Embed Size (px)
Citation preview
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
1
Paediatric Empirical Antimicrobial Guidance for Infections in Hospital
This guidance is for empirical treatment. Alternative antibiotics may be required if specific pathogens are identified or there is failure to respond.
Contact microbiology for advice.
Samples should be taken for culture sensitivity testing whenever possible and preferably before the administration of antibiotics. If appropriate, modify initial therapy once sensitivity results are available.
Viral infections and self-limiting illnesses should not be treated with antibiotics.
The route of administration depends on the severity of the infection. Review the need for IV treatment after 48 hours and then at least every 24
hours, changing to oral therapy as soon as possible. See appendix 1
The duration of therapy depends on the nature of the infection and the response to treatment. Use the shortest, effective duration of treatment.
All antimicrobial prescriptions should have a review date or duration of treatment stated on the prescription chart The indication for prescribing antibiotics MUST be clearly documented in the patients’ medical notes
Consider whether monitoring of drug levels is required e.g. Gentamicin and Vancomycin.
The dose of an antimicrobial varies according to age, weight, hepatic/renal function and severity of infection. Refer to current BNF for
children for dosing guidance and also for any potential drug interactions. It is important to clarify the history of a reported penicillin allergy. Those with a type 1 allergy to penicillin maybe prescribed
cephalosporins or carbapenems for severe infections under close observation. Seek microbiology advice if also history of severe allergy to cephalosporins and/or carbapenems. See appendix 2.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
2
Community Acquired Sepsis
Recognition of Sepsis
A child with suspected or proven infection AND at least 2 of the following:
● Core temperature <36°C or >38°C (observed or reported in previous 4 hours)
● Inappropriate tachycardia (Refer to National PEWS)
● Altered mental state (including: sleepiness / irritability / lethargy / floppiness)
● Reduced peripheral perfusion / prolonged central capillary refill / cool or mottled peripheries
Reduce Threshold for Sepsis
Some children are at higher risk of sepsis. You may consider treatment with fewer signs than above. These include, but are not
restricted to:
● Infants under 3 months
● Immunosuppressed / immunocompromised / chemotherapy / long term steroids
● Recent surgery
● Indwelling devices / lines
● Complex neurodisability or other long term conditions (may not present with high PEWS but observations may vary from their baseline)
● High index of clinical suspicion
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
3
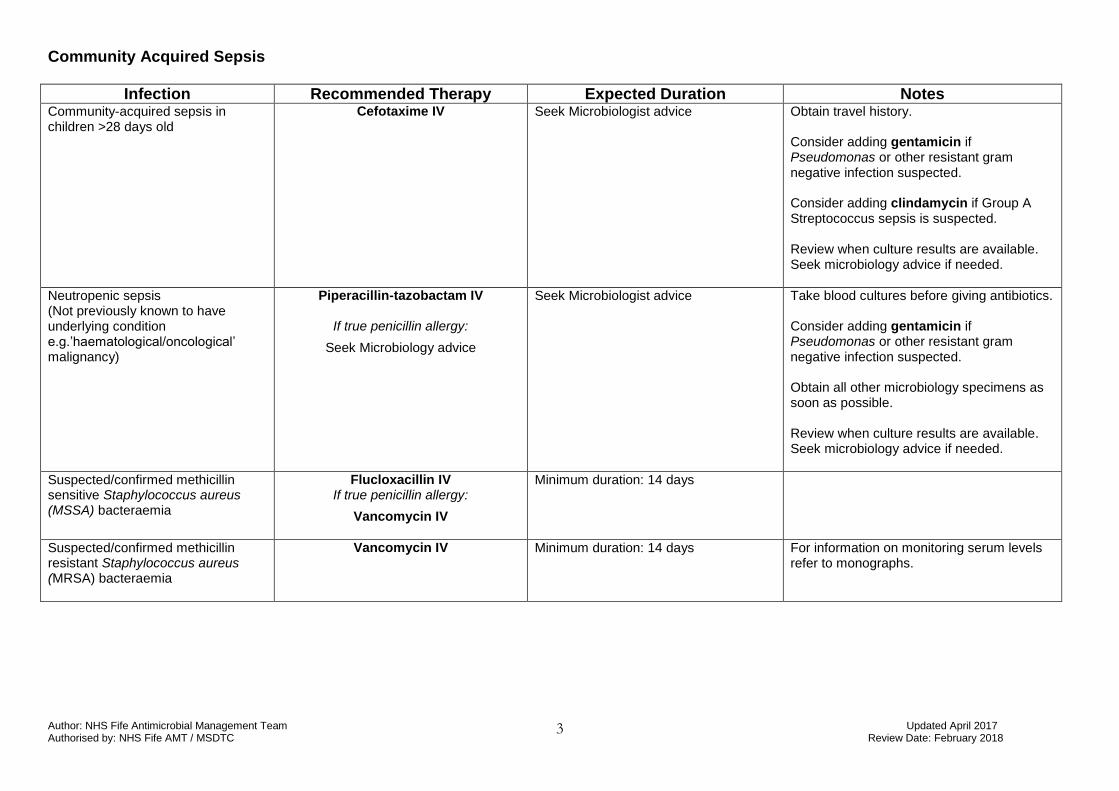
Community Acquired Sepsis
Infection Recommended Therapy Expected Duration Notes Community-acquired sepsis in children >28 days old
Cefotaxime IV
Seek Microbiologist advice Obtain travel history. Consider adding gentamicin if Pseudomonas or other resistant gram negative infection suspected. Consider adding clindamycin if Group A Streptococcus sepsis is suspected. Review when culture results are available. Seek microbiology advice if needed.
Neutropenic sepsis (Not previously known to have underlying condition e.g.’haematological/oncological’ malignancy)
Piperacillin-tazobactam IV
If true penicillin allergy:
Seek Microbiology advice
Seek Microbiologist advice Take blood cultures before giving antibiotics. Consider adding gentamicin if Pseudomonas or other resistant gram negative infection suspected. Obtain all other microbiology specimens as soon as possible. Review when culture results are available. Seek microbiology advice if needed.
Suspected/confirmed methicillin sensitive Staphylococcus aureus (MSSA) bacteraemia
Flucloxacillin IV If true penicillin allergy:
Vancomycin IV
Minimum duration: 14 days
Suspected/confirmed methicillin resistant Staphylococcus aureus (MRSA) bacteraemia
Vancomycin IV Minimum duration: 14 days
For information on monitoring serum levels refer to monographs.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
4
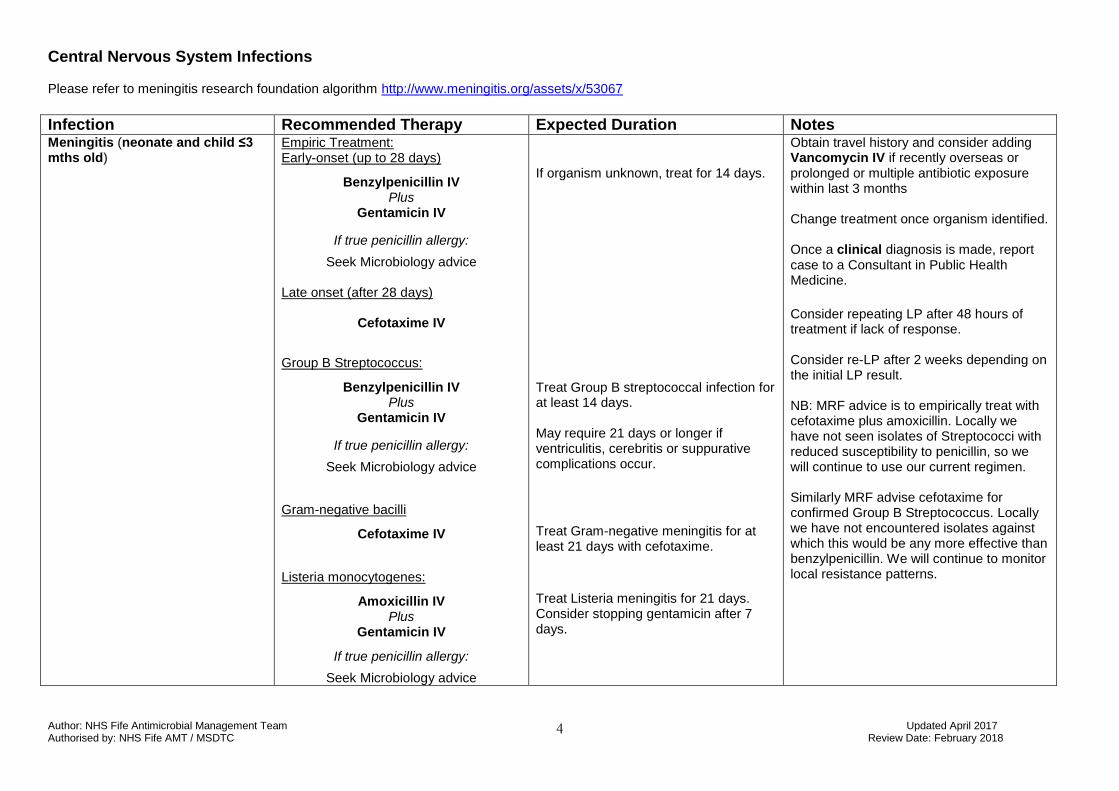
Central Nervous System Infections
Please refer to meningitis research foundation algorithm http://www.meningitis.org/assets/x/53067
Infection Recommended Therapy Expected Duration Notes Meningitis (neonate and child ≤3 mths old)
Empiric Treatment: Early-onset (up to 28 days)
Benzylpenicillin IV Plus
Gentamicin IV
If true penicillin allergy:
Seek Microbiology advice Late onset (after 28 days)
Cefotaxime IV
Group B Streptococcus:
Benzylpenicillin IV Plus
Gentamicin IV
If true penicillin allergy:
Seek Microbiology advice
Gram-negative bacilli
Cefotaxime IV
Listeria monocytogenes:
Amoxicillin IV Plus
Gentamicin IV
If true penicillin allergy:
Seek Microbiology advice
If organism unknown, treat for 14 days. Treat Group B streptococcal infection for at least 14 days. May require 21 days or longer if ventriculitis, cerebritis or suppurative complications occur.
