Embed Size (px)
Citation preview

Seizure 21 (2012) 780–784
Oxidative stress in patients with epilepsy is independent of antiepileptic drugs
Bindu Menon a,*, Krishnan Ramalingam b, Rajendiran Vinoth Kumar b
a Department of Neurology, Narayana Medical College and Superspeciality Hospital, Chintareddypalem, Nellore-2, Andhra Pradesh, Indiab Department of Biochemistry, Narayana Medical College and Superspeciality Hospital, Chintareddypalem, Nellore-2, Andhra Pradesh, India
A R T I C L E I N F O
Article history:
Received 3 April 2012
Received in revised form 31 August 2012
Accepted 2 September 2012
Keywords:
Lipid peroxidation
Protein carbonylation
Nitric oxide
Malondialdehyde
Seizures
Epilepsy
Antiepileptic drugs
A B S T R A C T
Purpose: Oxidative stress has been implicated in many pathological processes. The brain is highly
susceptible to oxidative stress because of its high lipid content. In this study, the oxidative parameters in
patients with epilepsy and those of a control group were measured. The study’s aim was to determine
whether there are differences between the oxidative levels of treated and untreated patients and
whether there are differences between individual antiepileptic drugs.
Methods: Oxidative parameters such as Malondialdehyde (MDA), Protein Carbonylation (PC) and Nitric
Oxide (NO) levels were evaluated in 100 patients with epilepsy and compared to an equal number of age
and sex matched healthy subjects. In the study group, the oxidative parameters of 25 untreated patients
were compared to treated patients and the control group. The treated patients were divided into 2
groups based on their antiepileptic drugs (AEDs). Group 1 consisted of patients on a single AED, and
group 2 was composed of patients taking more than one AED. A comparative study was performed on the
oxidative parameters of medicated patients on single drug regimens and multidrug regimens.
Results: The MDA and PC levels were significantly higher in patients than in the control group
(P < 0.0001). However, there was no significant difference in the NO levels of patients and those of the
control group. The 25 untreated patients had higher MDA and PC levels compared to both the control
group (P < 0.0001) and treated patients (P < 0.0001). There was no difference in the oxidative levels
between untreated patients and treated patients, group 1 and group 2, and individual AEDs.
Conclusions: In this study, we demonstrated the presence of significantly increased levels of oxidative
markers in patients with epilepsy as compared to the control group. AEDs did not influence the oxidative
markers, suggesting the presence of seizure-induced oxidative stress.
� 2012 British Epilepsy Association. Published by Elsevier Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Seizure
journal homepage: www.e lsev ier .com/ locate /yse iz
1. Introduction
Epilepsy is a chronic neurological disorder that requires longterm treatment. Various studies have demonstrated the role ofoxidative stress in the pathogenesis of atherosclerosis, psychiatricand neurodegenerative disorders.1–3 The brain is generally in abalanced redox state between oxidative and reactive conditions.However, reactive oxygen species have damaging effects when theyare produced in excessive amounts and are unable to be eliminatedby endogenous antioxidants. The brain remains particularlyvulnerable to oxidative stress because of its high demand foroxygen. The oxygen is needed because the brain derives energy fromoxidative phosphorylation in mitochondrial respiratory chains.4–6 Adisproportionate production of free radicals compared to antioxi-dant levels is thought to be an important contributory factor to thepathogenesis of several diseases by oxidative injury. Free radicals
* Corresponding author. Tel.: +91 861 2317963/64/68x2358;
mobile: +91 9866223905.
E-mail address: [email protected] (B. Menon).
