Embed Size (px)
Citation preview

PEDIATRIC
GastroesophagealRefluxEVALUATION AND MANAGEMENT
Craig A. FriesenChildren’s Mercy HospitalKansas City, MO
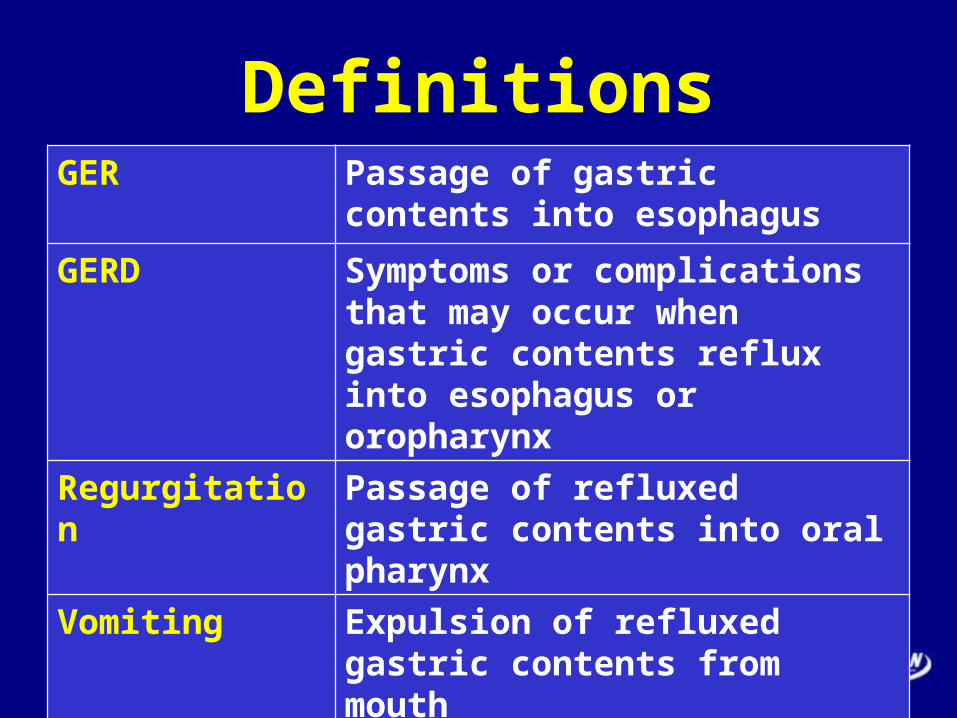
DefinitionsGER Passage of gastric contents into
esophagus
GERD Symptoms or complications that may occur when gastric contents reflux into esophagus or oropharynx
Regurgitation Passage of refluxed gastric contents into oral pharynx
Vomiting Expulsion of refluxed gastric contents from mouth
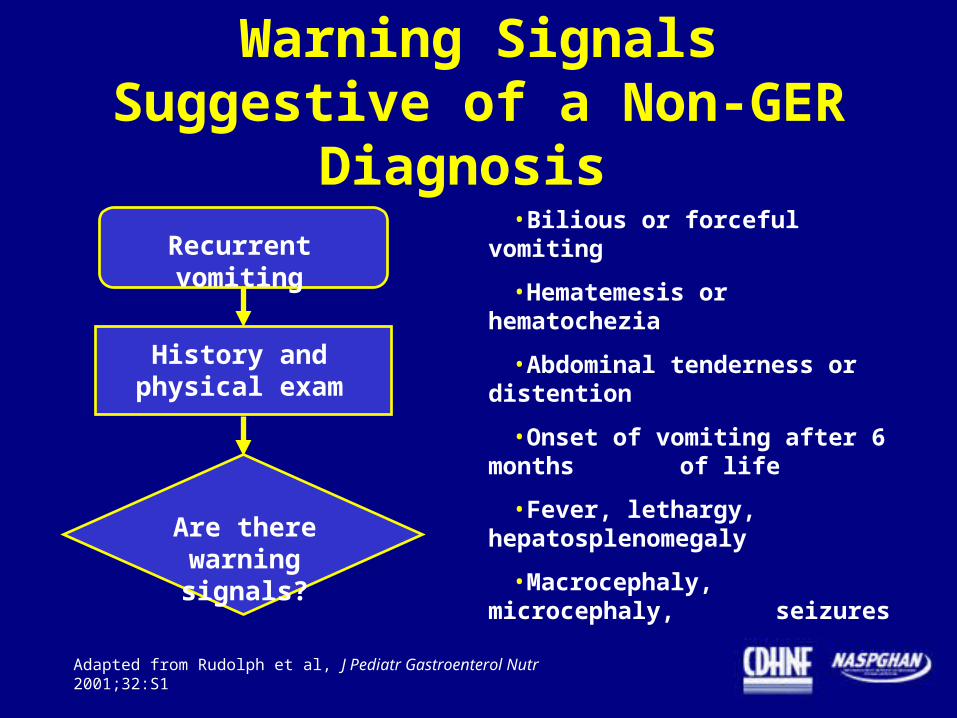
Warning Signals Suggestive of a Non-GER Diagnosis
Adapted from Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
•Bilious or forceful vomiting
•Hematemesis or hematochezia
•Abdominal tenderness or distention
•Onset of vomiting after 6 months of life
•Fever, lethargy, hepatosplenomegaly
•Macrocephaly, microcephaly, seizures
Recurrent vomiting
History andphysical exam
Are there warning signals?