Treat Gram-negative meningitis for at least 21 days with cefotaxime.
Treat Listeria meningitis for 21 days. Consider stopping gentamicin after 7 days.
Obtain travel history and consider adding Vancomycin IV if recently overseas or prolonged or multiple antibiotic exposure within last 3 months Change treatment once organism identified. Once a clinical diagnosis is made, report case to a Consultant in Public Health Medicine.
Consider repeating LP after 48 hours of treatment if lack of response. Consider re-LP after 2 weeks depending on the initial LP result. NB: MRF advice is to empirically treat with cefotaxime plus amoxicillin. Locally we have not seen isolates of Streptococci with reduced susceptibility to penicillin, so we will continue to use our current regimen. Similarly MRF advise cefotaxime for confirmed Group B Streptococcus. Locally we have not encountered isolates against which this would be any more effective than benzylpenicillin. We will continue to monitor local resistance patterns.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
5
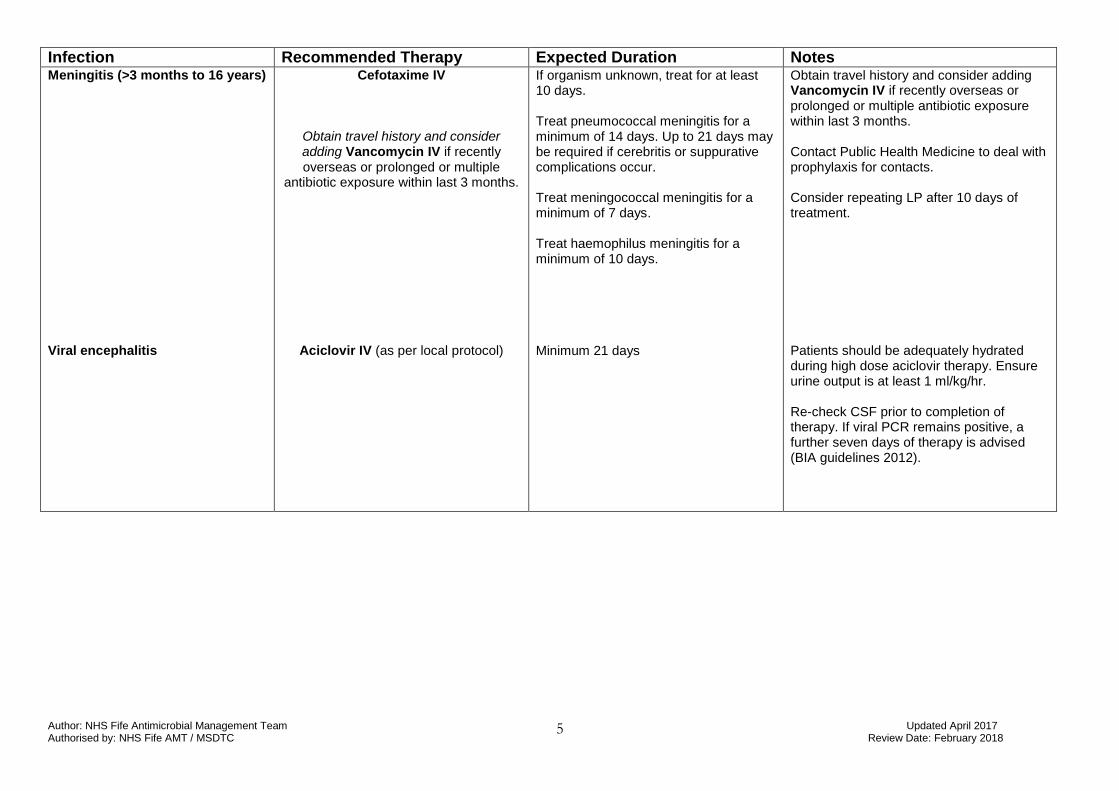
Infection Recommended Therapy Expected Duration Notes Meningitis (>3 months to 16 years) Viral encephalitis
Cefotaxime IV
Obtain travel history and consider adding Vancomycin IV if recently overseas or prolonged or multiple
antibiotic exposure within last 3 months.
Aciclovir IV (as per local protocol)
If organism unknown, treat for at least 10 days. Treat pneumococcal meningitis for a minimum of 14 days. Up to 21 days may be required if cerebritis or suppurative complications occur. Treat meningococcal meningitis for a minimum of 7 days. Treat haemophilus meningitis for a minimum of 10 days. Minimum 21 days
Obtain travel history and consider adding Vancomycin IV if recently overseas or prolonged or multiple antibiotic exposure within last 3 months. Contact Public Health Medicine to deal with prophylaxis for contacts. Consider repeating LP after 10 days of treatment. Patients should be adequately hydrated during high dose aciclovir therapy. Ensure urine output is at least 1 ml/kg/hr. Re-check CSF prior to completion of therapy. If viral PCR remains positive, a further seven days of therapy is advised (BIA guidelines 2012).
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
6
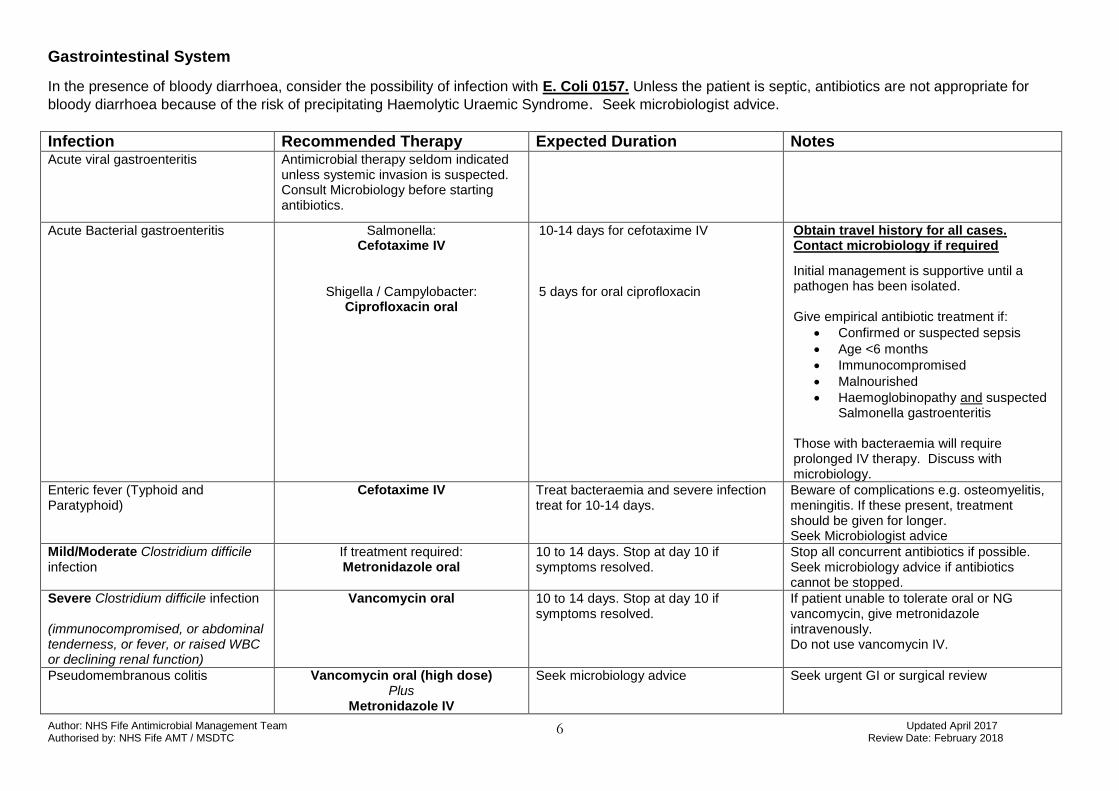
Gastrointestinal System
In the presence of bloody diarrhoea, consider the possibility of infection with E. Coli 0157. Unless the patient is septic, antibiotics are not appropriate for
bloody diarrhoea because of the risk of precipitating Haemolytic Uraemic Syndrome. Seek microbiologist advice.
Infection Recommended Therapy Expected Duration Notes Acute viral gastroenteritis Antimicrobial therapy seldom indicated
unless systemic invasion is suspected. Consult Microbiology before starting antibiotics.