1059-1311/$ – see front matter � 2012 British Epilepsy Association. Published by Else
http://dx.doi.org/10.1016/j.seizure.2012.09.003
can also exacerbate some forms of seizure. The end products of lipidperoxidation, protein carbonyl groups and nitric oxide have been themost studied markers of oxidative damage. Animal studies asseizure models have provided evidence of increased oxidative stress(increased lipid peroxidation and protein carbonylation) followingseizures.7–9 However, the role of nitric oxide is still debatable. Somestudies have shown increased levels of nitric oxide in patients,13
while other studies have demonstrated that nitric oxide has abeneficial role as an anticonvulsant11,12 or have had inconclusiveresults.10 AEDs may also modulate oxidative stress in epilepticpatients.14 Animal studies (in which antioxidants were used inaddition to anticonvulsants) showed decreased oxidative stress andreduced frequency of seizures.6,15,16 The complex mechanism ofepileptogenesis remains largely unclear. However, neuronal death isone of the important events, and factors altering or influencing thisevent may play an important role. Oxidative stress by free radicalgeneration does indeed play a role in mitochondrial dysfunction andcell death.
The aim of this study is to determine the effects of epilepsy onnitric oxide levels, lipid peroxidation and protein carbonylationlevels in patients with epilepsy and a healthy control group. The
vier Ltd. All rights reserved.

Table 1Demographic and treatment details of patients and control group.
Entire
group
Control Treated
patients
Untreated
patients
Age (yrs) 26.23�10.6 26.55�8.5 26.50�10.78 24.76�9.96
Sex (M:F) 56: 44 52:48 38:37 18:7
Duration of
illness (yrs)
7�6 – 6�5 4�2
Duration of
treatment (yrs)
7�5 – 5�4 –
Waist/hip ratio 0.95� 0.12 0.63–1.2 59.15�22.35 57.79�13.69
Body mass index 22.01�4.30 12–32.4 13.25�4.27 21.09�4.21
Table 2Biochemical and oxidative parameters in patients and control group.
Parameter Mean� SD P value
Patient Control
Haemoglobin, g/dl 13.40�2.11 13.36�1.81 0.88
Fasting blood sugar, mg/dl 84.18�14.63 83.11�7.45 0.51
Serum creatinine, mg/dl 0.95�0.16 1.04�0.24 0.002
Total cholesterol, mg/dl 178.40�40.04 167.5�37.78 0.05
HDL, mg/dl 46.49�11.63 45.4�10.06 0.48
LDL, mg/dl 112.70�27.71 102.5�29.08 0.01
Triglyceride, mg/dl 95.29�34.73 106.3�45.55 0.07
VLDL, mg/dl 19.23�7.04 20.97�9.047 0.13
Total bilirubin, mg/dl 0.82�0.05 0.82�0.072 0.33
SGOT, IU/L 36.22�21.11 37.21�18.7 0.72
SGPT, IU/L 30.31�20.79 27.05�19.56 0.25
Alkaline phosphatase, IU/L 223.40�72.55 181.6�59.44 <0.0001
Total proteins, g/dL 7.83�0.62 7.81�0.46 0.85
Albumin, g/dL 3.95�0.35 3.8�0.37 0.27
MDA, mmol/L 6.80�2.84 1.64�0.82 <0.0001
NO, nmol/L 50.41�18.29 51.95�9.56 0.45
PC, nmol/mg of protein 0.71�0.19 0.46�0.16 <0.0001
HDL: high density lipoprotein; LDL: low density lipoprotein; VLDL: very low density
lipoprotein; SGOT: serum glutamic oxaloacetic transaminase; SGPT: serum
glutamic pyruvate transaminase; MDA: malondialdehyde; PC: protein carbonyla-
tion; NO: nitric oxide.
B. Menon et al. / Seizure 21 (2012) 780–784 781
study also intends to assess the oxidative stress in patients withepilepsy who are not taking antiepileptic drugs and the effects ofAEDs, if any, in patients receiving monodrug or multidrug therapy.
2. Materials and methods
The study was composed of 100 patients with epilepsy whowere diagnosed with idiopathic generalised epilepsy on antiepi-leptic therapy. One hundred age and sex matched healthyvolunteers served as the control group.