Signs of Complicated GERD
Adapted from Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
•Poor weight gain
•Excessive crying or irritability
•Feeding problems
•Respiratory problems, including:
–wheezing
–stridor
–recurrent pneumonia
Recurrent vomiting
History andphysical exam
Are therewarning signals?
Are there signsof complicated
GERD?

Clinical Predictors of GERD
• Subjective symptom descriptions are unreliable in infants and children
• No symptoms or symptom clusters predict GERD complications
• No symptoms/clusters predict infants likely to respond to treatment
• ?diagnosis can be made in adolescents with typical heartburn symptoms

Cry Fuss Time in Response to Omeperazole in Infants with Esophagitis and /or Abnormal PH Study
0
50
100
150
200
250
300
Baseline Therapy
Omeperzazole
Placebo
(246)
(287)
(191)(201)
Cry Fuss Time(Mins/24 Hours)
Moore, Et al: J Pediatr, 2003

Open Label Omeperazole in Adolescents with Heartburn, Epigastria Pain, and Acid Regurgitation
0102030405060708090
100
Baseline 8 Weeks
(63.1)
(9.3)
% With ModerateSevereSymptoms
Gold, et al: JPGN, 2007

Esophageal pH Monitoring
•Cannot detect nonacidic reflux
•Cannot detect GER complications associated with “normal” range of GER
•Not useful in detecting association between GER and apnea unless combined with other techniques
Limitations
•Detects episodes of acid reflux
•Determines temporal association between acid GER and symptoms
•Assesses adequacy of H2RA or PPI dosage in unresponsive patients
Advantages

Non-Acid Reflux in Relation to Meals in Infants(N=34)
0
10
20
30
40
50
60
70
80
90
100
<1 Hour 1-2 Hours >2Hours
(61)
(39)
(29)
% of Total GER Episodes
Condino, et al; JPGN, 2006
Time After Meal

Physiologic Gastroesophageal Reflux(Mean upper limit of normal)
Infants
(N=509)
Children
(N=48)
Adults
(N=432)
No. of daily reflux episodes 73 25 45
No. of reflux episodes > 5 min 9.7 6.8 3.2
Reflux index (% of time pH < 4) 11.7% 5.4% 6%
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1

Difficulties in Interpreting pH Studies
• Normal ranges were determined with equipment and electrodes no longer in use
• ? Reproducibility• Sensitivity and specificity not well
established• ? Correlation with severity and/or
complications

Infant Gastroesophageal Reflux
45-90% OF GER EPISODES ARE
NON-ACIDIC

Multiple Intraluminal Electrical Impedance Measurement
Advantages• Detects nonacidic GER episodes
• Detects brief (<15 s) acidic GER episodes
• Useful for studying respiratory symptoms and GER in infants
Limitations• Normal values in pediatric age groups not yet defined
• Analysis of tracings time-consuming
• Portable device unavailable for outpatient studies
pH channel
pH 4
Impedancechannels
Z
t
1
Z4

PH Study Vs. Impedance for Correlating GER with Respiratory Symptoms in Children
0
10
20
30
40
50
PH Study Impedance
% Positive
Symptom
Indices
Rosen & Nurko; Am J Gastro, 2004
5.6%
33.3%

