-
7/31/2019 P-Economics in Hospital
1/80
1
Strategic Management of Hospitals:
Pharmacoeconomics as a Decision Tool
Hiren Mehta
-
7/31/2019 P-Economics in Hospital
2/80
2
Outline
Healthcare costs and choices
Pharmacoeconomics
Definitions
Methods
Applications Advantages and disadvantages
-
7/31/2019 P-Economics in Hospital
3/80
3
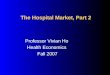
Canadian healthcare spending
1975-2005 (millions)
y = 1E-63e0.0782x
R2 = 0.9662
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
1970 1975 1980 1985 1990 1995 2000 2005 2010
-
7/31/2019 P-Economics in Hospital
4/80
4
Healthcare costs by type
0%
20%
40%
60%
80%
100%
1975 1980 1985 1990 1995 2000 2005
Other
Admin
Public Health
Capital
Drugs
Nursing, etc
Physicians
Institutions
Hospital
-
7/31/2019 P-Economics in Hospital
5/80
5
Trends hospital $ (Source: CIHI)
Hospital share is decreasing
From 44.7% in 1975 29.9% in 2005
28.7% decrease in share Hospital expenditures
$5.5 billion in 1975 [Total: $12 billion]
$42.4 billion in 2005 [Total: $142 billion]677% increase [Total:
1064%]
-
7/31/2019 P-Economics in Hospital
6/80
6
Trends drug $
Drug share increasing8.5% in 1985
17.5% in 2005
106% in share
Drug costs$1.1 billion in 1975
$24.8 billion in 20052200% increase
-
7/31/2019 P-Economics in Hospital
7/80
7
Reasons for increases Increase in utilization
More people taking drugs
More population
More >65, free drugs (access)
More disease more drugs
Longevity more disease more drugs
Increase in costResearch costs money
New drugs research intensive
-
7/31/2019 P-Economics in Hospital
8/80
8
Canada: population increase 1966-2006
y =0.3007x - 571.25
R2 =0.992
15
20
25
30
35
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010
-
7/31/2019 P-Economics in Hospital
9/80
9
Average cost per citizen covered
by BC PharmacareYear Cost
1987 $1921991 $354
1995 $406
1999 $478
-
7/31/2019 P-Economics in Hospital
10/80
10
Drug costs on the rise
-
7/31/2019 P-Economics in Hospital
11/80
11
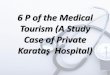
Costs of therapy (cancer drugs)
600
1,6204,980
7,600
12,000
18,000
26,000
0
5000
10000
15000
20000
25000
30000
$pertreatm
ent
Chl
oram
bucil
CHOP
Flud
arabin
e
CHOP
+G-CSF
Ritu
ximab
CHOP
+Ritu
ximab
Borte
zomib
Drug acquisition costs
-
7/31/2019 P-Economics in Hospital
12/80
12
Selecting drugs in hospital
Open formulary
No restriction
Pay for all drugs prescribed Formulary
Most standard drugs available
Medical staff + pharmacy decide on content Problem: demand
exceeds budget
Need a method for judging relative merits
-
7/31/2019 P-Economics in Hospital
13/80
13
Background
Economics = the study of the allocation ofresources
Health economics: application of economicprinciples to
healthcare
Basis = value for money
Money = common denominator forcomparisons
-
7/31/2019 P-Economics in Hospital
14/80
14
Pharmacoeconomics
Pharmaco = drugs
Application of health economics to drugs
and drug services
Techniques not different
Interpretations parallel
-
7/31/2019 P-Economics in Hospital
15/80
15
Levels of analysis
Macro (population)
Most PEA is this type
Applies to the average in the populationRequires translation to
apply to patients
Meso (group)
Usually applied at this level Micro (Individual)
Never done at this level in PEA
-
7/31/2019 P-Economics in Hospital
16/80
16
DefinitionPharmacoeconomics:
Evaluation of a drug against one or morecomparators with respect
toboth costsand outcomes.Comparator = depends on purpose
Placebo, do nothing
Standard treatment
-
7/31/2019 P-Economics in Hospital
17/80
17
Why?
