steps Ladder WHO Multimodal Analgesia

Rule of severe pain management
• Severe pain needs strong analgesic.
• Strong analgesic is Strong opioid .
1. Morphine Iv, tab IR MST continus tablet
2. Fentanyl iv, patch (transdermal) once in 3days
3. Hydromorphone tab once daily.
4. Oxycodone tab IR, CR. and iv.
available soon.
Strong opioid

Morphine is gold for opioid agonist
• “Natural opioid” and cheap
• “Gold standard” for cancer pain management.
• Widely available in multiple forms: oral pill and liquid, pills, parenteral
• Nausea, vomiting, obstipation.
• Histamine relies
• Hydrophilic

Apa yang dibutuhkan? Untuk mengtitrasi opioid pada nyeri
kanker?
Morphine rapid release
Liquid (syrup) or
Tablet
Untuk mengtitrasi opioid untuk mencapai dosis base line analgesia diperlukan opioid rapid release tab atau syrup.yg belum tersedia merata di indonesia..

Di Indonesia yang tersedia banyak adalah opiod kerja lama u maitanance
1. Morphine MST continue tablet
2. Fentanyl patch (transdermal) once in 3days
3. Hydromorphone tab Once daily.
2. Oxycodone Controled Release (single dose q/24 h and
multiple dose q/12 h)
Available Strong long acting opioid in Indonesia

1. Morphine Slow release (MST) has been used for 20 years
Twice a day

2. Fentany Patch
Once in 3 days ( Every 72 hours)

2. Fentanyl patch • Routes of Administration * Transdermal * Optimal action 18 hour • Duration of action 72 hours.
• Note! 1. Should not be used in naïve opioid (morphine)
patients. 2. Only for cancer pain patiens .

3.Hydromorphone Retard tablet
Once a day

4. Oxycodone tab Controlled Release q /12 h
Twice a day

Because cancer Pain is not 1 entity, it’s more complex and multifactorial in
nature.

Paracetamol
adjuvants
Weak Opioid for
mild to moderate
pain
Paracetamol
adjuvants
Strong Opioid for
severe pain
(Morphine)
Celecoxib
adjuvants
Increasing pain
WHO three step ladder

The main task of the doctor,
* To cure is sometime
* To treat is often, but …
* To comfort is always
Ambroise Pare (1590) the great French surgeon
“physician to the king of France”

I’m ready to die, but with…. No pain, No pain and No pain

Thank you so
much for your attention
Semoga Ada Manfaatnya

Pain in pancreatic cancer
• Pain syndrome associated with pancreatic cancer arise due to involvement of critical structure surrounding pancreas.
• Pain prevalence – Not all pancreatic cancer get pain
– 80% mild to moderate pain at internal cancer
– 44% has severe pain in advance stage
– Pain is linked with depression and anxiety underlines the importance to treat pain.

Pain in pancreatic cancer
• Can be both visceral and neuropathic
• Multifactorial
• Involvement of gut wall
• Nodal disease around the coeliac plexus
• Metastatic disease in the liver

What Is Palliative Care?
• Palliative care is specialized medical care for people with serious illnesses.
• It focuses on providing patients with relief from the symptoms and stress of a serious illness (cancer and chronic Illness).
• The goal is to improve quality of life for both the patient and the family.

Cure Treatment/ Disease Oriented
Palliative Care/ Symptom Oriented
Old concept of Palliative Care (Dichotomy)

Cure Treatment (Life-Prolonging Therapy)
New Concept of Palliative Care (Complementary)
Palliative Care

Palliative Care Concept (Continuum of Care Model)
Disease Progression
D E A T H
B E R E A V E M E N T
Curative Intent
Palliative Care
Curative Care

Goals of Palliative Care
Maintain quality of life; avoid prolongation of dying, prevent hasten the death.

Palliative care
Treats, Prevents, or Relieves,
the symptoms of a serious or chronic illness
but does not cure it.
“ Care beyond Cure”

Pancreatic Cancer
Nature of pancreatic cancer.
• Is one of the most lethal malignancies.
• Is the tenth most common malignancy.
• Survival rate is very low about 4% for all stages in USA
• Palliative care represents an important aspect of care.
• Identifying and treating disease related symptomology are priority.

Why Palliative care become first priority for pancreatic cancer?
1. Because most pancreatic cancer will present with metastatic or locally advanced disease.
2. Even surgical resection combine with adjuvant or adjuvant chemotherapy, disease will recur.
As such , pancreatic cancer patients arrive at a common endpoint where decisions pertaining to palliative care come to the forefront.