Acute Bacterial gastroenteritis
Salmonella: Cefotaxime IV
Shigella / Campylobacter: Ciprofloxacin oral
10-14 days for cefotaxime IV 5 days for oral ciprofloxacin
Obtain travel history for all cases. Contact microbiology if required
Initial management is supportive until a pathogen has been isolated. Give empirical antibiotic treatment if:
Confirmed or suspected sepsis
Age <6 months
Immunocompromised
Malnourished
Haemoglobinopathy and suspected Salmonella gastroenteritis
Those with bacteraemia will require prolonged IV therapy. Discuss with microbiology.
Enteric fever (Typhoid and Paratyphoid)
Cefotaxime IV Treat bacteraemia and severe infection treat for 10-14 days.
Beware of complications e.g. osteomyelitis, meningitis. If these present, treatment should be given for longer. Seek Microbiologist advice
Mild/Moderate Clostridium difficile infection
If treatment required: Metronidazole oral
10 to 14 days. Stop at day 10 if symptoms resolved.
Stop all concurrent antibiotics if possible. Seek microbiology advice if antibiotics cannot be stopped.
Severe Clostridium difficile infection (immunocompromised, or abdominal tenderness, or fever, or raised WBC or declining renal function)
Vancomycin oral 10 to 14 days. Stop at day 10 if symptoms resolved.
If patient unable to tolerate oral or NG vancomycin, give metronidazole intravenously. Do not use vancomycin IV.
Pseudomembranous colitis
Vancomycin oral (high dose) Plus
Metronidazole IV
Seek microbiology advice Seek urgent GI or surgical review
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
7
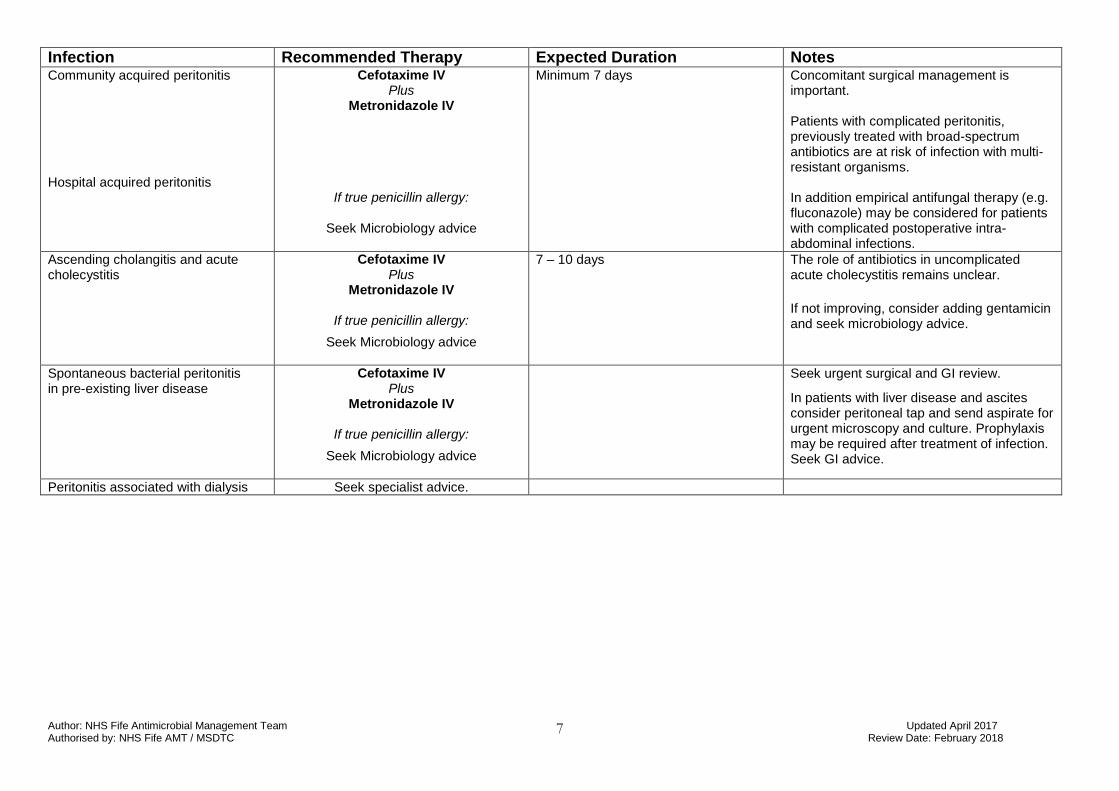
Infection Recommended Therapy Expected Duration Notes Community acquired peritonitis Hospital acquired peritonitis
Cefotaxime IV Plus
Metronidazole IV
If true penicillin allergy:
Seek Microbiology advice
Minimum 7 days Concomitant surgical management is important. Patients with complicated peritonitis, previously treated with broad-spectrum antibiotics are at risk of infection with multi-resistant organisms. In addition empirical antifungal therapy (e.g. fluconazole) may be considered for patients with complicated postoperative intra-abdominal infections.
Ascending cholangitis and acute cholecystitis
Cefotaxime IV Plus
Metronidazole IV
If true penicillin allergy:
Seek Microbiology advice
7 – 10 days The role of antibiotics in uncomplicated acute cholecystitis remains unclear.
If not improving, consider adding gentamicin and seek microbiology advice.
Spontaneous bacterial peritonitis in pre-existing liver disease
Cefotaxime IV Plus
Metronidazole IV
If true penicillin allergy:
Seek Microbiology advice
Seek urgent surgical and GI review.
In patients with liver disease and ascites consider peritoneal tap and send aspirate for urgent microscopy and culture. Prophylaxis may be required after treatment of infection. Seek GI advice.
Peritonitis associated with dialysis Seek specialist advice.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
8
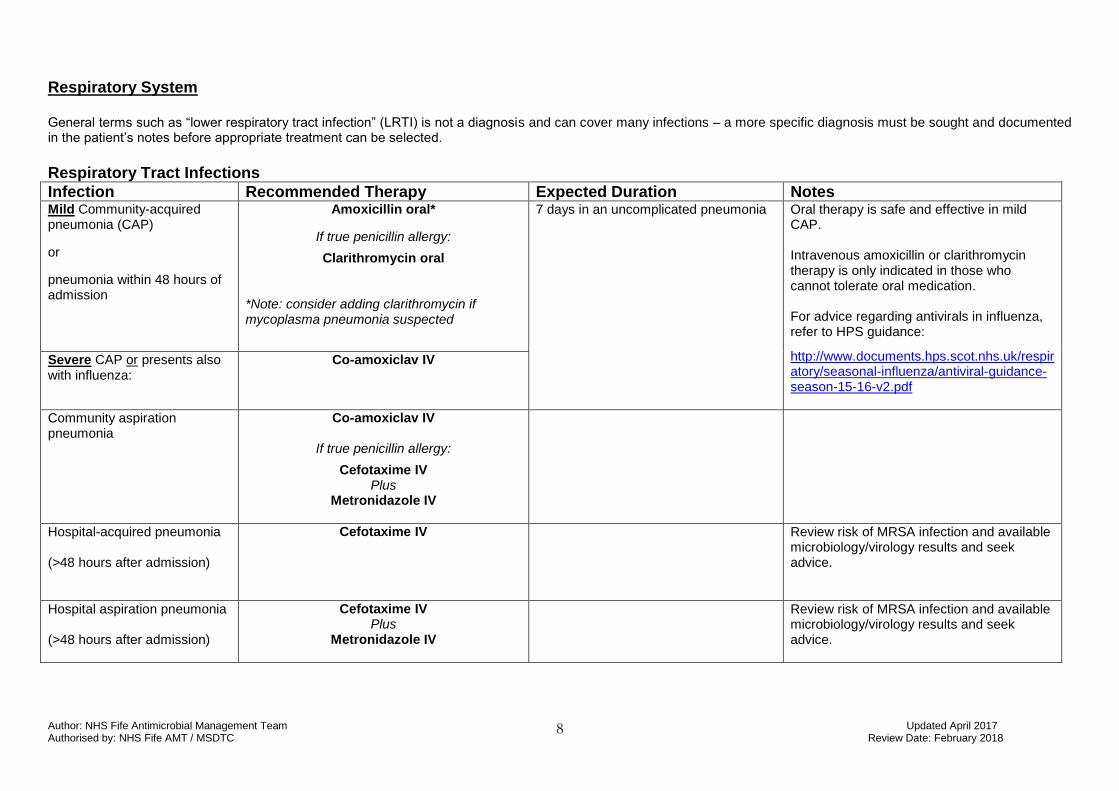
Respiratory System
General terms such as “lower respiratory tract infection” (LRTI) is not a diagnosis and can cover many infections – a more specific diagnosis must be sought and documented in the patient’s notes before appropriate treatment can be selected.
Respiratory Tract Infections
Infection Recommended Therapy Expected Duration Notes Mild Community-acquired pneumonia (CAP)
or
pneumonia within 48 hours of admission
Amoxicillin oral*
If true penicillin allergy:
Clarithromycin oral
*Note: consider adding clarithromycin if mycoplasma pneumonia suspected
7 days in an uncomplicated pneumonia
Oral therapy is safe and effective in mild CAP. Intravenous amoxicillin or clarithromycin therapy is only indicated in those who cannot tolerate oral medication. For advice regarding antivirals in influenza, refer to HPS guidance:
http://www.documents.hps.scot.nhs.uk/respiratory/seasonal-influenza/antiviral-guidance-season-15-16-v2.pdf
Severe CAP or presents also with influenza:
Co-amoxiclav IV
Community aspiration pneumonia
Co-amoxiclav IV
If true penicillin allergy:
Cefotaxime IV Plus
Metronidazole IV
Hospital-acquired pneumonia (>48 hours after admission)
Cefotaxime IV
Review risk of MRSA infection and available microbiology/virology results and seek advice.
