Embed Size (px)
Citation preview

PAIN MANAGEMENT
• Definition
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage (Merskey & Bogduk, 1994)
It is the most common reason for seeking health care. It occurs with many disorders, diagnostic tests, and treatments
• Nurses encounter patients in pain in a variety of settings, including acute care, outpatient, and long-term care settings, as well as in the home. Thus, they must have the knowledge and skills to assess pain, to implement pain relief strategies, and to evaluate the effectiveness of these strategies, regardless of setting.
• Pain management is considered such an important part of care that the American Pain Society coined the phrase “Pain: The 5th Vital Sign” (Campbell, 1995) to emphasize its significance and to increase the awareness among health care professionals of the importance of effective pain management.
• Documentation of pain assessment is now as prominent as the documentation of the “traditional” vital signs. Pain assessment and management are also mandated by the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) (2003).
• Calling pain the fifth vital sign suggests that the assessment of pain should be as automatic as taking a patient’s blood pressure and pulse.
• The JCAHO (2003) has incorporated pain and pain management into its standards. JCAHO’s standards state that “pain is assessed in all patients” and that “patients have the right to appropriate assessment and management of pain.” These standards reflect the importance of pain management.
• In health care, the primary care provider’s role is to assess and manage pain by administering medications and other treatments.
• In addition, the nurse serves as an educator to the patient and family, teaching them to manage the pain relief regimen themselves when appropriate
• Although it is important to believe the patient who reports pain, it is equally important to be alert to patients who deny pain in situations where pain would be expected.
• A nurse who suspects pain in a patient who denies it should explore with the patient the reason for suspecting pain, such as the fact that the disorder or procedure is usually painful or that the patient grimaces when moving or avoids movement.
• Exploring why the patient may be denying pain is also helpful. Some people deny pain because they fear the treatment that may result if they report or admit pain. Others deny pain for fear of becoming addicted to opioids (previously referred to as narcotics) if these medications are prescribed.
Types of Pain
• Pain is categorized according to its duration, location, severity, nature and etiology.
• Three basic categories of pain are generally recognized: acute pain, chronic (nonmalignant) pain, and cancer-related pain.
• ACUTE PAIN• Usually of recent onset and commonly associated with a specific injury,
acute pain indicates that damage or injury has occurred.
• Pain is significant in that it draws attention to its existence and teaches the person to avoid similar potentially painful situations. If no lasting damage occurs and no systemic disease exists, acute pain usually decreases along with healing.
• For purposes of definition, acute pain can be described as lasting from seconds to 6 months. However, the 6-month time frame has been criticized (Brookoff, 2000) as inaccurate since many acute injuries heal within a few weeks and most heal by 6 weeks.
• In a situation where healing is expected in 3 weeks and the patient continues to suffer pain, it should be considered chronic and treated with interventions used for chronic pain. Waiting for the full 6-month time frame in this example could cause needless suffering.
2. CHRONIC (NONMALIGNANT) PAIN• Chronic pain is constant or intermittent pain that persists beyond the expected
healing time and that can seldom (some time) be attributed to a specific cause or injury.
• It may have a poorly defined onset, and it is often difficult to treat because the cause or origin may be unclear.
• Although acute pain may be a useful signal that something is wrong, chronic pain usually becomes a problem in its own right.
• Chronic pain may be defined as pain that lasts for 6 months or longer, although 6 months is an arbitrary period for differentiating between acute and chronic pain.
• An episode of pain may assume the characteristics of chronic pain before 6 months have elapsed (past), or some types of pain may remain primarily acute in nature for longer than 6 months. Nevertheless, after 6 months, most pain experiences are accompanied by problems related to the pain itself. Chronic pain serves no useful purpose. If it persists, it may become the patient’s primary disorder.
• The nurse may come in contact with patients with chronic pain when they are admitted to the hospital for treatment or when they are seen out of the hospital for home care. Frequently the nurse is called on in community-based settings to assist patients in managing pain.
CANCER-RELATED PAIN
Pain associated with cancer may be acute or chronic. Pain in the patient suffering from cancer can be directly associated with the cancer (eg, bony infiltration with tumor cells or nerve compression), a result of cancer treatment (eg, surgery or radiation), or not associated with the cancer (eg, trauma). Most pain associated with cancer, however, is a direct result of tumor involvement.
PAIN CLASSIFIED BY LOCATIONPain is sometimes categorized according to location, such as pelvic pain, headache,and chest pain. This type of categorization is helpful in communicating and treating pain. For example, chest pain suggests angina or a myocardial infarction and indicates the need for treatment according to cardiac care standards.
PAIN CLASSIFIED BY ETIOLOGYCategorizing pain according to etiology is another way to think about pain and its management. Burn pain and postherpetic neuralgia are examples of pain described by their etiology.
