Embed Size (px)
Citation preview

Paediatric Procedural Sedationv.2011Royal Children HospitalECIICNVictorian Managed Insurance Authority

Program
Talk
Read handout on nitrous connections
Nitrous machine practical set up

Goal
Physical and psychological distress
Optimal environment for success
Analgesia
Anxiolysis
Amnesia
Awareness

Who is this talk for ?
Deliver quality care consistent with evidence base
Minimise risk and adverse events
Able to administer procedural sedation safely
Able to recognise and address undesirable events (rescue capacity)

http://www.youtube.com/watch?v=tGNyWDluELQ
http://www.youtube.com/watch?v=gmNwpJf1zUQ
Beware in asthmatics / RTI

General principles
Will my sedation plan achieve the best outcome for THIS patient ? Successful sedation doesn’t always guarantee
success of procedure or best outcome
What simple things can I do to reduce anxiety and need for sedation?
Preparation and post-procedural issues Patient, Staff, Place
Levels of sedationLevels of sedation
Minimal
Moderate
Deep
GA
American Society of Anesthesiologist (ASA) Classification (circle one)
1 A normal healthy patient
2 A patient with mild systemic disease
3 A patient with severe systemic disease
4 Moribund patient who is not expected to survive without the operation
*Class 3 or greater: Benefit of procedure outweighs risk of anesthesia

Reducing need for sedation
Early systemic analgesia Paracetamol, painstop, nurofen, IN fentanyl (1.5mcg/kg)
ALA (adr/lig/ameth) vs EMLA (lig/prilo)
Infants : Sucrose (5-8min), non-nutritional sucking
Non-pharmacological : distraction, balloon, bubbles, “safe person”, build rapport
Alternatives : glue, theatre (avoids repeat sedation)
Encourage coping behaviours
Modify environment
Parents
Reduce anxiety

Risk assessment
Disease factors Cerebral palsy, NM disorders, airway risk
(Prader-willi, Down’s)
Obvious contraindications / drug int
Previous sedation failure
Age < 1yo
IN fentanyl enhances NO2 sedation

The decision to sedate an unfasted patient for emergency procedures should be based on a careful assessment of the urgency of the procedure, the desired sedation depth, the fasting status and individual patient risk factors
The more urgent, the less fasting required, when less urgent, stick to minimum fasting guidelines
NO2: 2hrs Ketamine: 2hrs clear liquid
4hrs solids/milk
*consensus

Know your age-specific obs
Observations 5 minly if child deeply sedated 15 minly once improve
Discharge instructions Can child sit up/walk unaided? Tolerating fluids? Back to baseline consious state? Address carer concerns


N20
Inert colourless odourless
First synthesized in 1772 Joseph Priestley
“laughing gas” – Sir Humphry Davy
Promotes opioid peptide release from midbrain
Weak anaesthetic
Low solubility => rapid onset

N20 pros ?
Short acting, titratable
Fast onset 3-5 mins, fast offset
Inhalational analgesia and anasthesia
Safe
Requires a good seal with dedicated administrator

N20 cons ?
Vomiting (6% at home), light-headedness
Excessive sedation (caution URTI)
Requires cooperative child
Pregnant staff exclusion
Efficacy – not for all
Not useful for certain procedures
BM / Neurotoxicity, B12 def (rare)

N20 tips
Check supply
Check connections
Scavenger – medium flow
Suction
Bag : encourage blowing, hose : elephant nose
Additional O2 mask/BVM
Flavoured scents
Familiarise child with equipment
OK to apply obs postNO2 taking effect

Dose ?