Hospital aspiration pneumonia (>48 hours after admission)
Cefotaxime IV Plus
Metronidazole IV
Review risk of MRSA infection and available microbiology/virology results and seek advice.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
9
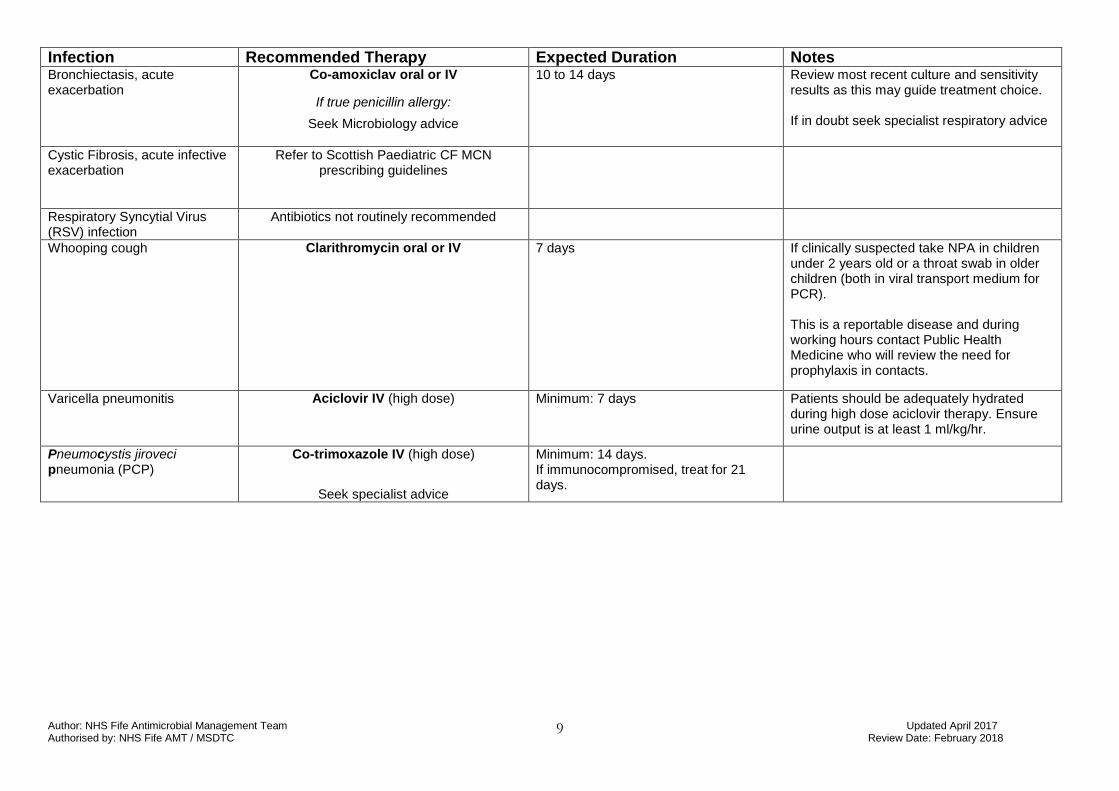
Infection Recommended Therapy Expected Duration Notes Bronchiectasis, acute exacerbation
Co-amoxiclav oral or IV
If true penicillin allergy:
Seek Microbiology advice
10 to 14 days
Review most recent culture and sensitivity results as this may guide treatment choice. If in doubt seek specialist respiratory advice
Cystic Fibrosis, acute infective exacerbation
Refer to Scottish Paediatric CF MCN prescribing guidelines
Respiratory Syncytial Virus (RSV) infection
Antibiotics not routinely recommended
Whooping cough
Clarithromycin oral or IV
7 days
If clinically suspected take NPA in children under 2 years old or a throat swab in older children (both in viral transport medium for PCR). This is a reportable disease and during working hours contact Public Health Medicine who will review the need for prophylaxis in contacts.
Varicella pneumonitis Aciclovir IV (high dose)
Minimum: 7 days Patients should be adequately hydrated during high dose aciclovir therapy. Ensure urine output is at least 1 ml/kg/hr.
Pneumocystis jiroveci pneumonia (PCP)
Co-trimoxazole IV (high dose)
Seek specialist advice
Minimum: 14 days. If immunocompromised, treat for 21 days.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
10
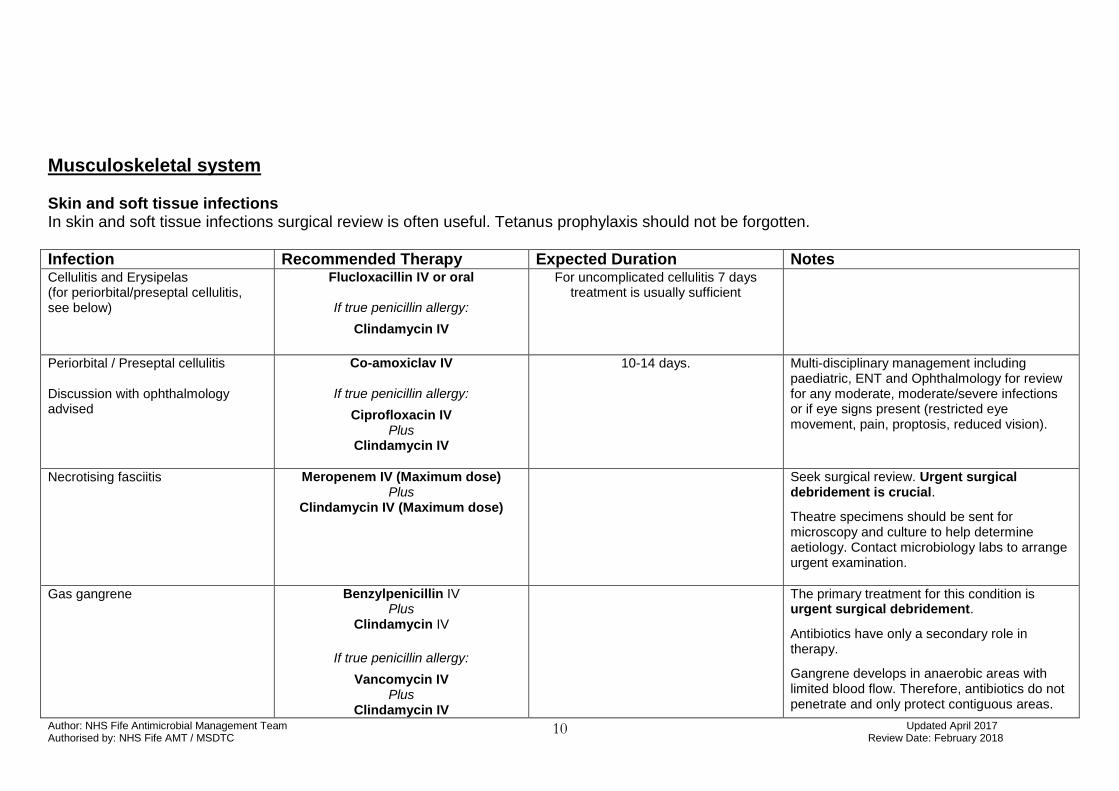
Musculoskeletal system
Skin and soft tissue infections In skin and soft tissue infections surgical review is often useful. Tetanus prophylaxis should not be forgotten.
Infection Recommended Therapy Expected Duration Notes Cellulitis and Erysipelas (for periorbital/preseptal cellulitis, see below)
Flucloxacillin IV or oral
If true penicillin allergy:
Clindamycin IV
For uncomplicated cellulitis 7 days treatment is usually sufficient
Periorbital / Preseptal cellulitis Discussion with ophthalmology advised
Co-amoxiclav IV
If true penicillin allergy:
Ciprofloxacin IV Plus
Clindamycin IV
10-14 days. Multi-disciplinary management including paediatric, ENT and Ophthalmology for review for any moderate, moderate/severe infections or if eye signs present (restricted eye movement, pain, proptosis, reduced vision).
Necrotising fasciitis Meropenem IV (Maximum dose) Plus
Clindamycin IV (Maximum dose)
Seek surgical review. Urgent surgical debridement is crucial.
Theatre specimens should be sent for microscopy and culture to help determine aetiology. Contact microbiology labs to arrange urgent examination.
Gas gangrene Benzylpenicillin IV Plus
Clindamycin IV
If true penicillin allergy:
Vancomycin IV Plus
Clindamycin IV
The primary treatment for this condition is urgent surgical debridement.
Antibiotics have only a secondary role in therapy.