Patients included in the study had been seizure free for morethan 3 days. All patients underwent a detailed examination whichincluded demographics, seizure frequency, duration of illness andtreatment. Patients with chronic medical illnesses such ashypertension, diabetes, rheumatoid arthritis, collagen vasculardisease, chronic neurological illness or localisation related epilep-sy; those who were smokers, alcoholics, tobacco chewers; andthose taking any other medications were excluded from the study.EEG was performed in all patients, and several patients underwentneuroimaging for definitive diagnoses.
Five millilitres of venous blood was collected after an overnightfast, and 2 ml was transferred to EDTA-coated vacutainers forhaemoglobin estimation. The remaining blood was transferred toclot activator coated vacutainers, allowed to clot and centrifugedfor 5 min at 3000 rpm to obtain serum that was stored at�20 8C forfurther analysis. The serum samples were used to analyse routinebiochemical investigation and oxidative biomarkers. The oxidativeparameters tested were lipid peroxidation, protein carbonylationand nitric oxide levels. Lipid peroxidation was estimated bymeasuring the Malondialdehyde levels using a UV-visible spec-trophotometer.17 We used the TBARS Assay (thiobarbituric acidreactive substances assay) to determine the Malondialdehyde(MDA) levels, the end product of lipid peroxidation.18 Proteincarbonylation (PC) was estimated with the Resnic and Packermethod.19 We measured the oxidation of the protein by addingcarbonyl groups to the spectrophotometric assay using 2,4-DNPH(2,4-dinitrophenylhydrazine) for detecting carbonyls.20 Carbony-lated plasma protein reacts with 2,4-DNPH, and the complex wasmeasured at 360 nm.21 Nitric oxide (NO) levels were determinedusing the Griess reagent in which NO reacts with 1% sulphani-lamide in 5% phosphoric acid, and 10% naphthalene ethylenedia-mine dihydrochloride forming chromospheres, which can be readat 543 nm.22
The oxidative levels were compared between patients and thecontrol group. The 25 patients who were not on AEDs werecompared with both patients on AEDs and the control group toeliminate the effects of the antiepileptic drugs. Depending upontreatment, the patients were divided into group 1 or group 2,composed of Monotherapy and Polytherapy recipients, respec-tively. Those patients on Monotherapy were treated with one ofthe following antiepileptic drugs: Carbamazepine, Phenytoin,Valproate, Clobazam, Phenobarbital, Lamotrigine, Topiramate orLevetiracetam. Group 2 was composed of patients on more thanone drug (Polytherapy). The oxidative parameters were comparedamong patients on Monotherapy. All patients provided writteninformed consent. The study was approved by the InstitutionalEthics Committee.
2.1. Statistical analysis
The data were analysed with the statistical package SPSS forWindows, version 11.5. Descriptive analyses are expressed asmean � S.D. Paired t-tests were performed between patients andcontrols, before treatment and controls, and before and aftertreatment. One way analysis of variance (ANOVA) was used toestimate the differences between the study groups. Correlation
coefficients were determined by Pearson’s correlation test. P < 0.05was considered to be statistically significant.
3. Results
The study included 100 patients with epilepsy (56 males, 44females) and 100 control subjects (52 males, 47 females). Themean ages of the patients and control group were 26 � 10 and26 � 8 years, respectively. The mean duration of illness in the patientswas 7 � 6 yrs. Twenty-five per cent of the patients were not ontreatment, 66% were on monotherapy (Carbamazepine 16%, Phenyt-oin 20%, Valproate 17%, others 13%), and 34% were on Polytherapy.The demographics and epilepsy profiles are shown in Table 1. Thebiochemical and oxidative parameters are shown in Table 2. The totalcholesterol, LDL and alkaline phosphatase levels were higher inpatients than in the control group with a significant p value (Table 2).The remainder of the biochemical parameters were normal.