Handout “Use of Nitrous Oxide in the ED”

“Vitamin K”
Dissociative anaesthetic
Hallucinatory reactions abused
Nightmares
Delirium

Ketamine pros
Major advantages Immobilisation Maintenance of airway and resp drive Profound analgesia
Mechanism of action
Cardiac stable

Ketamine cons?
Overall uncommon and minor Vomiting 8.6% Emergence 7.6% Airway / Resp 3.9%
No association with fasting
IV vs IM Longer onset and longer LOS with IM Balanced with distress of IV insertion

Respiratory
Resp depression (very young, rapid push)
Stridor (malpositioning of the airway)
Laryngospasm 0.002-0.3% incidence, 1/22 cases required ETT Idiosyncratic Airway support, PEEP and wait
Hypersalivation (X atropine, may increase events)

Emergence phenomenon
Range of behaviours
More common in adolescents, not an absolute CI
Responds well to midazolam but not as prophylaxis
Manage as per acute agitation

Others
Modest rise in HR, BP, metabolism
Hypertonicity, tremor, random movements Does not reflect depth of sedation
Seizures (case reports)
ICP/IOP elevation
Rash
Ataxia

CI
Children < one year / >12 years
Previous adverse reaction to ketamine
Active respiratory tract infection or disease
Procedures involving the lower airway or pharynx
Heart disease
Bowel obstruction
Psychosis / ADHD
Porphyria
Thyrotoxicosis
Unstable epilepsy
Glaucoma
Central nervous system masses, hydrocephalus

Practical tips
Full resus area with airway backup
Take time to explain to parents
Lights are on, but no one’s home
Saliva/tears not sign of pain or distress
Parents present
Rash spontaneously resolve
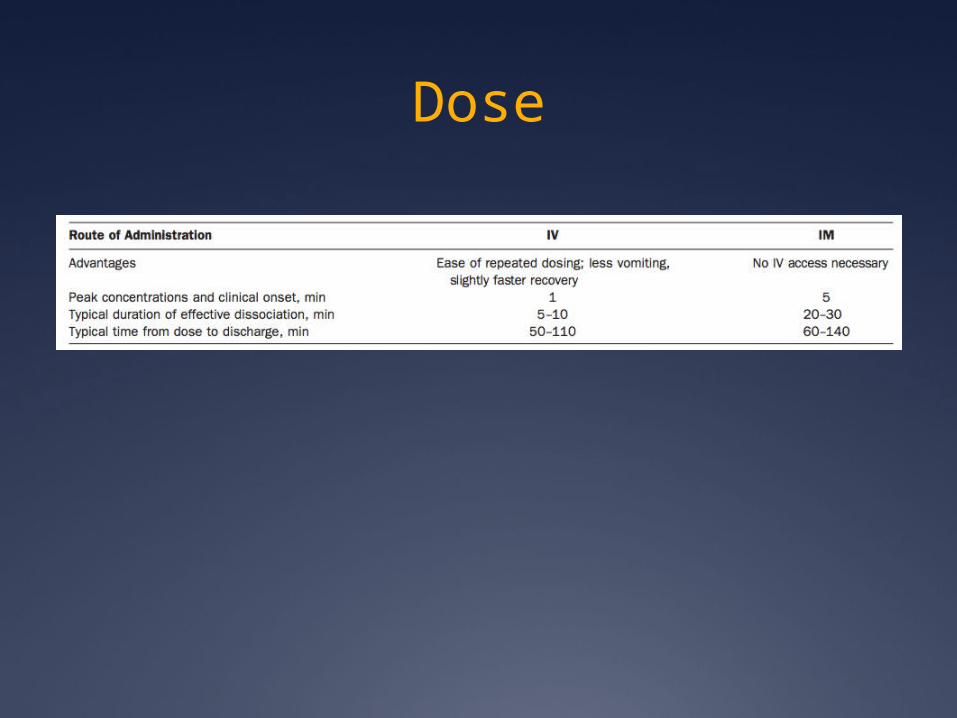
Dose








![procedural sedation 2009.ppt [Read-Only] · PDF fileProcedural Sedation Emergency Principles Brian Levine, MD ... Ketamine • “the safest ... procedural sedation 2009.ppt](https://img.pdfslide.us/doc/110x75/5abe33597f8b9ad8278cdc83/procedural-sedation-2009ppt-read-only-sedation-emergency-principles-brian-levine.jpg)