Embed Size (px)
Citation preview

Oxygen Consumption in Infants and Childrenduring Cardiac Catheterization under Different
Sedation RegimensBy DAVID E. FIXLER, M. D., TED CARRELL, B. S., RICHARD BROWNE, Ph.D.,
KATHRYN WILLIS, M.D., AND WILLIAM W. MILLER, M.D.
SUMMARYWe measured oxygen consumption in 426 infants and children during cardiac catheterization using an
open circuit, flow-through technique. Since this method does not require the cooperation of the patient,determinations were readily made in 170 infants. The purpose of this study was to determine those factorswhich significantly influence oxygen consumption and to determine the potential errors incurred in usingpredictive equations for estimating oxygen consumption. The type of sedation or anesthesia given was foundto be one of the most important variables influencing oxygen consumption; therefore patients were classifiedinto five anesthetic groups. Stepwise regression analysis revealed that each group had a distinctive set ofhemodynamic or physical factors which significantly affected oxygen consumption; hence each group re-
quired a different predictive equation. Body size in terms of surface area or weight was the only significantvariable common to all five patient groups. Using the predictive equations the estimated values differedfrom measured values by more than 20 percent in approximately one-fifth of the cases. These data indicatethat frequently oxygen consumption cannot be accurately estimated from predictive equations. Therefore ifblood flow is to be accurately determined by the Fick method in infants and children, oxygen consumptionshould be measured during the catheterization procedure.
Additional Indexing Words:Open circuit, flow-through technique Paramagnetic oxygen analyzer Ketamine anesthesia
CARDIAC CATHETERIZATION is an invasiveprocedure which provides information frequent-
ly used in determining operability of children withheart defects. Because of its invasive nature and itsimportant role in decision making, every effort shouldbe made to minimize the variability of the laboratoryfindings. Since the presence of intracardiac shuntsreduces the accuracy of measuring pulmonary bloodflow by the indicator dilution technique, blood flow iscommonly determined by the Fick method. Thismethod requires simultaneous measurement ofarterio-venous oxygen content differences and oxy-gen consumption during a steady state. Ideally then,oxygen consumption should be measured con-tinuously during the catheterization procedure todetermine if a steady state is present at the time ofblood sampling and to provide a direct measurementfor the Fick determination of cardiac output.
From the Department of Pediatrics, The University of TexasCenter for Health Sciences, Southwestern Medical School, Dallas,Texas.
Address for reprints: David E. Fixler, M.D., Department ofPediatrics, The University of Texas Health Science Center atDallas, 5323 Harry Hines Blvd., Dallas, Texas 75235.
Received February 22, 1974; revision accepted for publicationMay 28, 1974.
788
Many cardiac catheterization laboratories do notmeasure oxygen consumption in infants and smallchildren but assume a value based on predictive tablespublished in the literature.1 2 Unfortunately, somediscrepancies appear in the tables of different studiesand none have a large number of determinations inchildren under 2 years of age. The purpose of thepresent study was threefold: 1) to describe andcritically evaluate a relatively simple flow-throughtechnique for continuous measurement of oxygen con-sumption; 2) to determine those factors whichsignificantly affect oxygen consumption during thecardiac catheterization procedure; and 3) to presentnew predictive equations for estimating oxygen con-sumption and the potential error incurred in their use.
