Embed Size (px)
Citation preview
OxygenDr Mark B Smith
Oxygen
• History– Discovered by
• Carl Wilhelm Scheele, 1772 (German-Swedish)• Joseph Priestley, 1774 (British)
– Named by• Lavoisier, 1777 (French)
– Lost his head selling cheap tobacco
Oxygen• Atomic Number: 8• Atomic Weight: 15.9994• Melting Point: 54.36 K (-218.79°C or -361.82°F)• Boiling Point: 90.20 K (-182.95°C or -297.31°F)• Density: 0.001429 grams per cubic centimeter• Phase at Room Temperature: Gas• Element Classification: Non-metal• Period Number: 2 • Group Number: 16• Group Name: Chalcogen
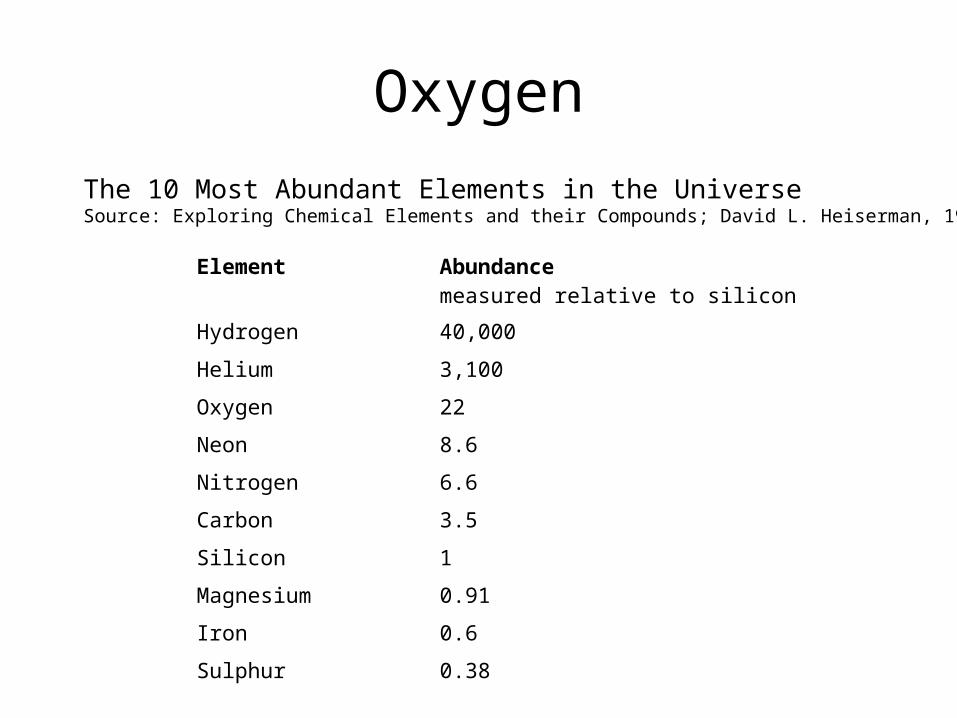
OxygenThe 10 Most Abundant Elements in the UniverseSource: Exploring Chemical Elements and their Compounds; David L. Heiserman, 1992
Element Abundancemeasured relative to silicon
Hydrogen 40,000
Helium 3,100
Oxygen 22
Neon 8.6
Nitrogen 6.6
Carbon 3.5
Silicon 1
Magnesium 0.91
Iron 0.6
Sulphur 0.38
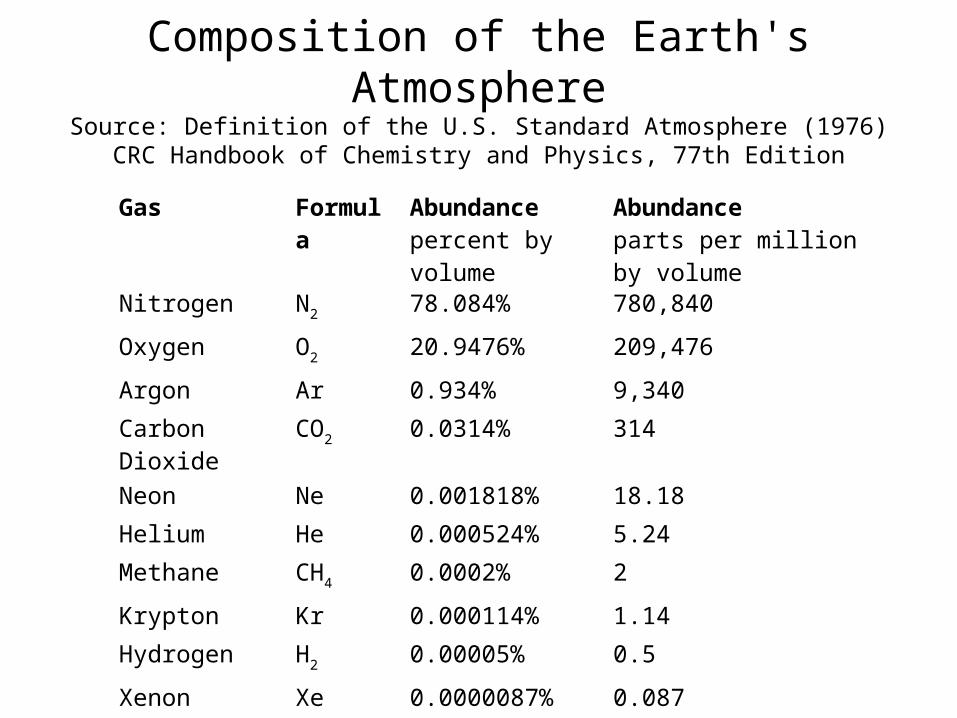
Composition of the Earth's AtmosphereSource: Definition of the U.S. Standard Atmosphere (1976)
CRC Handbook of Chemistry and Physics, 77th Edition
Gas Formula Abundancepercent by volume
Abundanceparts per million by volume
Nitrogen N2 78.084% 780,840
