Embed Size (px)
Citation preview
CMS has taken the next step toward adopting the new 2012 Life Safety Code® (LSC). In April, the federal agency published a proposed rule in the Federal Regis-ter to adopt the updated 2012 edition of the LSC, which it would use in its ongoing work to ensure the health and safety of patients, family, and staff in every pro-vider and supplier setting. The updated LSC contains new provisions that are vital to the health and safety of all patients and staff.
The LSC sets fire safety requirements for new and existing buildings, and is issued by the NFPA, a private, nonprofit organization dedicated to reducing loss of life due to fire. Currently, CMS applies the requirements of the 2000 edition of the LSC to healthcare providers in order to ensure patients’ and caregivers’ safety.
The proposed rule by CMS is consistent with the Administrative Procedure Act of 1946, which regulates
CMS publishes the proposed rule to adopt the 2012 LSC
Volume 16Issue No. 6 JUNE 2014
Healthcare Life Safety Compliance
The newsletter to assist healthcare facility managers with fire protection and life safety
how federal agencies add, change, or remove a rule. After World War II, Congress had great concerns about the expanding powers that federal agencies possessed. As a result, the Administrative Procedure Act was passed to effectively force the federal agencies to listen to the comments and concerns of the people whom a change in regulation would likely affect, preventing a dictatorial form of government.
Since the proposed rule was published in the Federal Register April 16 and the public comment period is typically 60 days long, that means that unless the com-ment period is extended, the public has until June 16 to send CMS their comments on the proposed rule. After the public comment period closes, CMS will begin the process of sorting though and analyzing every com-ment or suggestion that was submitted, then revise the rule accordingly.
Documentation strategiesTo help work with surveyors or accrediting organizations during survey, it’s best to have your documentation in order. Find tips and ideas inside. Oxygen cylinder suspected in hospital explosionRead about the investigation and response into an explosion at a New Jersey hospital. Q&AThis month’s Q&A looks at walk-in coolers, clinical business occupancies, emergency lighting, and more.
Organized document for surveyThis month’s bonus tool is intended to help prepare documentation for a Joint Commission survey.
P7
P8
P10
P12
Healthcare Life Safety Compliance June 2014
2 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Follow UsFollow and chat with us about all things healthcare compliance, management, and reimbursement. @HCPro_Inc
Healthcare Life Safety Compliance (ISSN: 1523-7575 [print]; 1937-741X [online]) is published monthly by HCPro, a division of BLR, 75 Sylvan St., Suite A-101, Danvers, MA 01923. Subscription rate is $329 for one year and includes unlimited telephone assistance. Single copy price is $25. Healthcare Life Safety Compliance, P.O. Box 3049, Peabody, MA 01961-3049. Copyright © 2014 HCPro, a division of BLR. All rights reserved. Printed in the USA. Except where explicitly encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, a division of BLR, or the Copyright Clearance Center at 978-750-8400. Please notify us immediately if you have received an unauthorized copy. For editorial comments or questions or for technical support with questions about life safety compliance, call 781-639-1872 or fax 781-639-7857. For renewal or subscription information, call customer service at 800-650-6787, fax 800-639-8511, or email [email protected]. Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be in cluded on this mailing list, please write to the marketing department at the address above. Opinions expressed are not necessarily those of HLSC. Mention of products and services does not constitute endorsement. Advice given is general and based on National Fire Protection Association codes and not based on local building or fire codes. No warranty as to the suitability of the information is expressed or implied. Information should not be construed as engineering advice specific to your facility and should not be acted upon without consulting a licensed engineer, architect, or other suitable professional. Final acceptability of such information and interpretations will always rest with the authority having jurisdiction, which may differ from that offered in the newsletter or otherwise. Advisory board members are not responsible for information and opinions that are not their own.
EDITORIAL ADVISORY BOARD
James R. Ambrose, PETechnical Director, HealthcareCode Consultants, Inc. St. Louis, Missouri
Frederick C. Bradley, PEPrincipalFCB Engineering Alpharetta, Georgia
Michael Crowley, PESenior Vice President, Engineering ManagerRolf Jensen & Associates, Inc. Houston, Texas
Joshua W. Elvove, PE, CSP, FSFPEFire Protection EngineerAurora, Colorado
A. Richard FasanoManager, Western OfficeRussell Phillips & Associates, LLC Elk Grove, California
Burton Klein, PEPresidentBurton Klein Associates Newton, Massachusetts
Henry KowalenkoSupervisor, Design Standards UnitOffice of Healthcare Regulation, Illinois Department of Public Health Chicago, Illinois
David MohilePresidentMedical Engineering Services, Inc. Leesburg, Virginia
James MurphyPresidentMRF, Ltd. Western Springs, Illinois
Thomas SalamoneDirector, Healthcare ServicesTelgian Corporation Atlanta, Georgia
William Wilson, CFPS, PEMFire Safety CoordinatorBeaumont Hospitals Royal Oak, Michigan
Senior Managing EditorMatt Phillion, [email protected]
Senior EditorBrad Keyes, CHSP Senior Consultant Keyes Life Safety Compliance www.keyeslifesafety.com
This document contains privileged, copyrighted information. If you have not purchased it or are not otherwise entitled to it by agreement with HCPro, a division of BLR, any use, disclosure, forwarding, copying, or other communication of the contents is prohibited without permission.
Contrary to popular belief, Congress will not vote on or officially review the proposed rule to adopt the 2012 LSC, nor the eventual final rule that CMS will issue. Similarly, neither the proposed nor final rules will need to be signed into law by the president. Once the final rule is issued through the federal rulemaking process, it becomes law.
According to its announcement, CMS’ key priority is to ensure that patients and staff continue to experi-ence the highest degree of safety possible, including fire safety. CMS says adopting the 2012 edition of the LSC would reduce the burden on healthcare providers, as it claims the new edition is aligned with the international building codes and would greatly simplify compliance across codes for Medicare- and Medicaid-participating facilities.