Resources scarce
Demands increasing
Forced to make choice
Pharmacoeconomics assessesvalue for money(common metric)
A tool for decision making
-
7/31/2019 P-Economics in Hospital
18/80
18
Perspective Whose viewpoint?
Need to identify the audience for the report
Need to specify the analytic viewpoint
Determines:
Data collected
Valuation of resources
Interpretation of results
-
7/31/2019 P-Economics in Hospital
19/80
19
Analytic perspectives
Society (Comprehensive, overall)
All costs considered, regardless of payer
Usually includes indirect costs
Payer
Insurer, government, individual
Standard:Societal + Ministry of Health (Canada)
-
7/31/2019 P-Economics in Hospital
20/80
20
Types of cost
Direct costs
Indirect costs
Economic NOT accounting definitionsused in PEA
Overhead costs included in hospitalperspective
-
7/31/2019 P-Economics in Hospital
21/80
21
Direct costs
Costs of resources consumed in treating patients
Cost centres:
Drugs (preparation, administration, monitoring)
Medical care (MD, specialist) Hospital (inpatient, units)
Laboratory (blood, urine, x-ray, NMR, CAT scans)
Allied healthcare (nursing, physio, massage, social work)
Transportation to therapy (sometimes)
Cost of managing ADRs
-
7/31/2019 P-Economics in Hospital
22/80
22
Using costs
Use standard lists for cost values The standard price that any
person would pay
Do NOT use special costs, bargains
Exception: hospitals analyzing their own data
Select year of analysis Usually current year or immediate past
year
Standardize all costs to year of analysis Use health component
of Consumer Price Index or
equivalent
-
7/31/2019 P-Economics in Hospital
23/80
23
Indirect costs Lost productivity
Early death Time totally lost forever
Decreased ability to work Absenteeism due to disease
Presenteeism On the job, being paid, not inefficient
Caretaker time Problems
Leisure time, retired people
Consider lost time equal Under-employment/unemployment
Use Friction method Counts only time to train replacement
personnel
-
7/31/2019 P-Economics in Hospital
24/80
24
Time horizon
Analysis must be over enough time toallow for all important
outcomesCancer drugs use lifetime
Antibiotics (acute) 1 month/3 months
Often use 1 year
Problem
Data availability over timeMust discount costs if >1 year
-
7/31/2019 P-Economics in Hospital
25/80
25
Discounting
Preference for benefits now and costs later
NOT because of inflation
Based on stable rates for safe investments(government bonds,
GICs, cash market)
Standard = 5%, vary in sensitivity analyses
over range 0-10%
-
7/31/2019 P-Economics in Hospital
26/80
26
Summary: costs
A: Identify resources consumed B: Quantify resource use
C: Qualify (cost) that use
Use standard costsDiscount if over >1 year
Total cost = S Resourcei*Costi Average across all patients
Extrapolate to population using
demographic statistics
-
7/31/2019 P-Economics in Hospital
27/80
27
Outcomes: ECHO modelEconomicDollars
ClinicalPositive: Cure, life saved, life-year gained
Negative: Case avoided (disease, death)
HumanisticQuality of life, patient preferences
-
7/31/2019 P-Economics in Hospital
28/80
28
QALYs Quality adjusted life-years
e.g., cancer patient
Estimate duration of life remaining Identify health states
involved
e.g., Phases II-IVMeasure length of each health state Adjust
each by utility value:
S Timei*Utilityi Average over all patients
Universal outcome Can compare across treatments Can compare
across diseases
-
7/31/2019 P-Economics in Hospital
29/80
29
Utilities
Standard gamble
Time tradeoff
Visual analog scale Whose?Patients
Accurate estimate of implications
Problem: adaptation to the condition
Normals (society) Need to help them understand the disease
-
7/31/2019 P-Economics in Hospital
30/80
30
Preferred outcomes
Ultimate outcomes:Cure, life-year gained, QALY
Avoided cases of: Disease (vaccine)
Death
Avoid intermediate outcomesDecrease in BP, serum cholesterol,
units on a
scale (pain, health status, etc.)