Gangrene develops in anaerobic areas with limited blood flow. Therefore, antibiotics do not penetrate and only protect contiguous areas.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
11
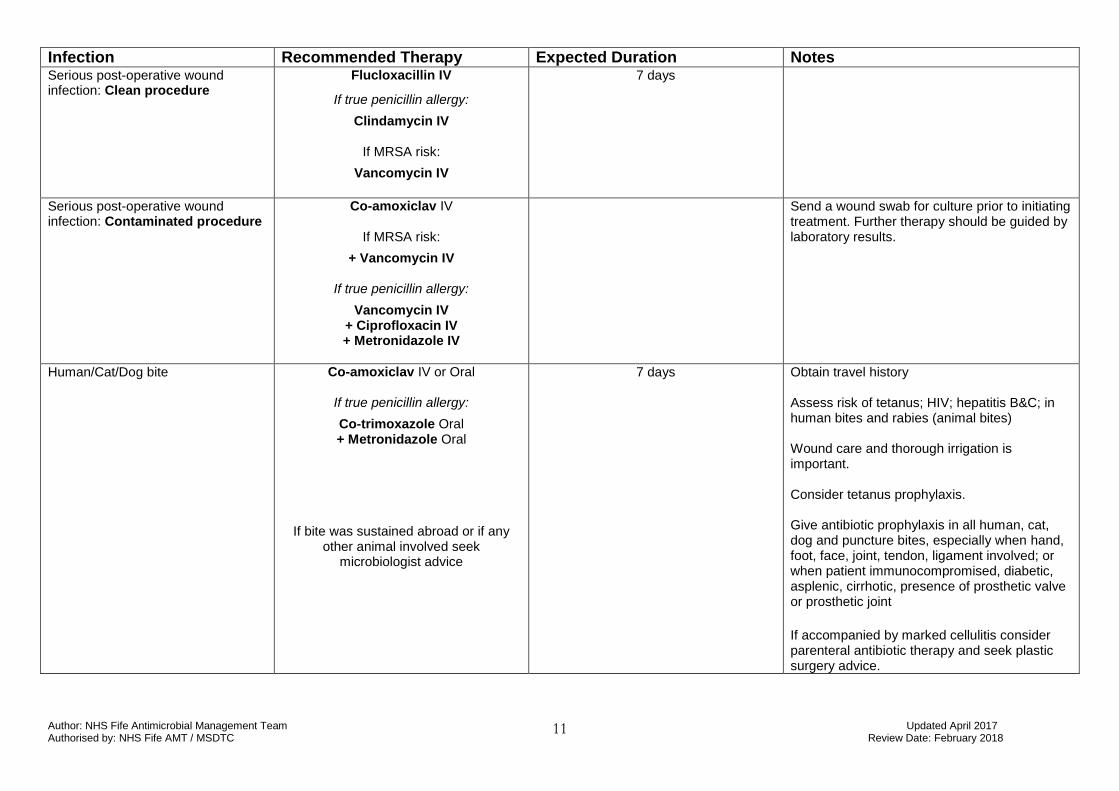
Infection Recommended Therapy Expected Duration Notes Serious post-operative wound infection: Clean procedure
Flucloxacillin IV
If true penicillin allergy:
Clindamycin IV
If MRSA risk:
Vancomycin IV
7 days
Serious post-operative wound infection: Contaminated procedure
Co-amoxiclav IV
If MRSA risk:
+ Vancomycin IV
If true penicillin allergy:
Vancomycin IV + Ciprofloxacin IV + Metronidazole IV
Send a wound swab for culture prior to initiating treatment. Further therapy should be guided by laboratory results.
Human/Cat/Dog bite Co-amoxiclav IV or Oral
If true penicillin allergy:
Co-trimoxazole Oral + Metronidazole Oral
If bite was sustained abroad or if any other animal involved seek
microbiologist advice
7 days Obtain travel history Assess risk of tetanus; HIV; hepatitis B&C; in human bites and rabies (animal bites) Wound care and thorough irrigation is important. Consider tetanus prophylaxis. Give antibiotic prophylaxis in all human, cat, dog and puncture bites, especially when hand, foot, face, joint, tendon, ligament involved; or when patient immunocompromised, diabetic, asplenic, cirrhotic, presence of prosthetic valve or prosthetic joint
If accompanied by marked cellulitis consider parenteral antibiotic therapy and seek plastic surgery advice.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
12
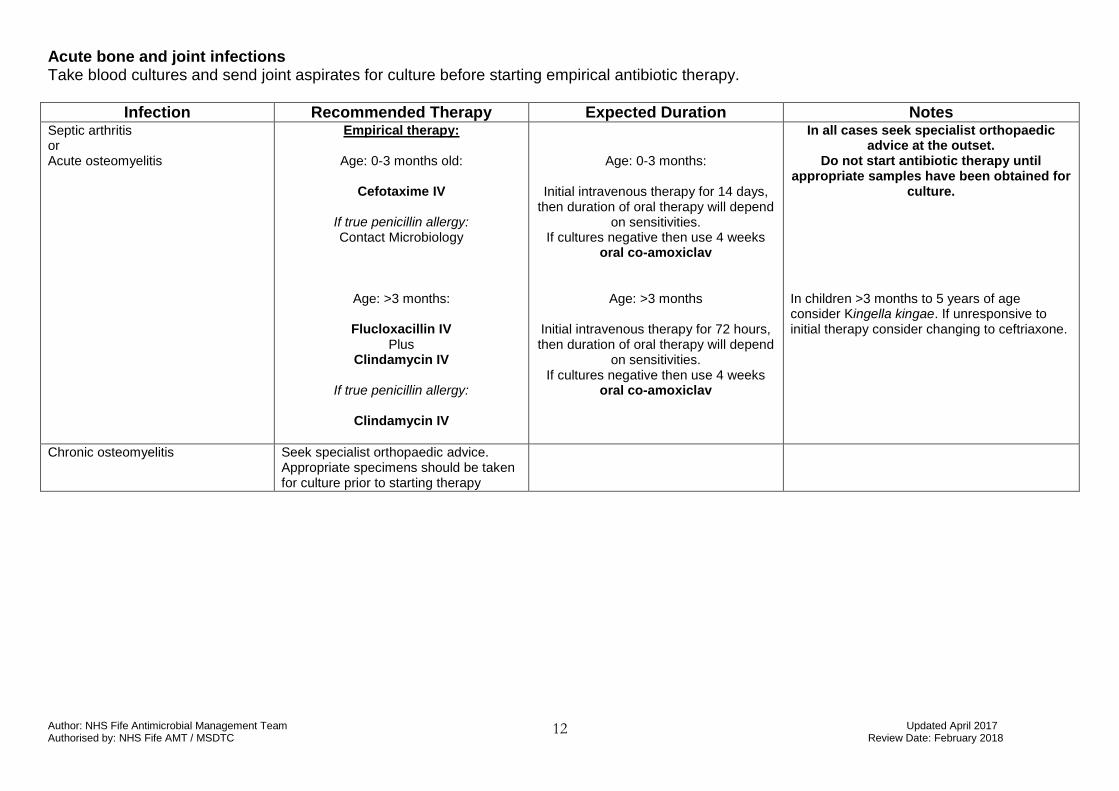
Acute bone and joint infections Take blood cultures and send joint aspirates for culture before starting empirical antibiotic therapy.
Infection Recommended Therapy Expected Duration Notes Septic arthritis or Acute osteomyelitis
Empirical therapy:
Age: 0-3 months old:
Cefotaxime IV
If true penicillin allergy: Contact Microbiology
Age: >3 months:
Flucloxacillin IV Plus
Clindamycin IV
If true penicillin allergy:
Clindamycin IV
Age: 0-3 months:
Initial intravenous therapy for 14 days, then duration of oral therapy will depend
on sensitivities. If cultures negative then use 4 weeks
oral co-amoxiclav
Age: >3 months
Initial intravenous therapy for 72 hours, then duration of oral therapy will depend
on sensitivities. If cultures negative then use 4 weeks
oral co-amoxiclav
In all cases seek specialist orthopaedic advice at the outset.
Do not start antibiotic therapy until appropriate samples have been obtained for
culture. In children >3 months to 5 years of age consider Kingella kingae. If unresponsive to initial therapy consider changing to ceftriaxone.