Not only is CMS proposing to adopt the 2012 edition of the LSC, but for the first time ever, it is also propos-ing to adopt NFPA 99, Health Care Facilities Code, although it has specifically excluded chapters 7, 8, 12, and 13 from NFPA 99. CMS states in the proposed rule that Chapter 7 on information technology, Chapter 8
on plumbing, and Chapter 13 on security management are not within the scope of the Conditions of Partici-pation and conditions for coverage for Medicare and Medicaid regulations. For Chapter 12 on emergency management, CMS has already issued a proposed rule in December 2013 on new emergency management regulations, so Chapter 12 would be redundant.
Why is CMS breaking tradition and adopting NFPA 99 now when it has not done so in previous years? One reason is the 2012 edition of NFPA 99 is now a code, rather than just a standard. The basic difference between a code and a standard is that a code tells you what to do and a standard tells you how to do it. There-fore, NFPA 99 is now a code in the same way that the LSC is a code.
“We decided to propose adopting the NFPA 99 be-cause it addresses additional building safety topics that are related to important fire safety issues,” CMS states in the proposed rule.
The 2012 edition of NFPA 99 contains more de-tailed provisions specific to healthcare and ambulatory care facilities. Adoption of this code would provide
Healthcare Life Safety ComplianceJune 2014
3HCPRO.COM© 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
minimum requirements for the installation, inspection, testing, maintenance, performance, and safe prac-tices of healthcare facility materials, equipment, and appliances.
The proposed adoption of the 2012 edition of NFPA 99 is significant, as currently CMS has not adopted the 1999 edition of NFPA 99. The Interpretive Guide-lines for CMS’ Conditions of Participation §482.41(a)(1) and §482.41(b)(1)–(3) for hospitals clearly refer to compliance with NFPA 99 through the references identified in the 2000 LSC. While the LSC does refer-ence certain sections of NFPA 99, it does not reference all of them. CMS’ proposed rule will change that for hospitals, and presumably all other healthcare facili-ties, by requiring compliance with the 2012 edition of NFPA 99 (with the exception, as already stated, of chapters 7, 8, 12, and 13).
Once the new edition of the LSC is adopted, it will apply to: • Hospitals • Long-term care (LTC) facilities • Critical access hospitals (CAH) • Programs for All Inclusive Care for the Elderly
(PACE) • Religious nonmedical healthcare institutions
(RNHCI) • Hospice inpatient facilities • Ambulatory surgical centers (ASC) • Intermediate care facilities for individuals with in-
tellectual disabilities (ICF-IID)
Adoption of the new LSC and NFPA 99 (applicable to hospitals, LTC facilities, CAHs, hospice inpatient facili-ties, PACE programs, and RNHCIs) would make the following changes:• Allow facilities to increase suite sizes • Require all high-rise buildings over 75 feet to be
fully sprinklered within 12 years• Allow controlled access doors to prevent wander-
ing patients• Address issues of alcohol-based hand rub (ABHR)
and aerosol dispensers in corridors and patient rooms
• Require a fire watch (the assignment of a person or persons to an area for the express purpose of noti-fying appropriate people during an emergency) or
building evacuation if a sprinkler system is out of service for more than four hours
• Require smoke control in anesthetizing locations• Reduce the frequency of non-flow fire pump test-
ing from weekly to monthly• Reduce the frequency of water flow switch testing
from quarterly to semiannually• Permit existing unoccupied rooms to open onto an
exit enclosure• Allow certain wheeled equipment to be left unat-
tended in a corridor
The key changes for ASCs would:• Require interior non-bearing walls to have a mini-
mum of two-hour fire resistance rating and be con-structed with fire-retardant treated wood
• Require all doors to hazardous areas to be self-closing or automatic closing
• Address the issue of placing ABHR dispensers in corridors
• Require a fire watch or building evacuation if a sprinkler system is out of service for more than four hours
• Require smoke control in anesthetizing locations
The major changes for ICF-IIDs would:• Expand sprinkler requirements to include habit-
able areas, closets, roofed porches, balconies, and decks in new facilities
• Require all attics to be sprinklered if they are used for living purposes, storage, or housing of fuel-fired equipment—if they are not used for these purposes, they may have heat detection systems instead
• Require all designated means of escape to be free from obstruction
• Require new facilities to have smoke alarms in-stalled on all levels
• Require hazardous areas to be separated from oth-er parts of the building by smoke partitions
• Require existing facilities to include certain fire alarm features when updating their fire alarm systems
One thing that will not change is the continued ban on roller latches on corridor doors. CMS reiterated its position in the proposed rule that it will not allow them,

Healthcare Life Safety Compliance June 2014
4 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
although the LSC does in certain applications. The 2000 LSC requires minor renovation work to
meet the same stringent requirements as those ap-plied to completely new construction. However, the 2012 LSC contains a new chapter entitled “Chapter 43 – Building Rehabilitation.” This new chapter replaces the requirements that all modernizations/renova-tions meet the requirements for new construction. The degree to which requirements for new construction must be met now varies with the rehabilitation work (e.g., repair, renovation, modification, reconstruction, change of use, change of occupancy, and addition), to which different standards apply. CMS believes that this clarification will assist healthcare facilities by reducing costs for minor construction projects.
CMS states in the proposed rule that it does not agree with the NFPA’s interpretation of what constitutes a healthcare occupancy. Both the 2000 and 2012 LSC classify a healthcare occupancy as a facility having four or more patients on an inpatient basis. However, CMS does not apply this LSC standard with respect to patient census numbers. Unless specifically noted, the requirements, Conditions of Participation, and condi-tions for coverage for all Medicare- and Medicaid-par-ticipating healthcare providers and suppliers subject to CMS’ rules would apply on a facility basis, regardless of the facility’s size or patient census. Therefore, all healthcare facilities that provide care to one or more in-patients would be required to comply with the relevant healthcare occupancy requirements of the 2012 LSC.
The 2012 LSC allows corridor projections of up to 6 inches, but CMS is citing the more restrictive allowance for corridor projections of 4 inches by the Americans With Disabilities Act (ADA). Therefore, CMS will not recognize the LSC 6-inch limit on corridor projections and will instead enforce the 4-inch projections as re-quired by the ADA.
CMS is firmly behind the new 2012 LSC requirement for existing high-rise healthcare occupancies to be fully protected with automatic sprinklers within 12 years of adopting the new code. (New construction high-rise healthcare occupancies would already be required to be fully sprinklered.) High-rise buildings are defined as buildings with floors of an occupiable story greater than 75 feet above the lowest level of fire department vehicle access. The reason to install sprinklers in existing high-
rise occupancies is to provide fire suppression to allow more time to safely evacuate the building.
