Embed Size (px)
Citation preview
Pain Management
Dr. J.M. Roesner, DVM, DABVP
Dr. Vanessa Lee, DVM
Ethics and Economics of Pain Management
Pain Pathway and Strategies for Pain Reduction
NSAIDS Tepoxalin Parting Thoughts
AVMA Position
“Animal pain and suffering are clinically important conditions that adversely
affect an animals quality of life. Drugs, technique or husbandry methods used
to prevent and control pain must be tailored to individual animals.”
(JAVMA 2001:218:1694)
Untapped Market:
60% or more of DJD dogs are not treated or managed by a DVM.
(JAVMA 2002:221:215-222)
“Ethical Economics”
Types of Pain
1. Somatic
Skin, musculoskeletal Dull, aching, localizable
2. Visceral
Compression, distension, infiltration of pelvic, abdominal or thoracic organs
May be difficult to localize
3. Neuropathic
Nerve compression, damage infiltration, +/-hyperalgesia
Severe burning or tingling
(Tranquilly, Teton Press)
NMDA Receptor
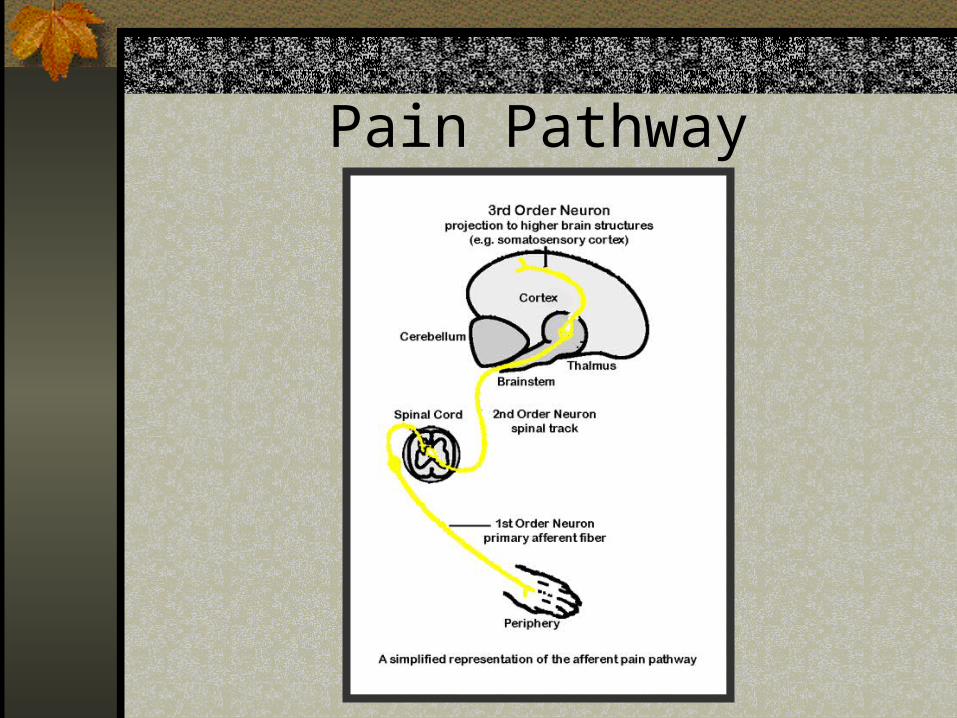
Pain Pathway
Pain Pathway Continued:
“First Pain” – A-delta, fast
“Second Pain” - C fibers, slow
Dorsal Root Ganglia – contains afferent cell bodies
Pain Pathway Continued:
Dorsal Horn of Spinal Cord (2nd order Neurons)
Site of Synapse of First Order Neurons:
A: excitatory and inhibitory interneurons
B: propriospinal neurons (segmental reflex activity)
C: projecting neurons to supraspinal centers (midbrain, cortex)
Spinothalamic, Spinocervical, Spinomesencephalic
Pain Pathway Continued:
3rd order neurons are within:
Medulla Pons Midbrain Thalamus Hypothalamus Cerebral Cortex
Pain Pathway Continued:
Descending inhibitory influences occur within cortex, thalamus, midbrain,
rostral medulla and brain stem.
Nociception:
A: Transduction: receptor translates physical energy into electrical energy
B: Transmission: A delta and C fibers propagate impulses
C: Modulation: endogenous descending analgesic systems (opiod, serotonergic and noradrenergic) inhibit stimuli processing in spinal dorsal horn cells.