MethodsMeasurement of Oxygen Consumption
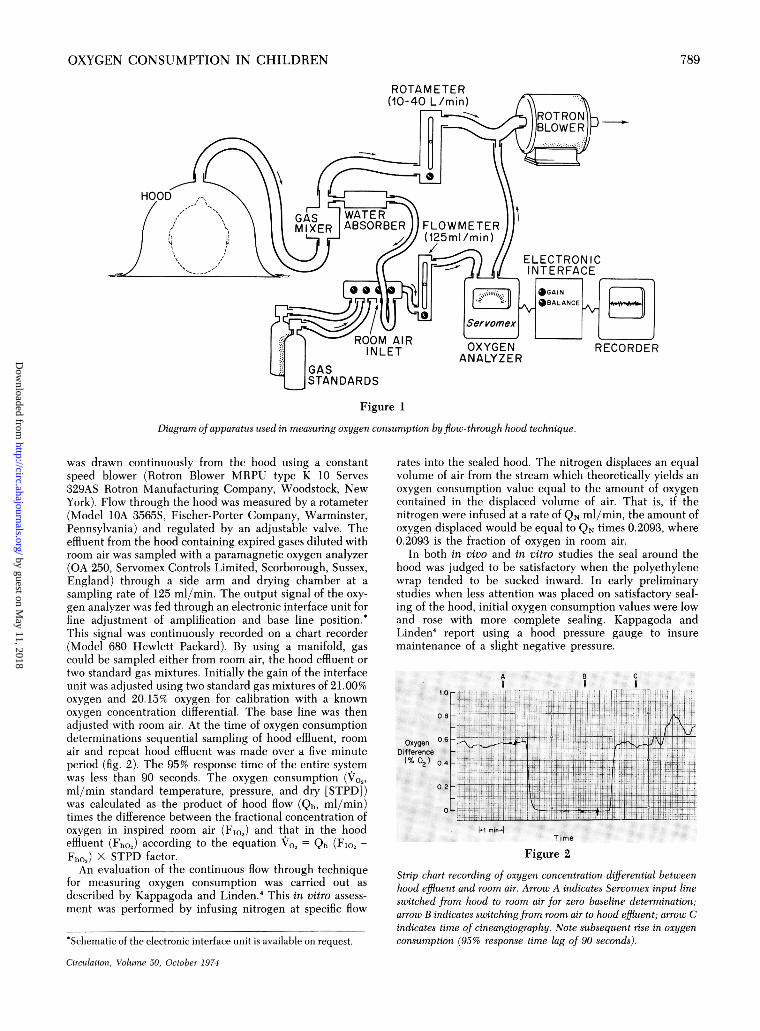
Oxygen consumption was measured by modification of aflow-through technique.3 In infants and small children thepatient's head, shoulders and arms were enclosed within atransparent, hemispherical hood; in older children only thehead was inserted (fig. 1). The opening around the neck orshoulders was sealed with a clear polyethylene wrap and theedges of the hood were sealed to the catheterization tablewith paper tape. Room air was sucked into the hood at a flowrate of approximately 10 times the patient's expectedminute volume to prevent carbon dioxide accumulation. Gas
Circulation, Volume 50, October 1974
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
OXYGEN CONSUMPTION IN CHRILDREN
Figure 1
Diagram of apparatus used in measuring oxygen consumption by flow -through hood technique.
was drawn continuously from the hood using a constantspeed blower (IRotron Blower MRPU type K 10 Serves329AS Rotron Manufacturing Company, Woodstock, NewYork). Flow through the hood was measured by a rotameter(Model TOA 3565S, Fischer-Porter Company, Warminster,Pennsylvania) and regulated by an adjustable valve. Theeffluent from the hood containing expired gases diluted withroom air was sampled with a paramagnetic oxygen analyzer(OA 250, Servomex Controls Limited, Scorborough, Sussex,England) through a side arm and drying chamber at a
sampling rate of 125 ml/min. The output signal of the oxy-
gen analyzer was fed through an electronic interface unit forfine adjustment of amplification and base line position.*This signal was continuously recorded on a chart recorder(Model 680 Hewlett Packard). By using a manifold, gascould be sampled either from room air, the hood effluent or
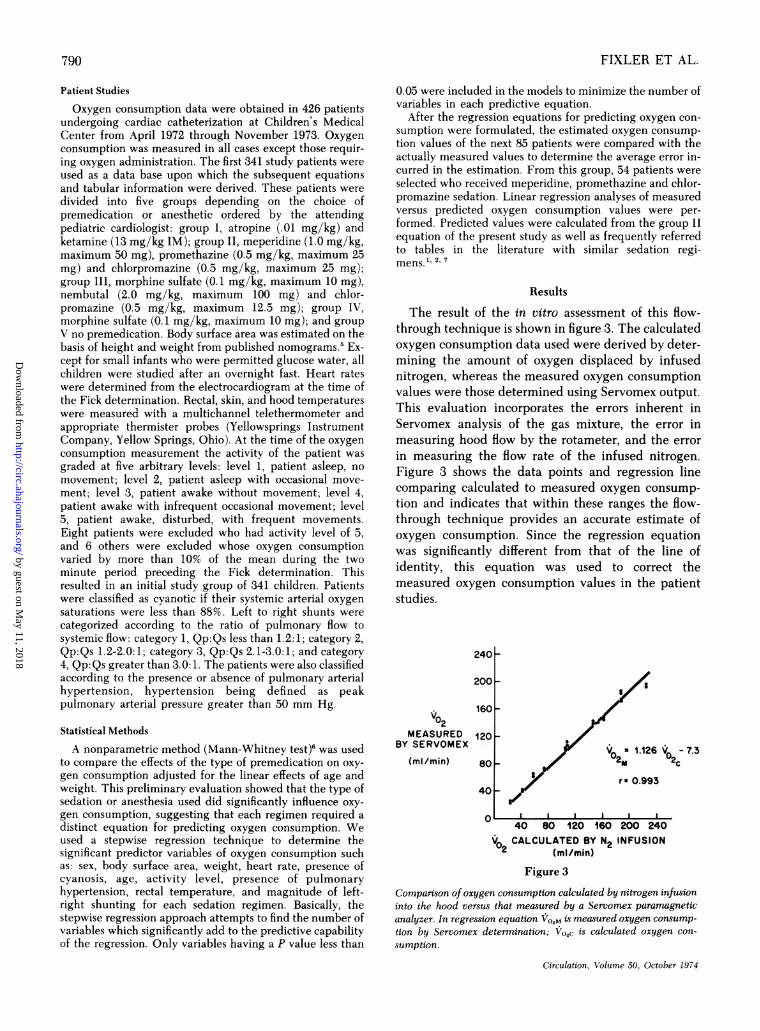
two standard gas mixtures. Initially the gain of the interfaceunit was adjusted using two standard gas mixtures of 21.00%oxygen and 20.15% oxygen for calibration with a knownoxygen concentration differential. The base line was thenadjusted vith room air. At the time of oxygen consumptiondeterminations sequential sampling of hood effluent, room
air and repeat hood effluent was made over a five minuteperiod (fig. 2). The 95% response time of the entire systemwas less than 90 seconds. The oxygen consumption (Vo2,
ml/min standard temperature, pressure, and dry [STPD])was calculated as the product of hood flow (Qh, ml/min)times the difference between the fractional concentration ofoxygen in inspired room air (FIO2) and that in the hoodeffluent (Fho,) according to the equation Vo2 Qh (FIO, -
Fh02) X STPD factor.An evaluation of the continuous flow through technique
for measuring oxygen consumption was carried out as
described by Kappagoda and Linden.4 This in vitro assess-
ment was performed by infusing nitrogen at specific flow
rates into the sealed hood. The nitrogen displaces an equalvolume of air from the stream which theoretically yields an
oxygen consumption value equal to the amount of oxygen
contained in the displaced volume of air. That is, if thenitrogen were infused at a rate of QN ml/min, the amount ofoxygen displaced would be equal to QN times 0.2093, where0.2093 is the fraction of oxygen in room air.