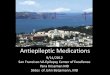
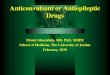
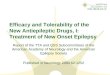
In the entire group, the MDA levels in patients(6.80 � 2.84 mmol/ml) were higher than those in the control group(1.64 � 0.82 mmol/ml) with a significant P < 0.001 (Graph 1). The PClevels (0.71 � 0.19 mg of protein/ml) in patients were higher thanthose of the controls (0.46 � 0.16 mg of protein/ml) with a significantP < 0.001 (Graph 2). However, the NO levels were not significantlydifferent between the patients (50.41 � 18.29) and control group(51.95 � 9.56) (P = 0.45) (Graph 3).
The mean ages of untreated patients and control group were24.76 � 9.96 and 25.72 � 7.77, respectively. Twenty-five patientswere not on AEDs. Hence, it was possible to evaluate the oxidativestress in these patients by eliminating the effects of AEDs.

[(Graph_1)TD$FIG]
Graph 1. Malondialdehyde levels in patients and the control group.
[(Graph_2)TD$FIG]
Graph 2. Protein carbonylation levels in patients and the control group.
[(Graph_3)TD$FIG]
Graph 3. Nitric oxide levels in patients and the control group.
B. Menon et al. / Seizure 21 (2012) 780–784782
The MDA levels of untreated patients (6.81 � 2.94 mmol/ml)were higher than those of the control group (1.75 � 0.94 mmol/ml),with a significant P < 0.001 (Graph 1). The PC levels (0.68 � 0.17 mgof protein/ml) of untreated patients were higher than those of thecontrol group (0.46 � 0.13 mg of protein/ml) with a significantP < 0.001 (Graph 2). However, the NO levels did not show anysignificant difference between untreated patients (47.96 � 18.00)and the control group (55.44 � 9.57) (P = 0.07) (Graph 3).
Table 3Demographics, lipid profiles and oxidative parameters in patients on various AED’s.
Parameter Mean� SD
Carbamazepine (n = 16) Phenytoi
Age 20.75�7.05 27.35�Total cholesterol 181.50�33.59 194.50�
HDL 48.00�7.81 52.45�
LDL 115.06�26.46 124.10�
Triglyceride 89.13�25.01 93.75�VLDL 17.63�5.06 18.55�MDA 6.52�2.01 6.66�NO 46.13�12.04 53.85�PC 0.77� 0.28 0.65�
HDL: high density lipoprotein; LDL: low density lipoprotein; VLDL: very low density li
There were no differences between the MDA levels in untreatedpatients (6.81 � 2.94 mmol/ml) versus the treated group(6.76 � 2.82 mmol/ml) (P = 0.94) (Graph 1), the PC levels in untreatedpatients (0.68 � 0.17 mg of protein/ml) and the treated group(0.71 � 0.19 mg of protein/ml) (P = 0.63) (Graph 2) or the NO levelsin untreated patients (47.96 � 18) and the treated group(51.08 � 15.26) (P = 0.44) (Graph 3).
3.1. Comparison between patients on monotherapy and polytherapy
No differences were found between groups 1 (monotherapy)and 2 (Polytherapy) with regard to the oxidative parameters. Theoxidative levels in monotherapy versus. Polytherapy were MDA(7.28 � 2.93 mmol/ml, monotherapy) (6.63 � 3.25 mmol/ml, poly-therapy) (P = 0.37) (Graph 1); PC (0.69 � 0.22 mg of protein/ml,monotherapy) (0.70 � 0.12 mg of protein/ml, polytherapy) (P = 0.89)(Graph 2); NO (49.69 � 18.67, monotherapy) (53.25 � 19.54, poly-therapy) (P = 0.43) (Graph 3), respectively.
3.2. Comparison between individual AEDs
The MDA, PC and NO levels of patients on Carbamazepine,Phenytoin and Valproate are shown in Table 3. ANOVA analysis didnot show any differences in oxidative levels between the groups.However, there was a difference in lipid parameters; the totalcholesterol, HDL and LDL levels were highest in patients takingPhenytoin and lowest in patients taking Carbamazepine.