Pain Recognition
HR, BP, RR, peripheral vasoconstriction
Restless Sedentary hunched Appetite Purring, vocalization Pain scores – VAS & NRS
Pain has negative consequences on healing, morbidity &
mortality.
Assume an animal is painful if you would be in a similar
circumstance.
Preemptive Analgesia
Rx Prior to stimulus Minimizes likelihood of chronic pain Pain is easier to prevent than to
alleviate (windup) e.q. premed opiods, NSAIDS, Alpha 2
agonists, local blocks, epidurals
Multimodal Analgesia
Synergistic Decreased potential for adverse reactions Effective E.g NSAID transduction Local Block stops transmission Opiod and Alpha 2 agonist modulation
Multimodal Analgesia
Decreases nociceptor sensitization (inflammation)
Decreases wind up (neuroplastic changes in cord)
Decreases tachyphylaxis Decreases neuroendocrine response Decreases convalescent time Improves healing (perfusion) Improves immune function
Sites of Drug Intervention in Pain Processing
Inhibit Transduction(peripheral sensitization of nociceptors)
Local anesthetics Opiods NSAIDs Corticosteriods
Inhibit Transmission(impulse conduction)
Local anesthetics Alpha 2 agonists
Modulation of Spinal Pathway(inhibit central sensitization)
Local anesthetics Opiods Alpha 2 agonists Trycyclic antidepressants Cholinesterase inhibitors NMDA antagonists NSAIDs Anticonvulsants
Inhibit Perception
General anesthetics Opiods Alpha 2 agonists Benzodiazepams Phenothiazines
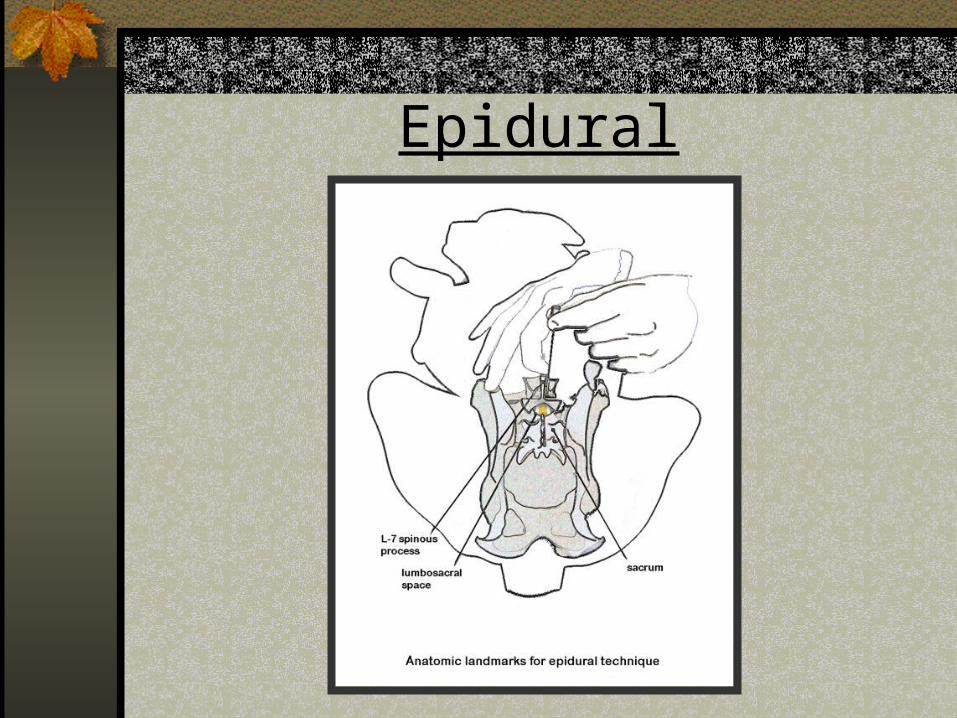
Epidural
Epidural
Lidocaine Bupivicaine 1 ml/4.5 kg or 1 ml/3.5 kg for abdominal
Morphine Fentanyl Alpha 2 Agonists Buprenorphine
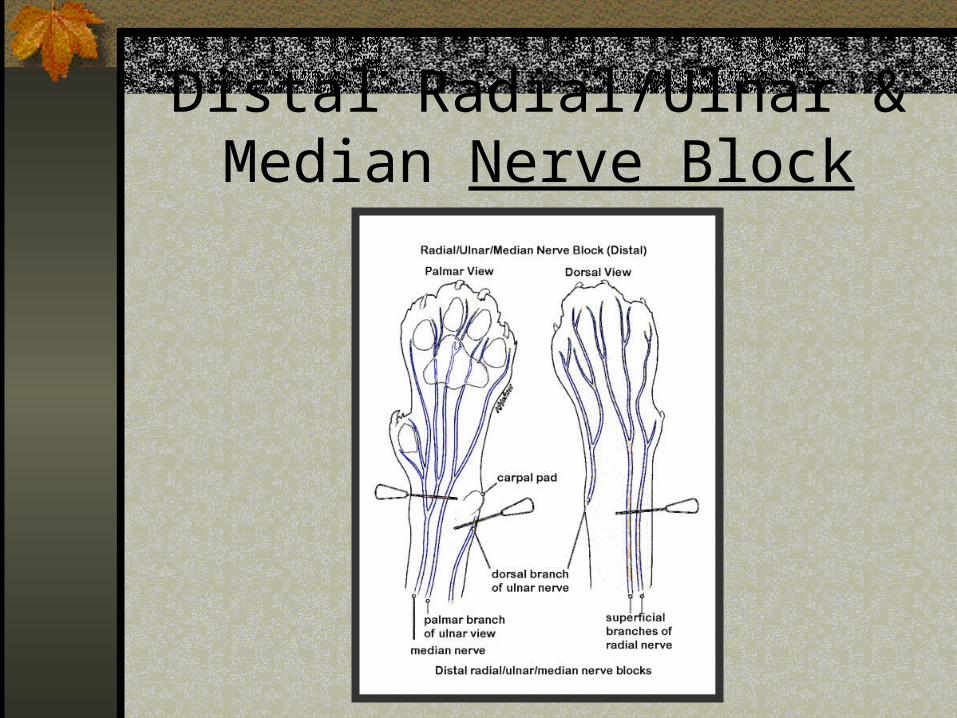
Distal Radial/Ulnar & Median Nerve Block
Articular Blocks - Stifle
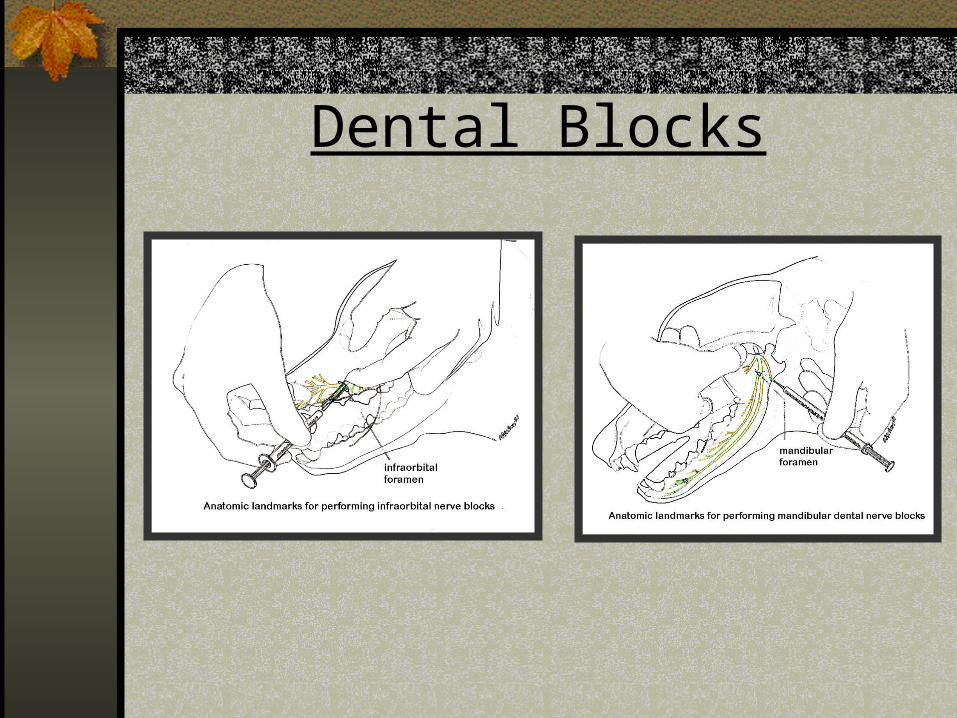
Dental Blocks
Intercostal Blocks
CRI’s
Can overcome short +/- ½ limitations Morphine, Ketamine, Butorphanol Calculator programs available
Transdermal