Changes in the new 2012 LSC specifically allow ABHR dispensers to be aerosol in addition to gel dis-pensers. The limitations in the LSC on aerosol dispens-ers are less restrictive, thereby allowing more dispens-ers per smoke compartment. In addition, the 2012 LSC has provisions that exclude one ABHR dispenser per patient room from counting toward the aggregate total of product per smoke compartment.
CMS is endorsing the changes in the 2012 LSC to allow automatic (touchless) dispensers in healthcare occupancies, provided the following provisions are met:• They do not release contents unless they are
activated• The activation occurs only when an object is within
4 inches of the sensing device• Any object placed in the activation zone and left in
place must not cause more than one activation• The dispenser must not dispense more than the
amount required for hand hygiene consistent with label instructions
• The dispenser is designed, constructed, and oper-ated in a way to minimize accidental or malicious dispensing
• All dispensers are tested in accordance with the manufacturer’s care and use instructions each time a new refill is installed
The new LSC also clarifies how close (side to side) an ABHR dispenser can be mounted to an ignition source: one inch, a measurement that CMS will uniformly enforce. ABHR dispensers cannot be mounted over the top of any ignition source.
The LSC references NFPA 25, Standard for the Inspection, Testing and Maintenance of Water-Based Fire Protection Systems, for all sprinkler system testing and inspection requirements. The 2000 LSC referenced the 1998 edition of NFPA 25, and the 2012 LSC refer-ences the 2011 edition of NFPA 25. The 1998 edition of NFPA 25 requires a fire watch when a sprinkler system is out of service for four or more hours in a 24-hour period, whereby the 2011 edition requires a fire watch when a sprinkler system is out of service for 10 or more hours in a 24-hour period. However, CMS will not allow the more lenient 10-hour time limit that the 2011
Healthcare Life Safety ComplianceJune 2014
5HCPRO.COM© 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
edition of NFPA 25 permits, and will retain the four-or-more-hour limitation identified in the 1998 edition. CMS says the reason it is staying with the four-hour limit is due to the increased reliance upon a facility sprinkler system. What the agency does not speak to is the intent of the technical committee for NFPA 25 that made the change from four to 10 hours. This change was made to allow a sprinkler system shutdown during the day shift without having to go to the trouble of a formal fire watch halfway through the shift. The ratio-nale is there are plenty of staff in the hospital during the day shift to act as a de facto fire watch.
When the 1999 edition of NFPA 99 was referenced by the 2000 LSC, there were provisions to have a smoke control ventilation system in anesthetizing locations. That requirement was eliminated in the 2012 edition of NFPA 99, which is referenced by the 2012 LSC. CMS states in its proposed rule that since fires in operating rooms continue to occur, the agency will retain the re-quirement for smoke control in anesthetizing locations identified in the 1999 edition of NFPA 99.
The 2000 LSC required every healthcare occupancy patient sleeping room to have an outside window or outside door. Window sills in new healthcare occu-pancies could be no higher than 36 inches above the floor, with certain exceptions. The 2012 LSC techni-cal committee eliminated this window requirement, stating windows are no longer needed for ventilation or fire escapes. However, CMS does not agree with this philosophy and states in the proposed rule that it will retain the requirements from the 2000 LSC for pa-tient room windows. Ironically, CMS cites the need for ventilation and patient evacuation as reasons to retain the windows in patient rooms—the very same reasons the NFPA technical committee cited when deciding the windows are no longer needed.
Turning to ambulatory healthcare occupancy re-quirements, CMS already has regulations under 42 CFR §416.44 that require all ambulatory surgical cen-ters to meet the provisions of ambulatory healthcare occupancy requirements, regardless of the number of patients served. CMS states that hospital outpatient surgical departments are comparable to ambulatory surgical centers and therefore should be likewise re-quired to comply with the applicable provisions of the ambulatory healthcare occupancy requirements.
CMS states in the proposed rule that it will retain its existing authority to grant waivers of LSC requirements when, under certain circumstances, the waiver would not adversely affect patient or staff health and safety; and when the LSC requirement imposes an unreason-able hardship on the facility. One of the more critical comments about the CMS waiver process is the neces-sity for the LSC deficiency to be cited by a state agency or an accreditation organization before CMS would consider the waiver request. While it did develop cat-egorical waivers in the past year for certain features of the new 2012 LSC to be used immediately, CMS doesn’t seem to be budging on this issue.
The agency states in the proposed rule: “We do not consider it always necessary for a facility to be cited for a deficiency before it can apply for or receive a waiver, and we have periodically issued communications re-garding specific provisions of the LSC that we evaluated and for which we have determined that a waiver would generally apply, subject to documentation maintained by the facility and verification of the applicability of the waiver when a survey of the facility is conducted. We plan to continue this approach.”
The 2000 LSC required every health-care occupancy patient sleeping room to have an outside window or outside door.
Window sills in new healthcare occupan-cies could be no higher than 36 inches
above the floor, with certain exceptions.
This appears to be stating that CMS will continue to issue categorical waivers when the LSC (or other standards) change for the advancement of healthcare organizations. But it does not address the need by healthcare organizations to request waivers before they are cited by an authority. Facility managers want to be proactive and request a waiver before a survey, but the CMS rule seems to prevent this approach.
When it comes to granting equivalencies, the proposed rule packs a strong statement against the accreditation organizations. CMS states the LSC recognizes alterna-tive systems, methods, and devices can be approved as equivalent by the authority having jurisdiction as being compliant with the LSC. The agency further states that,

Healthcare Life Safety Compliance June 2014
6 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
as the authority having jurisdiction for certification, it alone will approve equivalencies through the waiver process. What that means is no one other than CMS will approve equivalencies for any healthcare organiza-tion that is CMS certified. This is contrary to the current practice by some of the accreditation organizations. If this ability to approve equivalencies is removed from the accreditation organizations, CMS will have a large back-log of equivalencies to approve. And no longer will the economical “traditional equivalency” be allowed, as CMS will only accept an equivalency through the Fire Safety Evaluation System process as promulgated by NFPA 101A, Guide on Alternative Approaches to Life Safety.
