Embed Size (px)
Citation preview

Overview of Paediatric HIV Treatment and
Prevention: From Then to Now
Peter Mugyenyi,
Joint Clinical Research Centre
Kampala, Uganda

Outline
• The plight of HIV infected children (1980s and 1990s)
• Trends in new HIV infections and number of children treated
• Role of Global, Regional and National Efforts
• Sharing Uganda experience
• New Challenges and looking to the future

The plight of HIV infected children (1980s and 1990s)
• HIV access campaigns prioritized adults.
• High death rates of parents left up to 10 million orphans - many infected (UNAIDS)
• Initial access to ART reached only a tiny minority of adults and much fewer children
• Pharmaceutical companies did not invest much in paediatric ARV formulations

Equity and moral imperative
• Continuing suffering and horror when effective therapy was available (but unaffordable).

Significant Global ResponseStarted late
• 2003: President Bush announces Presidents Emergency Program for AIDS relief (PEPFAR
• 2004: Global Fund to fight AIDS, Tuberculosis and Malaria

Early HIV treatment studies were mainly among adults
• The children responded optimally to ART clinically, immunologically and virologically
– Just like in resource rich settings
– Similarly in urban and rural settings
– To both 1st and 2nd line ART

Recently the face of HIV Infection has changed with
ART
Then Now

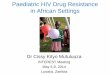
Numbers of Children on ART in Uganda
(2006 – 2014)
Source: MOH: Status of ART services in Uganda – Dec 2014
5,00
0
7,80
0
8,53
2
13,4
13
17,2
78 26
,69
9
35,4
43
43
,48
1 58,8
84
13%
18%20%
32%
22%
25%
35%
22%
32%
0%
5%
10%
15%
20%
25%
30%
35%
40%
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
2006 2007 2008 2009 2010 2011 2012 2013 2014
Number on ART % eligible on ART

Trends in AIDS-related deaths
0
50
100
150
200
250
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
(Th
ou
san
ds)
Estimated number of AIDS-related deaths, in 0 – 4yr age group, 2001-2014
Source: UNAIDS 2014 HIV and AIDS estimates, July 2015

New Infection trends
Source: UNAIDS. On the fast track to an AIDS free generation. 2016

Trends in AIDS-related deaths
0
50
100
150
200
250
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
(Th
ou
san
ds)
Estimated number of AIDS-related deaths, by 5-year age groups, 2001-2014
Age 0-4 Age 5-9 Age 10-14 Age 15-19 Age 20-24
Source: UNAIDS 2014 HIV and AIDS estimates, July 2015
AIDS-related deaths are increasing in adolescents aged 10-19 years

Disparities Between Adults And Children Percentage of ART Coverage Among Eligible Adults, Children and All
Ages in the 22 Global Plan Priority Countries (2012)
Source: UNAIDS, UNICEF and WHO, 2013 Global AIDS Response Progress Reporting. Note: Some numbers do not add up due to rounding. The coverage estimate is based on the estimated unrounded number of children receiving and eligible for ART.

Strategy to end AIDS epidemic:how are children doing?

Special issues and targets for ending Paediatric HIV
• Need for systematically addressing constraints peculiar to adolescents and children

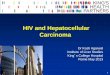
Implementation of Test and Treat: 74% increase in number of children
newly initiated on ART
Q1 2013 Q2 2013 Q3 2013 Q4 2013 Q1 2014 Q2 2014 Q3 2014 Q4 2014
5-14 yr 1158 1957 1167 983 2200 3306 4105 2719
2-4 yr 601 694 793 574 822 1048 1362 1125
<2 yr 819 979 1096 803 910 859 917 892
0
1000
2000
3000
4000
5000
6000
7000
Fig: Number of Children newly initiated on ART
Source: MOH – Uganda, May 2015
Implementation of Test and Treat

Viral Suppression in Test and Treat Era in Uganda
Proportion of children initiated on ART during the test and treat implementation
who are viral suppressed by age
Age ( years)
Number received viral
load test
Number with
suppressed viral load
% with suppressed
viral load
< 2 43 35 81%
2-4 168 128 76%
5-9 246 211 86%
10-14 336 289 86%
Overall 793 663 84%
Source: MOH – Uganda, May 2015

Access To Virologic HIV Testing(Early Infant Diagnosis) 2012
*Lesotho data represents 2011 coverage dataSource: UNAIDS, UNICEF and WHO, 2013 Global AIDS Response Progress Reporting, and UNAIDS modeling2012 HIV and AIDS estimates.

Results of early infant HIV testing in Kampala
PMTCT exposure Test status Number Percent
Yes
Negative 436 84.3
Positive 81 15.7
Total 517 100
No
Negative 174 72.8
Positive 65 27.2
Total 239 100
Uganda MOH 2006

Major issues to address
• Rate of Mother to Child transmission of HIV (6,100 infants are newly infected in 2015) remains unacceptably high,
• Number of children accessing timely EID services remains too low
• Retention on ART and viral suppression especially for under 5s (<70%) - low
Uganda MOH

Critical requirements to end Paediatric AIDS
99%
Pregnant Mothers
99%
EID for all children of
HIV infected mums
99%
ART drugs appropriate
to age

Finding the children:
potential opportunities to offer HIV testing
Sources: Fergusson et al, 2007; Hesseling et al. 2009; Ferrand et al. 2010; Cohen et al. 2010

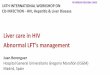
New challenge: Adolescents
0
100,000
200,000
300,000
400,000
500,000
600,000
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Estimated number of new HIV infections among children aged 0–14, adolescents aged 15–19 and young people aged 20–24, Global, 2001–2014
Children aged 0-14 Adolescents aged 15-19 Young people aged 20-24
Source: UNAIDS 2014 HIV and AIDS estimates, July 2015
New Infection trends: drop in adolescents not as sharp as for younger children

Adolescent specific interventions needed
• Adolescent friendly services
• Psychosocial support
• Peer counseling
• Sexual and reproductive health
• Skills training
• Community support
• Transition to adult clinics
Photos: JCRC Stigmaless band; Adolescent peer support meetings

Ending Paediatric AIDS epidemic achievable by identifying and addressing gaps
• Extend both ante-natal and EID coverage to all
• Maximize testing opportunities (e.gvaccination, clinics etc.) to cover children who missed out on EID
• Strengthen diagnostic, treatment and VL monitoring.
• Communication with policy makers and program partners to secure renewed commitment to 90-90-90

Acknowledgements
1. UNAIDS
2. JCRC research database
3. Uganda MOH AIDS control program
4. Dr Victor Musiime; Joint Clinical research
Centre/Makerere University

Thank you!