Fentanyl or lidoderm patches Topical gabapentin Emla cream
Drugs to Consider:
Tramadol Amatidine Dextromethorphan Gabapentin IV lidocaine
Butorphanol (Plumb 2005)
Kappa agonist, mu antagonist, sigma agonist
NOT adequate for severe pain NOT adequate for bone pain Controlled (C-IV) Short duration of analgesia (best in CRI,
has a ceiling effect)
Analgesic Doses
D: 0.1-1.0 mg/kg (SQ, IM, IV) C: 0.1-1.0 mg/kg (SQ, IM, IV) H: 0.1 (SQ, IM, IV) Ferret: 0.05-0.1 mg/kg (SQ, IM, IV) Rabbit, Rodent: 0.4 mg/kg (IV, SQ, IM) Avian: 2-4 mg/kg
Buprenorphine (Plumb 2005)
Partial mu agonist, weak kappa antagonist Long duration Sublingual and buccal use in cats Scheduled C-III May decrease analgesia from pure mu
agonists (controversial, may be species dependent)
Contra indicated in patients on MAOI Ceiling effect
Analgesic Doses
D: 0.005-0.03 mg/kg (IV, SQ, IM) C: 0.005-0.03 mg/kg (IV, SQ, IM or
buccal Ferret: 0.01-0.05 mg/kg (IV, SQ, IM) H: 0.004-0.02 mg/kg (IV, SQ, IM) Rabbit: 0.02-0.05 mg/kg (IV, SQ, IM) Rodent: 0.1-0.05 mg/kg (IV, SQ, IM)
Fentanyl (Plumb 2005)
Pure mu agonist CRI or patch Class C-II Alters amylase and lipase Do not combo with MAOI Some variation in patch absorption with
individual and site Dosing see pg. 328 Plumb
Tramadol (Plumb 2005)
Mu agonist, SSRI, decreases norepinephrin reuptake
Caution with combo in SSRI, MAOI, TCA, SAME, digoxin
Synergistic with NSAIDS Naloxone does not fully reverse Inexpensive, unscheduled Analgesic doses: PO D: 1-4mg/kg q 8-12
C: 4 mg/kg q 12 Injectable form available in Europe
Ketamine (Plumb 2005)
NMDA receptor antagonist, dissociative anesthetic
Decreases “wind up” in spinal cord processing of pain
Doses are lower for analgesia than anesthesia
Adverse effects are less than when used as an anesthetic, but still present
Use as adjunct with narcotics
Analgesic Doses
D: 0.1-1 mg/kg PO,IM, SQ q 4-6 h CRI 0.1-0.3 mg/kg h
C: 0.1-1 mg/kg IM,SQ q 4-6 h CRI 0.1-0.3 mg/kg h
