Embed Size (px)
Citation preview

Paediatric Renal Genetic Clinics
Adrian S. Woolf
University of Manchester

Children’s Hospital and University of Manchester, UK

The Nobel Prize in Physics 2010Andre Geim and Konstantin Novoselov
University of Manchester, UK
Discovered graphene…a new class of material…….2D atomic crystals

Clinical Importance of Malformations of the Human Kidney and Urinary Tract
● CHILDREN: Of the 800 children in the UK with renal
failure severe enough to need treatment with dialysis
and kidney transplantation, 40% have renal
malformations.
● ADULTS: Several thousands of UK adults who have
severe renal failure were born with abnormal kidneys.
● FETUSES: Renal tract malformations are among the
commonest anomalies detected upon fetal screening in
mid-gestation.

CLINICAL IMPORTANCE OF KIDNEY MALFORMATIONS
Three main histological varieties of
kidney malformations:
Hypoplasia (too few nephrons)
Dysplasia (undifferentiated kidney
sometimes with cysts)
Agenesis (absent kidney)

Worsening excretory function → →
Spectrum of Human Kidney Malformations

The Beginning of the Kidney:Ureteric Bud (UB)
Penetrates Renal Mesenchyme (RM)
RM
UB
Pitera JE et al Hum Mol Genet 17:3953-3964, 2008
Back in 1991, Genetics of Human Kidney Development Seemed Rather Simple….

TWO PAEDIATRIC RENAL GENETICS CLINICS
Between 2006 and 2009, I ran a clinic at Great Ormond Street Hospital, London with a focus
on ‘Genetics of Renal Tract Malformations' … A clinical genetics expert, Prof Raoul Hennekam
sat in with me and advised me. Since moving to Manchester in 2010, I have run a similar clinic with Dr Bronwyn Kerr

RENAL TRACT MALFORMATION/GENETICS CLINIC
• The idea was see whether we can help with genetic diagnosis and/or counselling in families with either:
• a child with a renal tract malformation and another organ involved, developmental delay, external dysmorphic features etc)
or• a child with a renal tract malformation and one
or more siblings or a parent with a renal tract malformation

CLINICAL REASONS TO MAKE GENETIC
DIAGNOSES OF RENAL TRACT MALFORMATIONS
● Finding mutations of developmental genes provides
families with reasons why disease occurred.
● Genetic diagnosis may suggest useful future health
screens and also external factors which can be modified
to enhance health.
● Better classification will optimise clinical follow-up
and allow better outcome studies.

SUMMARY OF CLINIC 2006-2009● Established as a clinical service rather than a
research clinic.
● A few relevant gene tests (especially HNF1B)
available on UK Genetic Testing Network and
comparative genomic hybridization by microarray
available at GOSH from 2008.
● 91 referrals (most from Paediatric Nephrologists
and Urologists), from 68 families.
● 27 children could be assigned to a recognised genetic
syndrome and/or were found to have a mutation
considered to be the cause of the renal malformation.


MULTICYSTIC DYSPLASTIC KIDNEY (MCDK)
Contralateral kidney
Often large (‘hypertrophy’)
Unilateral MCDK
Cysts → Atretic ureter →
Normal urinary bladder
FAMILY ONE
• JP – female now a teenager.• Antenatal diagnosis of right multicystic dysplastic
kidney: this involuted (spontaneously disappeared) after birth.
• Left solitary functioning kidney was ‘normal size’ (should be larger than normal) and was echobright on ultrasound scan.
• Between 9 and 12 years old, increasing weight centiles with normal fasting glucose and but raised insulin levels.
• Developed overt diabetes mellitus (non ketotoic) with blood sugar of 30 mM.

MULTICYSTIC DYSPLASTIC KIDNEY - RADIOLOGY
Shukunami K et al J Obstet Gynaecol24:458-459, 2004
Ultrasound scan32 weeks gestation
Postnatal renal isotope scan
‘Normal’ MCDK kidney (no uptake)
↑ ↑

INVOLUTION OF MULTICYSTIC DYSPLASTIC KIDNEYS
Neonatal ultrasound………..and two years later
● These massive structures usually ‘involute’ over weeks/months, prenatally or postnatally, often becoming undetectable by US

FAMILY ONE
● She has a heterozygous mutation of the
hepatocyte nuclear factor 1B (HNF1B)
transcription factor gene
● Predicted to result in aberrant splicing
● Parents have normal kidney US scans
●Mother has normal HNF1B; father not
yet tested.

