Embed Size (px)
Citation preview
OZLEM SORAN, MD, MPH, FACC, FESC
Director of EECP Treatment Lab
Associate Professor of Medicine
Associate Professor of Epidemiology/Research
Heart and Vascular Institute
University of Pittsburgh
Effects of EECP therapy on CAD and heart failure treatment and integration of
endothelial function measurement to
follow clinical outcomesObjectives–Brief history of counterpulsation–Hemodynamic effects of EECP–Summary of recent clinical trials –Mode of Action–Need for endothelial function measurement

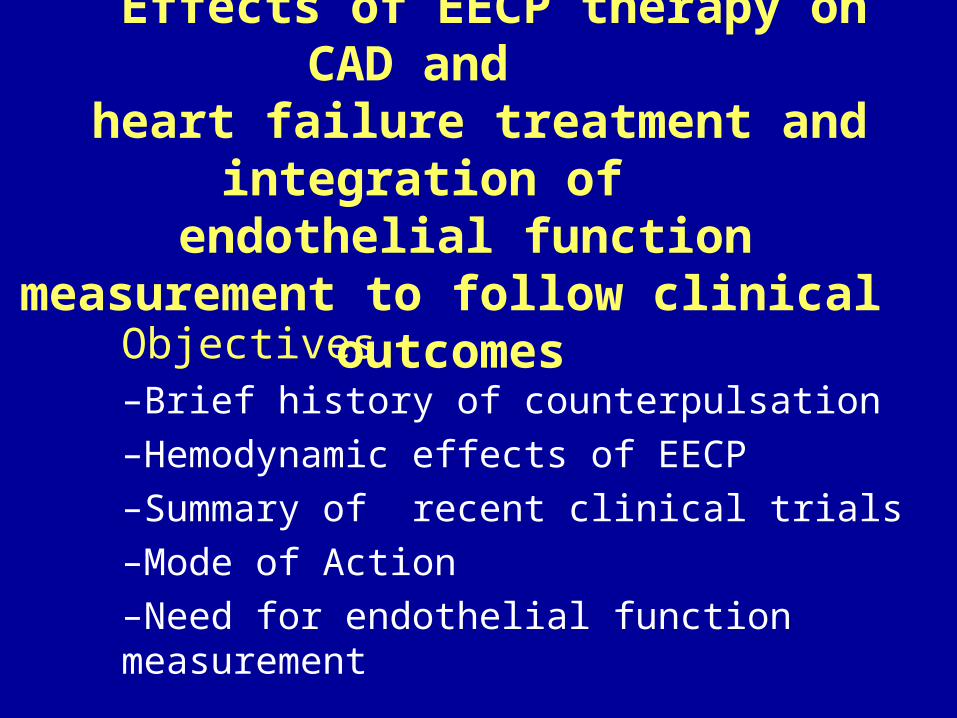
Neurohormonal ReleaseIncreases: NO, ANPDeceases: BNP, ET-1, ACE, ANG II
Hemodynamic Effects of EECPIncrease Cardiac Output
Systolic unloading
Increase Venous return
DiastolicRetrograde Flow
Diastolic Augmentation
Increase Shear Stress on endothelium
Increase coronary Perfusion
Pressure Gradients
occlusion
Enhance Collateral capillary sprouting
Improve Diastolic Filling
Remodeling
Release of Growth Factors
Angiogenesis andArteriogenesis
Improve Endothelial Function
Postulated Mechanisms of Action
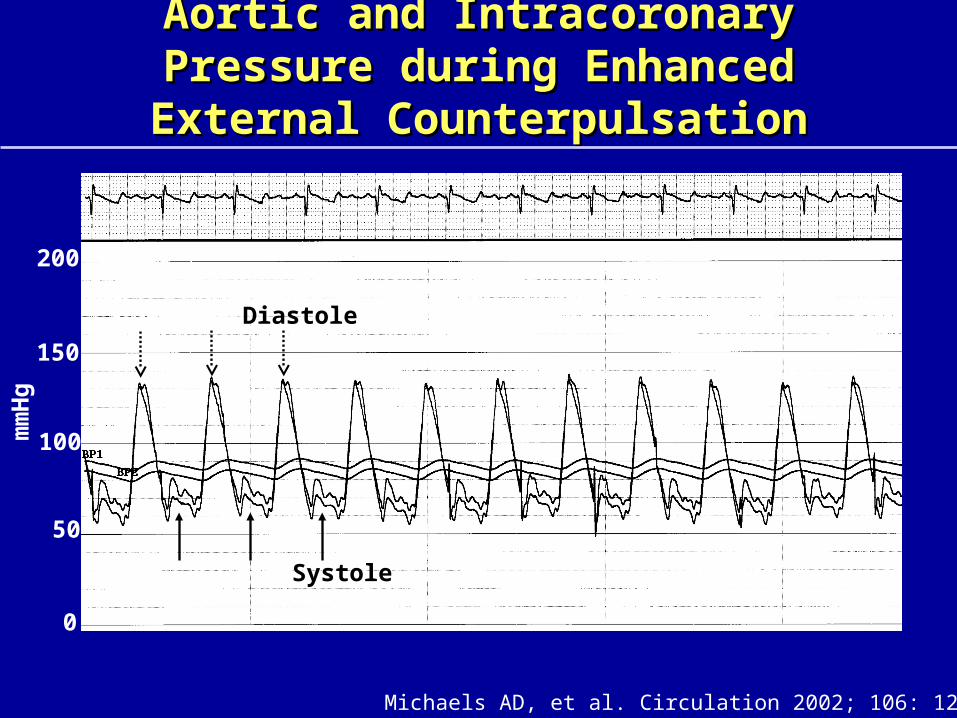
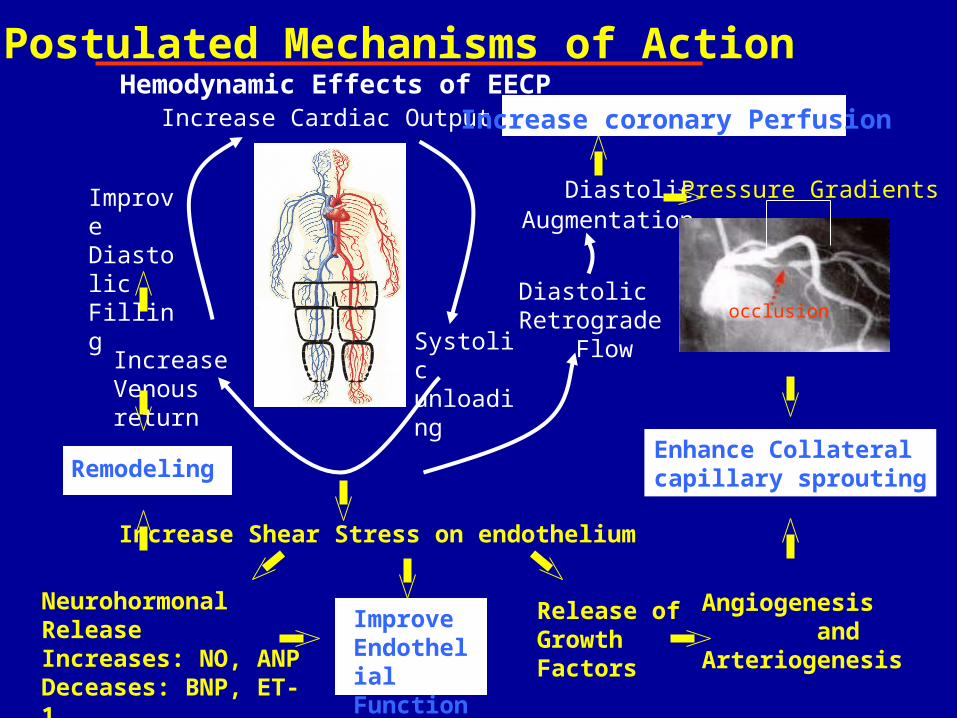
Aortic and Intracoronary Pressure during Aortic and Intracoronary Pressure during Enhanced External CounterpulsationEnhanced External Counterpulsation
Michaels AD, et al. Circulation 2002; 106: 1237-42.