Chronic osteomyelitis Seek specialist orthopaedic advice. Appropriate specimens should be taken for culture prior to starting therapy
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
13
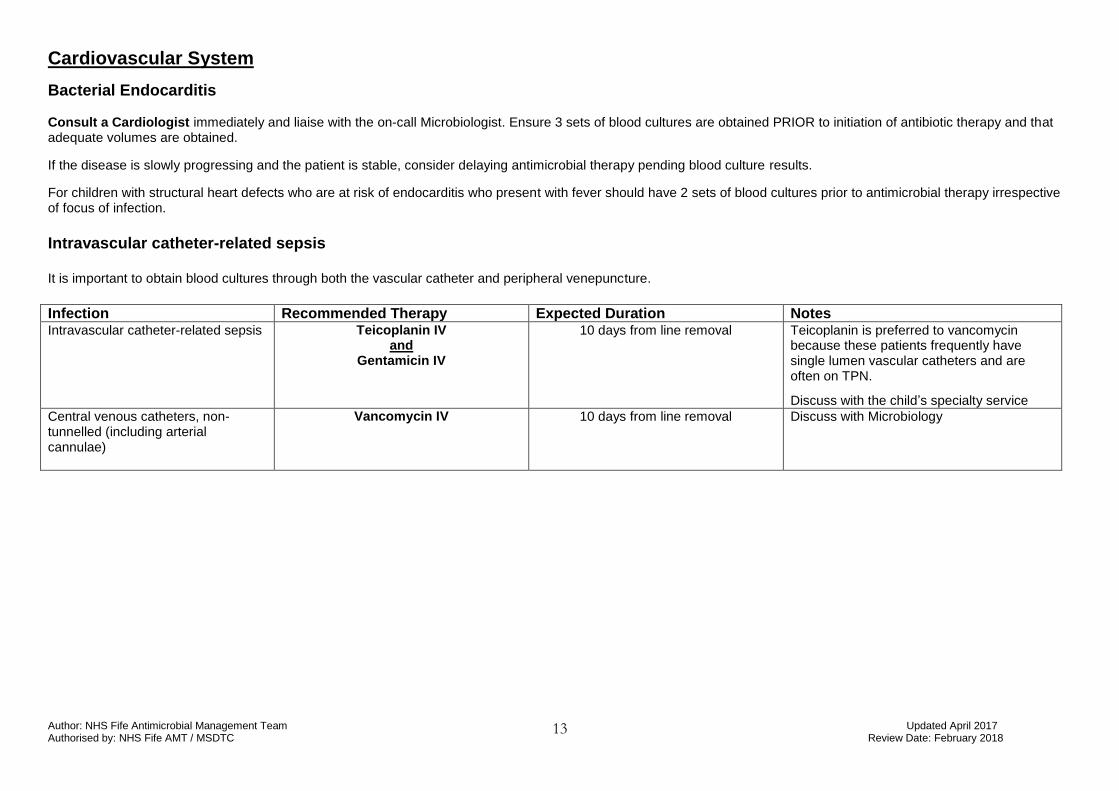
Cardiovascular System
Bacterial Endocarditis Consult a Cardiologist immediately and liaise with the on-call Microbiologist. Ensure 3 sets of blood cultures are obtained PRIOR to initiation of antibiotic therapy and that adequate volumes are obtained.
If the disease is slowly progressing and the patient is stable, consider delaying antimicrobial therapy pending blood culture results.
For children with structural heart defects who are at risk of endocarditis who present with fever should have 2 sets of blood cultures prior to antimicrobial therapy irrespective of focus of infection.
Intravascular catheter-related sepsis It is important to obtain blood cultures through both the vascular catheter and peripheral venepuncture.
Infection Recommended Therapy Expected Duration Notes Intravascular catheter-related sepsis
Teicoplanin IV and
Gentamicin IV
10 days from line removal Teicoplanin is preferred to vancomycin because these patients frequently have single lumen vascular catheters and are often on TPN.
Discuss with the child’s specialty service
Central venous catheters, non-tunnelled (including arterial cannulae)
Vancomycin IV
10 days from line removal Discuss with Microbiology
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
14
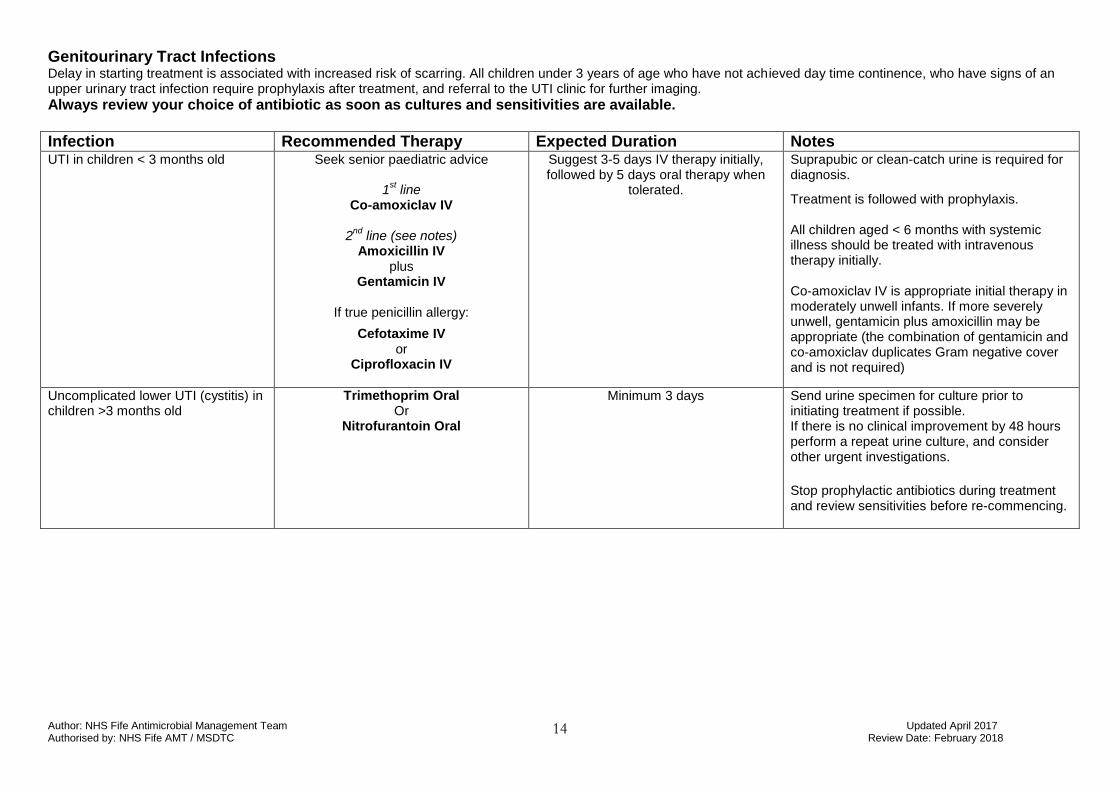
Genitourinary Tract Infections Delay in starting treatment is associated with increased risk of scarring. All children under 3 years of age who have not achieved day time continence, who have signs of an upper urinary tract infection require prophylaxis after treatment, and referral to the UTI clinic for further imaging.
Always review your choice of antibiotic as soon as cultures and sensitivities are available.
Infection Recommended Therapy Expected Duration Notes UTI in children < 3 months old
Seek senior paediatric advice
1st line
Co-amoxiclav IV
2nd
line (see notes) Amoxicillin IV
plus Gentamicin IV
If true penicillin allergy:
Cefotaxime IV or
Ciprofloxacin IV
Suggest 3-5 days IV therapy initially, followed by 5 days oral therapy when
tolerated.
Suprapubic or clean-catch urine is required for diagnosis.
Treatment is followed with prophylaxis. All children aged < 6 months with systemic illness should be treated with intravenous therapy initially. Co-amoxiclav IV is appropriate initial therapy in moderately unwell infants. If more severely unwell, gentamicin plus amoxicillin may be appropriate (the combination of gentamicin and co-amoxiclav duplicates Gram negative cover and is not required)
Uncomplicated lower UTI (cystitis) in children >3 months old
Trimethoprim Oral Or
Nitrofurantoin Oral
Minimum 3 days
Send urine specimen for culture prior to initiating treatment if possible. If there is no clinical improvement by 48 hours perform a repeat urine culture, and consider other urgent investigations.
Stop prophylactic antibiotics during treatment and review sensitivities before re-commencing.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
15
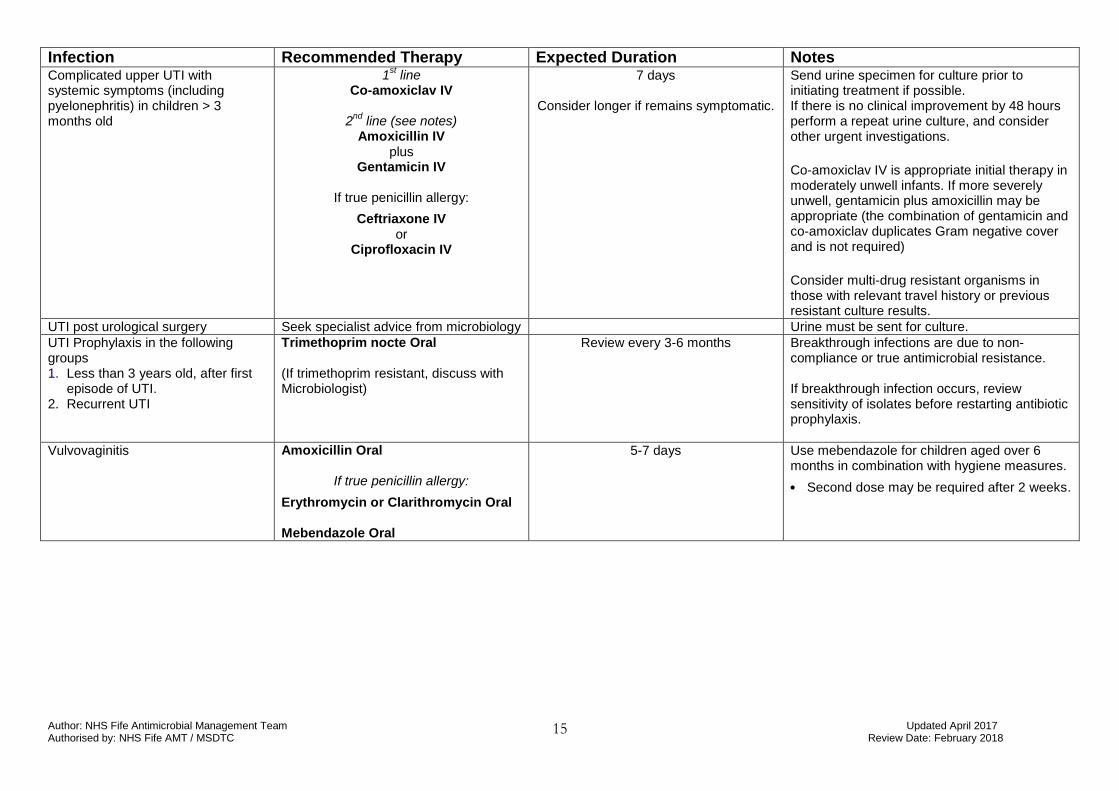
Infection Recommended Therapy Expected Duration Notes Complicated upper UTI with systemic symptoms (including pyelonephritis) in children > 3 months old
1st line
Co-amoxiclav IV
2nd
line (see notes) Amoxicillin IV
plus Gentamicin IV
If true penicillin allergy:
Ceftriaxone IV or
Ciprofloxacin IV
7 days
Consider longer if remains symptomatic.