PAIN CLASSIFIED BY SEVERITYMild, Moderate and Sever
PATHOPHYSIOLOGY OF PAIN
The sensory experience of pain depends on the interaction between the nervous system and the environment. The processing of noxious stimuli and the resulting perception of pain involve the peripheral and central nervous systems.
PAIN TRANSMISSION
Among the nerve mechanisms and structures involved in the transmission of pain perceptions to and from the area of the brain that interprets pain are nociceptors, or pain receptors, and chemical mediators. Nociceptors are receptors that are preferentially sensitive to a noxious stimulus. Nociceptors are also called pain receptors.
Nociceptors
• Nociceptors are free nerve endings in the skin that respond only to intense, potentially damaging stimuli. Such stimuli may be mechanical, thermal, or chemical in nature.
• The joints, skeletal muscle, fascia, tendons, and cornea also have nociceptors that have the potential to transmit stimuli that produce pain.
• However, the large internal organs (viscera) do not contain nerve endings that respond only to painful stimuli. Pain originating in these organs results from intense stimulation of receptors that have other purposes. For example, inflammation, stretching, ischemia, dilation, and spasm of the internal organs all cause an intense response in these multipurpose fibers and can cause severe pain.
Peripheral Nervous System
A number of algogenic (pain-causing) substances that affect the sensitivity of nociceptors are released into the extracellular tissue as a result of tissue damage.
Histamine, bradykinin, acetylcholine, serotonin, and substance P are chemicals that increase the transmission of pain. The transmission of pain is also referred to as nociception. Prostaglandins are chemical substances thought to increase the sensitivity of pain receptors by enhancing the pain provoking effect of bradykinin. These chemical mediators also cause vasodilation and increased vascular permeability, resulting in redness, warmth, and swelling of the injured area.
Once nociception is initiated, the nociceptive action potentials are transmitted by the peripheral nervous system (Porth, 2002). The first-order neurons travel from the periphery (skin, cornea, visceral organs) to the spinal cord via the dorsal horn.
There are two main types of fibers involved in the transmission of nociception. Smaller, myelinated Aδ (A delta) fibers transmit nociception rapidly, which produces the initial “fast pain.”
Type C fibers are larger, unmyelinated fibers that transmit what is called second pain. This type of pain has dull, aching, or burning qualities that last longer than the initial fast pain. The type and concentration of nerve fibers to transmit pain vary by tissue type.
If there is repeated C fiber input, a greater response is noted in dorsal horn neurons, causing the person to perceive more pain. In other words, the same noxious stimulus produces hyperalgesia, and the person reports greater pain than was felt at the first stimulus. For this reason, it is important to treat patients with analgesic agents when they first feel the pain. Patients require less medication and experience more effective pain relief if analgesia is administered before the patient becomes sensitized to the pain.
Chemicals that reduce or inhibit the transmission or perception of pain include endorphins and enkephalins. These morphine like neurotransmitters are endogenous (produced by the body). They are examples of substances that reduce nociceptive transmission when applied to certain nerve fibers. The term “endorphin” is a combination of two words: endogenous and morphine.
Endorphins and enkephalins are found in heavy concentrations in the central nervous system, particularly the spinal and medullary dorsal horn, the periaqueductal gray matter (gray matter around brain) , hypothalamus, and amygdala. Morphine and other opioid medications act at receptor sites to suppress the excitation initiated by noxious stimuli.
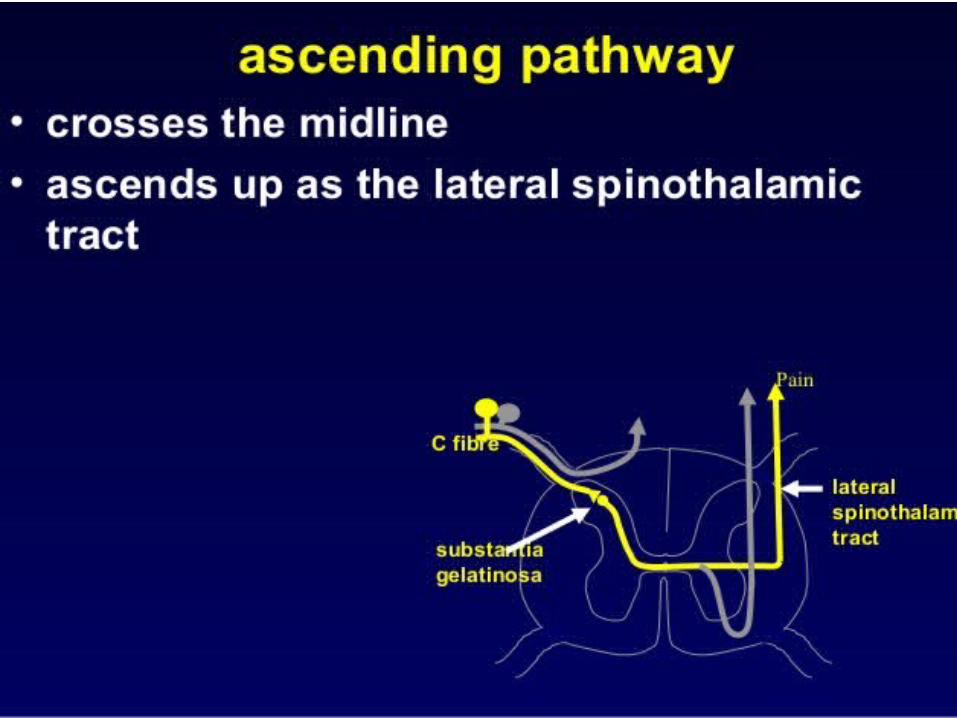
Central Nervous SystemAfter tissue injury occurs, nociception (the neurologic transmission of pain impulses) to the spinal cord via the Aδ and C fibers continues. The fibers enter the dorsal horn. In the substantia gelatinosa are projections that relay nociception to other parts of the spinal cord
Nociception continues from the spinal cord to the reticular formation, thalamus, limbic system, and cerebral cortex.