Oxygen O2 20.9476% 209,476
Argon Ar 0.934% 9,340
Carbon Dioxide
CO2 0.0314% 314
Neon Ne 0.001818% 18.18
Helium He 0.000524% 5.24
Methane CH4 0.0002% 2
Krypton Kr 0.000114% 1.14
Hydrogen H2 0.00005% 0.5
Xenon Xe 0.0000087% 0.087
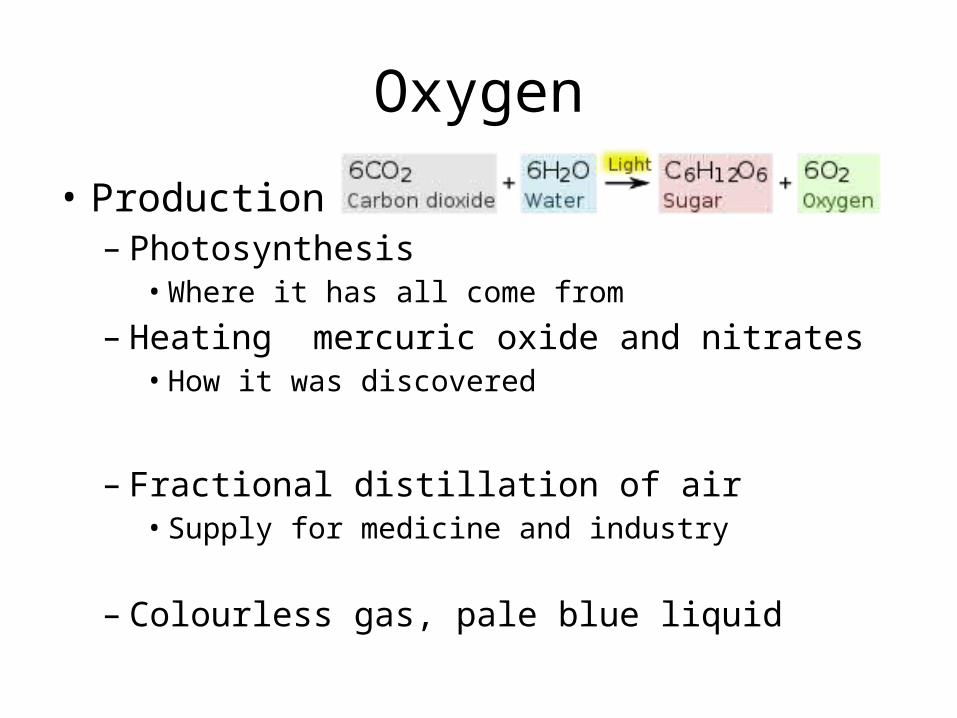
Oxygen
• Production– Photosynthesis
• Where it has all come from
– Heating mercuric oxide and nitrates• How it was discovered
– Fractional distillation of air• Supply for medicine and industry
– Colourless gas, pale blue liquid
Oxygen
• Daltons Law (John)
– total pressure exerted by a gaseous mixture is equal to the sum of the partial pressures of each individual component in a gas mixture
• Significance– At fixed total pressure “adding” another gas reduces
partial pressure of other gases• Water vapour• Carbon dioxide
Oxygen: Under pressure
760mmHg = 101.325 kPa = 1 atmosphere1 Pa = 1 Newton per square meter1 torr = 1 mmHg = 1/760 atmosphere
Specific fluid density = 13.591 g/cm3
(Density of mercury at 0oC)Specific gravity = 9.80665 m/s2
(Standard gravity)
Oxygen• The purpose of the cardio-respiratory system is to extract
oxygen from the atmosphere and deliver it to the mitochondria of cells.