Send urine specimen for culture prior to initiating treatment if possible. If there is no clinical improvement by 48 hours perform a repeat urine culture, and consider other urgent investigations.
Co-amoxiclav IV is appropriate initial therapy in moderately unwell infants. If more severely unwell, gentamicin plus amoxicillin may be appropriate (the combination of gentamicin and co-amoxiclav duplicates Gram negative cover and is not required) Consider multi-drug resistant organisms in those with relevant travel history or previous resistant culture results.
UTI post urological surgery Seek specialist advice from microbiology Urine must be sent for culture.
UTI Prophylaxis in the following groups 1. Less than 3 years old, after first
episode of UTI. 2. Recurrent UTI
Trimethoprim nocte Oral (If trimethoprim resistant, discuss with Microbiologist)
Review every 3-6 months Breakthrough infections are due to non-compliance or true antimicrobial resistance. If breakthrough infection occurs, review sensitivity of isolates before restarting antibiotic prophylaxis.
Vulvovaginitis Amoxicillin Oral
If true penicillin allergy:
Erythromycin or Clarithromycin Oral Mebendazole Oral
5-7 days Use mebendazole for children aged over 6 months in combination with hygiene measures.
• Second dose may be required after 2 weeks.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
16
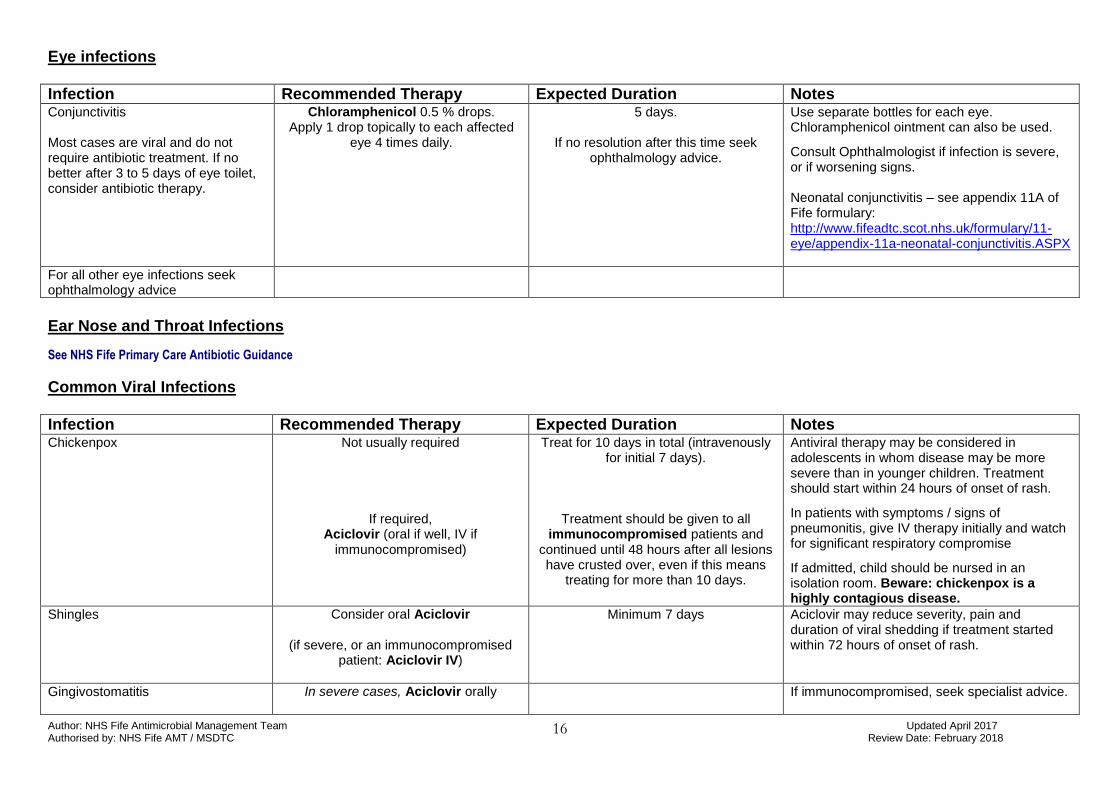
Eye infections
Infection Recommended Therapy Expected Duration Notes Conjunctivitis Most cases are viral and do not require antibiotic treatment. If no better after 3 to 5 days of eye toilet, consider antibiotic therapy.
Chloramphenicol 0.5 % drops. Apply 1 drop topically to each affected
eye 4 times daily.
5 days.
If no resolution after this time seek ophthalmology advice.
Use separate bottles for each eye.
Chloramphenicol ointment can also be used.
Consult Ophthalmologist if infection is severe, or if worsening signs. Neonatal conjunctivitis – see appendix 11A of Fife formulary: http://www.fifeadtc.scot.nhs.uk/formulary/11-eye/appendix-11a-neonatal-conjunctivitis.ASPX
For all other eye infections seek ophthalmology advice
Ear Nose and Throat Infections
See NHS Fife Primary Care Antibiotic Guidance
Common Viral Infections
Infection Recommended Therapy Expected Duration Notes Chickenpox Not usually required
If required, Aciclovir (oral if well, IV if
immunocompromised)
Treat for 10 days in total (intravenously for initial 7 days).
Treatment should be given to all immunocompromised patients and
continued until 48 hours after all lesions have crusted over, even if this means
treating for more than 10 days.
Antiviral therapy may be considered in adolescents in whom disease may be more severe than in younger children. Treatment should start within 24 hours of onset of rash.
In patients with symptoms / signs of pneumonitis, give IV therapy initially and watch for significant respiratory compromise
If admitted, child should be nursed in an isolation room. Beware: chickenpox is a highly contagious disease.
Shingles Consider oral Aciclovir
(if severe, or an immunocompromised patient: Aciclovir IV)
Minimum 7 days Aciclovir may reduce severity, pain and duration of viral shedding if treatment started within 72 hours of onset of rash.
Gingivostomatitis
In severe cases, Aciclovir orally
If immunocompromised, seek specialist advice.
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
17
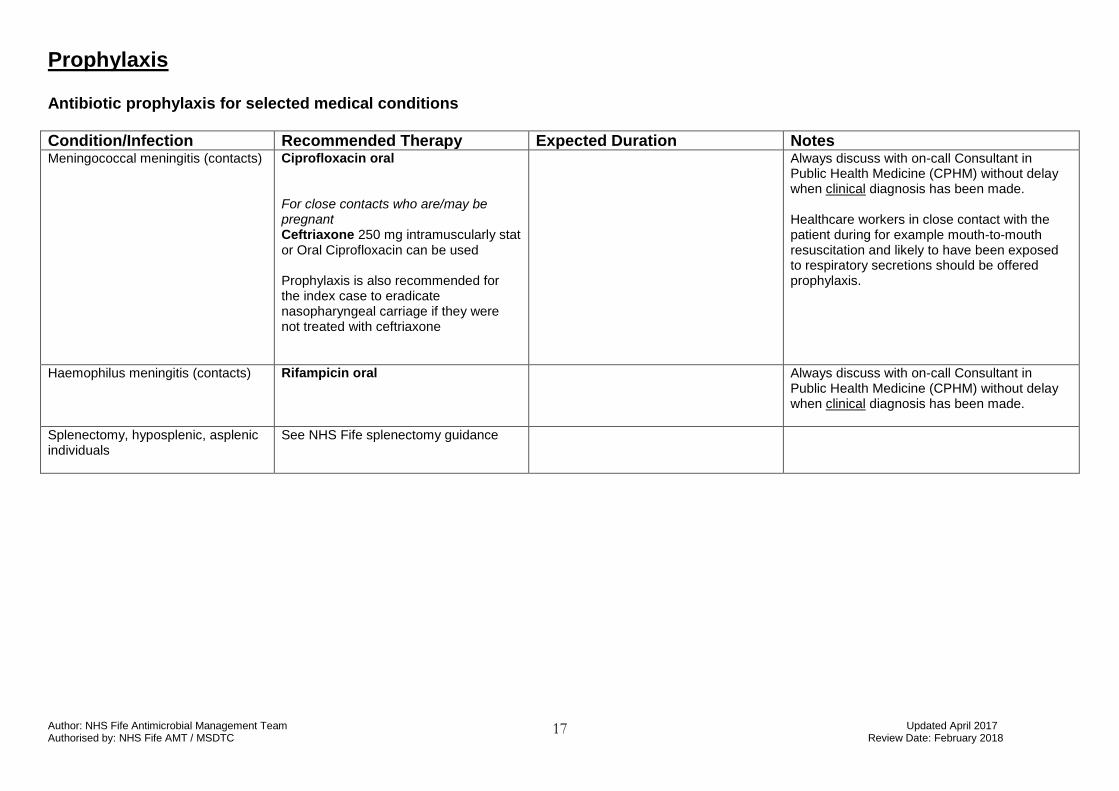
Prophylaxis Antibiotic prophylaxis for selected medical conditions
Condition/Infection Recommended Therapy Expected Duration Notes Meningococcal meningitis (contacts)
Ciprofloxacin oral For close contacts who are/may be pregnant Ceftriaxone 250 mg intramuscularly stat or Oral Ciprofloxacin can be used Prophylaxis is also recommended for the index case to eradicate nasopharyngeal carriage if they were not treated with ceftriaxone
Always discuss with on-call Consultant in Public Health Medicine (CPHM) without delay when clinical diagnosis has been made. Healthcare workers in close contact with the patient during for example mouth-to-mouth resuscitation and likely to have been exposed to respiratory secretions should be offered prophylaxis.