The involvement of the reticular formation, limbic, and reticular activating systems is responsible for the individual variations in the perception of noxious stimuli. Individuals may report the same stimulus differently based on their anxiety, past experiences, and expectations. This is a result of the conscious perception of pain.
For pain to be consciously perceived, neurons in the ascending system must be activated. Activation occurs as a result of input from the nociceptors located in the skin and internal organs. Once activated, the inhibitory interneuronal fibers in the dorsal horn inhibit or turn off the transmission of noxious stimulating information in the ascending pathway.
Descending Control SystemThe descending control system is a system of fibers that originate in the lower and midportion of the brain (specifically the periaqueductal gray matter) and terminate on the inhibitory interneuronal fibers in the dorsal horn of the spinal cord.
This system is probably always somewhat active; it prevents continuous transmission of stimuli as painful, partly through the action of the endorphins. As nociception occurs, the descending control system is activated to inhibit pain.
Cognitive processes may stimulate endorphin production in the descending control system. The effectiveness of this system is illustrated by the effects of distraction. The distractions of visitors or a favorite TV show may increase activity in the descending control system. Therefore, the person who has visitors may not report pain because activation of the descending control system results in less noxious or painful information being transmitted to consciousness. Once the distraction by the visitors ends, activity in the descending control system decreases, resulting in increased transmission of painful stimuli.
The interconnections between the descending neuronal system and the ascending sensory tract are called inhibitory interneuronal fibers. These fibers contain enkephalin and are primarily activated through the activity of non-nociceptor peripheral fibers (fibers that normally do not transmit painful or noxious stimuli) in the same receptor field as the pain receptor, and descending fibers, grouped together in a system called descending control.
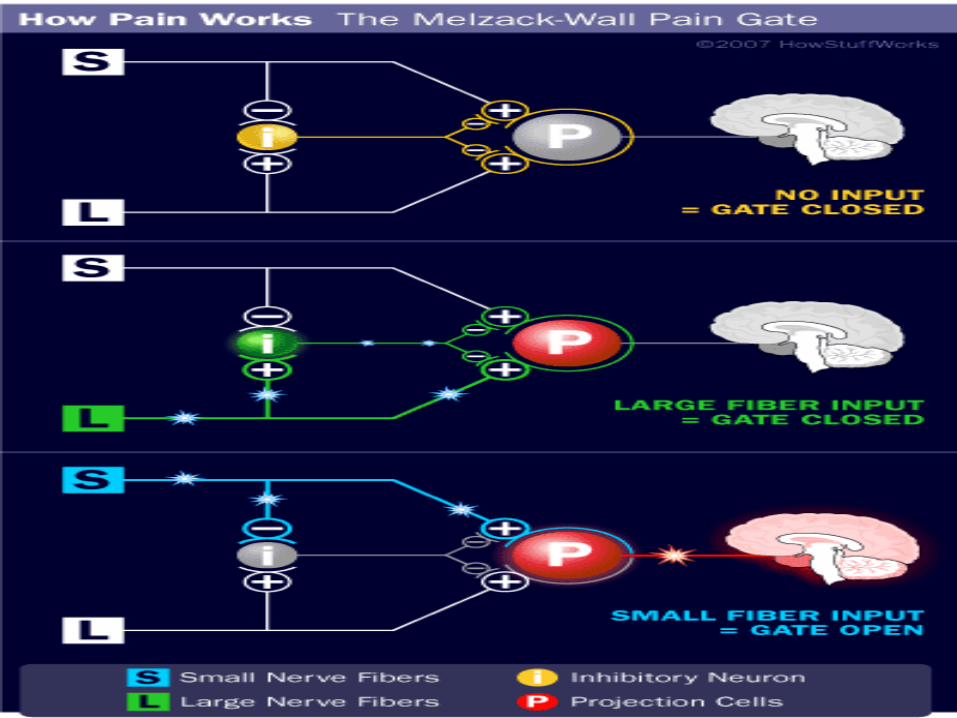
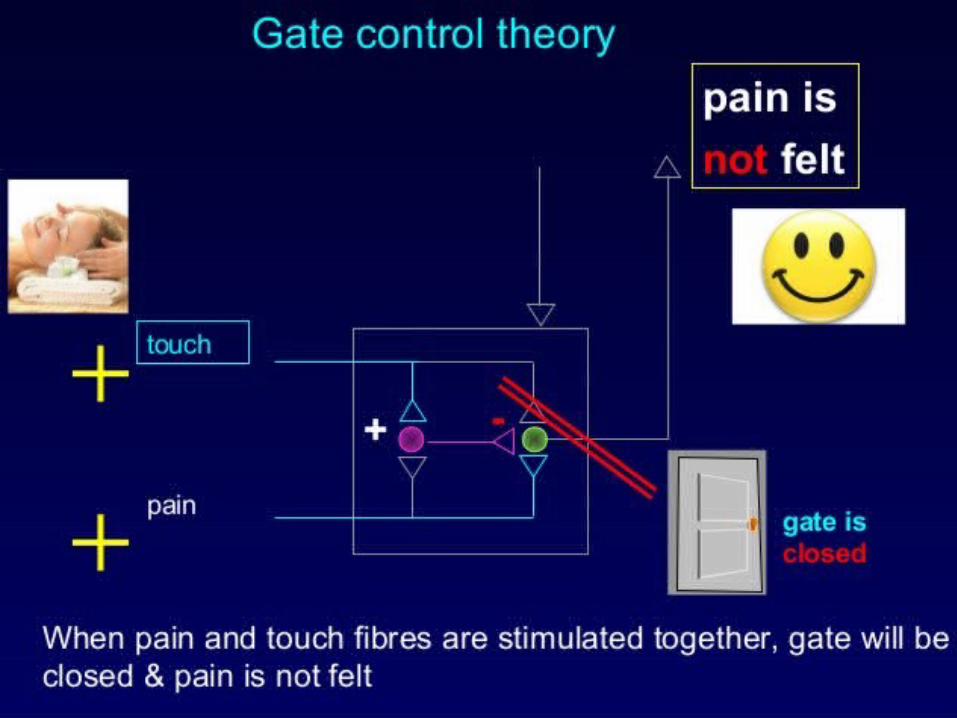
• First proposed in 1965 by Ronald Melzack and Patrick Wall, The gate control theory of pain asserts that non-painful input closes the "gates" to painful input, which prevents pain sensation from traveling to the central nervous system. Therefore, stimulation by non-noxious input is able to suppress pain.
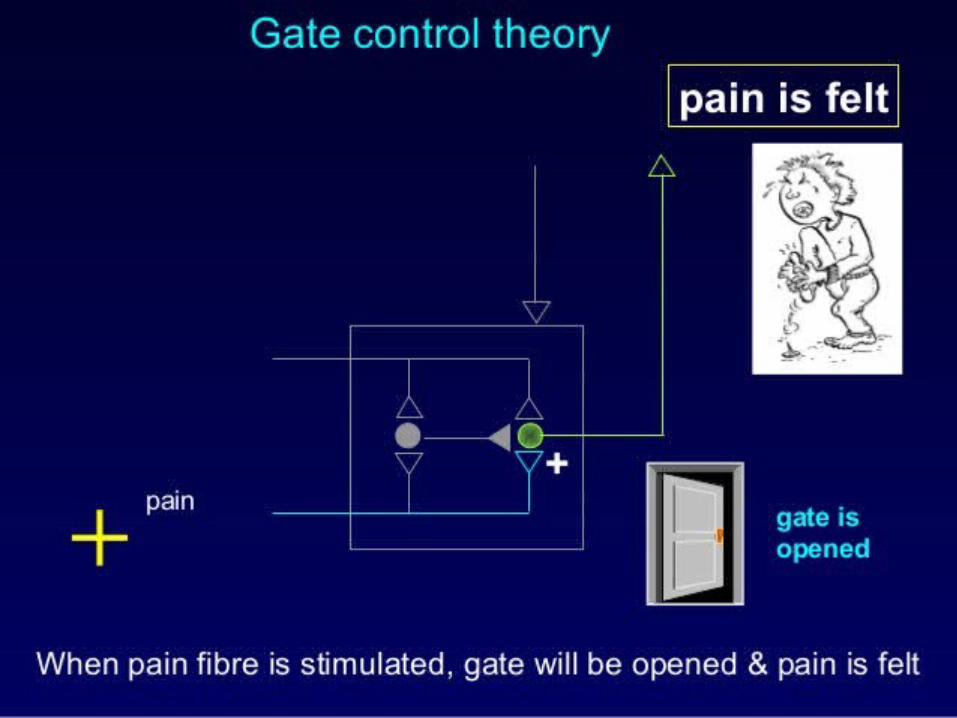
• According to the gate control theory, pain signals are not free to reach the brain as soon as they are generated at the injured tissues or sites. They need to encounter certain ‘neurological gates’ at the spinal cord level and these gates determine whether the pain signals should reach the brain or not.