Exotic Species-little analgesic data extrapolate from anesthetic doses
Amantidine (Plumb 2005)
NMDA receptor antagonist, antiviral Oral, inexpensive, gel cap Use as an adjunct in pain management
(especially with opioids, NSAIDS) Drug interactions: TMS, quinidine, thiazide,
diuretics, triamterene, CNS stimulants, anticholinergics
Analgesic Doses: D: 1.25-4 mg/kg PO q 12-24 h, C: 3 mg/kg PO q 24h
Dextromethorphan
NMDA antagonist, SSRI, antitussive Conflicting pain data Caution mixing with MAOI and SSRI
(serotonin syndrome) Doses: Dog: 1-2 mg/kg q 12h
Gabapentin (Plumb 2005)
Analgesic, anticonvulsant, psychiatric Rx Oral, fairly expensive Adjunct in management of chronic pain Mechanism unknown Drug interactions: antacids decrease
absorption, may increase AUC when combined with morphine or hydrocodone
False positive for protein on urine multistix
Analgesic Dose
D: 3 mg/kg PO q 24 h C: 3 mg/kg PO q 24 h Anectdotal: can be used in transdermal
prep applied to trigger points for fibromyalgia and migraines in man
Amitriptyline (Plumb 2005)
Tricyclic antidepressant Mechanism unclear: blocks amine pump
(increase NE, serotonin), sedation, anticholinergic Adjunct in chronic pain, antipuritic Caution in patients with seizures, MAOIs,
glaucoma, thyroid disease, cardiac or metabolic disease
May alter blood glucose levels Analgesic Doses: D: 1-2 mg/kg PO q 12-24h C:
0.5-2 mg/kg PO q 24 h
Lidocaine (Marc Raffe personal communication)
Local anesthetic, CRI useful in analgesia, antiarrythmic
Do not use lidocaine with epinephrine IV Cats may be more sensitive to CNS depression Emla cream Dose CRI: Dog: 2 mg/kg/hour MLK Protocol: Morphine 0.1 mg/kg/h,
Medetomidine 1 mcg/kg/h, Lidocaine 2 mg/kg/h, Ketamine 0.2 mg/kg/h
Serotonin Syndrome (ASPCA Poison Control
Center personal communication)
Causes: Drugs that increase synthesis (L trytophan; I-5HT) Drugs that increase presynaptic release (MAO