mm
Hg
0
50
100
150
200
Systole
Diastole

EECP Therapy Treatment Regimen
Outpatient therapy
Standard treatment is 1 hour per day
5 days per week for 7 weeks
A total of 35 treatment sessions
Benefits associated with EECP – including Placebo Controlled Clinical Trials and
International Registry Results
Significant•angina reduction, - in some cases no angina•improvement in quality of life,•prolongation of the time to exercise induced ST segment depression, •improvement in exercise capacity and duration,•improvement in myocardial perfusion,•reduction in nitrate use
stable angina pectoris unstable angina pectoris acute myocardial
infarctioncardiogenic shock
FDA approved indications -1995
EECP in Heart Failure: Results of a Pilot Study
Ozlem Z. Soran†, Teresa De Marco‡, Lawrence E. Crawford†, Virginia Schneider†, Paul-André de Lame+, Bruce Fleishman*, William Grossman‡,
Arthur M. Feldman†
† University of Pittsburgh Medical Center, Pittsburgh, PA; ‡ University of California San Francisco, San Francisco, CA; * Cardiovascular Research
Institute, Columbus, OH; + Anabase International Corp., Stockton, NJ
Soran OZ, et al. J Cardiac Failure 1999;5(3):53(195)
Enhamced External Counterpulsation in Patients with
Heart Failure : A Multicenter Feasibility Study
Ozlem Z. Soran†, Bruce Fleishman *, Teresa De Marco‡, William Grossman‡, Virginia Schneider†, Karen Manzo *, Paul-André de Lame+,
Arthur M. Feldman†
† University of Pittsburgh Medical Center, Pittsburgh, PA; ‡ University of California San Francisco, San Francisco, CA; * Cardiovascular Research
Institute, Columbus, OH; + Anabase International Corp., Stockton, NJ
Soran O, et al Congest Heart Fail 2002; 8(4):204-208Soran O, et al Congest Heart Fail 2002; 8(4):204-208