P-value
n (n = 20) Valproate (n = 17)
8.86 25.76�9.87
45.77 156.59�25.63 CBZ/VPA P<0.02
PHT/VPA P<0.00
12.60 38.82�9.16 CBZ/VPA P<0.00
PHT/VPA P<0.00
30.05 98.29�18.01 CBZ/VPA P<0.04
PHT/VPA P<0.00
46.50 93.94�17.46 NS
9.26 19.71�4.21 NS
2.12 7.64�3.72 NS
21.73 49.47�16.78 NS
0.15 0.75� 0.25 NS
poprotein; MDA: malondialdehyde; PC: protein carbonylation; NO: nitric oxide.

B. Menon et al. / Seizure 21 (2012) 780–784 783
4. Discussion
This study included 100 patients with epilepsy and 100 healthycontrol subjects. Our study demonstrated that MDA and PC levelswere significantly higher in patients with epilepsy than in thecontrol group (P < 0.001), which is a finding that is consistent withprevious studies.23–25 However, the NO levels did not varybetween the 2 groups. The brain has a high lipid content, andits oxygen consumption and oxidative metabolism make itsusceptible to oxidative stress. Lipid peroxidation involvesoxidative degradation of lipids. Measuring Malondialdehyde, theend product of lipid peroxidation, is a relatively easy method forestimating lipid peroxidation.18 Protein oxidation is irreversibleoxidative damage, and protein damage is considered to be amarker for severe oxidative stress.19,26
Nitric oxide is a free radical that is formed biologically throughthe oxidation of L-arginine by nitric oxide synthase. The exact roleof NO in the pathophysiology of epilepsy is still unclear. Severalstudies have shown that NO may act as an endogenousanticonvulsant.27–29 Although some studies have shown that NOacts as a proconvulsant,30–32 our study did not find any differencein NO levels between the patients and control group.
In our study, 75 out of the 100 patients with epilepsy were ontreatment for durations of 5 � 4 years. We report significantly highlevels of MDA (P < 0.001) and PC (P < 0.001) in 75 patients whencompared to those of the healthy control group, but with nodifference between NO levels. Our study showed that patients whowere not on AEDs also had high MDA (P < 0.001) and PC levels(P < 0.001) with no difference in NO levels when compared to thehealthy control group (P < 0.07). Because we found that patients whonot on AEDs also had high oxidative levels, we compared this groupwith patients on AEDs. We did not find any significant differencesbetween the 2 groups with regard to MDA (P = 0.54), NO (P = 0.51)and PC levels (P = 0.373). Furthermore, we did not find any differencein oxidative parameters in patients on monotherapy and polytherapy.Altogether, we conclude that oxidative stress is present in patientswith epilepsy and that AEDs do not appear to play any role. Similarresults have been documented in previous studies.23,24 Severalexperimental models of seizures have demonstrated increased levelsof oxidative stress markers in various regions of the brain afterseizures. Increased lipid peroxidation has been demonstrated inelectroshock-induced seizures in mice in the entire brain,33
Pentylenetetrazol (PTZ)-induced seizures in the entire cortex inrats,4 mice hippocampus6 and pilocarpine-induced status epilepticusin rat hippocampus.33 These experimental studies have suggestedthat seizures induce oxidative stress, which is confirmed in our studyas well as others.23,24 Recurrent seizures and prolonged seizures havebeen found to result in both necrosis and apoptosis of a specific area ofhippocampus, CA3, in experimentally induced seizures.34 Highoxidative stress and free radical generation are possible reasons forseizure-induced apoptosis and neuronal death.
Patients were also found to have high levels of cholesterol, LDLand serum alkaline phosphatase as compared to the control group.There are reports that show correlations between high LDL levels,oxidative stress and endothelial dysfunction.35,36 Furthermore,studies have shown that oxidative stress could be an early event inthe evolution of hyperlipidemia.37 In our study, correlationanalysis was not significant between lipid parameters andoxidative levels. Hence, we can only comment that patients withepilepsy had high oxidative stress with dyslipidemia, but furtherstudies are needed to confirm this correlation.