Adapted from Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms
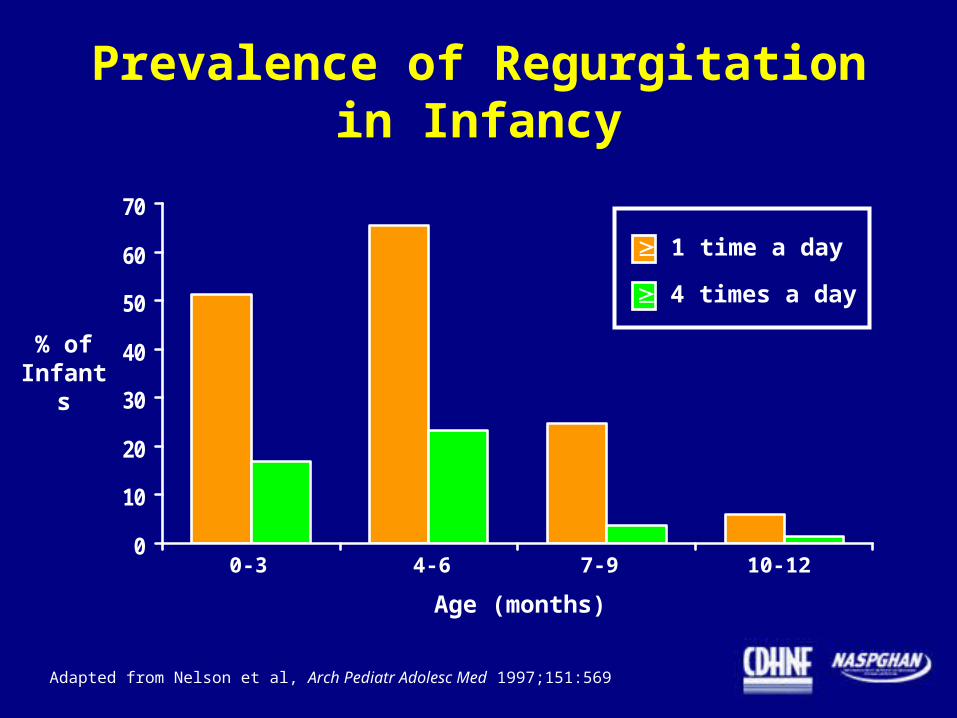
Prevalence of Regurgitationin Infancy
0
10
20
30
40
50
60
70
0-3 4-6 7-9 10-12
Age (months)
% of Infants
1 time a day
4 times a day
Adapted from Nelson et al, Arch Pediatr Adolesc Med 1997;151:569

Management of Infants With Recurrent Vomiting
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
•History & physical exam generallysufficient
•Parental education
– warning signals
– reassurance
•Consider
– thickened formula
– hypoallergenic formula
•Pharmacotherapy not recommended
•If no resolution by 18-24 months
– consider upper GI series or other test
– consider pediatric GI referralNo warning signals or signs of complicated GER

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Infant With Recurrent Vomitingand Poor Weight Gain
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
If warning signals present Consider other diagnoses
If inadequate calories offered Educate and follow up closely
If adequate calories offered Consider other causes of vomiting
•Metabolic disease
•Malabsorption
•Structural abnormalities

Management of Recurrent Vomiting and Poor Weight Gain
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
•Rule out other causes
•Optimize medical management
•Consider:–thickened feedings–hypoallergenic formula
•Follow up closely
•Consider EGD and biopsy
•Consider nasogastric or nasojejunal tube feeding

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Irritable Infant WithRecurrent Vomiting
•Minimal and conflicting evidence supports the contention that GER may cause irritability in infants
•Variations in parental perception of excessive crying/sleep disturbance complicate interpretation

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Older Child With Recurrent Vomiting
• No published studies on management of child who has vomiting
• Diagnostic approach? No data available
– Expert opinion suggests upper GI series
– No consensus regarding utility of endoscopy
• Treatment approach? Consider prokinetic

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Management of Heartburn or Chest Pain
H2RA or PPI for 2-4 weeks
Lifestyle changes:• Weight loss if obese• No alcohol• No caffeine• No smoking
No change Improvement
EGD with biopsy
Rx for2-3 months
Symptoms recur
•Symptoms may occur in presence or absence of esophagitis

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Evaluation and Management of Dysphagia or Odynophagia
Older Child/Adolescent
Barium esophagram to identify:- anatomic abnormality- motility disorder
Upper endoscopy with biopsy
Treatment without diagnostic evaluation not recommended
Infant
GER not demonstrated to cause feeding difficulties
Antireflux treatment not demonstrated to improve feeding
Empiric therapy for GER not recommended
If other symptoms suggest GERD time-limited medical therapy