• In other words, pain is perceived when the gate gives way to the pain signals and it is less intense or not at all perceived when the gate closes for the signals to pass through. This theory gives the explanation for why someone finds relief by rubbing or massaging an injured or a painful area
GATE CONTROL THEORY
Every organ or part of the human body has its own nerve supply and the nerves carry the electrical impulses generated in response to various sensations like touch, temperature, pressure and pain.
These nerves – that constitute the peripheral nervous system – transmit these impulses to the central nervous system (the brain and spinal cord) so that these impulses are interpreted and perceived as sensations.
The peripheral nerves send signals to the dorsal horn of the spinal cord and from there the sensory signals are transmitted to the brain through the spinothalamic tract. Pain is a sensation that alerts a person that a tissue or a particular part of the human body has been injured or damaged.
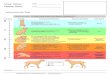
According to the axonal diameter and the conduction velocity, nerve fibers can be classified into three types – A, B and C. The C fibers are the smallest among all the three types. Among the ‘A’ fibers are four subtypes: A-alpha, A-beta, A-gamma and A-delta. Among the A subtypes, the A-alpha fibers are the largest and the A-delta fibers are the smallest.
The A fibers that are larger than the A-delta fibers, carry sensations like touch, pressure, etc. to the spinal cord. The A-delta fibers and the C fibers carry pain signals to the spinal cord. A-delta fibers are faster and carry sharp pain signals while the C fibers are slower and carry diffuse pain signals.
When considering the conduction velocity, the A-alpha fibers (the large nerve fibers) have higher conduction velocity when compared to the A-delta fibers and the C fibers (small nerve fibers). When a tissue is injured, the A-delta fibers are activated first, followed by the activation of the C fibers.
What does the gate control theory say?The gate control theory suggests that the signals encounter ‘nerve gates’ at the level of the spinal cord and they need to get cleared through these gates to reach the brain. Various factors determine how the pain signals should be treated at the neurological gates. They are:The intensity of the pain signalsThe intensity of the other sensory signals (touch, temperature and
pressure), if generated at the site of injuryThe message from the brain itself (to send the pain signals or not)
According to the original postulate of Melzack and Wall, the nerve fibers project to the substantia gelatinosa (SG) of the dorsal horn and the first central transmission (T) cells of the spinal cord.
The SG consists of inhibitory interneurons that act as the gate and determine which signals should reach the T cells and then go further through the spinothalamic tract to reach the brain.
When the pain signals carried by the small fibers (A-delta and C fibers) are less intense compared to the other non-pain sensory signals like touch, pressure and temperature, the inhibitory neurons prevent the transmission of the pain signals through the T cells.
The non-pain signals override the pain signals and thus the pain is not perceived by the brain. When the pain signals are more intense compared to the non-pain signals, the inhibitory neurons are inactivated and the gate is opened.
The T cells transmit the pain signals to the spinothalamic tract that carries those signals to the brain. As a result, the neurological gate is influenced by the relative amount of activity in the large and the small nerve fibers.
Emotions and thoughts determine the way how pain is perceived
• The theory also proposed that the pain signal transmission can be influenced by emotions and thoughts.
• It is well known that people do not feel a chronic pain or the pain does not disturb them when they concentrate on other activities that interest them. Whereas, people who are anxious or depressed feel intense pain and find it difficult to cope up with it.
• This is because the brain sends messages through descending fibers that stop, reduce or amplify the transmission of pain signals through the gate, depending on the thoughts and emotions of a person.
Gate control theory in pain management
The gate control theory has brought about a drastic revolution in the field of pain management. The theory suggested that pain management can be achieved by selectively influencing the larger nerve fibers that carry non-pain stimuli. The theory has also paved way for more research on cognitive and behavioral approaches to achieve pain relief.
One of the tremendous advances in pain management research is the advent of Transcutaneous Electrical Nerve Stimulation (TENS). The gate control theory forms the basis of TENS. In this technique, the selective stimulation of the large diameter nerve fibers carrying non-pain sensory stimuli from a specific region nullifies or reduces the effect of pain signals from the region.
TENS is a non-invasive and inexpensive pain management approach that has been widely used for the treatment of chronic and intractable pain that are otherwise non-responsive to analgesics and surgical treatments. TENS is highly advantageous over pain medications in the aspect that it does not have the problem of drug interactions and toxicity.
Many other invasive and non-invasive electrical stimulation techniques have been found to be useful in various chronic pain conditions like arthritic pain, diabetic neuropathy, etc.
