Embed Size (px)
Citation preview
Paediatric Advanced Nurse Practice Education
Helen RolléAdvanced Children’s Emergency Nurse Practitioner
Objectives
The role of the Advanced Children’s Emergency Nurse Practitioner
Explain how the role has changed since it’s original commission
‘The Team’ and it’s dynamics
Educational approaches taken to support ‘the gaps’
The KSF and appraisal process
Children’s Emergency Department:Background
Initially medical unit only: 13,500 children per year Merged with main A+E in 2009 Now classed as a traditional children’s A+E: 34,500 children per year
Arrivals: Self referral, GP referral, Other health referrals e.g. Out of Hours, Walk in centre, Minor injury units
Current target achievement is 99.3% against 4 hour target Staffing; Nurses, Emergency Nurse Practitioners, Advanced
Emergency Practitioners, SHO, Registrar, Consultants, GP VTS
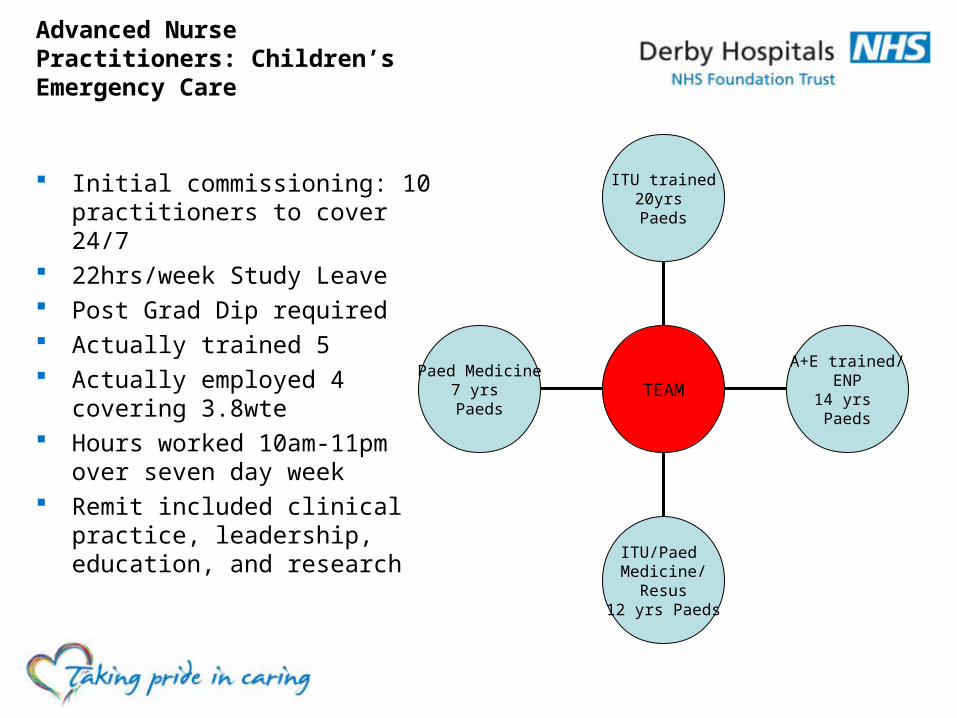
Advanced Nurse Practitioners: Children’s Emergency Care
Initial commissioning: 10 practitioners to cover 24/7
22hrs/week Study Leave Post Grad Dip required Actually trained 5 Actually employed 4 covering
3.8wte Hours worked 10am-11pm over
seven day week Remit included clinical practice,
leadership, education, and research
Paed Medicine7 yrs Paeds
ITU/Paed Medicine/
Resus12 yrs Paeds
A+E trained/ENP
14 yrs Paeds
ITU trained20yrs Paeds
TEAM
Advanced Children’s Emergency Nurse PractitionerRole Development
Bridge the gap between nursing and medical services in the Emergency Department
Initial commissioning: Patients with minor illness Role has developed to work as ‘SHO’ equivalent: All patients
Additional educational need Different working hours Additional Governance
Education
Medic &Multi-
disciplinary
Personal Opportunistic
On the jobTeaching
Traditional Academic
Course
Education
KSF Package
Interview with medical supervisor
Quality review of notes Case Based Discussion
Mini CEX
Direct Observation of procedure
Multi Source Feedback Tool
Learning development Plan
Teaching feedback formal
KSF appraisal
CORE DIMENSIONS
1 Communication: Level 3 2 Personal and people development: Level 3 3 Health, safety and security: Level 3 4 Service improvement: Level 3 5 Quality: Level 4 6 Equality and diversity: Level 3
Specific Dimensions also included
Medical Appraisal and Nursing Management Appraisal
Governance Framework
Professional Accountability & Assurance Framework for Advanced Practice
Introduction, Definitions, Boundaries General / specialist role Assessment strategies Competencies Support and supervision (clinical & medical) Activity Training, education, career and Continual Professional Development Regulation & accountability Non – Medial prescribing Medical rota Research, audit and disseminating activity Clinical leadership Sustainability, succession planning and talent spotting Managers roles and responsibilities Electronic repository with live register of practitioners Tool kitRecruitment and selection processJob descriptionPerson specificationRole
evaluationConsistency check list
The future
Future commissioning of service
Nursing staff v Medical staff
Role development and promotion opportunities
Any Questions ?