• Oxygen– exerts a partial pressure– determined by the prevailing environmental pressure– sea level atmospheric pressure is 760mmHg– oxygen makes up 21% (20.094% to be exact) air– oxygen exerts a partial pressure of 760 x 0.21 = 159mmHg
• The oxygen cascade– as one moves down through the body to the cell, oxygen is diluted
down, extracted or otherwise lost, so that at cellular level the PO2 may only be 3 or 4 mmHg.
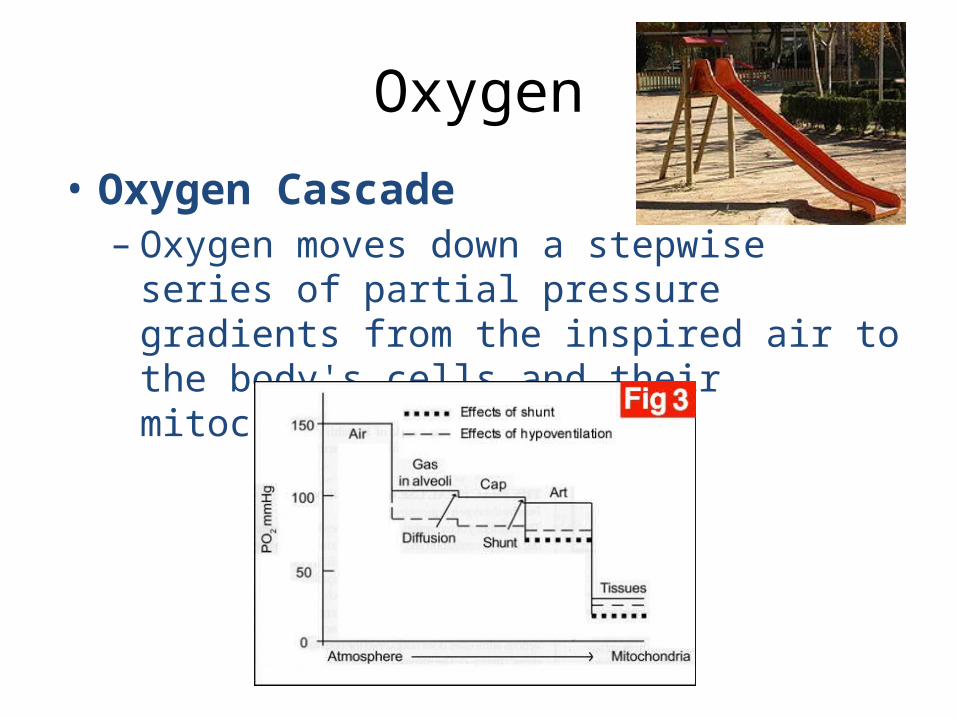
Oxygen
• Oxygen Cascade– Oxygen moves down a stepwise series of partial
pressure gradients from the inspired air to the body's cells and their mitochondria.
Oxygen
• Water vapour– humidifies inspired air– dilutes the amount of oxygen– reduces the partial pressure by the saturated
vapour pressure (47mmHg)– effect on the PIO2 (the partial pressure of inspired
oxygen)– recalculated as: (760 - 47) x 0.2094 = 149mmHg.