RENAL CYSTS AND DIABETES SYNDROME (RCAD)
● RCAD is a relatively newly-recognised syndrome which was defined at the start of the 2000’s● Autosomal dominant or sporadic● Diabetes mellitus (MODY5) and uterus malformations● Renal disease resulting from abnormal development (but not classic ‘diabetic nephropathy’)● Renal cysts (histology showing cystic dysplasia and/or glomerulocystic type of polycystic kidney disease)● Hepatocyte Nuclear Factor 1Btranscription factor mutations (chromosome 17cen-q21.3)

HNF1BGENE EXPRESSED IN HUMAN EMBRYONIC KIDNEY
Kolatsi-Joannou M et al, J Am Soc Nephrol 12:2175-2180, 2001

HNF1B MUTATIONS CAN BE ASSOCIATED WITH DIABETES MELLITUS AND
PANCREAS HYPOPLASIA
Body of pancreas Head of pancreas
Haldorsen IS et al Diabet Med 25:782-787, 2008
NormalIndividual
HNF1Bmutation

HNF1BMUTATIONS• Great Ormond Street Nephrology Unit
• Since we started looking in 2001, up to 2007 we found 21 families with mutations of HNF1B
• Renal phenotypes are rather varied and include MCDK, solitary functioning kidney,
cystic dysplastic kidneys, pelviureteric junction obstruction and the glomerulocystic variety of polycystic kidneys

HNF1B Mutations not only Cause Renal Malformations but also Lead to
Abnormal Kidney Physiology after Birth
● Blood magnesium levels in children with renalmalformations
● Those with HNF1B mutations can have low blood magnesium levels
● HNF1B transactivates FXYD2, a gene implicated in magnesium handling in the distal convoluted tubule
Adalat S et al
J Am Soc Nephrol 20:1123-1131, 2009
FAMILY TWO• CK – male 5 years old• Presented with icthyosis and undescended
testicles• Found to have a hypoplastic left kidney and
normal sized right kidney• Two of his mother’s brothers also had
icthyosis• One of them had a solitary functioning
kidney and went into end-stage renal failure

FAMILY TWO• Index case and his two uncles have X-linked
Kallmann syndrome. Recessive condition, so female carriers are well
• The gene is expressed in the ureteric bud and collecting ducts, and also in the front of the brain
• Patients have anosmia, hypogonadotrophic hypogonadism and often have unilateral renal agenesis
• In the index case, the icthyosis is caused by a continguous gene deletion of the Steroid Sulphatase gene