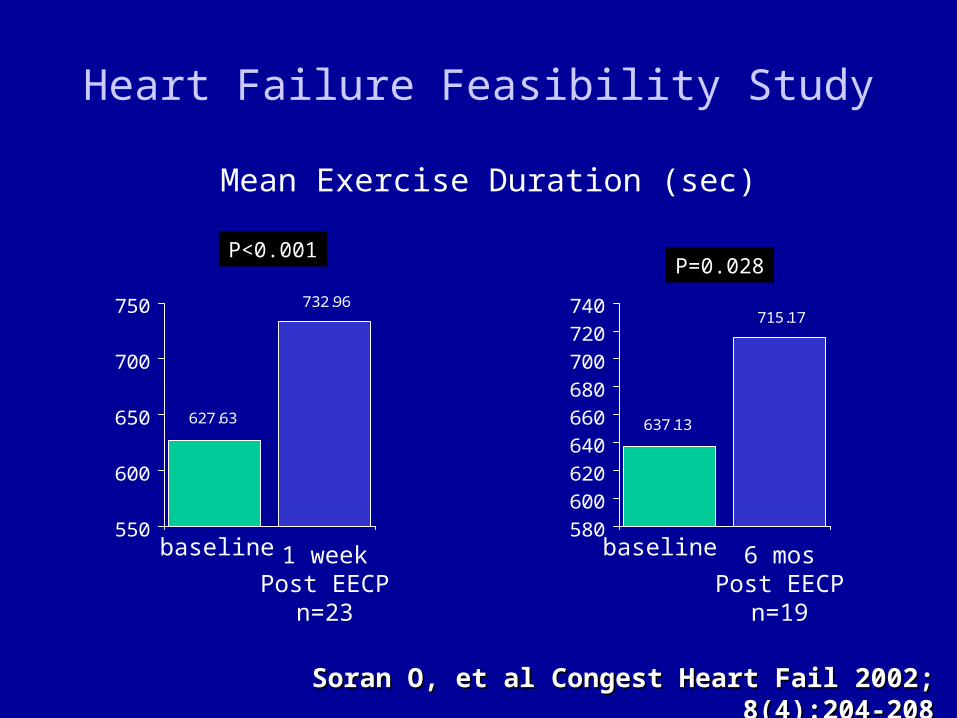
637.13
715.17
580
600
620
640
660
680
700
720
740
Heart Failure Feasibility Study Mean Exercise Duration (sec)
627.63
732.96
550
600
650
700
750
P<0.001P=0.028
Soran O, et al Congest Heart Fail 2002; 8(4):204-208Soran O, et al Congest Heart Fail 2002; 8(4):204-208
baseline 1 weekPost EECP
n=23
baseline 6 mosPost EECP
n=19
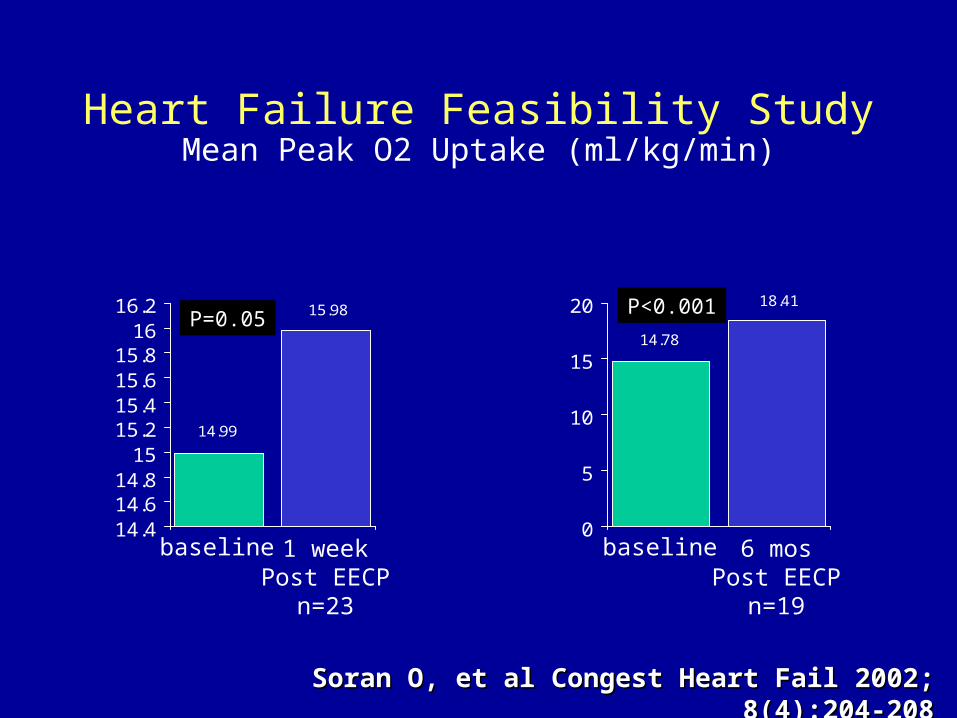
Heart Failure Feasibility StudyMean Peak O2 Uptake (ml/kg/min)
14.99
15.98
14.414.614.8
1515.215.415.615.8
1616.2
P=0.0514.78
18.41
0
5
10
15
20 P<0.001
Soran O, et al Congest Heart Fail 2002; 8(4):204-208Soran O, et al Congest Heart Fail 2002; 8(4):204-208
baseline 1 weekPost EECP
n=23
baseline 6 mosPost EECP
n=19
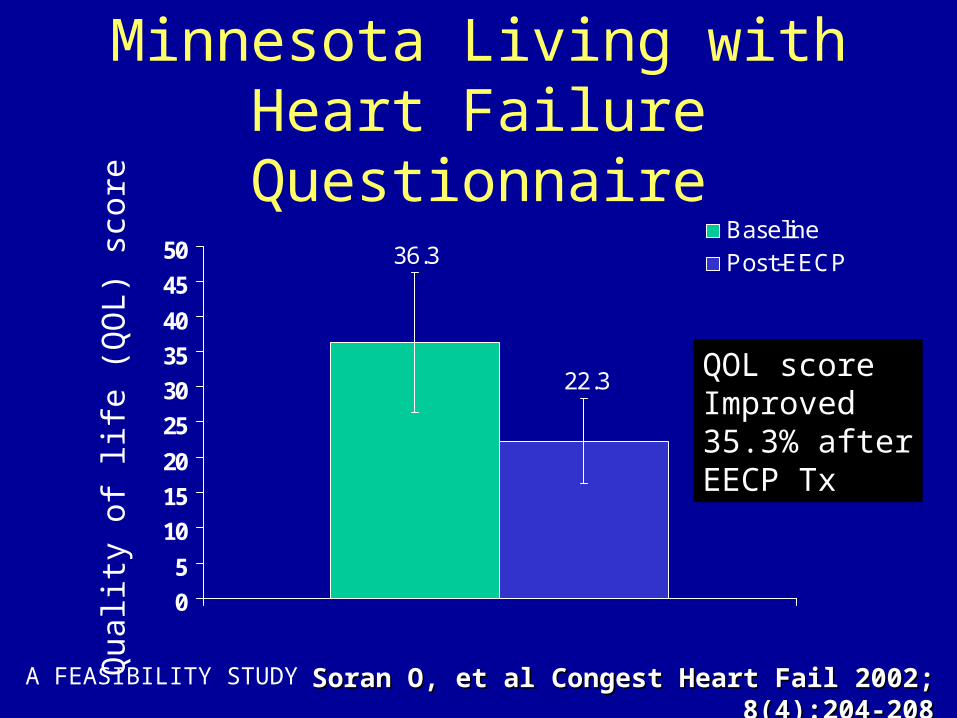
Minnesota Living with Heart Failure Questionnaire
A FEASIBILITY STUDY Soran O, et al Congest Heart Fail 2002; 8(4):204-208Soran O, et al Congest Heart Fail 2002; 8(4):204-208
36.3
22.3
0
5
10
15
20
25
30
35
40
45
50BaselinePost-EECP
Qua
lity
of li
fe (
QO
L) s
core
QOL scoreImproved35.3% afterEECP Tx
ASSESSMENT OF LV FUNCTION
• Preload-Adjusted Maximal Power (PAMP) was calculated as a relatively load-independent measure of LV function: Power = Pressure x Flow
• Echocardiographic Automated Border Detection measures of mid-LV cross-sectional area as a surrogate for LV volume (H-P Sonos 2500). Simultaneous noninvasive arterial pressure was estimated by finger photoplethysmography.
• Flow was calculated as dA/dt from the LV area signal. Maximum area was aligned with minimum arterial pressure to correct for the delay in the pressure signal.
• PAMP: (Pressure x Flow) / (End-diastolic Area) 3/2.
Mandarino et al. J Am Coll Cardiol 1998;31:861-868