Oxygen• Carbon dioxide
– alveolar carbon dioxide, the PACO2– is usually the same as the PaCO2
• measured by a blood gas analyzer– alveolar partial pressure of oxygen PAO2 calculated from the following
equation: PAO2 = PIO2 – PaCO2/R– R is the respiratory quotient
• represents the amount of carbon dioxide excreted for the amount of oxygen utilized• depends on the carbon content of food (carbohydrates high, fat low)
– let us assume that the respiratory quotient is 0.8– PAO2 will then be 149 – (40/0.8) = 100mmHg
– More Carbon dioxide means less Oxygen
Oxygen
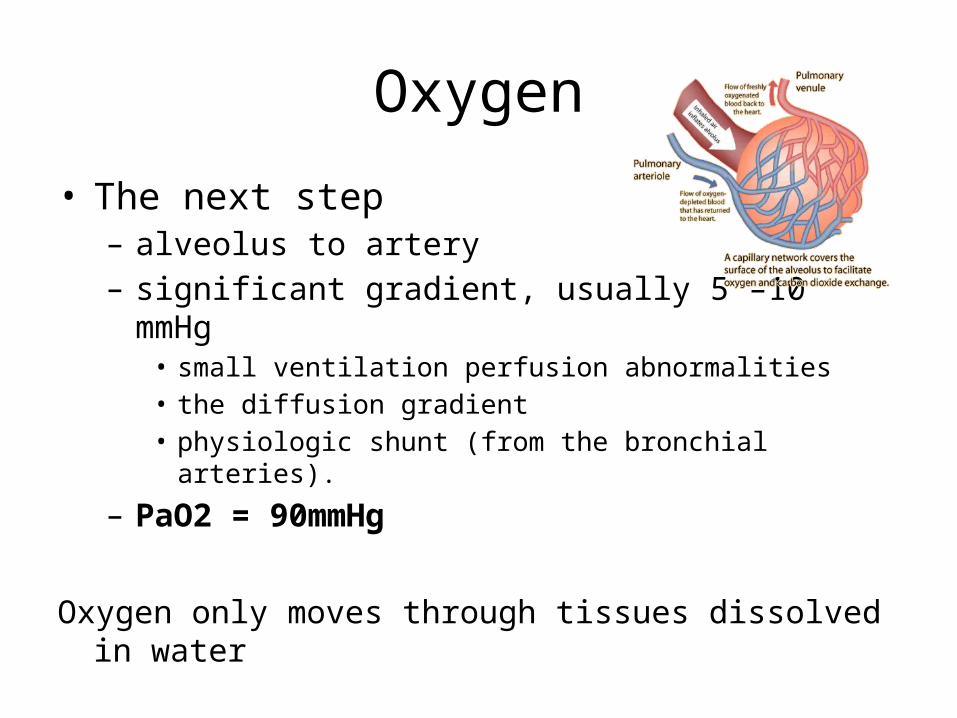
• The next step– alveolus to artery– significant gradient, usually 5 –10 mmHg
• small ventilation perfusion abnormalities• the diffusion gradient• physiologic shunt (from the bronchial arteries).
– PaO2 = 90mmHg
Oxygen only moves through tissues dissolved in water
Oxygen
• Oxygen transport– arterial tree
• minimal extraction
– progressively extracted through the capillary network
• interstitial space
– return via venous system• partial pressure of oxygen in mixed venous blood,
PVO2, is approximately 47mmHg.
Oxygen
• Oxygen cascade interference – At 19,000 feet (just above base camp at Mount
Everest, the barometric pressure is half that at sea level, and thus, even though the FiO2 is 21%, the PIO2 is only 70mmHg, half that at sea level
– Increased barometric pressure such as in hyperbaric chambers, the PIO2 will actually be higher
• More oxygen…but dissolved not on haemoglobin
Oxygen
• Four factors influence transmission of oxygen from the alveoli to the capillaries– Ventilation perfusion mismatch
• Pneumonia, pulmonary embolism
– Right to left shunt• ASD, VSD
– Diffusion defects• Pulmonary fibrosis, pulmonary oedema, COPD
– Cardiac output• Pump failure, Exercise
Oxygen
• The amount of oxygen in the bloodstream is determined by;– serum haemoglobin level– percentage of this haemoglobin saturated with
oxygen– cardiac output– the amount of oxygen dissolved (see below).
