Embed Size (px)
Citation preview

Page 1
The PepsiCo Foundation MeetingMarch 31, 2008
The PepsiCo Foundation
Addressing Malnutrition
Toby StillmanAdvisor, Emergency Health and Nutrition

2Page 2
• Review measures of undernutrition
• Review causes and consequences of undernutrition
• Introduce Save the Children’s operational approach to nutrition programming
– Children under the age of five
– School aged children
Outline

Page 3
Measures of Undernutrition Review
Stunting (Chronic)
Underweight(Both)
Wasting (Acute)
Index Height for Age
Weight for Age
Weight for Height or MUAC
Moderate
< -2 SD < -2 SD < -2 SD
Severe < - 3 SD < - 3SD < - 3SD

Page 4
Measures of Undernutrition Stunting:Height For Age

Page 5
Measures of Undernutrition Stunting:Weight For Age

Page 6
Measures of Undernutrition Wasting:Weight for Height
Marasmus (wasting) Kwashiorker (oedema)

Page 7
Measures of UndernutritionMid-upper Arm Circumference

Page 8
Measures of Undernutrition:Micronutrient deficiencies
• Vitamin A
• Zinc
• Iron
• Iodine

9Page 9
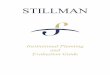
UndernutritionWhat are the Consequenses?
Pneumonia
19%
Diarrhea
17%
Malaria
8%Measles
4%
Aids
3%
Injuries
3%
Other
10%
Newborn
36%
Under-nutrition
• 35% to 55% of Child Mortality (children <5)
• Adult Size
• Intellectual Ability
• Economic Productivity
• Reproductive Performance
• Metabolic and Cardiovascular DiseaseIs build right? Why first bullet alone?

Page 10
UndernutritionWhen does it Happen?
First 2 years of life

Page 11
UndernutritionWhere does it Happen?

Page 12
Undernutrition Where does it Happen?
¾ of the world’s
underweight children reside in just 10
countries

Page 13
UndernutritionHow does it Happen?
Outcome Under-Nutrition
ImmediateCauses
InadequateDietary Intake Disease
UnderlyingHealth /NutritionCauses
Inadequate Care for Mothers
and Children
InsufficientAccess to Food
Lack of health services & unhealthy environment

Page 14
Addressing UndernutritionInterventions (1)

Page 15
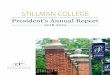
3947
4030
20
55
0102030405060708090
100
Exclusive BF Water,
Sanitation,
Hygiene
Treatment
(pneumonia)
Treatment
(diarrhea)
Oral
rehydration
therapy
Vitamin A
Addressing UndernutritionInterventions (2)
Source: Lancet Volume 362, PP. 65-71
The Coverage Gap

Page 16
Intended Impact:
Children are Healthy and Well-Nourished
Strategic Objective Increased Use of Key Health and Nutrition Practices and Services
Addressing UndernutritionSC Results Framework

Page 17
Addressing UndernutritionSC Priority Interventions
Practices Services
Nu
trition
• Immediate Breastfeeding
• Exclusive Breastfeeding through 6 months of age
• Timely introduction of appropriate complementary foods (Frequency of feeds, quality of feeds, etc.)
• Vitamin A supplementation (Maternal and Child)
• Iron supplementation
• Iodine supplementation
Health
• Proper disposal of feces
• Hand washing at appropriate times• Appropriate home care for Illness,
including oral rehydration therapy for children with diarrhea
• Timely referral of seriously ill children
• Measles immunization
• Timely appropriate treatment of ARI, diarrhea, malaria, and malnutrition including zinc therapy for diarrhea

Page 18
Intended Impact:
Children are Healthy and Well-Nourished
Strategic Objective Increased Use of Key Health and Nutrition Practices and
Services
Behaviors
Addressing UndernutritionSC Results Framework

Page 19
Strategic Objective Increased Use of Key Health and Nutrition Practices and
Services
Behaviors
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intermediate Result 3:Increased
Knowledge, Attitudes, and
Skills
Intermediate Result 4:
Enabling Social &
Policy Environment
Intermediate Result 2:
Increased Quality
Of Services
Intended Impact:
Children are Healthy and Well-Nourished
Addressing UndernutritionSC Results Framework

Page 20
Addressing UndernutritionMonitoring our Progress
Increased use of key health and nutrition practices and services
Improved Access
Strategies
Activities
Impacts
Outcomes
Time
Longer Term
Medium Term
Shorter Term
Children are healthy and well nourished% children <5 stunted
% children with diarrhea
% women exclusively breastfeeding
% children receiving timely care for illness
% population within 5 km of health care facility
Inputs & Outputs
# of community health workers trained in BCC
Improved Quality% children diagnosed and treated according to protocol
Improved KA&S% husbands supporting exclusive breastfeeding
Improved PoliciesNational policy on management of acute malnutrition in place