Baseline 3 Months 6 Months0
10
20
30
40
50
60
p < 0.05 vs. baseline
Eje
cti
on
Fra
cti
on
(%
)
* *
*
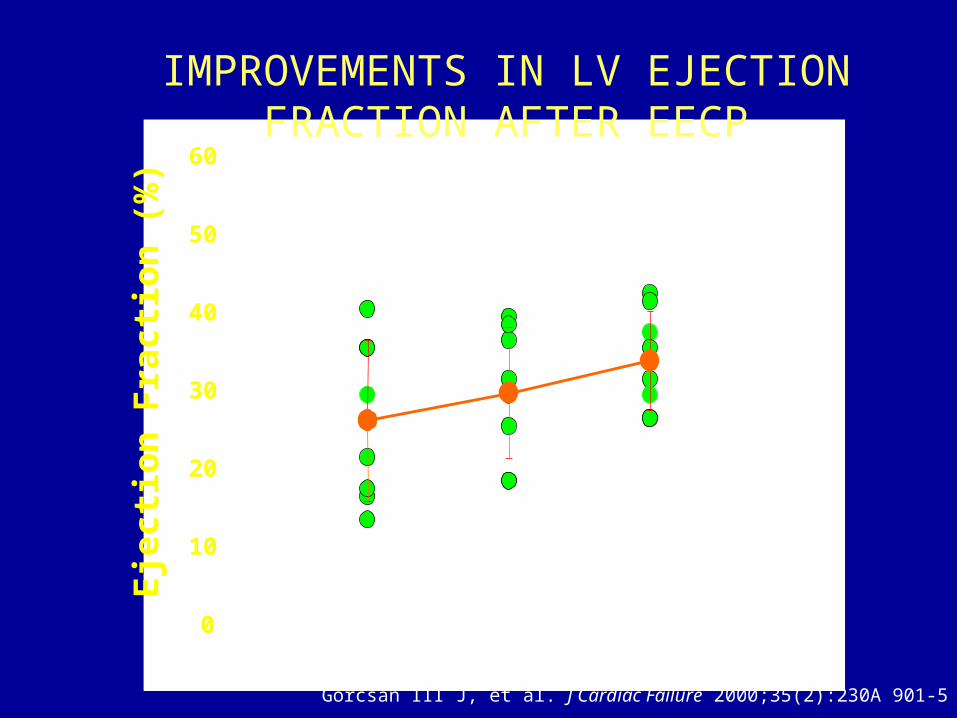
IMPROVEMENTS IN LV EJECTION FRACTION AFTER EECP
Gorcsan III J, et al. J Cardiac Failure 2000;35(2):230A 901-5
Baseline 3 Months 6 Months0
5
10
* p < 0.05 vs. baseline
*
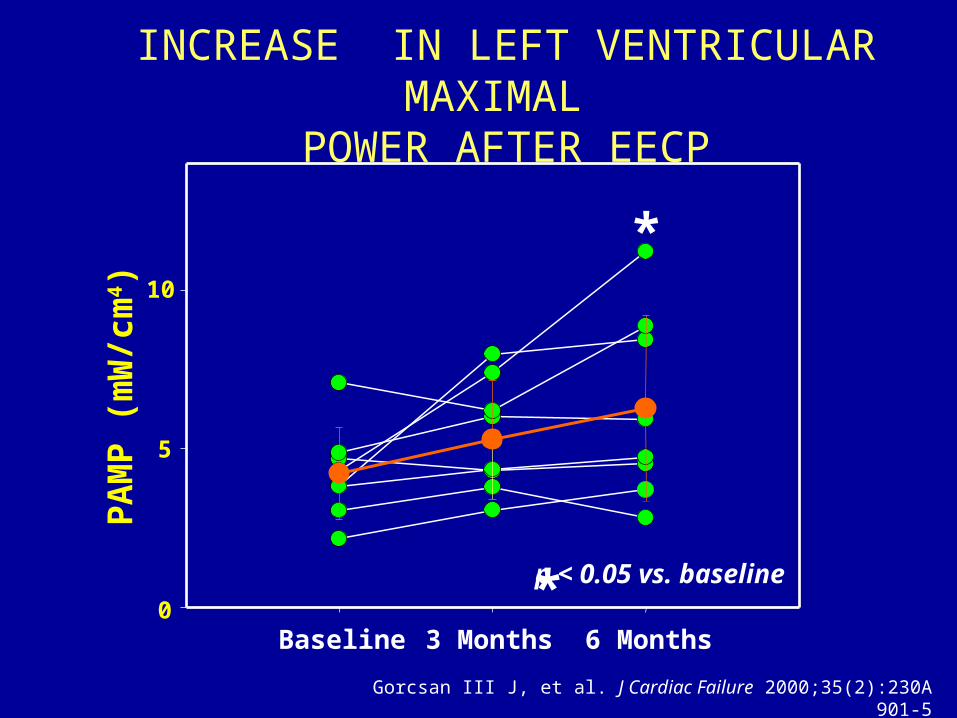
INCREASE IN LEFT VENTRICULAR MAXIMAL
POWER AFTER EECPP
AM
P (
mW
/cm
4 )
Gorcsan III J, et al. J Cardiac Failure 2000;35(2):230A 901-5
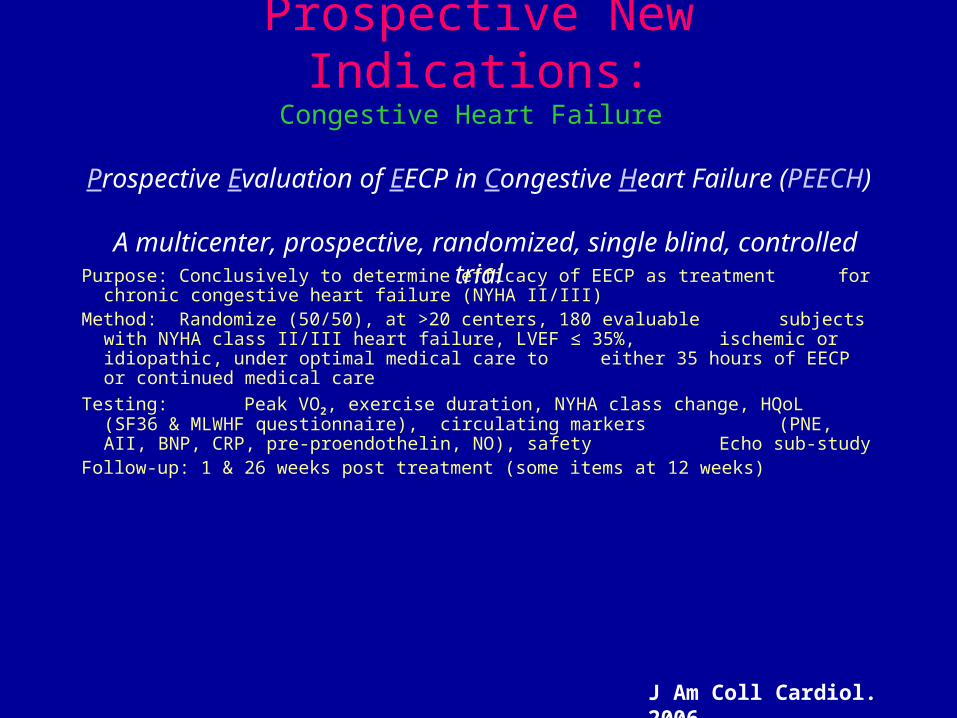
Prospective New Indications:Congestive Heart Failure
Prospective Evaluation of EECP in Congestive Heart Failure (PEECH)
A multicenter, prospective, randomized, single blind, controlled trial
Purpose: Conclusively to determine efficacy of EECP as treatment for chronic congestive heart failure (NYHA II/III)
Method: Randomize (50/50), at >20 centers, 180 evaluable subjects with NYHA class II/III heart failure, LVEF ≤ 35%, ischemic or idiopathic, under optimal medical care to either 35 hours of EECP or continued medical care
Testing: Peak VO2, exercise duration, NYHA class change, HQoL (SF36 & MLWHF questionnaire), circulating markers (PNE, AII, BNP, CRP, pre-proendothelin, NO), safety Echo sub-study
Follow-up: 1 & 26 weeks post treatment (some items at 12 weeks)
J Am Coll Cardiol. 2006
PEECH: Conclusions
• Primary end point for statistical improvement to exercise capacity was met
• The addition of a standard regimen of EECP to optimal pharmacologic therapy improves exercise time for at least 6 months
• Consistent with the improvement in exercise time, there was an improvement in QoL and NYHA classification
• Changes to pVO2 although positive at 1 week and 3 months did not demonstrate statistically significant differences at 6 months