inhibitors, cocaine, amphetamine) Drugs that inhibit uptake into presynaptic neurons
(SSRI, tricyclics, amphetamine, cocaine, dextromethorphan, meperidine)
Drugs that inhibit metabolism (MAO inhibitors) Drugs that act as serotonin agonists (buspirone,
sumatryptin, LSD)
Serotonin Syndrome Symptoms Myoclonus Mental aberration Agitation (can also be sedate) Hyperreflexia Tremors Diarrhea Atoxia Hyperthermia Man-3 of above (ASPCA Poison Control Center personal communication)
Serotonin Syndrome Treatment Cyproheptadine=non-selective serotonin
antagonist Dogs: 1.1 mg/kg Cats: 2-4 mg/kg Can be given PO or as an enema in saline Support (fluids, antidiarrheals, cooling etc.) Propranolol if tachycardic (Personal Communication
ASPCA Poison Control Center)
Inflammation
NF α, ILI from cells at site Eselecin on endoth cell L selectin on PMN intermittantly binds E & P
selectin on endoth PMN rolling on endoth Beta 2 CD 11/CD r8 integrin on PMN binds
ICAM1 & Icam2 on endoth Emigrate PMN through entotheliumChemotaxins C5a LT ect help direct emigration
A new class of NSAIDs… Dual inhibitors
(ZUBRIN)
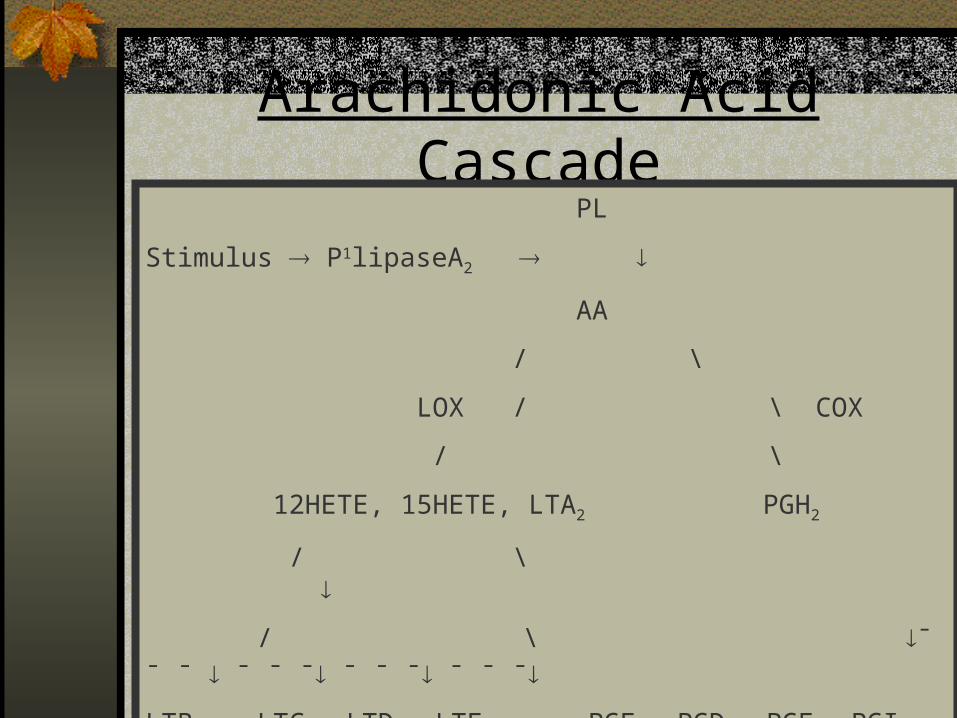
Arachidonic Acid Cascade PL
Stimulus P1lipaseA2
AA
/ \
LOX / \ COX
/ \
12HETE, 15HETE, LTA2 PGH2
/ \
/ \ ¯ ¯ ¯ ¯ ¯ ¯ ¯ ¯ ¯ ¯ ¯ ¯
LTB4 LTC4, LTD4, LTE4 PGE2 PGD2 PGF2α PGI2 TXAα
(SRSA) (“PC”)
Prostaglandin Actions(deLeval et al, 2002)
PG, PC Vasodilate TXA2 vasconstriction PC(PGI2) platelet aggregation TXA2 platelet aggregation PG, TX vascular permeability edema PG contract longitudinal GI muscle, relax
circular PG contract uterine smooth muscle PG RBF, stimulate diuress
Leukotriene Actions(deLeval et al, 2002)
PMN margination endothelial permeability Chemotatic egress WBC from tissue Contract respiratory smooth muscle Species variable contraction on GI muscle acid secretion (rabbit) Vasoconstrictive Stimulate bone reabsorbtion
Sources
COX1 GI epithelium Kidney Platelets Seminal Vesicles