Various studies have shown that AEDs appear to modulateoxidative stress. Studies have reported increased NO levels inpatients treated with VPA.38,39 Patients with epilepsy treated withPhenytoin, Carbamazepine and Valproate have increased MDAlevels.23,40,41 In our study, patients were on Carbamazepine,
Phenytoin and Valproate or Polytherapy regimens. Increased MDAand PC levels were found in patients on AEDs. There was a variationin the Cholesterol, HDL and LDL levels between individual AEDs,but there were no differences in the oxidative parameters.However, our study had a relatively small number of subjects ineach group. Studies with larger sample sizes are needed to confirmthese results.
These results have therapeutic implications. Whether freeradicals released after seizure episodes lead to further seizures orrefractory epilepsy needs to be addressed. However, oxidativestress has indeed been implicated in several other diseasesincluding epilepsy. Few studies in animal models show the effectsof antioxidants in decreasing the oxidative stress. Antioxidantmelatonin has been found to decrease seizure activity or delay thedevelopment of epileptiform discharges in ferric chloride inducedseizure models in rodents. This phenomenon was also found toaccompany decreased levels of lipid peroxidation.38,39
Most of the previous studies were performed on patients whowere already on treatment and could not conclude that theoxidative stress is a result of epilepsy or AEDs. Some studies havecompared treated and untreated patients and found no differ-ence.20,38 Considering the results of these studies, including ours,the role of AEDs in increasing oxidative stress is negligible.
In conclusion, our study demonstrated that there weresignificantly increased levels of oxidative markers in patientswith epilepsy. AEDs did not influence oxidative markers, whichsuggests that seizures induce oxidative stress. The mechanism ofepileptogenesis is still unclear. Even with the advent of newerAEDs, a significant proportion of patients are refractory totreatment. Hence, it is important to have novel methods oftherapy, which include AEDs with possible adjunctive antioxidanttherapy.
This study adds information to the existing literature andnecessitates further detailed research to understand the mecha-nism of epilepsy to promote newer modalities of diseasemodification.
Conflict of interest statement
None of the authors have any conflicts of interest to disclose.
Acknowledgement
The study was supported by a grant from the InternationalEpilepsy Trust.
References
1. Lohr JB. Oxygen radicals and neuropsychiatric illnesses. Archives of GeneralPsychiatry 1991;48:1097–106.
2. Christen Y. Oxidative stress and Alzheimer disease. American Journal of ClinicalNutrition 2000;71:621s–9s.
3. Coyle JT, Puttfarcken P. Oxidative stress, glutamate, and neurodegenerativedisorders. Science 1993;262:689–95.
4. Bashkatova V, Narkevich V, Vitskova G, Vanin A. The influence of anticonvulsantand antioxidant drugs on nitric oxide level and lipid peroxidation in the ratbrain during pentylenetetrazole-induced epileptiform model seizures. Progressin Neuro-Psychopharmacology and Biological Psychiatry 2003;27(3):487–92.
5. Erakovic V, Zupan G, Varljen J, Simonic A. Entylenetetrazole-induced seizuresand kindling: changes in free fatty acids, superoxide dismutase, and glutathioneperoxidase activity. Neurochemistry International 2003;42(2):173–8.
6. Patsoukis N, Zervoudakis G, Georgiou CD, Angelatou F, Matsokis NA, Panago-poulos NT. Effect of pentylenetetrazole-induced epileptic seizure on thiol redoxstate in the mouse cerebral cortex. Epilepsy Research 2004;62(1):65–74.
7. Barber AA, Bernheim F. Lipid peroxidation its measurement occurrence andsignificance in animal tissues. Advances in Gerontological Research 1967;2:355–403.