In both in vivo and in vitro studies the seal around thehood was judged to be satisfactory when the polyethylenewrap tended to be sucked inward. In early preliminarystudies when less attention was placed on satisfactory seal-ing of the hood, initial oxygen consumption values were lowand rose with more complete sealing. Kappagoda andLinden4 report using a hood pressure gauge to insuremaintenance of a slight negative pressure.
A
Or
OxygenDifference% 09)
0.6
0.4
0.2
OL
.H .......
i.l- ' E. . 1
=-
:
e1
.w..
A :0
B C
V .J.t.* 1
H _mm LL >=.=-r ]
Time
Figure 2
Strip chart recording of oxygen concentration differential betweenhood effluent and room air. Arrow A indicates Servomex input lineswitched from hood to room air for zero baseline determination;arrow B indicates switching from room air to hood effluent; arrow Cindicates time of cineangiography. Note subsequent rise in oxygen
consumption (95% response time lag of 90 seconds).*Schematic of the electronic interface unit is available on request.
Circulation, Volume 50, October 1974
c -! A - .. ll.. ... .. ..:-7-!-,-.7
789
o.8FS
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
FIXLER ET AL.
Patient Studies
Oxygen consumption data were obtained in 426 patientsundergoing cardiac catheterization at Children's MedicalCenter from April 1972 through November 1973. Oxygenconsumption was measured in all cases except those requir-ing oxygen administration. The first 341 study patients wereused as a data base upon which the subsequent equationsand tabular information were derived. These patients weredivided into five groups depending on the choice ofpremedication or anesthetic ordered by the attendingpediatric cardiologist: group I, atropine (.01 mg/kg) andketamine (13 mg/kg IM); group II, meperidine (1.0 mg/kg,maximum 50 mg), promethazine (0.5 mg/kg, maximum 25mg) and chlorpromazine (0.5 mg/kg, maximum 25 mg);group III, morphine sulfate (0.1 mg/kg, maximum 10 mg),nembutal (2.0 mg/kg, maximum 100 mg) and chlor-promazine (0.5 mg/kg, maximum 12.5 mg); group IV,morphine sulfate (0.1 mg/kg, maximum 10 mg); and groupV no premedication. Body surface area was estimated on thebasis of height and weight from published nomograms.5 Ex-cept for small infants who were permitted glucose water, allchildren were studied after an overnight fast. Heart rateswere determined from the electrocardiogram at the time ofthe Fick determination. Rectal, skin, and hood temperatureswere measured with a multichannel telethermometer andappropriate thermister probes (Yellowsprings InstrumentCompany, Yellow Springs, Ohio). At the time of the oxygenconsumption measurement the activity of the patient wasgraded at five arbitrary levels: level 1, patient asleep, nomovement; level 2, patient asleep with occasional move-ment; level 3, patient awake without movement; level 4,patient awake with infrequent occasional movement; level5, patient awake, disturbed, with frequent movements.Eight patients were excluded who had activity level of 5,and 6 others were excluded whose oxygen consumptionvaried by more than 10% of the mean during the twominute period preceding the Fick determination. Thisresulted in an initial study group of 341 children. Patientswere classified as cyanotic if their systemic arterial oxygensaturations were less than 88%. Left to right shunts werecategorized according to the ratio of pulmonary flow tosystemic flow: category 1, Qp:Qs less than 1.2:1; category 2,Qp:Qs 1.2-2.0:1; category 3, Qp:Qs 2.1-3.0:1; and category4, Qp:Qs greater than 3.0:1. The patients were also classifiedaccording to the presence or absence of pulmonary arterialhypertension, hypertension being defined as peakpulmonary arterial pressure greater than 50 mm Hg.