-
7/31/2019 P-Economics in Hospital
31/80
31
Types of analyses
Cost-minimization
Cost-effectiveness
Cost-utility
Cost-benefit
Comparison ofefficacy /
effectiveness
Cost comparisonTwo or morealternatives
Cost-outcome
description (Non-comparative CBA)
Outcome
assessment (e.g.,Quality of Lifemeasurement)
Cost description
(Cost ofTreatment,Burden of Illness)
One (No
comparison ofalternatives)
Costs +Outcomes
Outcomesonly
Costs onlyAlternatives
-
7/31/2019 P-Economics in Hospital
32/80
32
Cost analyses (non-PEA)
Burden of sickness
Cost of illness
Financial feasibility
Implementing a new pharmacy service
E.g., cost-revenue model
-
7/31/2019 P-Economics in Hospital
33/80
33
Burden of sickness/illness Macro level (population based)
Top down analysis
Dollars spent on a disease
Direct costsDrugs, MD, hospital
Indirect costsMorbidity, mortality, time lost from work,
decreased productivity (presenteeism), etc.
-
7/31/2019 P-Economics in Hospital
34/80
34
Cost of illness/Cost of treatment
Micro level
Bottom up analysis
Individual based Itemize resources consumed
Drug, visits to MD, tests, etc.
Chart review, database analysis, modelled
-
7/31/2019 P-Economics in Hospital
35/80
35
Approaches to COI analysis Incidence based
Start at onset of disease Follow until resolution/death E.g.,
Gonzalez JC, Einarson TR. Cost of Type-2 diabetes in Colombia.
PharmacoEconomics 2008 (in press). Prevalence based
Cross sectional All cases in one year Example: Pain due to
multiple sclerosis: analysis of
the prevalence and economic burden in Canada. PainRes Manag
2007;12(4):259-65
-
7/31/2019 P-Economics in Hospital
36/80
36
Contribution
Identifies costs
Burden to society
Cost to treat individual Basis for pharmacoeconomic
evaluation
(Baseline)
BUT, does not address appropriateness or
outcomes
-
7/31/2019 P-Economics in Hospital
37/80
37
COI Example: bisphosphonatesResource Cost
Bisphosphonate $5,421
Other Drugs $6,290
Hospital $18,229
Clinic $7,715Laboratory $2,020
Imaging $3,355
Radiation $2,657Physicians $2,170
Total $47,857
Kruk. Supportive Care in Cancer2004; 12: 844-51.
-
7/31/2019 P-Economics in Hospital
38/80
38
Burden of ADRs (USA)
Resource Events Cost (millions)
Physician visits 115,654,949 $7,460
Additional prescriptions 76,347,604 $1,933
Emergency visits 17,053,602 $5,321
Hospital admissions 8,761,861 $47,445
LTC admissions 3,149,675 $14,399
Deaths 198,815Total $76,558
Johnson. Arch Intern Med 1995;155(18):1949-56.