EXPRESSION OF ANOSMIN-1
Glomerular basement membrane
Ureteric bud epithelia
Hardelin JP et al Dev Dyn 215:26-44, 1999
FAMILY THREE• LS – one year old
• Normal antenatal renal scan
• Respiratory distress
• Found to have raised creatinine and
bilateral hypoplastic kidneys
• Visual impairment with abnormal visual
evoked potentials
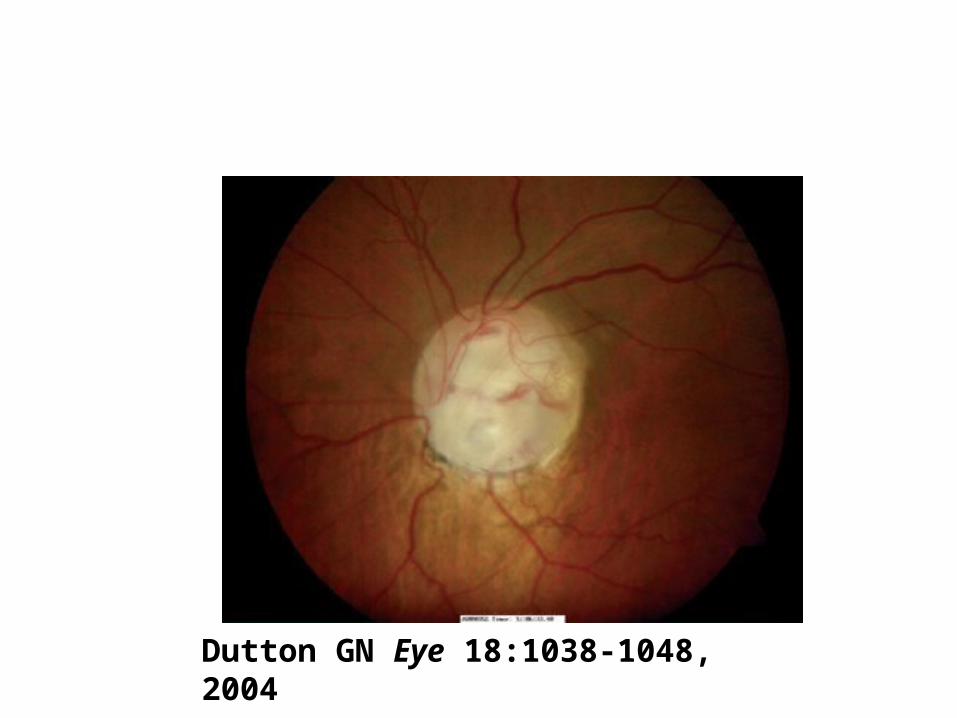
Dutton GN Eye 18:1038-1048, 2004

OPTIC NERVE COLBOMA
Dutton GN Eye 18:1038-1048, 2004

FAMILY THREE• Index case has heterozgous mutation of
the Paired Box 2 (PAX2) gene
• Renal coloboma syndrome
• Commonest renal lesions are hypoplasia; VUR and MCDK also reported
• Father of the index case has ‘slightly anomalous optic disc up’
BREAKTHROUGH IN 1995
Sanyanusin P et al Nature Genetics 9:358-364, 1995

RENAL COLOBOMA SYNDROME
Sanyanusin P et al Nature Genetics 9:358-364, 1995Eccles MR and Schimmenti LA Clin Genet 56:1-9, 1999
● Autosomal dominant inheritance● Highly variable presentation even in the same family● Optic nerve colobomas● Kidney hypoplasia or dysplasia● ? Secondary glomerular lesions● Ureter malformations

PAX2 TRANSCRIPTION FACTOR
Human fetal ureter Human fetal kidney
Winyard PJ et al J Clin Invest 98:451-459, 1996
PAX2 is expressed in the developing eye and renal tract. It prevents death of undifferentiated cells

FAMILY FOUR• ES – female 2 years old
• Presented with ‘hidden eyes’ (cyryptophthalmos), laryngeal web, fused fingers and toes, abnormal genitalia and malformed hindgut.
• Has a solitary, pelvic kidney
• Previous sibling – terminated and had bilateral renal agnenesis

FRASER SYNDROME
● Autosomal recessive
● Slavotinek and Tifft (J Med Genet
2005) reviewed 117 cases……..
Major criteria: cryptophthalmos,
syndactyly, abnormal genitalia,
and a sibling with Fraser syndrome

RENAL FEATURES OF FRASER SYNDROME
● Slavotinek and Tifft (J Med Genet 2005)
review of 117 cases…….
27% had ‘bilateral renal agenesis’
19% had ‘unilateral renal agenesis’
14% had renal ‘cystic dysplasia’
14% had renal ‘hypoplasia’
20% had absent or small urinary bladder

FRAS1 PROTEIN AND HOMOZYOUS MUTATIONS
(MacGregor L et al Nature Genet 34:203-208, 2003)
Human Blebbed mouse
FRAS1 codes for a 4007 amino acid protein

IN FRASER SYNDROME THE URETERIC BUD (UB) FAILS TO
PENETRATE RENAL MESENCHYME (RM)
RM
UB
Pitera JE et al Hum Mol Genet 17:3953-3964, 2008

FAMILY FIVE• AF – female index case now seven years old
• Potter sequence (oligohydramnios and
bilateral renal malformation) in two previous
siblings.
• Oligohydramnios at 33 weeks gestation.
• Subsequently she had a diagnosis of bilateral
renal hypoplasia/dysplasia
• Aged 3 years, her renal function was about
1/5th of normal.