Statistical Methods
A nonparametric method (Mann-Whitney test)6 was usedto compare the effects of the type of premedication on oxy-gen consumption adjusted for the linear effects of age andweight. This preliminary evaluation showed that the type ofsedation or anesthesia used did significantly influence oxy-gen consumption, suggesting that each regimen required adistinct equation for predicting oxygen consumption. Weused a stepwise regression technique to determine thesignificant predictor variables of oxygen consumption suchas: sex, body surface area, weight, heart rate, presence ofcyanosis, age, activity level, presence of pulmonaryhypertension, rectal temperature, and magnitude of left-right shunting for each sedation regimen. Basically, thestepwise regression approach attempts to find the number ofvariables which significantly add to the predictive capabilityof the regression. Only variables having a P value less than
0.05 were included in the models to minimize the number ofvariables in each predictive equation.
After the regression equations for predicting oxygen con-sumption were formulated, the estimated oxygen consump-tion values of the next 85 patients were compared with theactually measured values to determine the average error in-curred in the estimation. From this group, 54 patients wereselected who received meperidine, promethazine and chlor-promazine sedation. Linear regression analyses of measuredversus predicted oxygen consumption values were per-formed. Predicted values were calculated from the group IIequation of the present study as well as frequently referredto tables in the literature with similar sedation regi-mens.1 2, 7
Results
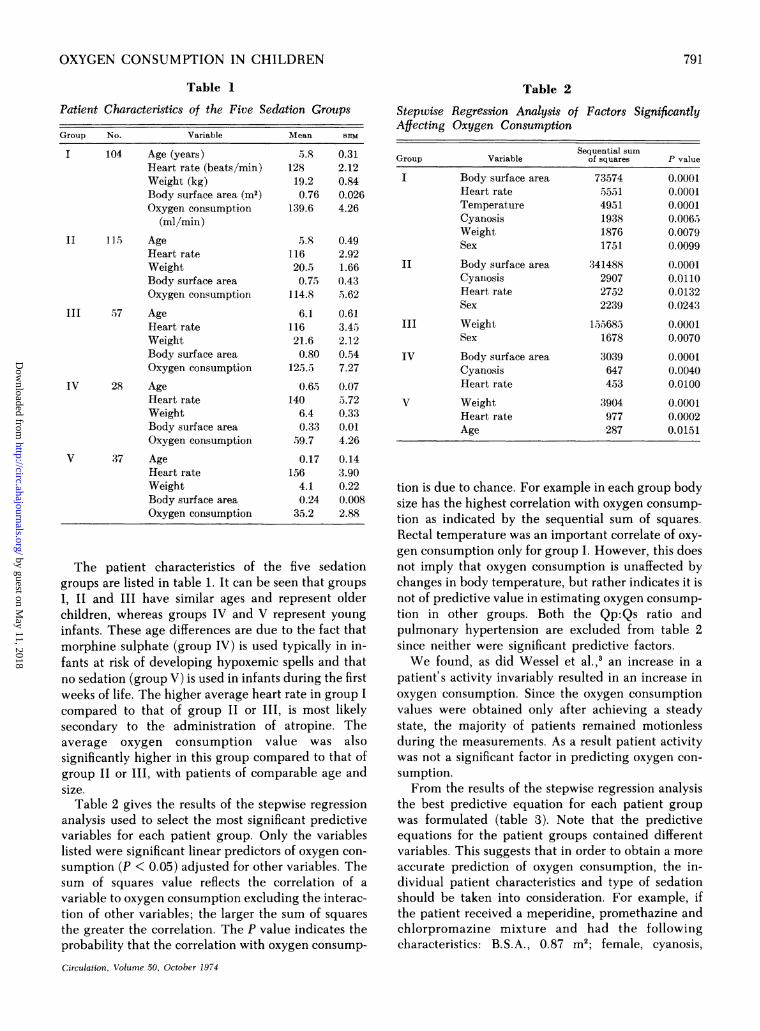
The result of the in vitro assessment of this flow-through technique is shown in figure 3. The calculatedoxygen consumption data used were derived by deter-mining the amount of oxygen displaced by infusednitrogen, whereas the measured oxygen consumptionvalues were those determined using Servomex output.This evaluation incorporates the errors inherent inServomex analysis of the gas mixture, the error inmeasuring hood flow by the rotameter, and the errorin measuring the flow rate of the infused nitrogen.Figure 3 shows the data points and regression linecomparing calculated to measured oxygen consump-tion and indicates that within these ranges the flow-through technique provides an accurate estimate ofoxygen consumption. Since the regression equationwas significantly different from that of the line ofidentity, this equation was used to correct themeasured oxygen consumption values in the patientstudies.
240 P
2001
V02MEASURED
BY SERVOMEX
(ml min)
1601
1201
80F
40
0' a a a a a
a~~~~~~
V a 1.126160~ ~ ~~0
r 0.993
V -7302c
- 40 80 120 160 200 240V0 CALCULATED BY N2 INFUSION
02 (mlImin)Figure 3
Comparison of oxygen consumption calculated by nitrogen infusioninto the hood versus that measured by a Servomex paramagneticanalyzer. In regression equation VO2M is measured oxygen consump-tion by Servomex determination; Vo,c is calculated oxygen con-
sumption.