In creating its proposed rule, CMS is required by law to identify the financial impact the new rule would have on the people and organizations it would affect. Contrary to previous statements, this new rule will cost some healthcare providers substantial resources.
Take the requirement of the 2012 LSC that mandates a high-rise building containing healthcare occupancies to be fully protected with automatic sprinklers 12 years after the code is adopted. CMS is on record of stating it will retain the 12-year time period to install the sprin-klers and not shorten it.
Based on information provided by individual state agencies, it is estimated there are 176 high-rise health-care occupancies in the United States that are not fully protected with sprinklers. According to additional statistics supplied by the states, CMS estimates it will cost $78,934,966 to install sprinklers in the remain-ing high-rise healthcare occupancies that are not fully sprinklered, or $448,494 per building. When averaged out over 12 years, that will cost approximately $6.6 million per year, or $37,375 per building. This cost will have to be funded by the healthcare providers.
Or take the 2012 LSC provision for ambulatory healthcare occupancies that requires all doors to haz-ardous areas to be self-closing or automatically closing. According to CMS, this provision was added to provide an extra level of protection for the patients. It also aligns the requirements for both ambulatory surgical centers and hospitals to ensure the same basic levels of protection for all patients.
However, this provision is also not without an associ-ated price tag. The estimated cost to add self-closing doors in all ambulatory healthcare occupancies that
require upgrading is $1.35 million, which will likely need to be accomplished within one year of the new LSC being adopted.
Adoption of the 2012 LSC has been under discussion for some time now, and facility managers have time to get ready. If you haven’t already started, the time is now to read the new code and prepare for the changes.
“Many in the healthcare industry are excited that the new 2012 LSC will be advantageous to ongoing compli-ance efforts, and in many instances this will be true,” says Jim Murphy, RA, NCARB, president of MRF, Ltd., in Western Springs, Illinois. “However, it should be noted that some provisions will bring new concerns and require additional efforts to ensure compliance. Facilities need to carefully study the effects of the proposed changes and prepare accordingly well in advance of adoption.”
The proposed rule is currently on display at https://www.federalregister.gov/articles/2014/ 04/16/2014-08602/fire-safety-requirements- for-certain-health-care-facilities-medicare-and- medicaid-programs. The deadline to submit comments is June 16. H
Writing books and speaking on audio conferences and at
seminars are great ways to share your industry knowledge
with peers. With the guidance of a solid publishing company,
you’ll see your thoughts and tips become beacons to others in
your field.
We’re always looking for new authors, speakers, and
reviewers, and we offer competitive compensation. For more
than 20 years, HCPro has been a leading provider of integrated
healthcare information, education, training, and consulting
products. Among HCPro’s need-to-know information products
are a vast array of books, newsletters, websites, annual
broadcast events, and annual live events.
Contact me at [email protected] and let me know your
areas of expertise and interests in publishing or training. Please
do not send unpublished manuscripts or specific proposals for
future works.
—Matt Phillion
Senior Managing Editor
We’re seeking experts for books, audio conferences, and seminars
Healthcare Life Safety ComplianceJune 2014
7HCPRO.COM© 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Documentation strategies for fire safety equipment
Surveyors and inspectors, whether they are from The Joint Commission, HFAP, DNV, CIHQ, or your state agency surveying on behalf of CMS, all find it a bit frustrating when they have to wait and wait for hospital facility managers to dig through their piles of paper-work in search of a specific test or inspection report. And making a surveyor frustrated is not a good thing during a survey.
Surveyors will cite an organization for noncompli-ance with a standard if the hospital cannot present the evidence to document that a test or inspection related to the standard was completed —regardless of whether the hospital actually performed that test or inspec-tion. As such, a couple of hours of preparation prior to the survey can help make the whole documentation review process go a lot easier.
It is suggested that you put all the inspection and testing work orders or contractor reports in a three-ring binder, and categorize them by topic. Maintain the binders in an area where they are easily retrievable by anyone in case you are not on-site when the survey begins. You can have a single binder covering multiple categories or multiple binders each covering a single category, whatever method works for you. Since fire alarm test reports can be rather lengthy, they may deserve their own binder. Similarly, some contracted testing/inspection reports may be presented to you in their own binders.
Each binder should reflect one year’s worth of docu-mentation for the category (or categories) it covers, or one inspection/test if the intervals for that test are more than one year long. For example, it doesn’t make sense to have a yearly binder for fire & smoke damper testing when the test intervals are every six years for hospitals.
In your binders, only include documents that actually demonstrate a test or an inspection was performed. Do not include copies of invoices, purchase orders, or any other irrelevant documentation. All too often a hospital will present a purchase order or a contractor’s invoice as evidence that a life safety device was tested. These
documents don’t prove the device was tested, only that you contracted or paid someone to do so. Do not add unnecessary information, such as a reprint of the standard that specifies the testing/inspection activities. The surveyors are not interested in that; they only want to see the evidence that proves the devices were tested or inspected.
If a device was found to be defective or impaired during a testing/inspection activity and it was not repaired/replaced the same day the defect was dis-covered, make sure you have a copy of the interim life safety measures (ILSM) assessment document in the binder. All Life Safety Code® (LSC) deficien-cies need to be assessed for ILSMs when they can-not be immediately resolved. Having proof that you assessed the deficiency for ILSMs in the binder right next to the report is a turnkey approach to managing the problem.
If repairs or follow-up activities are required, include copies of work orders, contractor test reports, or work tickets that demonstrate the device was repaired or replaced and retested. You must be able to prove to the surveyor that the device was repaired or replaced, that the repaired or replaced device was tested, and that it passed its test. Have a copy of this information stapled to the test report so you don’t have to spend time look-ing for it. Make sure all of these documents are legible. You may need to request originals where carbonless copies are not readable.
A common question concerning documentation is, “How long must I keep test and inspections reports?” The generally accepted answer to that is forever. Don’t throw anything out. You never know when you will need to prove something to your boss, a surveyor, or (heaven forbid) a lawyer.