COX2 Endothelial cells Monocytes Macrophage Fibroblast Synovial cells Chondrocytes
PMN’s Eosinophiles Macrophage Reticulocytes Mast Cells
Leukotriene Sources (deLeval et al, 2002)
The Old Story:COX2 inducible inflammatoryCOX1 constituative housekeeping
INFORMATION TO CONSIDER: (Papich NAVC, 2004)
Invitro data for COX1:COX2 does not always reflect in vivo, species
Both COX1 and COX2 must be inhibited in man to produce analgesia.
COX2 selective drugs have similar rates of GI side effects as non selective.
Concentration at site of action may be different than that of in vitro systems and drug may reflect different selectivity at that concentration.
COX2 products are essential for GI ulcer healing.
Thrombosis (Hennan et al circulation 2001, 104, 820-825)
COX2 PGI2(PC) vasodilation and decreased platelet aggregation
COX1 TxA2 increased aggregation ie COX2 inhibition may be prothrombotic
Invitro Selectivity Data
E.g Carprofen COX1:COX2 = 129 (Canine Enzyme system, Rickets et al
1998) 1.0 (sheep, rodent, Vane et al, 1995) 1.75 (canine macrophate, Kay-Mungford,
2000) No effect either COX1 or COX2 (Bryant et
al, 2003)
5-LOX and Leukotrienes
LT when block COX(Gilroy et al EurJ Pharmacol, 1998)
Potential Alternative Mechanism for NSAIDs
Stimulus Cell Membrane
Transcription Factor 1kB Nucleus
Nuclear Factor Kappa B Gene Transcription Cytokines
TEPOXALIN
Parent drug, LOX inhibition, 3-5 hours Active metabalite COX inhibition, > 24 hours No accumulation Reaches therapeutic levels in 1-2 hours in
human knee Feeding enhances absorption ODT
Site Specific PG Inhibition(Wallace et al Gastroenterology, 1993)
PGE2 levels in gastric mucosa, liver & blood of rats was not decreased.
PGE2 levels at sites of inflammation were decreased.
May impact joint pathology positively by LT
1982 Palmoske and Brandt;More significant joint lesions in humans on
chronic high dose COX inhibitors.