Circulation, Volume 50, October 1974
790
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
OXYGEN CONSUMPTION IN CHILDREN
Table 1
Patient Characteristics of the Five Sedation Groups
Group No. Variable Mean SEM
104 Age (years) 5.8 0.31Heart rate (beats/min) 128 2.12Weight (kg) 19.2 0.84Body surface area (m2) 0.76 0.026Oxygen consumption 139.6 4.26
(ml/min)
II 115 Age .5.8 0.49Heart rate 116 2.92Weight 20.5 1.66Body surface area 0.75 0.43Oxygen consumption 114.8 5.62
III 57 Age 6.1 0.61Heart rate 116 3.45Weight 21.6 2.12Body surface area 0.80 0.54Oxygen consumption 125.5 7.27
IV 28 Age 0.65 0.07Heart rate 140 5.72Weight 6.4 0.33Body surface area 0.33 0.01Oxygen consumption J59.7 4.26
V 37 Age 0.17 0.14Heart rate 156 3.90Weight 4.1 0.22Body surface area 0.24 0.008Oxygen consumption 35.2 2.88
The patient characteristics of the five sedationgroups are listed in table 1. It can be seen that groupsI, II and III have similar ages and represent olderchildren, whereas groups IV and V represent younginfants. These age differences are due to the fact thatmorphine sulphate (group IV) is used typically in in-fants at risk of developing hypoxemic spells and thatno sedation (group V) is used in infants during the firstweeks of life. The higher average heart rate in group I
compared to that of group II or III, is most likelysecondary to the administration of atropine. Theaverage oxygen consumption value was alsosignificantly higher in this group compared to that ofgroup II or Ill, with patients of comparable age andsize.
Table 2 gives the results of the stepwise regressionanalysis used to select the most significant predictivevariables for each patient group. Only the variableslisted were significant linear predictors of oxygen con-
sumption (P < 0.05) adjusted for other variables. Thesum of squares value reflects the correlation of a
variable to oxygen consumption excluding the interac-tion of other variables; the larger the sum of squaresthe greater the correlation. The P value indicates theprobability that the correlation with oxygen consump-
Circulation, Volume 50, October 1974
Table 2
Steptise Regression Analysis of Factors SignificantlyAffecting Oxygen Consumption
Sequential sumGroup Variable of squares P value
I Body surface area 73574 0.0001Heart rate 5551 0.0001Temperature 4951 0.0001Cyanosis 1938 0.0065Weight 1876 0.0079Sex 1751 0.0099
II Body surface area 341488 0.0001Cyainosis 2907 0.0110Heart rate 2752 0.0132Sex 2239 0.0243
III Weight 155685 0.0001Sex 1678 0.0070
IV Body surface area 3039 0.0001Cyanosis 647 0.0040Heart rate 453 0.0100
V Weight 3904 0.0001Heart rate 977 0.0002Age 287 0.0151
tion is due to chance. For example in each group bodysize has the highest correlation with oxygen consump-tion as indicated by the sequential sum of squares.Rectal temperature was an important correlate of oxy-gen consumption only for group I. However, this doesnot imply that oxygen consumption is unaffected bychanges in body temperature, but rather indicates it isnot of predictive value in estimating oxygen consump-tion in other groups. Both the Qp:Qs ratio andpulmonary hypertension are excluded from table 2since neither were significant predictive factors.We found, as did Wessel et al.,3 an increase in a
patient's activity invariably resulted in an increase inoxygen consumption. Since the oxygen consumptionvalues were obtained only after achieving a steadystate, the majority of patients remained motionlessduring the measurements. As a result patient activitywas not a significant factor in predicting oxygen con-sumption.From the results of the stepwise regression analysis
the best predictive equation for each patient groupwas formulated (table 3). Note that the predictiveequations for the patient groups contained differentvariables. This suggests that in order to obtain a moreaccurate prediction of oxygen consumption, the in-dividual patient characteristics and type of sedationshould be taken into consideration. For example, ifthe patient received a meperidine, promethazine andchlorpromazine mixture and had the followingcharacteristics: B.S.A., 0.87 m2; female, cyanosis,
791
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
FIXLER ET AL.
Table 3
Derived Regression Equations for Predicting Oxygen Consumption
Patientgroup Predictive equation 95% Tolerance limits
I Yo2 mI/mil = -663.3 + 188 B.S.A. - 1.47 Weight + 0.397 H.It. + 17.0 Temp -37 ml/min+ 22.8 (if cyanotic) - 11.3 (if female)
II Vo2 mI/mi - 10.56 + 132 B.S.A. -8.20 (if female) -20.6 (if cyanotic) -35 ml/min+ 0.263 H.W
III Vo2 mI/min = 58.96 + 3.29 Weight- 11.0 (if female) -30 ml/miiiIV Vo2 ml/miii = -62.22 + 243 B.S.A. + 0.41 H.R. - 15.5 (if cyanotic) -22 ml/minV Vo2 ml/min = -65.75 + 9.37 Weight + 0.38 H.R. + 19.17 Age -13 ml/min
Abbreviations: Vo2 = Oxygen consumption; B.S.A. = Body surface area (i2); Temp. = Rectal temperature(centigrade); H.R. = Heart rate (beats/min); Weight = Kilograms; Cyanotic = Systemic arterial oxygensaturationi <88%o; Age = Years.