The Joint Commission states that it wants to see a 12-month track record for testing and inspection on all fire safety systems, or back to the last cycle of test-ing, whichever is longest, but the accreditor does have the right to look back even farther if it wants. There have been multiple cases where surveyors found
Healthcare Life Safety Compliance June 2014
8 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
On April 10, an explosion occurred in The University Medical Center of Princeton at Plainsboro (New Jersey) and left a nurse in critical condition. The explosion occurred in a patient room on the third floor shortly before 9 p.m. The nature of the woman’s injuries was not disclosed, but an eyewitness to events following the blast said he saw a woman lying on the floor, possibly unconscious, with a facial injury.
Preliminary findings indicate that a compressed oxygen cylinder exploded, followed by a brief fire. It was not immediately clear whether the explosion was due to excessive pressure, excessive heat, or other factors. It is apparent that the oxygen enriched the nurse’s clothing and surrounding linen, leading to a fire that resulted in major burns for the healthcare worker.
The patient and visitor who were in the room with the nurse each suffered smoke inhalation. Eighteen patients in rooms near where the explosion occurred were moved to rooms on other floors.
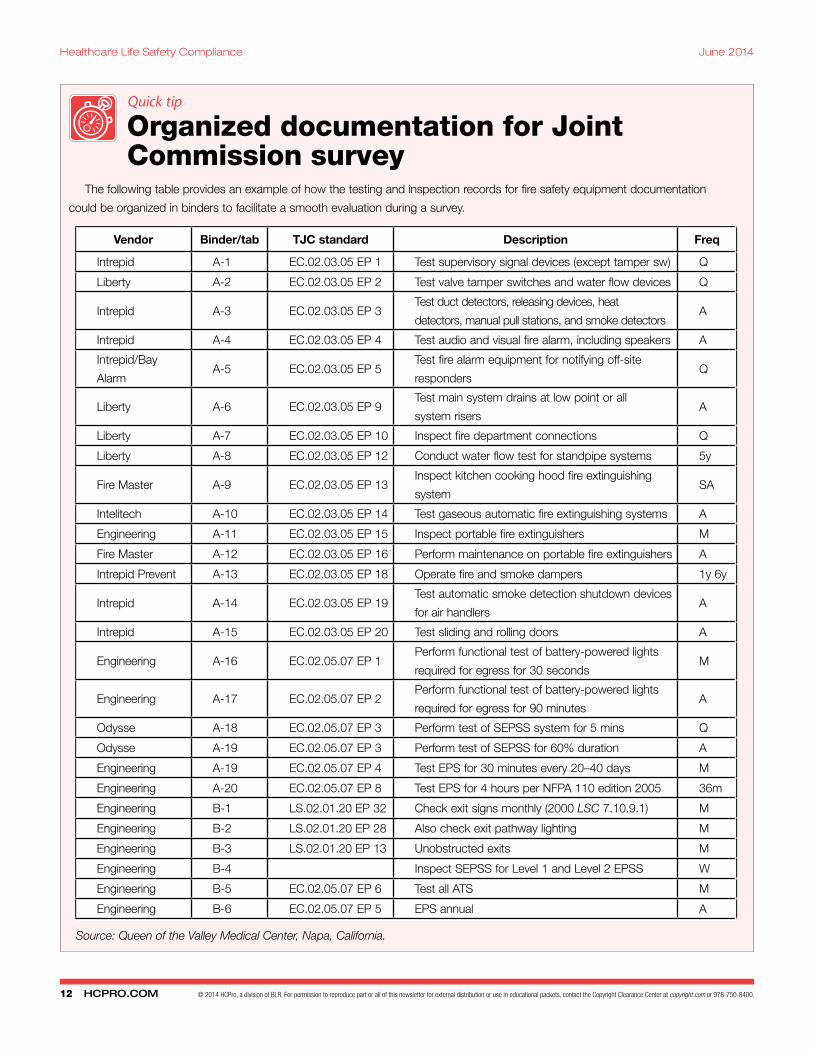
“I have applied this method with success for years now,” says Taquin. “All of our binders have an Excel spreadsheet showing the Joint Commission EC and LS standards, organizing the documents in the same order as they are found in the standards.”
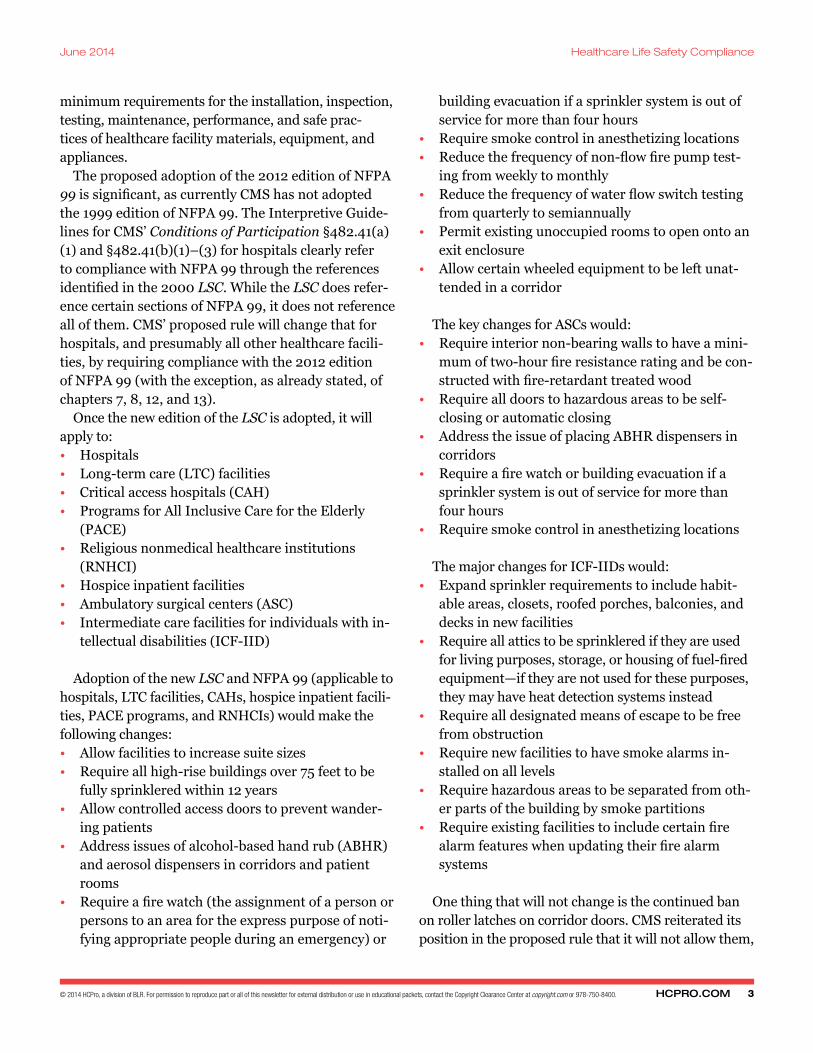
Taquin is referring to a matrix that he developed, which is repeated for you on p. 12.