No more place for treatment or resection to pancreatic cancer
No improvement in the last 40 years in pancreatic cancer. (Dr. Holly Taylor, England September 2018)

Why pancreatic cancer patients mostly come lately
• These is no well known warning signs in pancreatic cancer.
– New onset of DM in old age patient has been associated with pancreatic cancer.
– Pan less jaundice Is often though as the typical presentation of pancreatic cancer
– Some time mild pain in the abdomen or back can be the sign with depression.
One case

One case…
• Female 60 year old was consulted by Internal Medicine doctor to me due her mild-moderate pain in her abdomen & back – No tenderness – No jaundice – No ascites – Liver is not palpable – CT abdomen np
• She Look very depression and can not sleep Ʀ - Ultracet (paracetamol + tramadol) - Dizepam

Palliative care
• Palliative care is part of supportive care
– Holistic care of patients with incurable advanced progressive illness
– Aim to prevent or treat symptoms as soon as possible
– Management of pain and other symptoms
– Includes psychological, social and spiritual support

What does palliative care involve in
your patients?
Not just physical symptom management…
• Advance care planning
• Social support
• Financial support
• Psychological support
• Continuity

Management of pain
• Morphine drug of choice in liver failure • Buprenorphine also safe • Avoid oxycodone and codeine
• When there is both liver and renal failure, often a choice of
which is worse. Should consider discussing these patients with us!
• Dexamethasone 4-6 mg od should be considered if liver capsule
pain is thought to be a problem
• Neuropathic agents • Amitriptyline, pregabalin gabapentin

WORLD HEALTH ORGANISATIONS
ANALGESIC LADDER
Step 3
Opioid for mod- severe pain
+Non-opioid -/+ Adjuvant
Step 2
Opioid for mild- mod pain
+Non-opioid -/+ Adjuvant Step 1
Non-Opioid
-/+ Adjuvant Pain
Persists
or increases
Pain
Persists
or increases

Cantoh pemberian Obat - By the mouth sebisa mungkin - By the clock
Pasien harus dituliskan skedulnya Jam 06.00 - Paracetamol 500 mg - Celecoxib 200 mg Jam 12.00 - Paracetamol 500 mg Jam 18.00 - Paracetamol 500 mg - Celecoxib 200 mg Jam 22.00 - Paracetamol 500 mg ± Adjuvants

Di Indonesia yang tersedia banyak adalah opiod kerja lama u maitanance
1. Morphine MST continue tablet
2. Fentanyl patch (transdermal) once in 3days
3. Hydromorphone tab Once daily.
2. Oxycodone Controled Release (single dose q/24 h and
multiple dose q/12 h)
Available Strong long acting opioid in Indonesia

1. Morphine Slow release (MST) has been used for 20 years
Twice a day

2. Fentany Patch
Once in 3 days ( Every 72 hours)

2. Fentanyl patch • Routes of Administration * Transdermal * Optimal action 18 hour • Duration of action 72 hours.
• Note! 1. Should not be used in naïve opioid (morphine)
patients. 2. Only for cancer pain patiens .

3.Hydromorphone Retard tablet
Once a day

Oxycodone tab Controlled Release q /12 h
Twice a day

Principles of Palliative Care
• Affirms life, regards dying as a normal process.
• Neither hastens nor postpones death
• Fundamental purpose is to alleviate pain and suffering
• Focuses on treatment that enhances comfort and improves quality of life
• Dying is a process, not an illness

Rule 10 Multi-modal pain management. Intervention pain management techniques a rarity.
1 August 2019 Naveen Salins 2016 12


Rule of severe pain management
• Severe pain needs strong analgesic.
• Strong analgesic is Strong opioid .
1. Morphine Iv, tab IR MST continus tablet
2. Fentanyl iv, patch (transdermal) once in 3days
3. Hydromorphone tab once daily.
4. Oxycodone tab IR, CR. and iv.
available soon.
Strong opioid

The difference between Hospice & Palliative
Hospice
• To improve QoL for both patients and family
• End of life, less 6 M
• No more treatment of disease
• Only for terminal cancer patients.
Palliative
• To improve QoL for both patients and family
• Start from diagnose
• Together with treatment of disease.
• For any kind of serious disease at any age any stage of diseases.

Not only Cancer but also
all severe illness
Hospice
Palliative Care
Only terminal cancer patients,
about 6 M

Use WHO Three Step Ladder, (1986)
5 essential concepts
1. By mouth
2. By the clock
3. By the ladder
4. By individual
5. With attention to detail
By this stepwise about 90% of cancer pain can be relieved.

Palliative Care of Pancreatic Cancer
• Pain Management
• Intestinal Obstruction
• Biliary Obstruction
• Depression
• Fatigue
• Pancreatic Insufficiency
• Cachexia

Palliative Care of Pancreatic Cancer
• Pain Management
• Obstructive Jaundice
• Gastric Outlet obstruction
• Prophylactic Gastrojejunostomy
• Endoscopic Palliation
• Endoscopic Stenting Versus Gastrojejunostomy
Other issue in pancreatic Cancer
Nutrition in Pancreatic Cancer.
Thromboembolic Disease