heart rate 120, then oxygen consumption would bepredicted by the following calculations:-10.56 + (132) (0.87) - 8.20 - 20.6 + (0.263) (120);which equals 107 ml/mim.To test the true predictive capabilities of the model
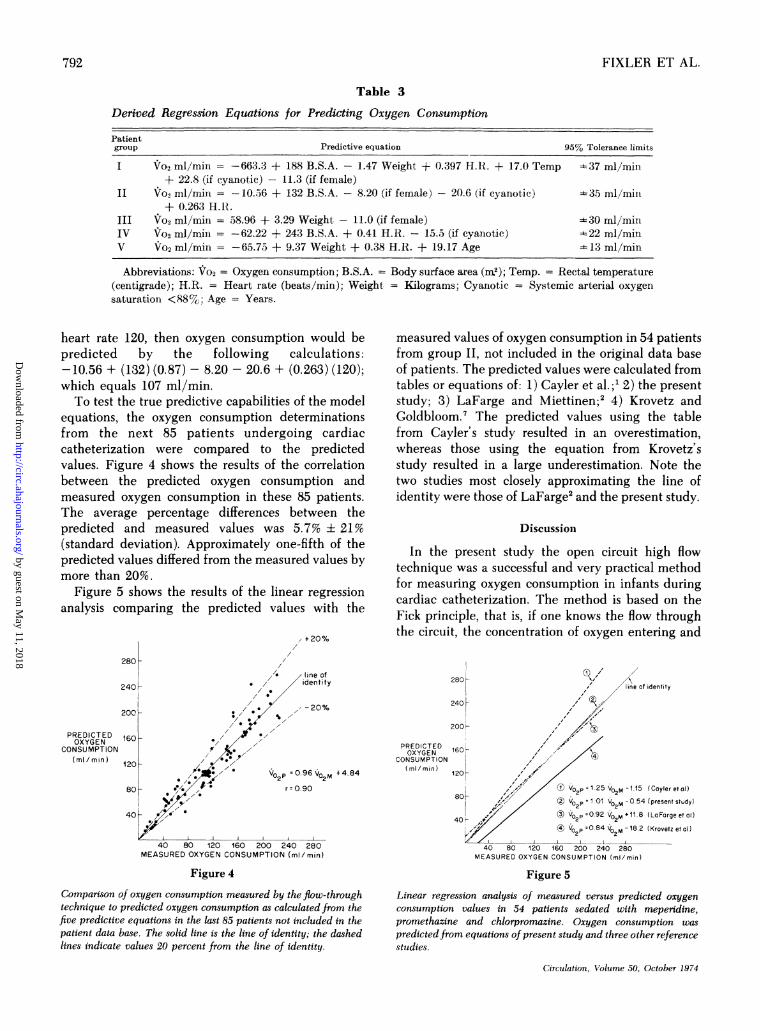
equations, the oxygen consumption determinationsfrom the next 85 patients undergoing cardiaccatheterization were compared to the predictedvalues. Figure 4 shows the results of the correlationbetween the predicted oxygen consumption andmeasured oxygen consumption in these 85 patients.The average percentage differences between thepredicted and measured values was 5.7% ± 21%(standard deviation). Approximately one-fifth of thepredicted values differed from the measured values bymore than 20%.
Figure 5 shows the results of the linear regressionanalysis comparing the predicted values with the
+20%
measured values of oxygen consumption in 54 patientsfrom group II, not included in the original data baseof patients. The predicted values were calculated fromtables or equations of: 1) Cayler et al.;' 2) the presentstudy; 3) LaFarge and Miettinen;2 4) Krovetz andGoldbloom.7 The predicted values using the tablefrom Cayler's study resulted in an overestimation,whereas those using the equation from Krovetz'sstudy resulted in a large underestimation. Note thetwo studies most closely approximating the line ofidentity were those of LaFarge2 and the present study.
Discussion
In the present study the open circuit high flowtechnique was a successful and very practical methodfor measuring oxygen consumption in infants duringcardiac catheterization. The method is based on theFick principle, that is, if one knows the flow throughthe circuit, the concentration of oxygen entering and
280L
line of2401- * / / identity
200 --20%
160 -
120-/,/W' Vo P = 0.96VOM+ 4.84
2280- *% r=O.9O
40 t4O ,g', I
40 80 120 160 200 240 280MEASURED OXYGEN CONSUMPTION (mI/min)
line of identity
240 h200;r
PREDICTED 6OXYGEN
CONSUMPTION(mi/min) 1201-
801-
40-
p=1.25 VOM 1.15 ICoyler etol)
V°P 1 01 VO2M -0 54 (present study)
,/ (X) 02 p0.92 V02M+11 8 (LaForgeet al)4 V02p 084 VO2M -182 (Krovetzetal)
40 80 120 160 200 240 280MEASURED OXYGEN CONSUMPTION (mi/min)
Figure 4
Comparison of oxygen consumption measured by the flow-through
technique to predicted oxygen consumption as calculated from thefive predictive equations in the last 85 patients not included in thepatient data base. The solid line is the line of identity; the dashedlines indicate values 20 percent from the line of identity.