O O O
O O O
-
7/31/2019 P-Economics in Hospital
39/80
39
HOSPITAL CARE EXPENDITURE BY DIAGNOSTIC CATEGORY,
CANADA,1993
DIAGNOSTIC CATEGORY 1993 Cost($1000)
% ofTotal
Cardiovascular Diseases 4,862,322 18.6
Mental Disorders 3,631,788 13.9
Cancer 2,467,408 9.5
Injuries 2,253,487 8.6
Digestive Diseases 2,093,374 8.0
Respiratory Diseases 1,788,230 6.9
Pregnancy 1,649,707 6.3
Well-patient Care 1,349,205 5.2
Musculoskeletal Diseases 1,285,910 4.9
Genitourinary Diseases 1,075,828 4.1
Nervous System and Sense Organ Diseases 792,862 3.0
Endocrine and Related Diseases 526,785 2.0
Perinatal Conditions 518,012 2.0
Infectious and Parasitic Dieseases 345,071 1.3
Birth Defects 231,923 0.9
Skin and Related Diseases 223,015 0.9
Blood Diseases 156,808 0.6
Ill-defined Conditions 844,567 3.2
TOTAL 26,096,300 100.0
SUBCATEGORY
Coronary Heart Disease 1,571,999 6.0
Stroke 1,258,063 4.8
Chronic Bronchitis / Emphysema / Asthma 636,491 2.4
Motor Vehicle Traffic Accidents 283,106 1.1
Diabetes 274,621 1.1
Female Cancers 206,068 0.8
HOSPITAL CARE EXPENDITURE BY DIAGNOSTIC CATEGORY,
CANADA,1993
DIAGNOSTIC CATEGORY 1993 Cost($1000)
% ofTotal
Cardiovascular Diseases 4,862,322 18.6
Mental Disorders 3,631,788 13.9
Cancer 2,467,408 9.5
Injuries 2,253,487 8.6
Digestive Diseases 2,093,374 8.0
Respiratory Diseases 1,788,230 6.9
Pregnancy 1,649,707 6.3
Well-patient Care 1,349,205 5.2
Musculoskeletal Diseases 1,285,910 4.9
Genitourinary Diseases 1,075,828 4.1
Nervous System and Sense Organ Diseases 792,862 3.0
Endocrine and Related Diseases 526,785 2.0
Perinatal Conditions 518,012 2.0
Infectious and Parasitic Dieseases 345,071 1.3
Birth Defects 231,923 0.9
Skin and Related Diseases 223,015 0.9
Blood Diseases 156,808 0.6
Ill-defined Conditions 844,567 3.2
TOTAL 26,096,300 100.0
SUBCATEGORY
Coronary Heart Disease 1,571,999 6.0
Stroke 1,258,063 4.8
Chronic Bronchitis / Emphysema / Asthma 636,491 2.4
Motor Vehicle Traffic Accidents 283,106 1.1
Diabetes 274,621 1.1
Female Cancers 206,068 0.8
-
7/31/2019 P-Economics in Hospital
40/80
Pharmacoeconomic
analysisProperties
ModelsOutcomesIssues
-
7/31/2019 P-Economics in Hospital
41/80
41
Pharmacoeconomic analysis
Compare 2 or more options Need to identify, describe each
Usually a new drug trying to enter the market
Requires an estimate for each of: Costs
Outcomes produced
Other requirements: Analytic time horizon, perspective, discount
rate(s)
Clinical consequences and their management
-
7/31/2019 P-Economics in Hospital
42/80
42
Purpose of PEA
Permission to market drug NOC in Canada
License in other countries
Acceptance by formulary Provided by system (e.g., ODB)
Paid by insurer (in whole or in part)
Purpose
model, approach
-
7/31/2019 P-Economics in Hospital
43/80
43
Approaches: licensure Population based model
Evidence = Efficacy data
Data source = RCTs
Assume full compliance, ideal conditions
Per protocol analysis Defined population
Limited to eligible patients who take full treatment
Comparator = placebo, standard
Viewpoint = societal
-
7/31/2019 P-Economics in Hospital
44/80
44
Approaches: formulary Meso (Group) model
Evidence = Effectiveness data
Data source: Effectiveness trials
Real life experience
Unselected patients
Compliance matters
Model via RCT + other factors (adherence)
Intent-to-treat analysis Population = all possible
candidates
Comparator = standard therapy
Viewpoint = payer
-
7/31/2019 P-Economics in Hospital