Differential Diagnosis of Esophagitis
• Gastroesophageal reflux
• Food allergy or intolerance
• Primary eosinophilic esophagitis
• Drug induced
• Infection– Candida– herpes simplex– cytomegalovirus

Respiratory Symptoms of GER
• Apnea/ALTE
• Stridor and hoarseness
• Cough
• Wheezing
• Recurrent pneumonia

Prevalence of Gastroesophageal Reflux in Children With Pulmonary Disease
47 48 49
59 61 63 64
0
10
20
30
40
50
60
70
% of Patients
Friedland et al,1973
Berquist et al,1981
Shapiro et al,1979
Euler et al,1979
Danus et al,1976
Martin et al,1982
Buts et al,1986

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

ALTE
Definition Frightening episode in infant that is characterized by:
- apnea- change in color- change in muscle tone- choking or gagging
and requires intervention by caretaker
Potential causes - Cardiac disorder - Upper airway obstruction - CNS disorder- Infection- GER- Intentional suffocation

•Recurrent regurgitation in 60% to 70% of infants with ALTE
•Abnormal esophageal pH studies in 40% to 80%
•Relationship between GER and obstructive or mixed apnea most convincing when infant was:
–awake
–supine
–fed within past hour
GER and ALTE
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1

Association of GER with Apnea
Herbst et al, J Pediatr 1979;95:763
Time (sec)
EsophagealpH
NasalAirFlow
ChestWallMovement

Management of GER-Associated ALTE
•Esophageal pH monitoring is useful only if performed simultaneously with measurement of respiration and chest wall movement
•Infant is more likely to respond to antireflux therapy if:–emesis or regurgitation is present at time of ALTE–infant is awake–obstructive apnea is present
•Therapeutic options include:–thickened feedings–acid suppression
•Antireflux surgery is considered only in severe cases
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

GER Asthma
GER Asthma
GER Asthma
GER Asthma
Does GER Cause Asthma?

Effect of Antireflux Pharmacotherapy in Children
with Asthma
N=168 pts in 4 case series
Clinical improvement or reduced dosages of antiasthmatic therapy in 63% of asthma patients with GER treated with:• Conservative management• Prokinetic monotherapy• H2RA monotherapy
Duration of therapy (>3 months) important (adult studies)
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
63%

Effect of Antireflux Surgery in Children With Asthma
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
N=258 pts in 6 case series
•Clinical improvement or reduced dosages of
antiasthmatic therapy in 85% of children
•Persistent asthma requiring intensive steroid therapy before surgery
•GER most often confirmed by pH studies
•Failure of antireflux medical therapy did not preclude response to antireflux surgery
85%

Asthma: When to Treat for GERD
Persistent asthma and GER symptoms
Persistent asthma and no GER symptoms
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
Vigorous acid-suppressive therapy for 3 months, monitoring outcome variables
Consider esophageal pH monitoring or empiric treatment trial in children with
• recurrent pneumonia• nocturnal asthma > 1X weekly• corticosteroid dependence
If pH studies positive 3-month trial of antireflux medical therapy, monitoring outcome variables
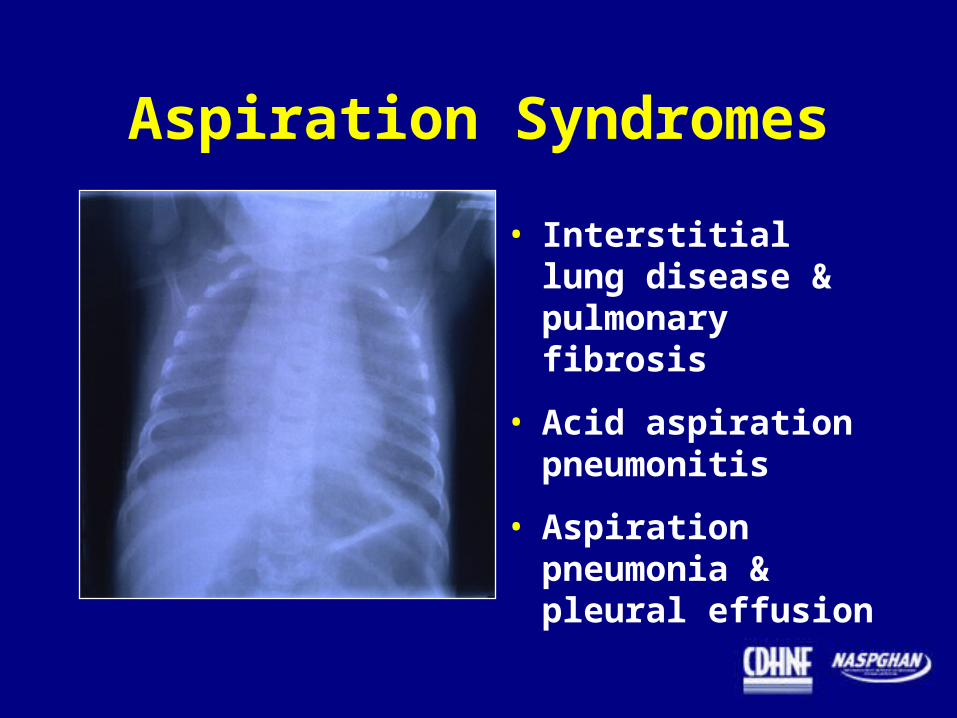
Aspiration Syndromes
• Interstitial lung disease & pulmonary fibrosis
• Acid aspiration pneumonitis
• Aspiration pneumonia &pleural effusion