8. Singh R, Pathak DN. Lipid peroxidation and glutathione peroxidase, glutathionereductase, superoxide dismutase, catalase and glucose 6 phosphate dehydro-genase activities in FeCl induced epileptogenic foci in the rat brain. Epilepsia1990;31(1):15–26.

B. Menon et al. / Seizure 21 (2012) 780–784784
9. Lapouble E, Montecot C, Sevestre A, Pichon J. Phosphinothricin induces epilepticactivity via nitric oxide production through NMDA receptor activation in adultmice. Brain Research 2002;957(1):46–52.
10. Arhan E, Serdaroglu A, Ozturk B, Ozturk HS, Ozcelik A, Kurt N, et al. Effects ofepilepsy and antiepileptic drugs on nitric oxide, lipid peroxidation and xanthineoxidase system in children with idiopathic epilepsy. Seizure 2011;20(2):138–42.
11. Barbiro-Michaely E, Mendelman A, Mayevsky A. The evaluation of nitric oxideinvolvement in Metrazol induced status epilepticus using multiparametricmonitoring. Brain Research 2011;1377:50–9.
12. Ayyildiz M, Yildirim M, Agar E. The involvement of nitric oxide in the anticon-vulsant effects of alpha-tocopherol on penicillin-induced epileptiform activityin rats. Epilepsy Research 2007;73(2):166–72.
13. Ibragic S, Sofic E, Suljic E, Avdagic N, Bajraktarevic A, Tahirovic I. Serum nitricoxide concentrations in patients with multiple sclerosis and patients withepilepsy. Journal of Neural Transmission 2012;119(1):7–11.
14. Yuksel A, Cengiz M, Seven M, Ulutin T. Erythrocyte glutathione, glutathioneperoxidase, superoxide dismutase and serum lipid peroxidation in epilepticchildren with valproate and carbamzepine monotherapy. Journal of BasicClinical Pharmacology 2000;11(1):73–81.
15. Tan DX, Manchester LC, Reiter RJ, Qi W, Kim SJ, El-Sokkary GH. Melatoninprotects hippocampal neurons in vivo against kainic acid-induced damage inmice. Journal of Neuroscience Research 1998;54(3):382–9.
16. Willmore LJ, Triggs WJ, Gray JD. The role of iron-induced hippocampal peroxi-dation in acute epileptogenesis. Brain Research 1986;382(2):422–6.
17. Yagi K, Lipid peroxides. human a disease. Chemistry and Physics of Lipids1987;45(2–4):337–51.
18. Marnett LJ. Lipid peroxidation-DNA damage by malondialdehyde. MutationResearch 1999;424(1–2):83–95.
19. Reznick. Packer L. Oxidative damage to proteins: spectrophotometric methodfor carbonyl assay. Methods in Enzymology 1994;233:357–63.
20. Levine RL, Williams JA, Stadtman ER, Shacter E. Carbonyl assays for determina-tion of oxidatively modified proteins. Methods in Enzymology 1994;233:346–57.
21. Levine RL, Wehr N, Williams JA, Stadtman ER, Shacter E. Determination ofcarbonyl groups in oxidized proteins. Methods in Molecular Biology 2000;99:15–24.
22. Giustarini D, Rossi R, Milzani A, Dalle-Donne I. Nitrite and nitrate measurementby Griess reagent in human plasma: evaluation of interferences and standardi-zation. Methods in Enzymology 2008;440:361–80.
23. Hamed SA, Abdellah MM. Trace elements and electrolytes homeostasis andtheir relation to antioxidant enzyme activity in brain hyperexcitability ofepileptic patients. Journal of Pharmacological Sciences 2004;96(4):349–59.
24. Rao AV, Rao A. Oxidative stress and antioxidants in epilepsy. Clinica ChimicaActa 2001;303(1–2):19–24.
25. Ercegovac M, Jovic N, Simic T, Beslac-Bumbasirevic L, Sokic D, Djukic T, et al.Byproducts of protein, lipid and DNA oxidative damage and antioxidant en-zyme activities in seizure. Seizure 2010;9(4):205–10.