Figure 5
Linear regression analysis of measured versus predicted oxygen
consumption values in 54 patients sedated with mependine,promethazine and chlorpromazine. Oxygen consumption was
predictedfrom equations of present study and three other referencestudies.
Circulation, Volume 50, October 1974
PREDICTEDOXYGEN
CONSUMPTION(mi min)
792
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from

OXYGEN CONSUMPTION IN CHILDREN
the concentration of oxygen leaving, then the ex-change of oxygen ('Jo2) in the circuit can be calculated.The requirements for applying the Fick principle are:1) constancy of flow, 2) ability to measure represen-tative samples of inflow and outflow oxygen concen-trations, 3) no loss of gas from the circuit. With thepresent method, constancy of flow is assured by con-tinuous monitoring with a rotameter. Since thedifferences between inflow and outflow oxygen con-centrations are very small (on the order of 0.50%), theoxygen analyzer must be extremely sensitive andstable. For example, to be able to measure the oxygenconcentration differential to within an accuracy ofi 10%, the analyzer must be capable of measuringoxygen differences as small as 0.05 percent. Kap-pagoda and Linden4 have demonstrated that the Ser-vomex paramagnetic oxygen analyzer has suitablestability and sensitivity. To decrease potential loss ofexpiratory gases this flow-through technique producesa small negative pressure within the hood. However itis still essential to meticulously seal the edges of thehood to the patient and to the table to insure that lossof expiratory gases does not occur. Previous authors4have measured the pressure within the hood using adifferential air pressure gauge to check that negativepressure is maintained. It is also important to adjusthood flow such that the oxygen concentrationdifferential between inflow and outflow gases is lessthan 1.0% to prevent carbon dioxide accumulation.Many pediatric cardiology laboratories do not
measure oxygen consumption in infants and smallchildren but assume a value from predictive tables.The validity of making such an assumption is open toserious questions since the individual patientcharacteristics may differ significantly from those ofthe population upon which the tables were based. Un-fortunately the amount of oxygen consumed by an in-dividual during the catheterization procedure is ex-tremely variable, being influenced by environmentaltemperature, level of activity, sedation, andcatecholamine secretion. Most cardiac catheterizationlaboratories make an effort to control environmentaltemperature, especially when dealing with small in-fants, to minimize this effect upon metabolism andcirculation. Similar precautions were taken in thisstudy; however, rectal temperature was a significantvariable influencing oxygen consumption in thepatient group anesthetized with atropine andketamine. These data indicate that when using thisregimen, temperature should be monitored and takeninto account if assuming an oxygen consumptionvalue.Baum and coworkers8 studied the effect of a
sedation mixture (meperidine, promethazine andchlorpromazine) on oxygen consumption in childrenCirculation, Volume 50, October 1974
undergoing cardiac catheterization. They found thatoxygen consumption fell in all patients during the car-diac catheterization procedure, reaching a minimumone-half to two hours after receiving the sedation andreturning to control levels near the end of theprocedure. They recommended oxygen consumptionbe measured at the time of blood sampling because ofthe temporal changes. In the present study the effectof different sedation regimens on oxygen consumptionwas determined after oxygen consumption hadstabilized thereby insuring that a steady state hadbeen achieved. The data were analyzed by a non-parametric technique taking into account the differentpatient characteristics of the five sedation groups. Thefact that each group had a distinctive set of variableswhich significantly influenced oxygen consumptionindicates that for a most accurate prediction thepatient should be classified according to the sedationregimen used. Since combinations of drugs were usedin most cases it is difficult to ascribe the action of aspecific drug as being responsible for the differencesbetween the sedation regimens.To our knowledge this is the first study which
reports oxygen consumption data in a large number ofinfants (170) continuously recorded during the cardiaccatheterization procedure. The study probably mostfrequently referred to for estimating oxygen consump-tion in infants is that of Cayler et al.' which reportsmeasurements in only 18 patients under the age of 2years. We felt that by using a larger data base ofpatients, regression equations could be formulatedwhich would provide a more accurate prediction ofoxygen consumption especially in this younger agegroup. The patients were separated according to thetype of sedation or anesthetic used in order to offsetthis one particular variable. The patients in Cayler'sstudy' received a sedation mixture similar to ourgroup II (they gave approximately 80 percent moremeperidine). Figure 5 shows the results of regressionanalysis of measured versus predicted oxygen con-sumption values in 54 patients sedated with this mix-ture. The predicted oxygen consumption values usingCayler's tables resulted in a large overestimation ofoxygen consumption. A major difference between thatstudy and ours is that they collected expired air usinga face mask or a mouthpiece, whereas the presentstudy collected expired gases without disturbing thepatient. These data suggest that the application offacial apparatus may significantly increase oxygenconsumption and raises the question whether oxygenconsumption in undisturbed patients can be predictedaccurately from data obtained in infants having masksor mouthpieces. Figure 5 also demonstrates that usingthe predictive equation published by Krovetz andGoldbloom7 resulted in a large underestimation of oxy-
793
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
FIXLER ET AL.
gen consumption. This difference may be due to thefact that patients in the present study had significantheart disease whereas their patients had nohemodynamically significant heart disease. This againpoints out the pitfall of assuming an individual patienthas similar characteristics to those of the populationupon which the predictive tables were based.