• EECP therapy is well tolerated in this group of patients
• These results suggest that EECP provides adjunctive therapy in patients with NYHA Class II-III heart failure receiving optimal pharmacologic therapy
J Am Coll Cardiol. 2006
Clinical Outcomes, Event Free Survival Rates and Incidence of Repeat Enhanced
External Counterpulsation in CAD Patients with Left Ventricular Dysfunction
- A 2 Year Cohort Study
Soran O et al. Am J Cardiol. 2006 Jan 1; 97(1): 17-20
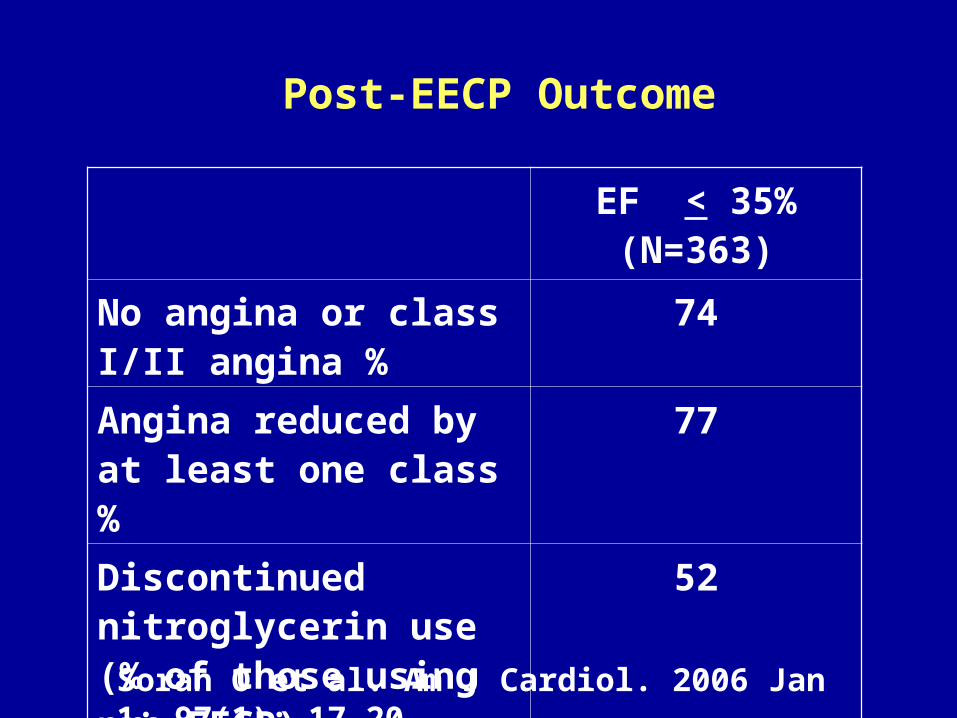
Post-EECP Outcome
EF < 35%(N=363)
No angina or class I/II angina %
74
Angina reduced by at least one class %
77
Discontinued nitroglycerin use (% of those using pre-EECP)
52
Soran O et al. Am J Cardiol. 2006 Jan 1; 97(1): 17-20
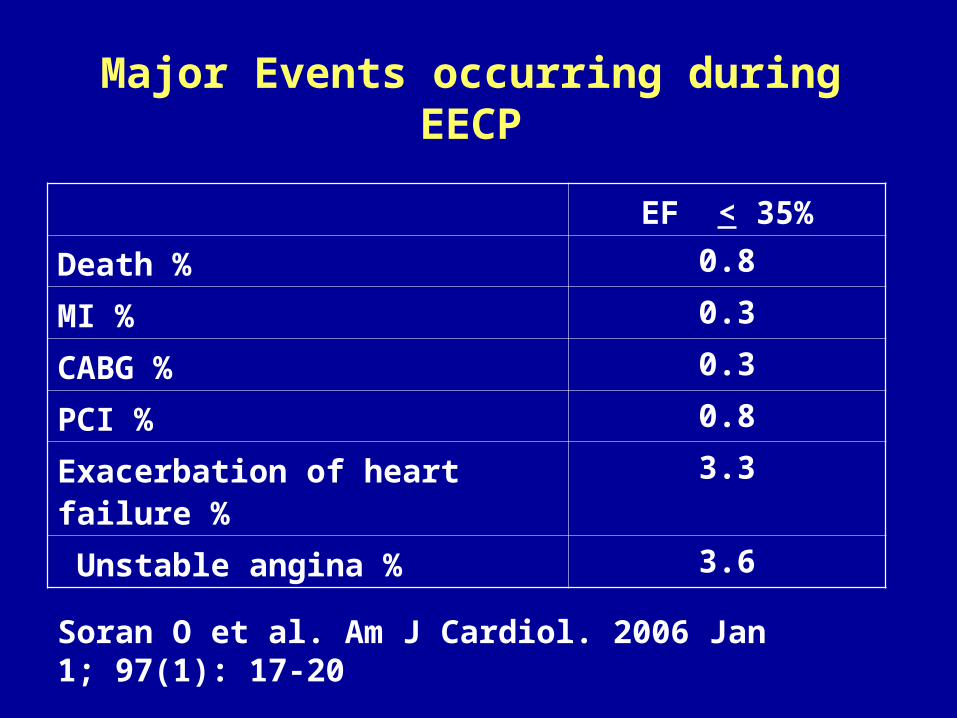
Major Events occurring during EECP
EF < 35%
Death % 0.8
MI % 0.3
CABG % 0.3
PCI % 0.8
Exacerbation of heart failure % 3.3
Unstable angina % 3.6
Soran O et al. Am J Cardiol. 2006 Jan 1; 97(1): 17-20
81% had no congestive Heart Failure exacerbation during the 2
year follow-up period.
Soran O et al. Am J Cardiol. 2006 Jan 1; 97(1): 17-20
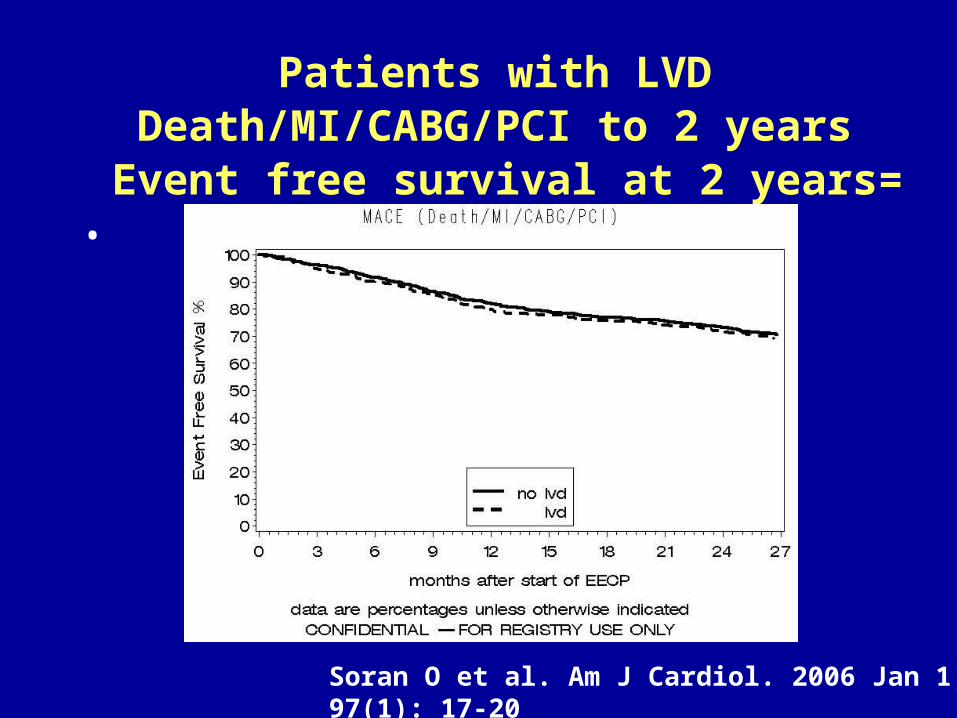
Patients with LVDDeath/MI/CABG/PCI to 2 years
Event free survival at 2 years= 70 %
Soran O et al. Am J Cardiol. 2006 Jan 1; 97(1): 17-20
•
THE IMPACT OF ENHANCED EXTERNAL
COUNTERPULSATION TREATMENT ON
EMERGENCY ROOM VISITS AND
HOSPITALIZATIONS
Soran et al, Congest Heart Fail. 2007;13(1):36-40
Methods
• Clinical outcomes, number of ER visits and hospitalizations within the six months prior to EECP therapy were compared with those at 6 month follow up. Statistical analysis was performed using paired t-tests and chi-square tests.