45/80
45
Product
Need to describe drug in detail
Identify therapeutic category
ATC system
Comparators
What is being used now
Utilization rates, costs, burden Justify WHY this drug is being
examined
-
7/31/2019 P-Economics in Hospital
46/80
46
Population
Indication
Disease How diagnosed, classified, e.g., ICD-10
Severity Mild, moderate, severe
Population
Types of patients Males, females Ages
-
7/31/2019 P-Economics in Hospital
47/80
47
Comparator Placebo
Form identical to drug of interest
Do nothing alternative
Standard therapyGuidelines
Actual practice
Expert panel
Hospital setting:
Usual treatment
-
7/31/2019 P-Economics in Hospital
48/80
48
Pharmacoeconomic modelsProspective
RetrospectivePredictive
-
7/31/2019 P-Economics in Hospital
49/80
49
Prospective models
Pharmacoeconomic RCT
Designed specifically for PEA
Add-on to clinical RCTPiggy-back trials
Collect data
Identify resources used
Cost concurrently or later
-
7/31/2019 P-Economics in Hospital
50/80
50
RCT advantages Prospective data collection
Data are stochastic Can calculate Mean, SD
All factors controlled Ideal conditions Provides efficacy
data
Valid for NOC, licensing
Disadvantages:
Sample not representative Patients, conditions, drugs taken,
age, sex, etc. Cannot extrapolate results to real life
-
7/31/2019 P-Economics in Hospital
51/80
51
Retrospective models
Model existing RCT
Chart review
Database analysis
-
7/31/2019 P-Economics in Hospital
52/80
52
Modelling RCTs Easy to do
Efficacy from trial
Determine costs
Problems: Retrospective bias
Artificial conditions (extrapolation)
Requires expert input
-
7/31/2019 P-Economics in Hospital
53/80
53
Chart Reviews Easy to do, not expensive (usually)
Problems:
Time consumingMissing data
Outcomes
Resources used (not planned for)
Patients d/c, re-entry, move
-
7/31/2019 P-Economics in Hospital
54/80
54
Database Analyses
Available, easy to use
Powerful - huge samples
Versatile:Cohort, case control, matching
Time series, cross sectional
-
7/31/2019 P-Economics in Hospital
55/80
55
Disadvantages
Missing data
Diagnosis, outcomes, status (smoking, alcohol, etc)
Confounding
Causation = ? Assumptions (Consumption, indication,
compliance)
Cost = large, delays long
-
7/31/2019 P-Economics in Hospital
56/80
56
Predictive decision models Most common model
Relatively easy to perform
Software (TreeAge/Data
) Often require expert panel
Applies to average patient
Population based
-
7/31/2019 P-Economics in Hospital
57/80
57
Decision Types
Decision treeFixed time period
Non-recursive (one-way only)All outcomes included
Markov modelRecursive model (can move backwards)
Cumulates values over time
Versatile
-
7/31/2019 P-Economics in Hospital
58/80
58
Markov model
EDSS 6-6.5
EDSS 5-5.5
EDSS 4-4.5
EDSS 3-3.5
EDSS 2-2.5
EDSS 0-1.5
Monosymptomatic
Clinically
Defined MS
Second Event
1st Year Transitions
Expanded Disability Status ScaleIskedjian et al. Multiple
Sclerosis2005; 11: 542-51
-
7/31/2019 P-Economics in Hospital
59/80
59
Markov model
Monosymptomatic
EDSS 0-1.5
EDSS 2-2.5
EDSS 3-3.5
EDSS 4-4.5
EDSS 5-5.5
EDSS 6-6.5
Second Event
Multiple Year Transitions
Iskedjian et al. Multiple Sclerosis2005; 11: 542-51
-
7/31/2019 P-Economics in Hospital
60/80
60
Base case analysis Identify what happens to the typical
patient
Number of treatments undergoneComponents of each treatment
Resources consumed
What happens if success, fail, etc.