The theory has also been extensively studied in the treatment of chronic back pain and cancer pain. However, favorable results are not attained in some conditions and the long term efficacy of the techniques based on the theory is under question.
Nevertheless, the gate control theory has dramatically revolutionized the field of pain research and it has sown seeds for numerous studies that aim at presenting a pain-free lifestyle to the patients who suffer from chronic pain.
Harmful Effects of Pain
Regardless of its nature, pattern, or cause, pain that is inadequately treated has harmful effects beyond the suffering it causes.
EFFECTS OF ACUTE PAIN
Unrelieved acute pain can affect the pulmonary, cardiovascular, gastrointestinal, endocrine, and immune systems. The stress response (“neuroendocrine response to stress”) that occurs with trauma also occurs with other causes of severe pain.
This is particularly harmful in patients compromised by age, illness, or injury.
The stress response generally consists of increased metabolic rate and cardiac output, impaired insulin response, increased production of cortisol, and increased retention of fluids
• Increased heart rate and blood Pressure to Better perfusion of vital organs by Increasing cardiac output due to increased myocardial contractility
• Increased blood glucose level to increase available energy by increase in liver and muscle glycogen breakdown and increased breakdown of adipose tissue triglycerides
• Increase Mental acuity to increase Alert state by Increase in amount of blood shunted to the brain from the abdominal viscera and skin
• Dilated pupils to Increased awareness by Contraction of radial muscle of iris
• Increased ventilation (may be rapid and shallow) to Provision of oxygen for energy by Stimulation of respiratory center in medulla; bronchodilation
• Increased coagulability of Blood to Prevention of hemorrhage in event of trauma
EFFECTS OF CHRONIC PAIN
Like acute pain, chronic pain also has adverse effects. Suppression of the immune function associated with chronic pain may promote tumor growth. Also, chronic pain often results in depression and disability.
Although health care providers express concern about the large quantities of opioid medications required to relieve chronic pain in some patients, it is safe to use large doses of these medications to control progressive chronic pain. In fact, failure to administer adequate pain relief may be unsafe because of the consequences of unrelieved pain (McCracken & Iverson, 2001).
Regardless of how the patient copes with chronic pain, pain for an extended period can result in disability. Patients with a number of chronic pain syndromes report depression, anger, and fatigue (Meuser, Pietruck, Radruch et al., 2001; Raymond et al., 2001).
The patient may be unable to continue the activities and interpersonal relationships he or she engaged in before the pain began. Disabilities may range from curtailing participation in physical activities to being unable to take care of personal needs, such as dressing or eating.
The nurse needs to understand the effects of chronic pain on the patient and family and needs to be knowledgeable about pain relief strategies and appropriate resources to assist effectively with pain management.
FACTORS INFLUENCING THE PAIN RESPONSE
• Past experiences with pain• Anxiety• Culture• Age• Gender,• Expectations about pain relief.
Placebo Effect
A placebo effect occurs when a person responds to the medication or other treatment because of an expectation that the treatment will work rather than because it actually does so. Simply receiving a medication or treatment may produce positive effects.
The placebo effect results from the natural (endogenous) production of endorphins in the descending control system.
A patient’s positive expectations about treatment may increase the effectiveness of a medication or other intervention.
A person who is informed that a medication is expected to relieve pain is more likely to experience pain relief than one who is told that a medication is unlikely to have any effect.
Nursing Assessment of Pain
The pain assessment begins by observing the patient carefully, noting the patient’s overall posture and presence or absence of overt pain behaviors and asking the person to describe, in his or her own words, the specifics of the pain.
The words used to describe the pain may point toward the etiology. For example, the classic description of chest pain that results from a myocardial infarction includes pressure or squeezing on the chest. A detailed history should follow the initial description of pain.