Soran et al, Congest Heart Fail. 2007;13(1):36-40
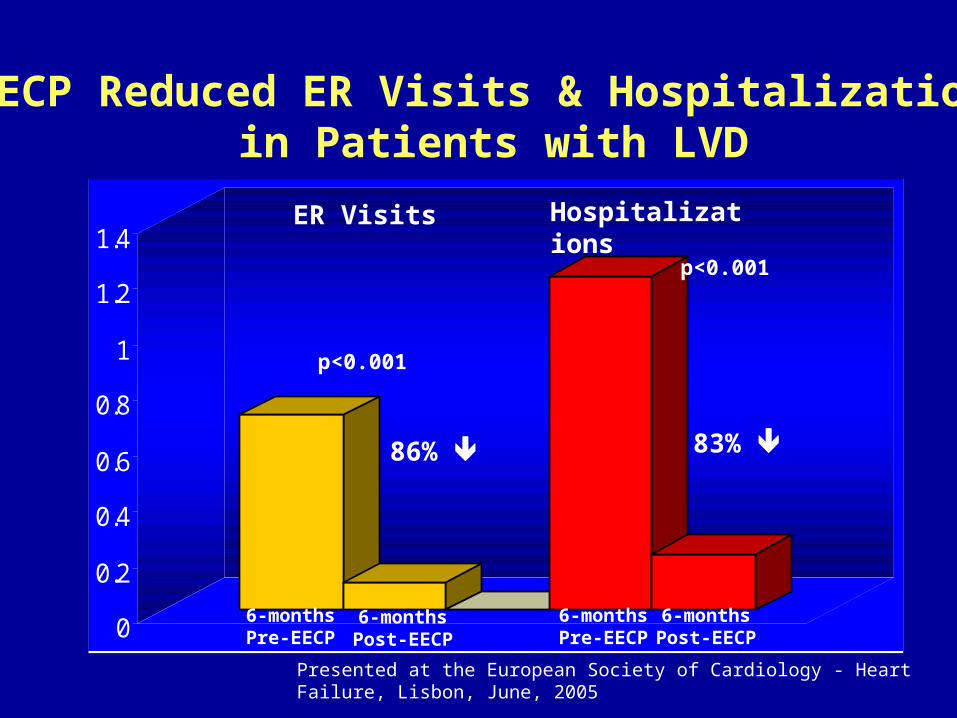
EECP Reduced ER Visits & Hospitalizationsin Patients with LVD
0
0.2
0.4
0.6
0.8
1
1.2
1.4
86% 83%
6-monthsPre-EECP
6-monthsPost-EECP
p<0.001
p<0.001
ER Visits Hospitalizations
6-monthsPre-EECP
6-monthsPost-EECP
Presented at the European Society of Cardiology - Heart Failure, Lisbon, June, 2005
Published in Congestive Heart Failure - Soran et al - Jan 2007,
RESULTS
Hospitalization for angina pectoris decreased with 82%, 12 month after treatment compared to 6 month before. CCS class
improved with persistent benefit 6 and 12 month after treatment. No patient deteriorated in CCS class. One
patient experienced pain along the ischias nerve; otherwise no adverse events were recorded.
Petterson T, et all. Presented at the Swedish Cardiology Meeting
FDA Indications for EECP Therapy
• March 1995 – stable and unstable angina, acute myocardial infarction
and cardiogenic shock
• June 2002– Clinical indications are expanded to include
congestive heart failure
Benefits associated with EECP – including Placebo Controlled Clinical Trials and
International Registry Results• angina reduction, • improvement in quality of life,• prolongation of the time to exercise induced ST
segment depression, • resolution of myocardial perfusion defects,• reduction of nitrate use• reduction in hospitalization• improvement in LV Functions• Low MACE rates at long term follow up
