Embed Size (px)
DESCRIPTION
A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized unresectable pancreatic cancer: E4201. P. J. Loehrer Sr., M. Powell, H. Cardenes, L.Wagner, J. Brell, R. Ramanathan, C. Crane, S. Alberts, A. B. Benson - PowerPoint PPT Presentation
Citation preview

A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized unresectable pancreatic cancer: E4201
P. J. Loehrer Sr., M. Powell, H. Cardenes, L.Wagner, J. Brell, R. Ramanathan, C. Crane, S. Alberts, A. B. Benson
On behalf of The Eastern Cooperative Oncology Group

Faculty Disclosure
Research Funding:
- Eli Lilly- Novartis- AstraZeneca- Imclone

Background:Radiation in Pancreatic Cancer
• In locally advanced pancreatic cancer, radiation plus FU has been a standard of therapy (GITSG: Moertel,1981)
• Trials in the US and Europe have questioned the role of radiation in pancreatic cancer:– ESPAC (Neoptolemos JP,2001)2001) – ECOG: 5-FU vs. 5-FU plus XRT
(Klaassen,1985)

J Clin Oncol 3: 373-78, 1985

Background: Gemcitabine plus Radiation
• Gemcitabine in pancreatic cancer– Superior to 5-FU (Burris, 1997Burris, 1997)
– Potent radiation sensitizer in vitro (Lawrence, 1996).
• Numerous phase I/II trials with once or twice weekly gemcitabine plus radiation– Phase I trial (Fox Chase, Michigan, Indiana): 50.4 Gy
plus GEM (DLT- 600 mg/m2) (McGinn, ASCO 1997). – Phase II trial (HOG): Six PR/28 pts (21%), MST 7.9
mos and 31% one year survival (Moore, ASCO 2004)

E4201: Schema
ARM A: INDUCTIONGEMCITABINE 1000mg/M2
Once weekly x 6 weeks
ARM B: INDUCTIONGEMCITABINE 600 mg/M2
Once weekly x 6 weeksCONCURRENT RT 180 cGy/day
5 days week x 6 weeksTotal dose 50.40 Gy
ARM A: CONSOLIDATIONGEMCITABINE 1000mg/M2
Once weekly x 3 weeksFollowed by 1 week rest x 5 cycles
1 cycle = 4 weeks
ARM B: CONSOLIDATIONGEMCITABINE 1000mg/M2
Once weekly x 3 weeksFollowed by 1 week rest x 5 cycles
1 cycle = 4 weeks
1 week rest
4 weeks rest
Stratify:• PS (0 vs 1)
• Weight loss( >10% vs <10%)
RANDOMIZE

Radiation Therapy
• 3D-conformal Therapy• PTV1: 3960 cGy
– GTV (primary + gross nodal disease) + 2-3 cm margin
– Immediately adjacent lymph node regions + 1.5 cm margin
– Adjust margins to accommodate normal tissue tolerance requirements
– PTV2: 5040 cGy• GTV + 1.5-2 cm margin
• Treatment dose-volume were centrally reviewed (submitted within 3 days)

Endpoints
• Primary:– Overall Survival
• Secondary:– Response Rates– Progression Free Survival– Quality of Life (not presented today)

Inclusion Criteria
• Histological confirmation of adenocarcinoma or adenosquamous carcinoma of the pancreas
• Loco-regionally advanced disease• Unresectable disease without evidence of
metastasis• No prior therapy• Measurable or evaluable disease• Adequate hematological, renal and hepatic
functions• ECOG performance status of 0 or 1

Statistics
• Primary Endpoint: Overall Survival– 88% Power to detect a 50% difference in median
survival (8 months vs. 12 months)– Two-sided log-rank test (alpha = 0.05)– Accrual goal: 316 patients
• Activated April 2003; terminated December 2005– Reason: “poor accrual” (i.e. <10 entries per month)– Final accrual was 74 patients– All patients have expired
• Data updated May, 2008

Patient Population
GEM GEM/XRT
No. eligible patients 38 36
Ineligible (metastases) 1 2
Total evaluable for survival 37 34
Total evaluable for toxicity 35 34

Patient characteristics
GEM alone (n=37)
GEM plus XRT(n=34)
Median Age (yrs.) 68.7 65.7
% Female 51% 44%
PS = 1 76% 82%
>10% Weight Loss 43% 47%

Grade 3/4 ToxicitiesGEM alone
(n=35)
GEM plus XRT
(n=34)
p value*
Neutropenia 3% 12% ns
Thrombocytopenia 6% 21% ns
Hemorrhage 0% 3% ns
Gastrointestinal 14% 38% 0.03
Fatigue 6% 32% 0.006
Overall Grade 3/4 82% 93% ns
* Two sided Fisher’s exact test
Two grade 5 toxicities: Cardiac (GEM) and ARDS (GEM/XRT)

Response
GEM alone GEM plus XRT
Partial Resp. 5% 6%
Stable Disease 35% 68%
Progression 16% 6%
Inevaluable* 46% 21%
* Clinical “progression’ without confirmation scansor scans performed outside of scheduled times

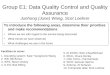
Overall SurvivalGEM
GEM plus XRT
GEM: Median Survival 9.2 Months (95% CI [7.8, 11.4]) -----------------------
GEM + Radiation: Median Survival 11.0 Months (95% CI [8.4, 15.5]) -----------------------
GEM
p-value = 0.034
Two-Sided, stratified Log rank

Survival
6 mos 12 mos 18 mos 24 mos
GEM alone 76% 32% 11% 4%
GEM plus XRT 74% 50% 29% 12%

Progression-Free Survival
p-value = 0.50
Two-Sided, stratified Log rank
GEM: Median PFS 6.7 Months (95% CI [4.6, 8.7]) -----------------------
GEM + Radiation: Median PFS 6.0 Months (95% CI [5.6, 8.4]) -----------------------
GEM plus XRT
GEM

Sites of Relapse
GEM alone GEM plus XRT
Local 41% 23%
Distant 14% 23%
Local and Distant 5% 9%
Not documented* 41% 44%
* Clinical “progression’ without confirmation scansor scans performed outside of scheduled times

Progression-Free Survival in Pancreatic cancer: Problems
• Definition of PFS: “The shorter of:– The time from registration to progression.– The time from registration to death from any
cause without documentation of progression”
• Difficulty measuring objective response
• Surrogate markers of progression (e.g. pain, anorexia, performance status)

“Explanations” for poor accrual
• Competing trials in metastatic disease include locally advanced disease
• Dosages of gemcitabine not equal
• “Unethical” not to use radiation therapy
• “Unethical” to use radiation therapy

E4201: Limitations
• Survival only modestly prolonged
• Response Rate and PFS not different
• Toxicity: Treatment or disease related?
• Single study
• Small sample size

Conclusions
• Gemcitabine plus radiation therapy has superior survival compared to gemcitabine alone (11.0 mos vs. 9.2 mos; p=0.034)
• Similar PFS and overall response rates• Toxicity is very common, but manageable
in both arms (QOL to be reported later)• Locally advanced and stage IV pancreatic
cancers should be treated as separate entities

Final Personal Comments
• Clinical significance: – Some: an affirmation for radiation – Others: an underpowered trial
• If combined modality therapy is considered for locally advanced pancreatic cancer, gemcitabine is more attractive than 5-FU
• It remains a sobering reality that in nearly three decades of research, the true impact of radiation therapy in pancreatic cancer is still controversial

Acknowledgments
• The patients who participated in this study
• Those investigators and nurses within ECOG and the CTSU who continue to work hard for their patients and to seek knowledge on their behalf