CHARACTERISTICS OF PAIN
The factors to consider in a complete pain assessment are the:- 1. Intensity (pain tolerance)2. Timing (the nurse inquires about the onset, duration,
relationship between time and intensity, and whether there are changes in rhythmic patterns. The patient is asked if the pain began suddenly or increased gradually
3. Location4. Quality (burning, aching can be offered )5. Personal meaning6. Aggravating and alleviating factors, and 7. Pain behaviors
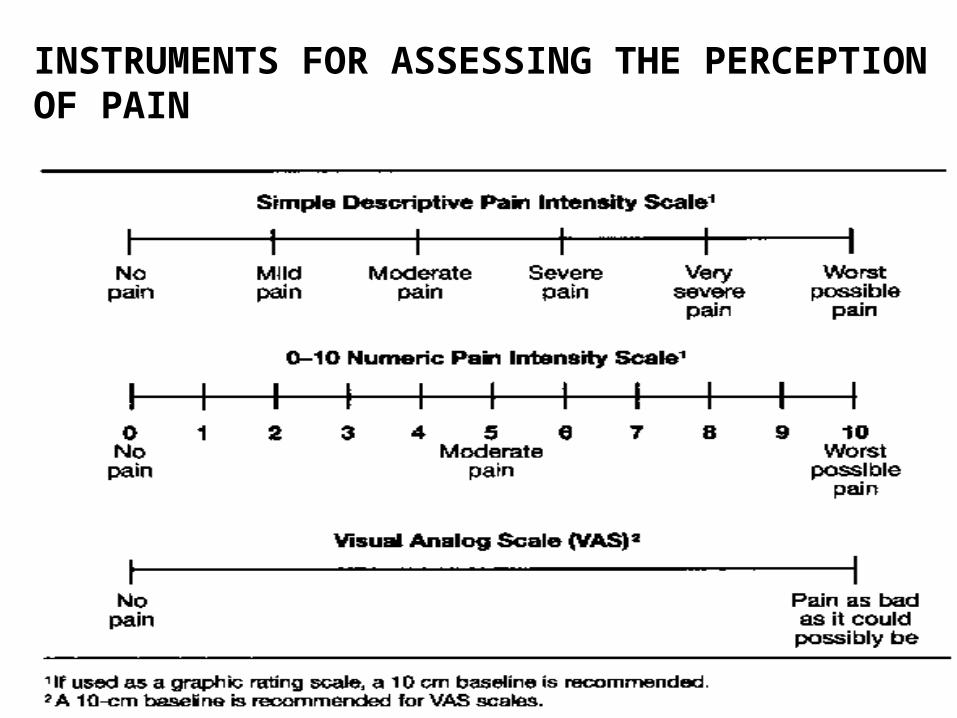
INSTRUMENTS FOR ASSESSING THE PERCEPTION OF PAIN
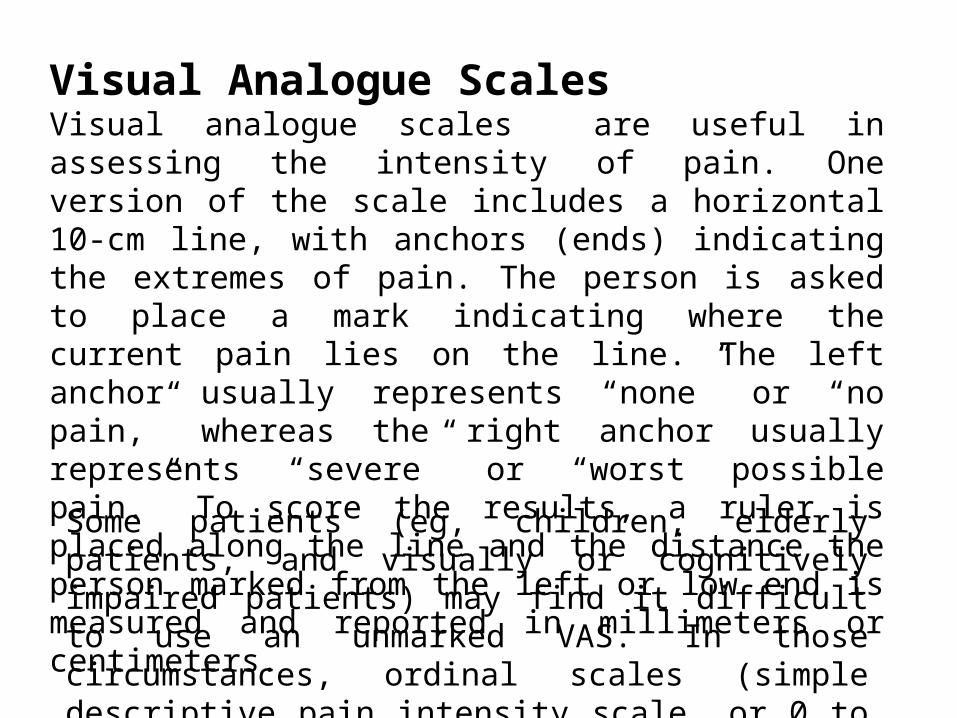
Visual Analogue ScalesVisual analogue scales are useful in assessing the intensity of pain. One version of the scale includes a horizontal 10-cm line, with anchors (ends) indicating the extremes of pain. The person is asked to place a mark indicating where the current pain lies on the line. The left anchor usually represents “none” or “no pain,” whereas the right anchor usually represents “severe” or “worst possible pain.” To score the results, a ruler is placed along the line and the distance the person marked from the left or low end is measured and reported in millimeters or centimeters.