Research: More than 15.000 patients have
been treated with EECP for research purpose
Routine Practice: Currently > 300 000 patients have been treated with EECP
Mechanism of Action
Mechanism of Action-I
• Enhanced diastolic flow increases shear stress
• Increased shear stress activates the release of growth factors
• Augmentation of growth factor release activates angiogenesis
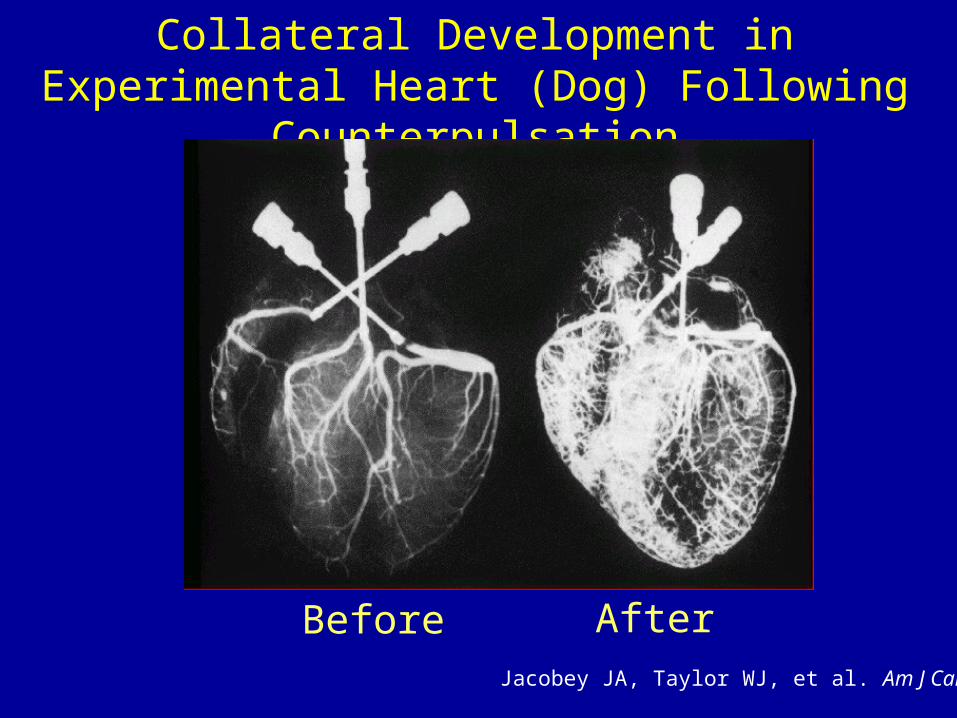
Collateral Development in Experimental Heart (Dog) Following Counterpulsation
Before AfterJacobey JA, Taylor WJ, et al. Am J Cardiol
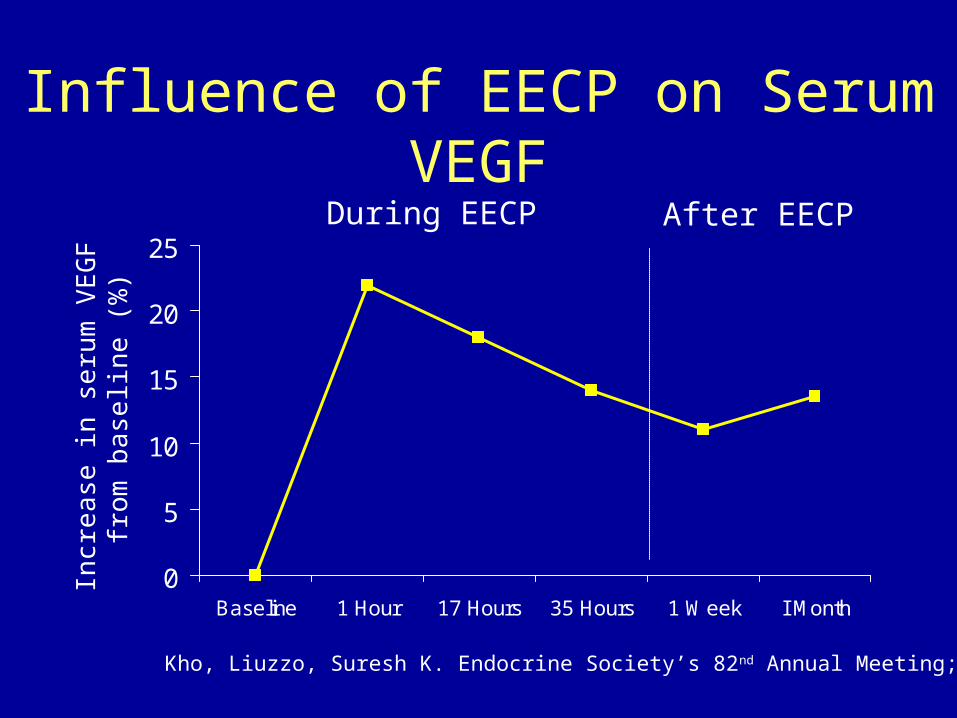
Influence of EECP on Serum VEGF
0
5
10
15
20
25
Baseline 1 Hour 17 Hours 35 Hours 1 Week I Month
Incr
ea
se in
se
rum
VE
GF
fr
om
ba
selin
e (
%)
Kho, Liuzzo, Suresh K. Endocrine Society’s 82nd Annual Meeting; Canada
During EECP After EECP
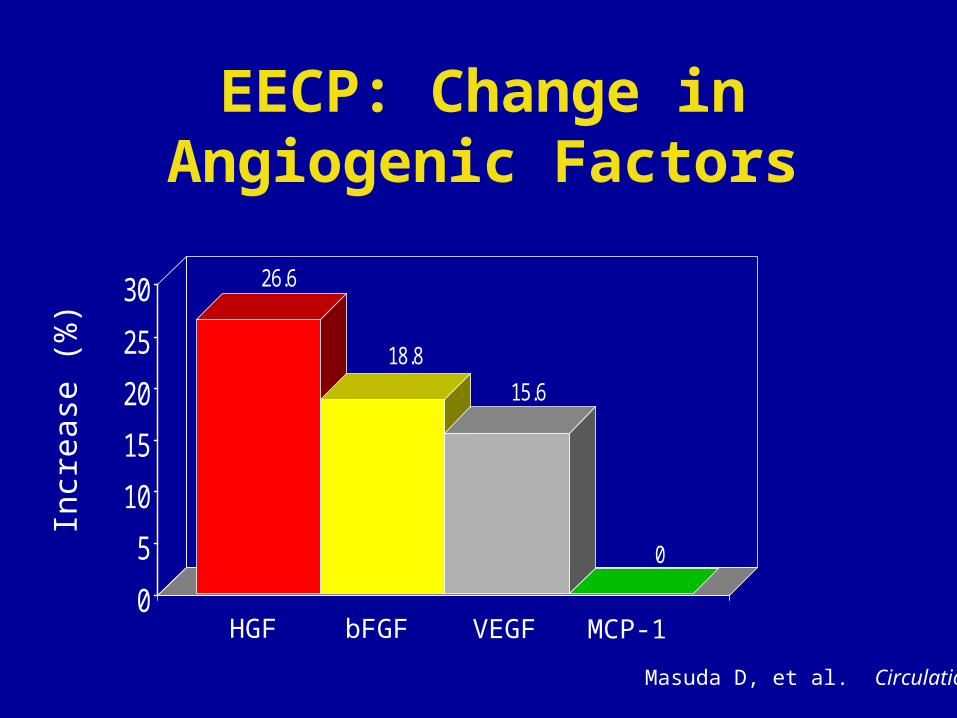
EECP: Change in Angiogenic Factors
26.6
18.8
15.6
0
0
5
10
15
20
25
30
Incr
ease
(%
)
HGF bFGF VEGF MCP-1
Masuda D, et al. Circulation
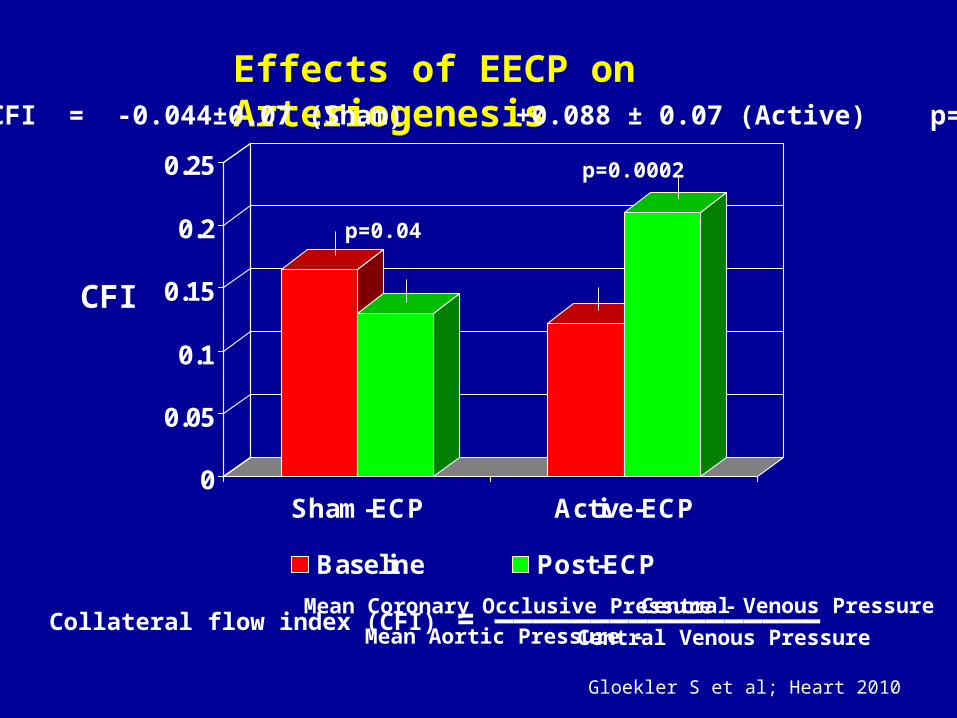
Effects of EECP on Arteriogenesis
Collateral flow index (CFI) = ————————————————— Mean Coronary Occlusive Pressure -Central Venous Pressure
Mean Aortic Pressure - Central Venous Pressure
0
0.05
0.1
0.15
0.2
0.25
Sham-ECP Active-ECP
Baseline Post-ECP
CFI
p=0.04
p=0.0002
CFI = -0.044±0.07 (Sham) +0.088 ± 0.07 (Active) p=0.00005