Haemophilus meningitis (contacts)
Rifampicin oral
Always discuss with on-call Consultant in Public Health Medicine (CPHM) without delay when clinical diagnosis has been made.
Splenectomy, hyposplenic, asplenic individuals
See NHS Fife splenectomy guidance
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
18
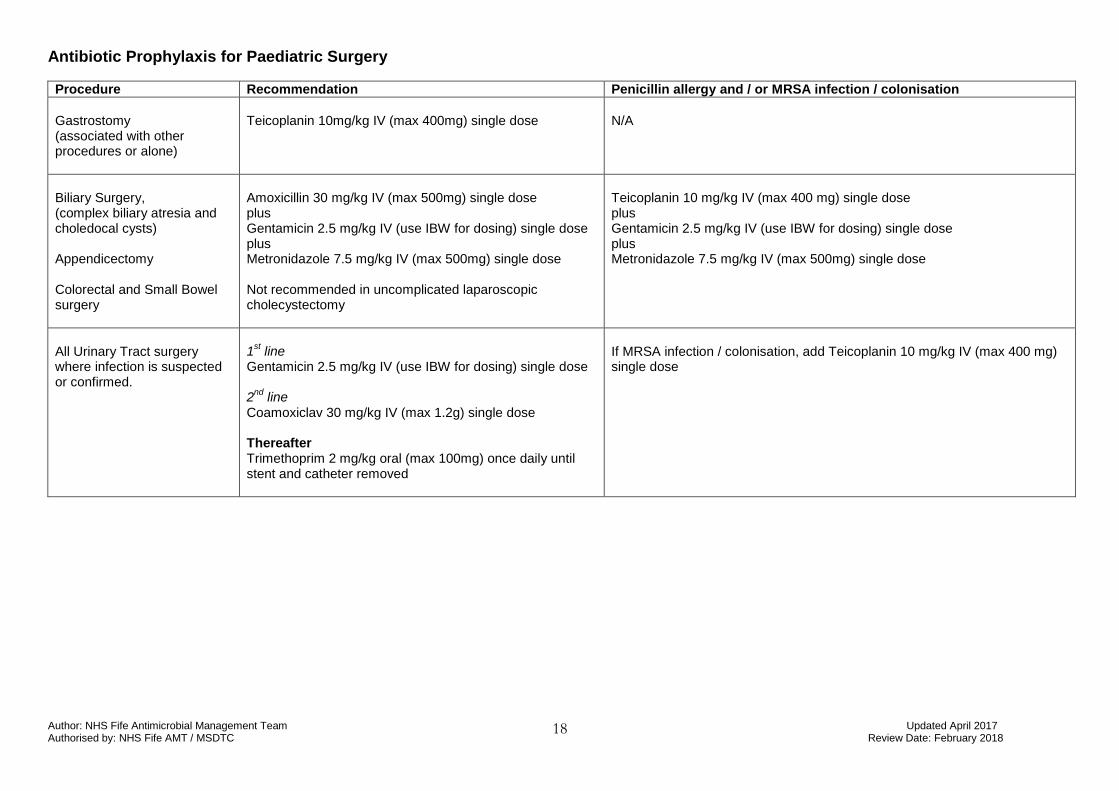
Antibiotic Prophylaxis for Paediatric Surgery
Procedure Recommendation Penicillin allergy and / or MRSA infection / colonisation
Gastrostomy (associated with other procedures or alone)
Teicoplanin 10mg/kg IV (max 400mg) single dose
N/A
Biliary Surgery, (complex biliary atresia and choledocal cysts) Appendicectomy Colorectal and Small Bowel surgery
Amoxicillin 30 mg/kg IV (max 500mg) single dose plus Gentamicin 2.5 mg/kg IV (use IBW for dosing) single dose plus Metronidazole 7.5 mg/kg IV (max 500mg) single dose Not recommended in uncomplicated laparoscopic cholecystectomy
Teicoplanin 10 mg/kg IV (max 400 mg) single dose plus Gentamicin 2.5 mg/kg IV (use IBW for dosing) single dose plus Metronidazole 7.5 mg/kg IV (max 500mg) single dose
All Urinary Tract surgery where infection is suspected or confirmed.
1
st line
Gentamicin 2.5 mg/kg IV (use IBW for dosing) single dose 2
nd line
Coamoxiclav 30 mg/kg IV (max 1.2g) single dose Thereafter Trimethoprim 2 mg/kg oral (max 100mg) once daily until stent and catheter removed
If MRSA infection / colonisation, add Teicoplanin 10 mg/kg IV (max 400 mg) single dose
Author: NHS Fife Antimicrobial Management Team Updated April 2017 Authorised by: NHS Fife AMT / MSDTC Review Date: February 2018
19
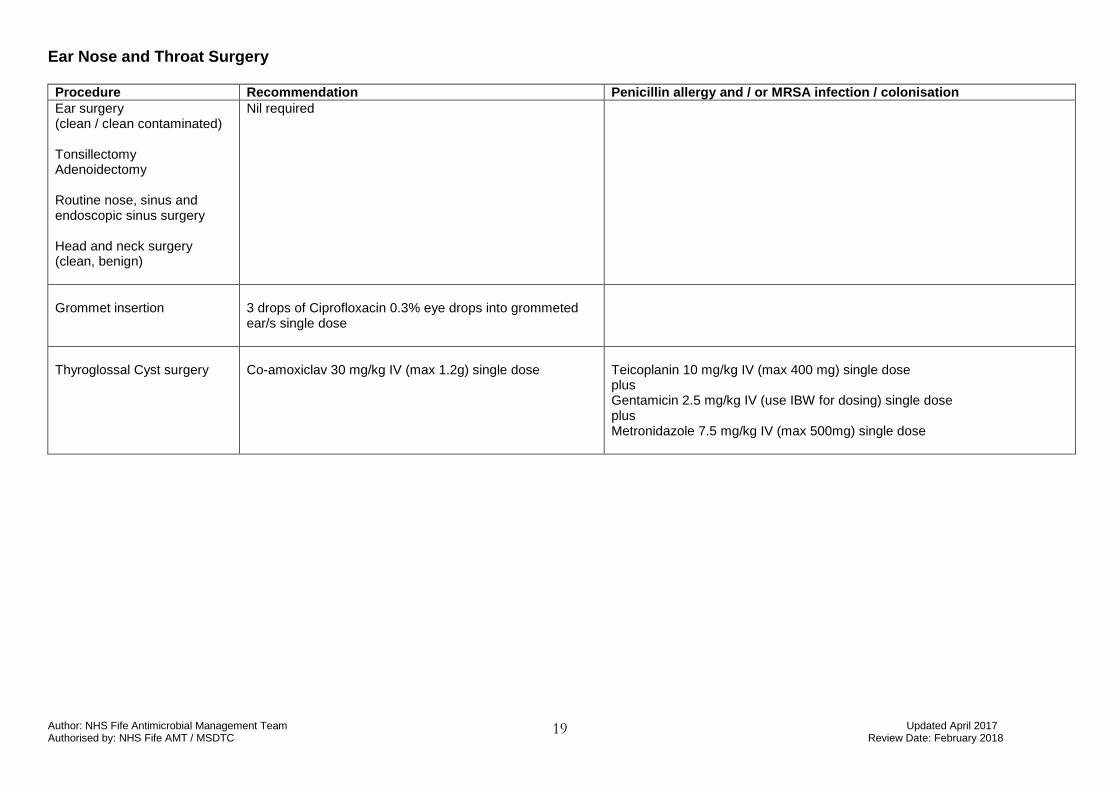
Ear Nose and Throat Surgery Procedure Recommendation Penicillin allergy and / or MRSA infection / colonisation
Ear surgery (clean / clean contaminated) Tonsillectomy Adenoidectomy Routine nose, sinus and endoscopic sinus surgery Head and neck surgery (clean, benign)
Nil required
Grommet insertion
3 drops of Ciprofloxacin 0.3% eye drops into grommeted ear/s single dose
Thyroglossal Cyst surgery
Co-amoxiclav 30 mg/kg IV (max 1.2g) single dose
Teicoplanin 10 mg/kg IV (max 400 mg) single dose plus Gentamicin 2.5 mg/kg IV (use IBW for dosing) single dose plus Metronidazole 7.5 mg/kg IV (max 500mg) single dose





