Other properties of Tepoxalin(deLeval et al, 2002)
Inhibits IL6 in astrocytes Inhibits IL1 in vitro human synovium Inhibits Mac1 & Eselectin expression Inhibits NF kappa beta activation rgene
expression
PO tepoxalin in man PGE2 and lT in osteoarthritis knee (Willburger et al, 1998)
PO tepoxalin in dogs PGE2 and LT B4 in knee model (Schering Plough Data on file)
PO tepoxalin in rats PMN number adherence and diapedesis (Kirchner PG, LT and EFA, 1997)
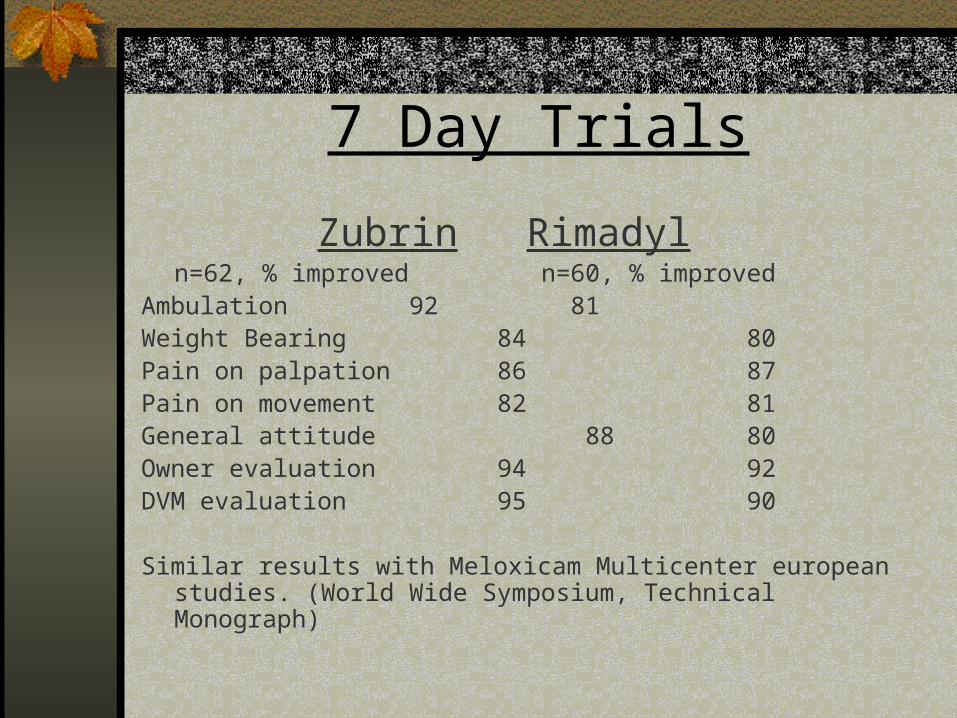
7 Day Trials
Zubrin Rimadyln=62, % improved n=60, % improved
Ambulation 92 81Weight Bearing 84 80Pain on palpation 86 87Pain on movement 82 81General attitude 88 80Owner evaluation 94 92DVM evaluation 95 90
Similar results with Meloxicam Multicenter european studies. (World Wide Symposium, Technical Monograph)
28 day Efficacy Study
84% of dogs improved Incremental benefit if extend 14 28
days(Technical Monograph Worldwide Symposium)
Safety/SIDE EFFECTS
GI Direct chemical vs PG medication Differential COX2 inhibition COX2 products needed for ulcer healing LT mediate ulceration
Renal COX2 constituative in kidney
(Rossa et all, 1999) PG mediated ischemic necrosis
Hepatic Any NSAID has potential for idiosyncratic response

Medicolegal Monitor bloodwork Reminders Decrease dose

VID in 7 day trial
Tepoxalin vs Carprofen Zubrin vs Meloxicam
% dogs with 5.4 7.5 10.3 19.2
vomiting or
Diarrhea
n=82 n=77 n=107 n=99

SAFETY STUDIES
28 days, 32 dogs, up to 300mg/kg No adverse effects No drug accumulation
13 weeks, 6 dogs, 100mg/kg No adverse effects
13 weeks, 6 dogs, 300mg/kg protein, albumin, Ca, PCV in 1 dog Small pyloric ulcer in 1 dog
13 weeks, 6 dogs, 20mg/kg No adverse effects

SAFETY STUDIES: 6 Months
20mg/kg n=8 no adverse effects 100 mg/kg n=8 1 ulcer on gross 300 mg/kg n=8 3 ulcers

No chemical change in hepatic or renal biochemical
parameters in any of the above.

Safety Studies: 1 Year
100 mg/ml n=8 no renal hepatic or GI toxicity
30 mg/kg n=8 no renal hepatic or GI toxicity
300 mg/kg n=8 2 dogs with GI erosions & small ulcers
(World Wide Symposium)

European Study (World Wide Symposium)
9/02 – 4/03 data, 1294 cases, 134 DVMs Acute or chronic musculoskeletal disease 10 mg/kg SID x 1-4 weeks Questionnaire completed by DVM 82% good or excellent response Concomitant disease in 23.3% Adverse events:
3.9% emesis 2.2% diarrhea 0.9% anorexia 0.6% lethargy 0.23% severe event (hemorrhagic diarrhea ect)