Aspiration From Swallowing or GER?
Lipid-Laden Macrophages

Aspiration From Swallowing or GER?
Technetium-99m SalivagramBarium Swallow

Causes of Recurrent Pneumonia in Children
Aspiration 48 %
Immune disorder 10
Congenital heart disease 9
Asthma 8
Respiratory tract anomaly 8
GER 5
Other/unknown 12
N = 238 children hospitalized with pneumonia
Owayed et al, Arch Pediatr Adolesc Med 2000;154:190
Causes Frequency

Recurrent Pneumonia and GER
• GER can cause recurrent pneumonia in absence of esophagitis
• Normal esophageal pH studies do not exclude GER as a cause
• Before considering GER, rule out other causes
–neuromuscular disease or esophageal or laryngeal anatomic abnormalities
• Incidence of GER-related recurrent aspiration in otherwise healthy infants and children is rare
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1

Management of RecurrentPneumonia and GER
• Combination of tests may aid in diagnosis
–flexible bronchoscopy with pulmonary lavage
–nuclear scintigraphy
–swallowing assessment (VSS, FEES)
• Severely impaired lung function consider antireflux surgery
–balance potential benefits with potential complications
• Minimal pulmonary disease consider medical therapy

Presenting Symptoms and Signs of GERD
• Recurrent vomiting in infant
• Recurrent vomiting and poor weight gain in infant
• Recurrent vomiting and irritability in infant
• Recurrent vomiting in older child
• Heartburn in child/adolescent
• Esophagitis
• Dysphagia or feeding refusal
• Apnea or ALTE
• Asthma
• Recurrent pneumonia
• Upper airway symptoms

Normal Reflux laryngitis

Evaluation and Management of GER-Related Laryngeal Symptoms
• Laryngoscopy generally indicated to rule out anatomic abnormalities of airway protection
• No randomized controlled trials of antireflux therapy in adults or children with laryngeal symptoms
• Adult studies suggest that therapeutic trial must last >3 months to adequately assess efficacy
• Clinical improvement followed by recurrence off treatment association with GER
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1

Pharmacotherapy
• Antacids
• Histamine-2 receptor antagonists
• Proton pump inhibitors
• Prokinetic agents
• Surface agents

Adapted from Sanders SW, Clin Therapeutics 18, 2-34. Copyright 1996 by Excerpta Medica Inc.
Inhibition of Acid Secretionin Gastric Parietal Cell

Effect of H2RAs on Healing of Esophagitis
Cucchiara et al, J Pediatr Gastroenterol Nutr 1989;8:150
N = 32 children with esophagitis treated with cimetidine 30-40 mg/kg/d or placebo for 12 weeks
Cimetidine
Placebo 20%
Significant symptom improvement with cimetidine, not placebo
Simeone et al, J Pediatr Gastroenterol Nutr 1997;25:51
N = 26 children with esophagitis treated with nizatidine 10 mg/kg/d or placebo for 8 weeks
Nizatidine
Placebo
Esophagitis Healing
Esophagitis Healing
15%
71%
69%
“Vomiting” reduced in both treatment arms; significant improvement in other GERD symptoms only with nizatidine

Recommended Oral H2RADosages for GERD
Rudolph et al, J Pediatr Gastroenterol Nutr 2001;32:S1
Infants and Children Adults
Cimetidine 40 mg/kg/day divided TID or QID 1600 mg/day
Famotidine 1 mg/kg/day divided BID 20 or 40 mg BID
Nizatidine 10 mg/kg/day divided BID 150 mg BID or 300 mg HS
Ranitidine 5-10 mg/kg/day divided TID 150 mg BID - QID

Proton Pump Inhibition
Adapted from Sanders SW, Clin Therapeutics 18, 2-34. Copyright 1996 by Excerpta Medica Inc.