Page 21
Addressing UndernutritionSC Priority Interventions (1)
Practices Services
Nu
trition
• Immediate Breastfeeding
• Exclusive Breastfeeding through 6 months of age
• Timely introduction of appropriate complementary foods (Frequency of feeds, quality of feeds, etc.)
• Vitamin A supplementation (Maternal and Child)
• Iron supplementation
• Iodine supplementation
Health
• Proper disposal of feces
• Hand washing at appropriate times• Appropriate home care for Illness,
including oral rehydration therapy for children with diarrhea
• Timely referral of seriously ill children
• Measles immunization
• Timely appropriate treatment of ARI, diarrhea, malaria, and malnutrition including zinc therapy for diarrhea

Page 22
Intended Impact:
Children are Healthy and Well-Nourished
Addressing UndernutritionSC Priority Interventions (1)
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intermediate Result 3:Increased
Knowledge, Attitudes, and
Skills
Intermediate Result 4:
Enabling Social & Policy Environment
Intermediate Result 2:Increased
Quality Of Services
Strategic Objective Increased Use of Key Health and Nutrition Practices and
Services
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intermediate Result 3:Increased
Knowledge, Attitudes, and
Skills
Intervention: Timely introduction of appropriate complementary foods

Page 23
Complementary FeedingIR 3: Knowledge, Attitudes, and Skills
• Formative Research (E.g. TIPS, PD)
• Mother to mother support groups
• Growth monitoring and promotion
• Mass Communication
• PD/Hearth
Why does IR3 come before IR1 on next page?

Page 24
Complementary FeedingIR 1: Access to Food
• Resource transfers for the most vulnerable
• Food and/or nutrient supplements
• Micro-credit programs
• Food production and income generation (sustainable agriculture)
– Inputs and services: agricultural inputs, financial services, access to markets
– Improved practices: training and entrepreneurshipWhat should be under sustainable ag—
you trailed off, see word in green

Page 25
Addressing UndernutritionSC Priority Interventions (2)
Practices Services
Nu
trition
• Immediate Breastfeeding
• Exclusive Breastfeeding through 6 months of age
• Timely introduction of appropriate complementary foods (Frequency of feeds, quality of feeds, etc.)
• Vitamin A supplementation (Maternal and Child)
• Iron supplementation
• Iodine supplementation
Health
• Proper disposal of feces
• Hand washing at appropriate times• Appropriate home care for Illness,
including oral rehydration therapy for children with diarrhea
• Timely referral of seriously ill children
• Measles immunization
• Timely appropriate treatment of ARI, diarrhea, malaria, and malnutrition including zinc therapy for diarrhea
Why isn’t 2nd last bullet on bottom left—home care for diarrheaBolded under this intervention?

Page 26
Intended Impact:
Children are Healthy and Well-Nourished
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intermediate Result 3:Increased
Knowledge, Attitudes, and
Skills
Intermediate Result 4:
Enabling Social & Policy Environment
Intermediate Result 2:Increased
Quality Of Services
Strategic Objective Increased Use of Key Health and Nutrition Practices and
Services
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intervention: Timely appropriate care for ARI, Diarrhea, Malaria, and Malnutrition
Addressing UndernutritionSC Priority Interventions (2)

Page 27
Take services closer to the population
• The community health worker as prescriber for pneumonia, diarrhea, and malaria
“Community Case Management”
• Front-line health workers as providers of first choice for severe acute malnutrition
Community-based Management Of Acute Malnutrition
Timely, Appropriate CareIR 1: Access to Treatment

Page 28
SC Child Nutrition ProgramsProducing Results• Mozambique (2002 – 2007)
– Exclusive breastfeeding increased from 5% to 74%– Months of adequate food provisioning from 7.9 to 10.7 months
• Bangladesh (2005 – 2007)– Underweight reduced from 52% to 44% in first 2 years of program
• Vietnam – Immediate breastfeeding increased from 74% to 92%– Exclusive breastfeeding increased from 39% to 52%
• Bolivia (2002 – 2007)– Reduced stunting from 37% to 30.2% – Exclusive breastfeeding increased from 75% to 83%
• Nicaragua (2002 – 2007)– Reduced stunting from 20.5% to 9.6% – Exclusive breastfeeding increased from 37% to 84%

Page 29
The School-aged ChildOutcomes of Interest
Growth Educational Attainment
The equivalent of 200 million school years are lost each year in low income countries as a result of poor health and nutrition – World BankIs the build on this right—why words at top come in later?

Page 30
Intended Impact:
Children are well educated
The School Aged ChildSC Results Framework
Strategic Objective Increased Use of Key Health and Nutrition Practices and Services

Page 31
The School Aged ChildSC Priority Interventions
• Micronutrient supplementation: Vitamin A, Iron, Iodine
• De-worming
• Proper disposal of excreta and hand washing at appropriate times
• Health and Nutrition education
• Alleviation of short-term hunger

Page 32
Nutrition in the School-aged Child
Intermediate Result 1:Increased
Access to, & Availability of, Services and
Supplies
Intermediate Result 3:Increased
Knowledge, Attitudes, and
Skills
Intermediate Result 4:
Enabling Social & Policy Environment
Intermediate Result 2:Increased
Quality Of Services
Strategic Objective Increased Use of Key Health and Nutrition Practices and Services
Intended Impact:
Children are well educated