“The spreadsheet allows me to update the standards and the documents to ensure continuous readiness,” he says. “The matrix not only helps us organize our documents, but it also impresses the surveyors that we know what we are talking about, we are organized, and we are compliant.”
Taquin is not just showboating when he says this. Surveyors really do pay attention to how well organized the documentation is, which can positively affect the overall survey.
“I have rarely seen a surveyor go very deep into the binders once he realizes how organized we are,” says Taquin. “When the LSC surveyor says to our adminis-tration at the exit conference that he is going to feel good driving home because the place is in such good hands, you know that you have succeeded.” H
something that was suspect or wrong, such as a lack of proper main drain tests being conducted, and they traced back three years to see if the test was ever done successfully. This is ultimately helpful to the hospi-tal—in many cases, it allows the organization to prove to the surveyor that the test was originally conducted but, for whatever reason, just was not conducted at the time of the survey. If a surveyor realizes that the organization has a history of the test being conducted but the test simply got missed somehow, that may prevent a more serious finding under a leadership standard requiring staff to be held accountable for their responsibilities.
Some state agencies who perform validation sur-veys on behalf of CMS want to see three years’ worth of testing and inspection documentation for all fire safety systems. It is apparent that these agen-cies can and will hold you accountable for all of this documentation.
The three-ring binder strategy has worked well for years for Philippe Taquin, CHFM, director of engineering and safety officer for Queen of the Valley Medical Center in Napa, California.
Oxygen cylinder suspected in hospital explosion Multiple witnesses said that the explosion was very
loud. One man who was three floors above the explo-sion said it sounded like a “gunshot.”
Princeton resident Vito Tortaro said he was on the same floor where the explosion occurred, visiting his mother. According to Tortaro, the scene was chaotic as people ran around, smoke filled the air, and ceiling tiles buckled. He described seeing the nurse on the floor before she was taken away on a stretcher.
When fire and rescue workers arrived on scene Thursday, they did not see any fire, according to Plains-boro Fire Lt. Tom Healey. He said that ceiling tiles in the affected room had buckled from the explosion and there was a “haze” when first responders arrived. Thermal imaging equipment did not detect any fire in the walls, and the incident was mainly confined to one room, Healey said.
In a statement, hospital officials said the explosion happened at about 8:50 p.m. “The fire department was

Healthcare Life Safety ComplianceJune 2014
9HCPRO.COM© 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
immediately called. One staff member was seriously hurt and a visitor is currently being evaluated,” the state-ment said. “As a precautionary measure, 18 patients on the unit were moved to other floors within the hospital. The cause of the explosion is under investigation, but is believed to be accidental and related to an oxygen tank.”
Ten days after the incident, Barry S. Rabner, presi-dent and CEO of Princeton HealthCare System, which owns and operates the University Medical Center of Princeton at Plainsboro, released this statement to the local press:
I am writing to express our deep appreciation for the exceptional work of local first responders following the explosion at University Medical Cen-ter of Princeton at Plainsboro last Thursday night.
The collaboration between all first responders at the hospital that night helped us to ensure the safety and well-being of our patients and visitors, as well as the injured staff member.
An oxygen cylinder exploding in a patient room, away from the usual sources that would cause excessive heat or pressure, may be baffling to many. But the circum-stance is not entirely unheard of. As far back as 1996, contaminated aluminum body regulators have been identified as the cause of oxygen cylinder explosions. The International Association of Fire Fighters (IAFF) conducted its own investigation after several of its mem-bers were injured from exploding oxygen cylinders. As a result, the IAFF requested that the FDA take action and demand a recall on the suspect regulators.
In 1998, the FDA announced that Allied Healthcare Products, Inc., issued a recall on its regulator models L270-020 and L270-050. The FDA notice identified that the regulators were involved with six exploding oxygen cylinders over the previous three years. Inves-tigations revealed the regulator fires were the result of contamination (grease, oil, or a substance containing hydrocarbons) introduced into the regulators during maintenance or use.
Further, in March 1999, Allied Healthcare Products announced another recall of all oxygen regulators sold under the Life Support Products (LSP) brand to replace aluminum components in the regulator’s high-pressure chambers with brass components. The models subject to the second recall included LSP 106,
LSP 270, LSP 280, LSP 370, and LSP 735 regulators.A paper published in the November/December 2008
issue of ASTM Standardization News explains the gen-esis of oxygen regulator fires resulting in catastrophic explosions:
When the cylinder valve is opened by using the valve handle, high pressure oxygen expands across the valve seat, flows into the regulator and rapidly recompresses at the regulator valves seat. The compression of oxygen generates heat within the gas and can be sufficient to ignite nonmetallic materials such as the seat of the regulator. This is known as heat of compression ignition.
Other than igniting the regulator materials, heat of compression is capable of igniting any con-taminants present. Contaminates (i.e., flammable foreign matter not intended to be present in oxy-gen components) such as hydrocarbon oils are eas-ily ignited by heat of compression compared to the solid materials. Once ignited, contaminants can re-lease sufficient energy from their heat of combus-tion to kindle the materials in the regulator.
The IAFF issued advice on the proper use, storage, handling, and maintenance of regulators:• Replace aluminum regulators with oxygen regula-
tors constructed of materials having oxygen com-patibility at least equivalent to brass.
• Make sure that staff using oxygen equipment are adequately trained in its operation and in oxygen safety, and have knowledge of manufacturer’s in-structions for using the equipment.
• Visually inspect the post valve gasket and regulator inlet prior to installation. If they are not visually clean, they should not be used.