Despite our attempts to minimize the many factorswhich influence oxygen consumption our predictiveequations had rather broad 95% tolerance levels (table3). These findings are similar to the data of LaFargeand Miettinen2 who reported that the standard devia-tion of the differences between measured oxygen con-sumption/m2 and the corresponding value calculatedfrom their regression equation was 28.0 ml/min/m2.Kappagoda et al.,' using a similar flow-throughtechnique as in the present report, found the 95%tolerance limit for predicted values was 30 ml/min.Since it is a dictum of statistics that one can usuallypredict best with the same data used in deriving theregression equations, we checked the true predictivecapabilities by using data obtained in the next 85patients who were not in the original data base (fig. 4).In this latter sample the average percent differencebetween the measured and the predicted oxygen con-sumption values was 5.7% + 21 (SD). In ap-proximately one-fifth of the cases predicted valuesdiffered from measured values by more than 20%. Inour own study strict requirements were made toachieve a steady state before oxygen consumption wasmeasured and even then, large errors occurred withestimating oxygen consumption.Many pediatric centers do not measure oxygen con-
sumption because of the false impression that only byusing expensive, complicated instruments andprolonging the catheterization procedure can suchmeasurements be accomplished. Previous reports3' 4 aswell as the present study demonstrate that the flow-through method is particularly suitable for measuringoxygen consumption in the pediatric catheterizationlaboratory. It has several distinct advantages in that itis not disturbing to the patient, does not interfere withthe catheterization procedure itself, is learned readilyby the technician, and is relatively inexpensive. Incontrast, Douglas bag collections of expired gases aretime consuming, may increase oxygen consumption,and require the full cooperation of the patient. In the
present study the output of the Servomex oxygenanalyzer was recorded continuously, readily allowingrecognition of a steady state and thereby indicatingwhen oxygen consumption measurements and bloodsampling could optimally be performed.
In conclusion although the present study providesmore accurate predictive equations for estimatingoxygen consumption, the data indicate that relativelylarge errors may result when oxygen consumption isestimated. A simple method for measuring oxygenconsumption is presented which has been criticallyevaluated by several investigators. The apparatus isrelatively inexpensive and particularily suitable foruse in the pediatric laboratory. It is thereforerecommended that oxygen consumption not be es-timated from tables or regression equations but bemeasured continuously throughout the catheteriza-tion procedure.
Acknowledgment
The authors express their appreciation to William Romans of theBiomedical Engineering Section for assembling the apparatus.
References
1. CAYLER CG, RUDOLPH AM, NADAS AS: Systemic blood flow ininfants and children with and without heart disease.Pediatrics 32: 186, 1963
2. LAFARCE CG, MIETTINEN OS: The estimation of oxygenconsumption. Cardiovasc Res 4: 23, 1970
3. WESSEL HU, RORENi D, MUSTER AJ, ACEVEDO RE, PAUL MH:The continuous determinations of oxygen uptake in sedatedinfants and children during cardiac catheterization. Am JCardiol 24: 376, 1969
4. KAxPPACODA CT, LINDEN RJ: A critical assessment of an opencircuit technique for measuring oxygen consumption. Car-diovasc Res 6: 589, 1972
5. TALBOT NB, SOBELEH EH, McARTHUR JW, CRAWFORD JD:Functional Endocrinology From Birth through Adolescence.Cambridge, Mass. Commonwealth Fund, Harvard Univer-sity Press, 1952
6. SNEDE OR GW, COCHRAN WG: Statistical Methods. Ames: IowaState University Press, 1967
7. KROVETZ LJ, GOLDBLOOM S: Normal standards forcardiovascular data. 1. Examination of the validity of cardiacindex. Hopkins Med J 130: 174, 1972
8. BAUtxi D, BAUNI AC, CHURCH SC: Effect of sedation on oxygenconsumption of children undergoing cardiac catheterization.Pediatrics 39: 891, 1967
9. KAPPA(.ODA CT, GREENWOOD P, MACARTNEY FJ, LINDEN RJ:Oxygen consumption in children with congenital disease ofthe heart. Clin Sci 45: 107, 1973
Circulation, Volume 50. October 1974
794
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from
WILLIAM W. MILLERDAVID E. FIXLER, TED CARRELL, RICHARD BROWNE, KATHRYN WILLIS and
Different Sedation RegimensOxygen Consumption in Infants and Children during Cardiac Catheterization under
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1974 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.50.4.788
1974;50:788-794Circulation.
http://circ.ahajournals.org/content/50/4/788the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 11, 2018
http://circ.ahajournals.org/D
ownloaded from





