PPIs in Infants andChildren With GERD
• Pharmacologic studies with omeprazole and lansoprazole
• No randomized placebo-controlled trials
• Multiple case series of children refractory to H2RA
Pharmacology of Omeprazole in Children
• Pharmacokinetic (PK) values are generally within range previously reported for adults
• Children achieved these values with higher doses on per-kilogram basis than in adults
• Esophageal pH <4 for <6% of 24 h was achieved in 72% of 57 children with esophagitis with 0.7 or 1.4 mg/kg/day
Andersson et al, Am J Gastroenterol 2000;95:3101; Hassall et al, J Pediatr 2000;137:800
0
20
40
60
80
Overall Heartburn Dysphagia Irritability Coughing
% of Patients*
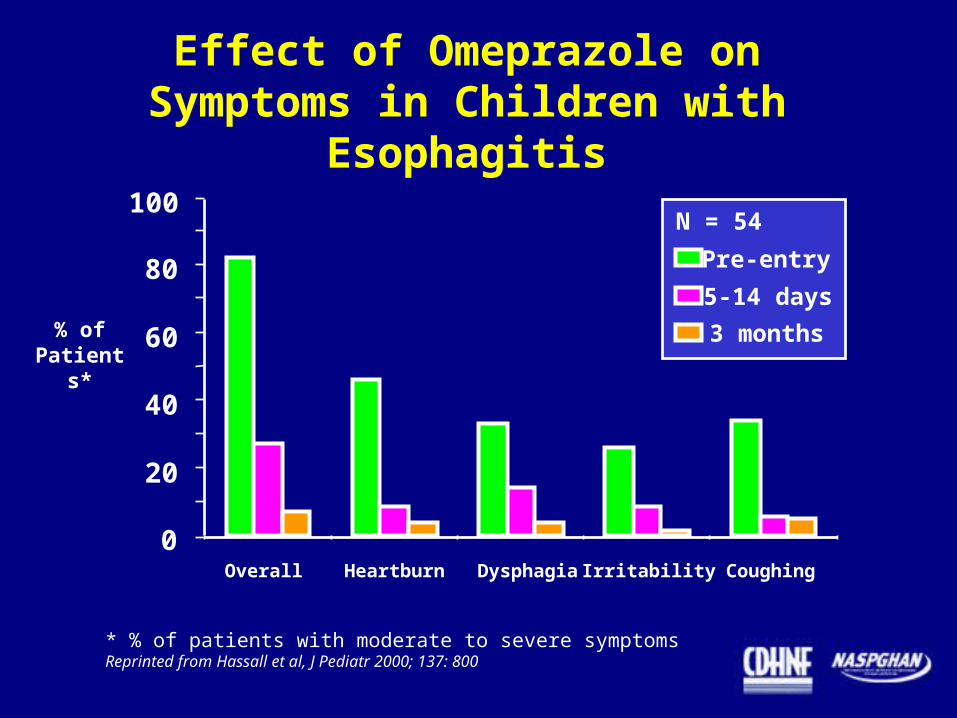
Effect of Omeprazole onSymptoms in Children with Esophagitis
* % of patients with moderate to severe symptomsReprinted from Hassall et al, J Pediatr 2000; 137: 800
Pre-entry
5-14 days
3 months
N = 54100

Effect of Lansoprazole on GERD Symptoms
Tolia et al, J Pediatr Gastroenterol Nutr 2002 suppl (in press)
N = 66 children with GERD symptoms treated with lansoprazole 15-30 mg QD-BID for 8-12 weeks
Median % of Days With GERD
Symptoms
100
80
60
40
20
0Baseline Wk 2 Wk 12
100%
79%
20%
P<.01
Optimal Timing of PPI Dose
Single PPI dose:
Administer 1 half-hourbefore breakfast
If second PPI dose:
Administer 1 half-hourbefore evening meal

Complications of Hypochlorhydria
• community acquired pneumonia
• gastroenteritis
• Candidemia
• necrotizing enterocolitis
• food allergy?





