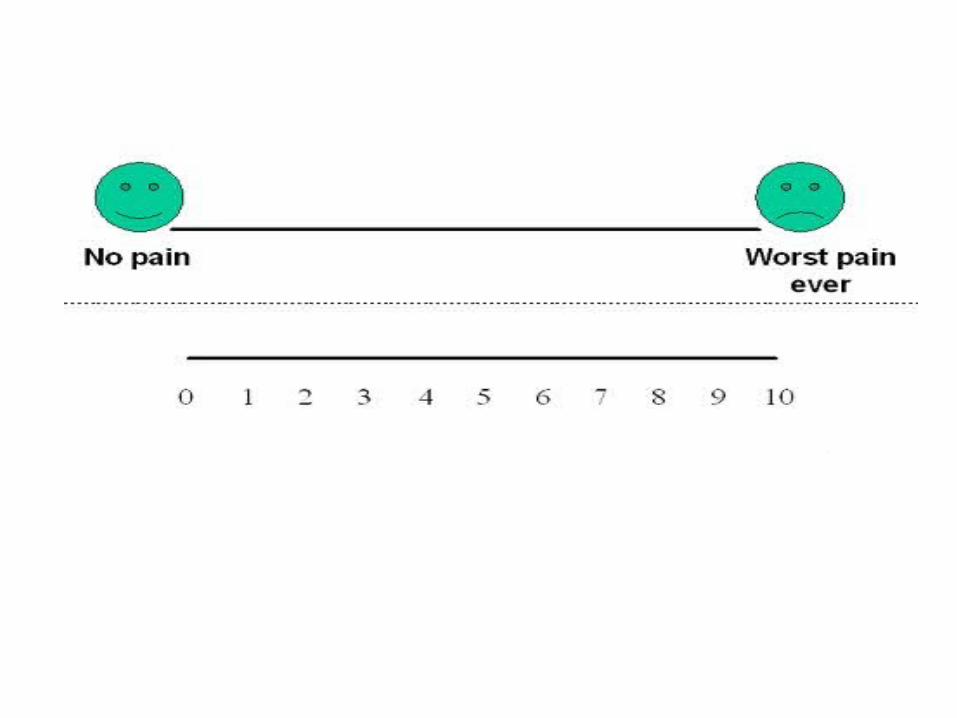
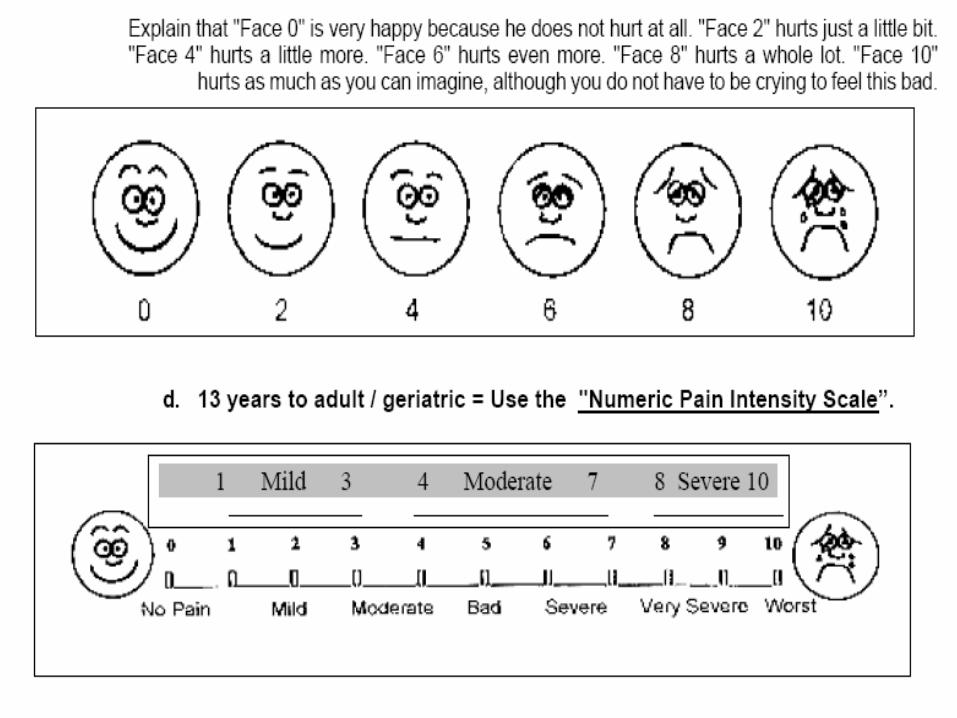
Some patients (eg, children, elderly patients, and visually or cognitively impaired patients) may find it difficult to use an unmarked VAS. In those circumstances, ordinal scales (simple descriptive pain intensity scale, or 0 to 10 numeric pain intensity scale) may be used.
Common Concerns and Misconceptions About Pain and Analgesia
• Complaining about pain will distract my doctor from his primary responsibility—curing my illness.• Pain is a natural part of aging.• I don’t want to bother the nurse—he/she is busy with other patients.• Pain medicine can’t really control pain.• People get addicted to pain medicine easily.• It is easier to put up with pain than with the side effects that come from pain medicine.• Good patients avoid talking about pain.• Pain builds character. It’s good for you.• Patients should expect to have pain; it’s part of almost every hospitalization.