Gloekler S et al; Heart 2010
Mechanism of Action-2
• EECP enhances vascular reactivity
• Like athletic training, the vascular effects of EECP might be mediated through changes in the neurohormonal milieu
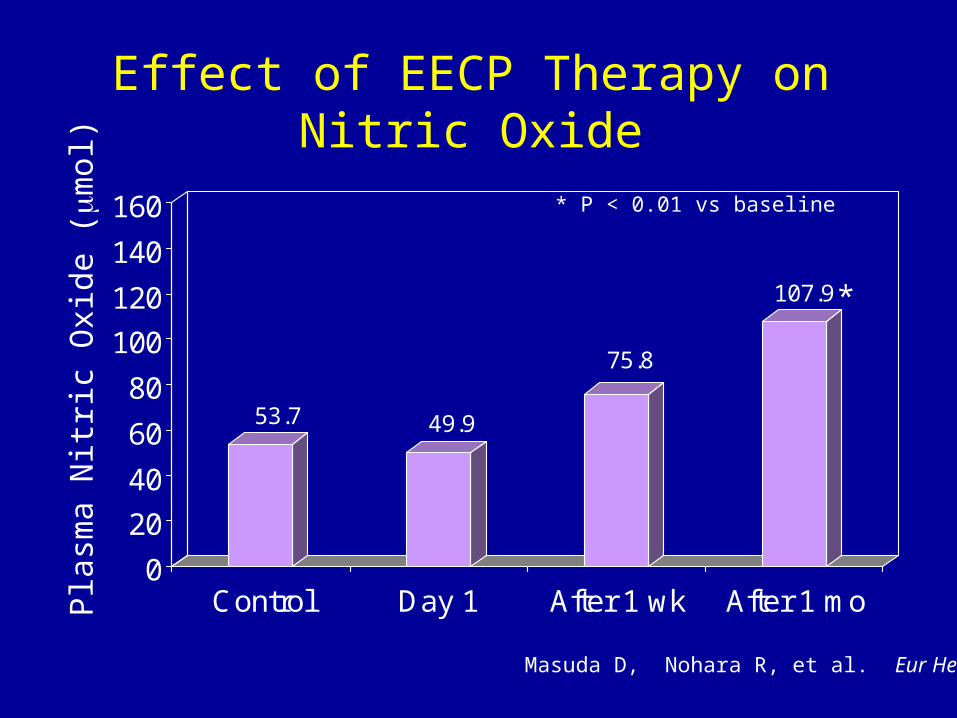
Pla
sma
Nit
ric
Oxi
de (m
ol)
Masuda D, Nohara R, et al. Eur Heart J
Effect of EECP Therapy on Nitric Oxide
53.7 49.9
75.8
107.9
0
20
40
60
80
100
120
140
160
Control Day 1 After 1 wk After 1 mo
* P < 0.01 vs baseline
*
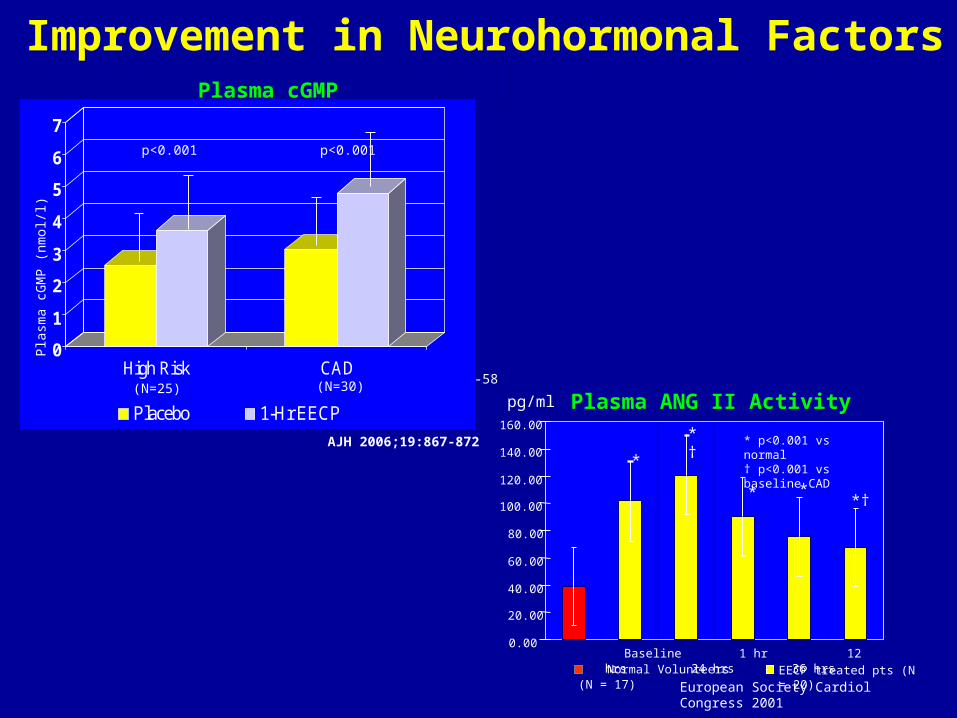
Improvement in Neurohormonal Factors
Eur Heart J 2001;22(16):1451-58
Eur Heart J 2001;22(16):1451-58
0
1
2
3
4
5
6
7
High Risk CAD
Placebo 1-Hr EECP
Plas
ma
cGM
P (n
mol
/l)
p<0.001 p<0.001
(N=25) (N=30)
Plasma cGMP
AJH 2006;19:867-872
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
160.00
Normal Volunteers (N = 17) EECP treated pts (N = 20)
pg/ml
*
*†
*†
European Society Cardiol Congress 2001
Baseline 1 hr 12 hrs 24 hrs 36 hrs
* p<0.001 vs normal† p<0.001 vs baseline CAD
Plasma ANG II Activity
* *
Mechanism of Action-3
EECP improves endothelial function

Easy /on the spot:Assessment of Functional CapacitySymptom and QoL6 min testEndothelial Function Measurement (non-invasive, accurate,reliable, easy to use, inexpensive , done in 10-15 min)
Somewhat time consuming and/or costlyEchoMPI/ Stress Test
InvasiveCath??
How to Follow Clinical Outcomes of Patients Undergoing EECP in the Routine Clinical Practice