-
7/31/2019 P-Economics in Hospital
61/80
61
Requirements for PEA
Drug of interest
Comparator(s)
Measurements of both Success (and/or other) rates Costs of
inputs (in $)
Patient outcomes
Outcomes expressed incrementally
-
7/31/2019 P-Economics in Hospital
62/80
62
Clinical efficacy
Source of data RCT
Head-to-head or IndirectObservational studies
Type of data
Intention to treat
Per protocol (completers)
-
7/31/2019 P-Economics in Hospital
63/80
63
PEA types
CCA = cost consequence analysis
CBA = cost benefit analysis
CMA = cost minimization
CEA = cost effectiveness
CUA = cost utility
-
7/31/2019 P-Economics in Hospital
64/80
64
Cost consequence (CCA)
No summary statistic calculated
Costs valued in $
Outcomes quantified and listed
Reader judges importance
Could be in every PEA
-
7/31/2019 P-Economics in Hospital
65/80
65
Cost benefit (CBA)
Measurement:Costs $
Outcomes $ Benefit: Cost ratio calculatedB:C >1 socially
beneficial
Incremental ratio used
-
7/31/2019 P-Economics in Hospital
66/80
66
CBA example
If a program costs $2000 and produces$5000 in benefits, as
compared with theexisting program costing $1000 with
benefits of $2000, Ratio1 = $5000/$2000 = 2.5
Ratio2 = $2000/$1000 = 2.0
Since ratio1:2 = 2.5/2.0 =1.25 >1, the newprogram produces
more benefits and ispreferred, if affordable
-
7/31/2019 P-Economics in Hospital
67/80
67
CBA Advantages:
Theory based
Can use willingness to pay
Contingent valuation
Disadvantages
Valuations
Intangibles (pain, suffering)
-
7/31/2019 P-Economics in Hospital
68/80
68
Cost minimization (CMA)
All outcomes sameMust be demonstrated
Consider only costs Decision rule: lowest cost is preferred
choice
Example: gent vs tobra ??
-
7/31/2019 P-Economics in Hospital
69/80
69
Cost-effectiveness (CEA)
Costs = $
Outcomes = natural units
Cures, deaths avoided Intermediate outcomesNot desirable (need
linkage)
e.g., Blood level (cholesterol)
-
7/31/2019 P-Economics in Hospital
70/80
70
Cost utility (CUA)
Cost = $
Outcome = patient utility
QALY = quality adjusted life year Assess quality of life utility
Quantify and adjust by utility
Compare incrementally between drugs
-
7/31/2019 P-Economics in Hospital
71/80
71
Interpreting outcomes
Incremental cost-outcome ratio:
Cost1 Cost2__________________
Benefit1 Benefit 2
-
7/31/2019 P-Economics in Hospital
72/80
72
Incremental analysis
Compare costs and outcomes
Ideal = lower cost + better outcomes
Usual = more cost more outcome Problem = assessment
-
7/31/2019 P-Economics in Hospital
73/80
73
Incremental CEA
If cost lower + benefit greater = dominant
If incremental cost cost/outcome, then
CEA If lower cost + lower outcome, could be
OK
-
7/31/2019 P-Economics in Hospital
74/80
74
Interpretation of PEA results
Outcome+
Outcome-
Cost+
IncrementalCE
Dominated
Cost- Dominant ???
-
7/31/2019 P-Economics in Hospital
75/80
75
Interpretation: Suggestion
-
7/31/2019 P-Economics in Hospital
76/80
76
CEA example
New drug cost = $500, cure = 0.7 (70%)
Old drug cost $400, cure = 0.5 (50%)
ICER = ($500 - $400)/(0.7 0.5) = $500 peradditional cure
Old drug cost $400/0.5 = $800/cure; therefore,the new drug is
cost-effective and should be
adopted, if it can be afforded
-
7/31/2019 P-Economics in Hospital
77/80
77
CEA example 2
New drug cost = $500, cure = 0.7
Old drug cost $100, cure = 0.5
ICER = ($500 - $100)/(0.7 0.5) = $1,000 per additional cure
Requires judgment (no real rules)
-
7/31/2019 P-Economics in Hospital
78/80
78
CEA interpretation
Dominant = adopt (if affordable)
If the incremental cost cost/outcome of
standard, then the new drug may beconsidered to be cost
effective
Otherwise, judgment required
S
-
7/31/2019 P-Economics in Hospital
79/80
79
Summary
PEA requires at least 1 drug and 1comparison treatment
PEA involves simultaneous analysis ofcosts AND outcomes
Decision makers prefer dominanttreatments they provide
savings;incremental cost-effectiveness involves
increased costs
-
7/31/2019 P-Economics in Hospital
80/80
Thank You