• Momentarily open and close (“crack”) the post valve to blow out debris prior to installing a regulator.
• Ensure that the regulator is set with the flow knob in the off position before attaching it to the cylinder.
• Position the equipment so the valve is pointed away from the user and other persons.
• Open the cylinder valve slowly and completely to minimize the heat produced and achieve the de-sired flow conditions within the equipment.
• Do not look at the regulator pressure gauge until the cylinder valve is fully opened. H
Healthcare Life Safety Compliance June 2014
10 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
&AnswersQuestions
Editor’s note: Each month, Senior Editor Brad Keyes, CHSP, owner of Keyes Life Safety Compliance, answers your questions about life safety compliance. Our editorial advisory board also reviews the
Q&A column. Follow Keyes’ blog on life safety at www.keyeslifesafety.com for up-to-date information.
Walk-in coolers
Q During a recent survey, the life safety surveyor wrote a finding that my refrigerator and freezer
walk-in coolers are not in compliance with the build-ing having full sprinkler coverage. The walk-In cool-ers were installed prior to 1982, and two units do have sprinklers, but three do not. The state fire marshal re-viewed us and said we’re okay. What do you think?
A It appears to me that the issue is whether you’re taking credit for the building being ful-
ly sprinklered. If you have a certain construction type (see Table 19.1.6.2 of the 2000 Life Safety Code®
[LSC]) that requires sprinklers; if you have equiva-lencies or waivers that requires the building to be ful-ly sprinklered; if you have performed any renovations or alterations in the walk-in coolers since March 11, 2003; or if you have delayed egress locks located any-where in the building, then yes, the walk-in coolers must be protected with sprinklers. But if none of that has occurred and there is no apparent requirement for the smoke compartment where the walk-in cool-ers are located (or for the entire building) to be sprin-klered, then you should be okay.
Keep in mind that it doesn’t matter that one of your authorities having jurisdiction (AHJ) approved this installation. If another AHJ disagrees, it is that AHJ’s privilege to enforce the codes and standards as it understands them; the AHJ is not bound by what the state fire marshal says. Installing dry-head type
sprinklers in freezing environments is not that diffi-cult, nor is it particularly expensive. I would consider upgrading and installing dry-heads.
Clinic: Business occupancy
Q Our new clinic integration program has made us look closely at the clinic’s life safety process.
The clinic is classified as a business occupancy. Is the assessment for life safety compliance different than an acute care hospital?
A While the clinic is classified as a business occupancy, the approach to a life safety
assessment would be similar to conducting a life safety assessment for a healthcare occupancy (hospital); however, you would not assess the clinic to the same set of standards as a hospital. Healthcare occupancies must comply with the core chapters of the 2000 LSC, which are chapters 1–4 and 6–11, and they have to comply with the occupancy chapters 18 and 19. Business occupancies likewise have to comply with chapters 1–4 and 6–11, but they have a different set of occupancy chapters to comply with: chapters 38 & 39. Chapter 38 is for new construction and chapter 39 is for existing construction. A facility is considered new construction if its construction plans and documents were approved by the local authorities after March 11, 2003. A facility is considered existing construction if its construction plans and documents were approved by the local authorities on or before March 11, 2003. Also, any renovation conducted in existing construction buildings on or after March 11, 2003, must comply with new construction requirements.
Why the date of March 11, 2003? This is the date that CMS adopted the 2000 edition of the LSC. Assuming your clinics qualify for exist-ing construction occupancy, you must assess the
Healthcare Life Safety ComplianceJune 2014
11HCPRO.COM© 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
building for compliance with Chapter 39. You will find that the life safety requirements are far less restrictive for business occupancies as compared to healthcare occupancies. Examples where there will be significant differences (and leniencies) in compliance are:• Construction type (39.1.6)• Overhead rolling fire doors (39.2.2.2.7)• Means of egress arrangement (39.2.5)• Emergency lighting (39.2.9)• Hazardous areas (39.3.2)• Fire alarm systems (39.3.4)• Sprinkler systems (39.3.5)• Corridor walls (39.3.6)• Smoke compartments (39.3.7)• Fire drills (39.7.1)• Fire extinguisher training (39.7.2)
While fire damper testing in healthcare occu-pancies enjoys a six-year cycle, that is not the case in business occupancies, which requires a four-year testing interval. You will have to research each issue individually to determine your level of compliance.
Emergency lighting
Q Is there a NFPA standard for emergency lighting placement in an anesthetizing location? A spe-
cific requirement where on the wall or ceiling it must be mounted? Do the self-check devices still require a manual 30-second and 90-minute test?
A NFPA 99 (1999 edition) section 3-3.2.1.2(a)(5) discusses electrical needs in anesthetizing loca-
tions. Basically, all it says is that one or more battery-powered emergency lighting units must be installed in accordance with NFPA 70, article 700-12(e), which describes the electrical requirements for an emergen-cy lighting fixture, such as:• A rechargeable battery• A battery charging means• Provisions for one or more lamps mounted on
the equipment• A relay device to energize the emergency lighting
upon loss of normal power
Article 410 of NFPA 70 discusses lighting fixtures and locations in general. Basically, the article address-es wet, damp, corrosive locations; as well as mounting fixtures in closets, in ducts and hoods, in showers, and near combustible materials; but it does not address where fixtures need to be mounted for anesthetizing locations. A further review of NFPA 99 does not reveal anything about location of emergency lighting. Neither NFPA 110 nor NFPA 111 addresses emergency lighting locations. Section 7.9 of the 2000 edition of the LSC does discuss emergency lighting, and it uses the term “means of egress” to describe where emergency light-ing needs to be located, but specific to wall or ceiling mounting.
While fire damper testing in health-care occupancies enjoys a six-year
cycle, that is not the case in business occupancies, which requires a four-year testing interval. You will have
to research each issue individually to determine your level of compliance.
Ironically, this section does not require battery-powered fixtures for emergency lighting needs and references NFPA 110 if emergency lighting is powered by generators. Therefore, in this case, NFPA 99 would supersede the LSC, and you would need to install battery-powered emergency lighting in anesthetizing locations, even if you had generator-powered emer-gency lighting.