Oxygen
• How much oxygen is in the blood?
• The amount of oxygen in the blood is calculated using the formula: [1.34 x Hb x (SaO2/100)] + 0.003 x PO2 = 20.8ml per 100ml blood
EMERGENCY MOBILE MEDICAL UNIT Training Weekend
HYPOVENTILATION
• A RISE IN PaCO2 CAUSES A FALL IN PaO2
THIS IS THE BASIS OF THE ALVEOLAR GAS EQUATION
PaO2 = FiO2(Pb-PaH2O)-PaCO2/0.8
EMERGENCY MOBILE MEDICAL UNIT Training Weekend
• TREATMENT– OXYGEN TO OBTAIN SaO2>90%
• IF THE PATIENT BECOMES TIRED THE PaCO2 MAY RISE
• IF RISING PaCO2 OR DROWSY PROVIDE ASSISTED VENTILATION

EMERGENCY MOBILE MEDICAL UNIT Training Weekend
HIGH CONCENTRATIONS OF INSPIRED OXYGEN DO NOT DEPRESS VENTILATION IN PATIENTS WITH ACUTE RESPIRATORY FAILURE
EMERGENCY MOBILE MEDICAL UNIT Training Weekend
• OXYGEN THERAPY ON GENERAL WARDS MUST BE PRESCRIBED
• TYPE OF OXYGEN DELIVERY SYSTEM• FLOW RATE OF OXYGEN (OR %)• DURATION OF THERAPY• MONITORING TO BE UNDERTAKEN
Oxygen is a drug
EMERGENCY MOBILE MEDICAL UNIT Training Weekend
OXYGEN DELIVERY SYSTEMS
• VARIABLE PERFORMANCE
• FIXED PERFORMANCE
VARIABLE PERFORMANCE SYSTEMS
NASAL CANNULA
• 24-40% DEPENDING ON FLOW RATE• INSPIRED CONCENTRATION VARY BETWEEN
BREATHS• DEPENDS UPON RATE AND DEPTH• MAXIMUM FLOW RATE APPROX 4 l/min
VARIABLE PERFORMANCE SYSTEMS
SIMPLE FACE MASK
• MASK INCREASES RESERVOIR • MINIMAL FLOW RATE APPROX 4 l/min• NO INCREASED INSPIRED OXYGEN ABOVE 15 l/min• INSPIRED OXYGEN OF UP TO 60%
VARIABLE PERFORMANCE SYSTEMS
PARTIAL REBREATHING MASKS
• FACEMASK AND RESERVOIR BAG
• INSPIRED OXYGEN >60%
• FLOW RATES OF APPROX 15 l/min REQUIRED
FIXED PERFORMANCE SYSTEMS
VENTURI MASK• ENTRAINS AIR
• HIGH FLOW MAINTAINS HIGH INSPIRED OXYGEN CONCENTRAION THROUGHOUT RESPIRATORY CYCLE
• COLOUR CODED VENTURI HEADS
FIXED PERFORMANCE SYSTEMS
ANAESTHETIC MACHINE– Open system
• Magill Circuit• Bains system• Maplesons C
– Closed system• Circle
Inspired Oxygen v Tissue Oxygen
• Inspired oxygen greater than alveolar oxygen– Oxygen cascade
– Water vapour– Carbon dioxide
• Normal and pathological physiological effects– Oxygen cascade, continued
– Intrapulmonary ventilation/perfusion mis-match– Cardiac shunts– Arterial oxygen loss– Oxygen diffusion in water solution
EMERGENCY MOBILE MEDICAL UNIT Training Weekend
SUMMARY
ALL CRITICALLY ILL PATIENTS REQUIRE OXYGEN
Oxygen cascade occurs regardless
Maximise inspired Oxygen
MONITOR

















![The PhotoReading Whole Mind System - Paul Scheele [CuPpY]](https://img.pdfslide.us/doc/110x75/55cf92b7550346f57b9909d5/the-photoreading-whole-mind-system-paul-scheele-cuppy-567d94be8b5fa.jpg)