THREE GENERATIONS AFFECTED BY KIDNEY
HYPOPLASIA AND DYSPLASIA
Kerecuk L et al Nephrol Dial Transplant 22:259-263, 2007
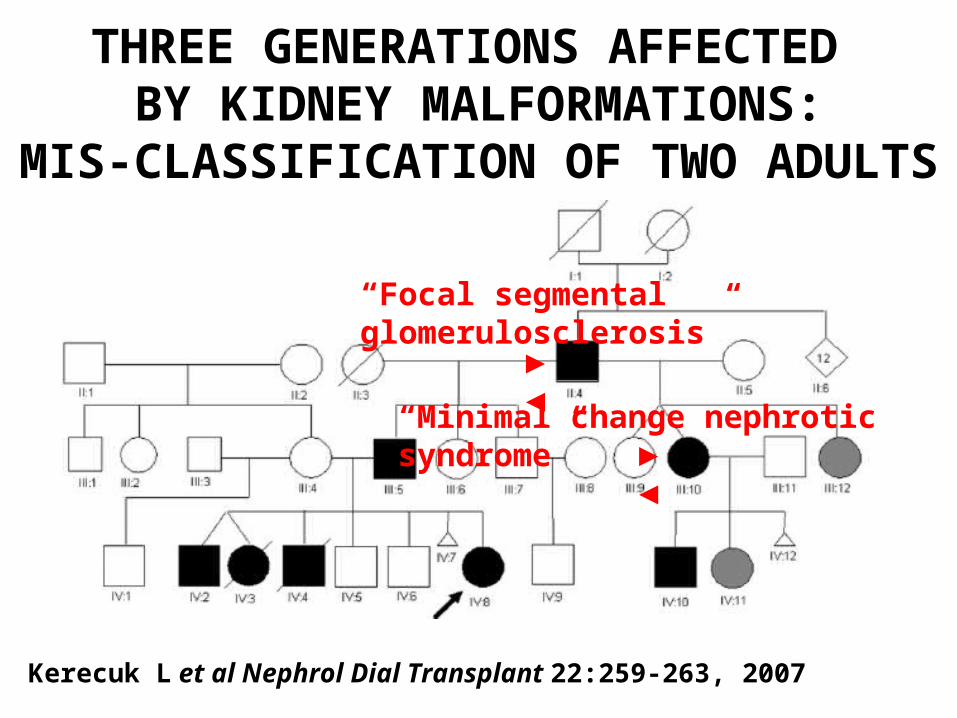
THREE GENERATIONS AFFECTED BY KIDNEY MALFORMATIONS:
MIS-CLASSIFICATION OF TWO ADULTS
Kerecuk L et al Nephrol Dial Transplant 22:259-263, 2007
► ◄
► ◄
“Focal segmental glomerulosclerosis”
“Minimal change nephrotic syndrome”

FAMILY FIVE• Looks like an autosomal dominant
disorder
• Very variable expression of kidney disease with fetal, childhood and adult presentations
• No syndromic clinical features
• Normal analyses of PAX2, HNF1 and EYA1 genes
• ? A new renal malformation gene ?

FINAL THOUGHTS AND QUESTIONS• Genetic testing may cost several hundred Euros
but……• Finding a mutation provides a family with an answer to
their often long-sought question “why was my child born with a kidney malformation?”
but…..• Should we perform genetic and/or renal ultrasound
screening of parents, siblings and the ‘next generation’.• Nephrologists need to link-up with clinical geneticists
for help with counselling • Why can the severity of renal malformation vary
considerably within one family? (‘modifying’ genes)














![Virginia Woolf[1]](https://img.pdfslide.us/doc/110x75/577cd2761a28ab9e78957fb1/virginia-woolf1.jpg)