Section 7.9.3 of the LSC does require 30-second testing of battery-powered emergency lighting fixtures at 30-day intervals, as well as 90-minute tests annually. However, in lieu of the regular monthly 30-second tests, the exception to 7.9.3 does allow self-diagnostic battery-powered emergency lighting equipment that automatically performs a test for not less than 30 seconds not less than every 30 days and indicates failures by a status indicator. Such equipment is exempt from the 30-day func-tional test, provided a visual inspection is performed at 30-day intervals. H
Healthcare Life Safety Compliance June 2014
12 HCPRO.COM © 2014 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Vendor Binder/tab TJC standard Description Freq
Intrepid A-1 EC.02.03.05 EP 1 Test supervisory signal devices (except tamper sw) Q
Liberty A-2 EC.02.03.05 EP 2 Test valve tamper switches and water flow devices Q
Intrepid A-3 EC.02.03.05 EP 3 Test duct detectors, releasing devices, heat
detectors, manual pull stations, and smoke detectorsA
Intrepid A-4 EC.02.03.05 EP 4 Test audio and visual fire alarm, including speakers A
Intrepid/Bay
AlarmA-5 EC.02.03.05 EP 5
Test fire alarm equipment for notifying off-site
respondersQ
Liberty A-6 EC.02.03.05 EP 9 Test main system drains at low point or all
system risersA
Liberty A-7 EC.02.03.05 EP 10 Inspect fire department connections Q
Liberty A-8 EC.02.03.05 EP 12 Conduct water flow test for standpipe systems 5y
Fire Master A-9 EC.02.03.05 EP 13 Inspect kitchen cooking hood fire extinguishing
systemSA
Intelitech A-10 EC.02.03.05 EP 14 Test gaseous automatic fire extinguishing systems A
Engineering A-11 EC.02.03.05 EP 15 Inspect portable fire extinguishers M
Fire Master A-12 EC.02.03.05 EP 16 Perform maintenance on portable fire extinguishers A
Intrepid Prevent A-13 EC.02.03.05 EP 18 Operate fire and smoke dampers 1y 6y
Intrepid A-14 EC.02.03.05 EP 19 Test automatic smoke detection shutdown devices
for air handlersA
Intrepid A-15 EC.02.03.05 EP 20 Test sliding and rolling doors A
Engineering A-16 EC.02.05.07 EP 1 Perform functional test of battery-powered lights
required for egress for 30 secondsM
Engineering A-17 EC.02.05.07 EP 2 Perform functional test of battery-powered lights
required for egress for 90 minutesA
Odysse A-18 EC.02.05.07 EP 3 Perform test of SEPSS system for 5 mins Q
Odysse A-19 EC.02.05.07 EP 3 Perform test of SEPSS for 60% duration A
Engineering A-19 EC.02.05.07 EP 4 Test EPS for 30 minutes every 20–40 days M
Engineering A-20 EC.02.05.07 EP 8 Test EPS for 4 hours per NFPA 110 edition 2005 36m
Engineering B-1 LS.02.01.20 EP 32 Check exit signs monthly (2000 LSC 7.10.9.1) M
Engineering B-2 LS.02.01.20 EP 28 Also check exit pathway lighting M
Engineering B-3 LS.02.01.20 EP 13 Unobstructed exits M
Engineering B-4 Inspect SEPSS for Level 1 and Level 2 EPSS W
Engineering B-5 EC.02.05.07 EP 6 Test all ATS M
Engineering B-6 EC.02.05.07 EP 5 EPS annual A
Quick tip
Organized documentation for Joint Commission survey
The following table provides an example of how the testing and inspection records for fire safety equipment documentation
could be organized in binders to facilitate a smooth evaluation during a survey.
Source: Queen of the Valley Medical Center, Napa, California.
1. (T) (F) CMS published its final rule to adopt the 2012 Life Safety Code® (LSC) in April.
2. (T) (F) The final rule to adopt the 2012 LSC must be voted on by Congress and signed into law by the president.
3. (T) (F) CMS is also proposing to adopt the 2012 edition of NFPA 99 because NFPA 99 is now a code rather than a standard.
4. (T) (F) In its proposed rule, CMS reiterates its current position and will continue to ban roller latch-es for corridor doors.
5. (T) (F) CMS notes that the Americans With Disabilities Act (ADA) requires corridor projections to be no more than 4 inches, but it proposes to accept the 2012 LSC allowance of 6-inch projec-tions in corridors.
6. (T) (F) In its proposed rule to adopt the 2012 LSC, CMS states that as the authority having jurisdic-tion for certification, it alone will approve equivalencies.
7. (T) (F) High-rise healthcare occupancies that are not fully sprinklered will have to install sprinklers within 12 years after the 2012 LSC is adopted.
8. (T) (F) Surveyors will accept purchase orders and invoices as evidence that a life safety feature was tested.
9. (T) (F) A can of cleaning fluid was suspected as the source of explosion and fire in the University Medical Center of Princeton at Plainsboro (New Jersey).
10. (T) (F) Allied Healthcare Products, Inc., had multiple recalls on its regulators with aluminum components.
QuizQuizHealtHcare life Safety complianceThe newsletter to assist healthcare facility managers with fire protection and life safety
Vol. 16 No. 6June 2014
Quiz questions June 2014 (Vol. 16, No. 6)
A supplement to Healthcare Life Safety Compliance
Quiz answers June 2014 (Vol. 16, No. 6)
1. False. CMS published its proposed rule to adopt the 2012 LSC in April. The final rule will be pub-lished after the 60-day comment period closes and CMS reviews all of the comments.
2. False. This is a myth. According to the Administrative Procedure Act of 1946, Congress does not vote on final rules, and the president does not sign them into law.
3. True.
4. True.
5. False. CMS proposes to adopt the ADA limitation of 4 inches for corridor projections, even though the LSC allows 6 inches.
6. True.
7. True.
8. False. Purchase orders and invoices do not demonstrate that a life safety feature was tested or inspected, and they have no bearing as evidence.
9. False. An oxygen cylinder was identified as the source of explosion and fire.
10. True.
Copyright 2014 HCPro, a division of BLR. Current subscribers to Healthcare Life Safety Compliance may copy this quiz for use at their facilities. Use by others, including those who are no longer subscribers, is a violation of applicable copyright laws. ® Registered trademark, the National Fire Protection Association, Inc.