26. Stadtman ER, Starke-Reed PE, Oliver CN, Carney JM, Floyd RA. Protein modifi-cation in aging. EXS 1992;62:64–72.
27. RondouinG,Lerner-NatoliM,ManzoniO,Lafon-CazalM,BockaertJ.Anitricoxide(NO)synthase inhibitor accelerates amygdala kindling. Neuroreport 1992;3(9):805–8.
28. Theard MA, Baughman VL, Wang Q, Pelligrino DA, Albrecht RF. The role of nitricoxide in modulating brain activity and blood flow during seizure. Neuroreport1995;6(6):921–4.
29. Bosnak M, Ayyildiz M, Yildirim M, Agar E. The role of nitric oxide in theanticonvulsant effects of pyridoxine on penicillin-induced epileptiform activityin rats. Epilepsy Research 2007;76(1):49–59.
30. Mollace V, Bagetta G, Nistico G. Evidence that L-arginine possesses proconvul-sant effects mediated through nitric oxide. Neuroreport 1991;2(5):269–72.
31. Osonoe K, Mori N, Suzuki K, Osonoe M. Antiepileptic effects of inhibitors ofnitric oxide synthase examined in pentylenetetrazolinduced seizures in rats.Brain Research 1994;663(2):338–40.
32. Murashima YL, Yoshi M, Suzuki J. Ictogenesis and epileptogenesis in EL mice.Epilepsia 2002;43:S130–5.
33. Dal-Pizzol F, Klamt F, Vianna MM, Schroder N, Quevedo J, Benfato MS, et al.Lipid peroxidation in hippocampus early and late after status epilepticusinduced by pilocarpine or kainic acid in Wistar rats. Neuroscience Letters2000;291(3):179–82.
34. Qi ST, Huang LJ, Wang KW, Kong WD, Fang LX, Peng L, et al. Association ofepileptiform activity with neuronal death in the CA3 subfield of the hippocam-pus following focally evoked limbic seizures. Di Yi Jun Yi Da Xue Xue Bao2001;21(11):831–3.
35. Al-Benna S, Hamilton CA, McClure JD, Rogers PN, Berg GA, Ford I, et al. Low-density lipoprotein cholesterol determines oxidative stress and endothelialdysfunction in saphenous veins from patients with coronary artery disease.Arteriosclerosis Thrombosis and Vascular Biology 2006;26(1):218–23.
36. Aikawa M, Sugiyama S, Hill CC, Voglic SJ, Rabkin E, Fukumoto Y, et al. Lipidlowering reduces oxidative stress and endothelial cell activation in rabbitatheroma. Circulation 2002;106(11):1390–6.
37. Yang RL, Shi YH, Hao G, Li W, Le GW. Increasing oxidative stress with progres-sive hyperlipidemia in human: relation between malondialdehyde and athero-genic index. Journal of Clinical Biochemistry and Nutrition 2008;43(3):154–8.
38. Peker E, Oktar S, Ari M, Kozan R, Dogan M, Cagan E, et al. Nitric oxide, lipidperoxidation, and antioxidant enzyme levels in epileptic children using val-proic acid. Brain Research 2009;1297:194–7.
39. Karabiber H, Yakinci C, Durmaz Y, Temel I, Mehmet N. Serum nitrite and nitratelevels in epileptic children using valproic acid or carbamazepine. Brain andDevelopment 2004;26(1):15–8.
40. Liu CS, Wu HM, Kao SH, Wei YH. Phenytoin-mediated oxidative stress in serumof female epileptics: a possiblepathogenesis in the fetal hydantoin syndrome.Human and Experimental Toxicology 1997;16(3):177–81.
41. Verrotti A, Scardapane A, Franzoni E, Manco R, Chiarelli. Increased oxidativestress in epileptic children treated with valproic acid. Epilepsy Research2008;78(2–3):171–7.