Embed Size (px)
Citation preview
OXFORD HEALTH NHS FT NICOTINE REPLACEMENT THERAPY (NRT) GUIDELINES
FOR:
SMOKING CESSATION/HARM REDUCTION
ENFORCED ABSTINENCE
February 2015
This guideline is an update to the April 2012 Oxford Health NHS FT NRT guideline
Approved by: Oxford Health NHS FT Drugs & Therapeutics Group Date: 25th February 2015 Version: 2 (minor amendment on page 10)
CONTENTS
Page
Background
3
Aims and Objectives
3
Smoking Cessation Advisors
4
Nicotine Replacement Therapy (NRT)
4
Drug Interactions
5
Counselling
5
NRT products available
6
How to choose which NRT to prescribe
8
NRT assessment and supplies
9
NRT prescription examples
10
Management and monitoring prescriptions for planned quit
10
Contact details
11
References
11
Appendix A- Smoking cessation advice for Named Nurse
12
Appendix B – Smokers questionnaire
13
Appendix C – Smoking Cessation Pathway
15
Appendix D – Nicotine Replacement Therapy (NRT) Prescription Chart
16
Appendix E – Enforced smoking abstinence protocol for nursing staff
17
3
BACKGROUND
The Trust will be smoke free across all its sites from March 2nd 2015. No smoking will be allowed in
any of the trust’s buildings or within the grounds. The move brings the trust in line with with the
National Institute for Health and Clinical Excellence (NICE) guidelines to have 100% smoke-free
sites.
Oxford Health cares for patients with a wide range of conditions – both physical and mental. All hospitals have a duty of care to help smokers to quit and all Oxford Health patients should be given the support to stop if they wish to. Smoking rates are much higher among people with mental health problems than the general population and many of these people want to stop smoking but do not receive the advice and support they need to do so. Good evidence exists that smokers with mental health problems can be helped to stop smoking in line with current NICE guidelines.
Ideally, abrupt quitting offers the best chance of lasting smoking cessation. However, this is very hard for most smokers to do due to their addiction to nicotine. Nicotine replacement therapy (NRT) aims to replace the nicotine from cigarettes by other means of delivery; such as via transdermal patches, chewing gum, lozenges, sublingual tablets, inhalators or nasal spray. NRT can be expected to deliver less nicotine (and none of the other potentially disease-causing agents) than would be obtained from cigarettes; thereby providing a background level of nicotine that reduces craving and withdrawal, while producing lower blood nicotine concentrations than smoking does. NRT can help smokers to cut down before stopping, reduce smoking or abstain from smoking altogether. Evidence show that NRT together with behavioural support increases quit chances by up to 20% from 6% if using NRT alone. NRT, therefore, should ideally only be prescribed as part of a programme of support in which the smoker makes a commitment to stop smoking on or before a particular date (target stop date). Smokers should be offered advice and encouragement to aid their attempt to quit. To maximize the benefits of NRT, people wishing to use this service should be strongly encouraged to access the behavioural support provided as part of their quit attempt.
Local Stop Smoking Services can provide specialist advice to help health professionals support smokers to stop. There is a need for staff in different clinical areas to gain basic smoking cessation training and act as smoking cessation advisors. Varenicline and bupropion may only be prescribed following advice from a trained smoking cessation advisor and patient review by GP or Trust prescribers. This must take into account any safety concerns in patients with psychiatric illness. The prescribing of varenicline or bupropion is outside the scope of this guideline For general information about varenicline and also information about psychiatric adverse effects see Oxford Health NHS FT varenicline medicines information bulletin Vol 10 No 2. NRT. Varenicline and bupropion should not be offered in any combination. AIM OF GUIDELINES 1. To act as a framework under which appropriately trained staff will operate the Trust Smoking
Cessation Initiative. This scheme involves training of appropriate healthcare staff to provide educational support and advice to patients motivated to stop or reduce smoking.
Inpatients wanting to stop smoking can approach or be referred to trained smoking cessation advisors and receive individually tailored smoking advice. This may involve the recommendation of specific treatment such as NRT and counselling about smoking
3
5
cessation. In the absence of a trained adviser, the named nurse should follow the guidance in appendix A for brief intervention advice. Smokers admitted to an in-patient unit may be provided with an appropriate form of NRT to alleviate craving/withdrawal after suitable assessment and completion of an appropriate care plan.
2. To provide guidance to staff offering nicotine replacement therapy to patients who are not motivated to stop smoking, but who are unable to leave the grounds to smoke.
OBJECTIVES The objectives of these guidelines are to encourage safe and effective use of NRT by Oxford Health NHS FT patients.
SMOKING CESSATION ADVISORS There are 3 levels of advisors. Level 1 advisors increase awareness of smoking cessation with patients and provide appropriate information about referral to level 2 advisors. All in-patient staff should have level 1 training Level 2 advisors provide smoking cessation treatment services. They offer 1:1 advice, motivation and support. The Specialist Stop Smoking Service can provide this training.
Advisors will meet criteria laid out in this guideline and will offer smoking cessation advice to patients within Oxford Health NHS FT
Advisors should undertake regular continuing professional development (CPD) for this role (at least yearly)
Level 3 advisors offer intensive support and advice for highly dependent smokers. There is a high focus on treatment with NRT in addition to varenicline and bupropion. Level 3 service is usually provided by the Clinical Commissioning Group (CCG) smoking cessation service
NICOTINE REPLACEMENT THERAPY
Inclusion criteria:
Patients who wish to quit smoking i.e. willing to set a quit date and to receive appropriate support through the guidance of a Smoking Cessation Advisor.
Patients admitted who are already prescribed NRT in the community and being offered behavioural support while on the ward.
Smokers who are unable to quit smoking abruptly with NRT but want to cut smoking frequency as a prelude to quitting (the ‘nicotine assisted reduction to stop [NARS] strategy).
Patients who do not wish to quit smoking but who are temporarily abstinent due to being unable to leave the Trust grounds to smoke, or those who are too physically unwell to smoke.
Exclusion criteria:
Patients with a previous serious reaction to NRT or any of the other ingredients contained in the products, e.g. glue in patch
Patches only – clients with chronic generalised skin disease such as psoriasis, chronic dermatitis and urticaria; clients who have had a previous reaction to transdermal patches; occasional smokers
Nasal sprays only – clients with chronic nasal disorders such as polyposis, vasomotor rhinitis and perennial rhinitis
4
5
Caution
Unstable cardiac disease, diabetes, hyperthyroidism, severe renal or hepatic impairment and peptic ulcer
Patients aged 12-18 years. Limited data in this age group indicates efficacy and no particular safety issues
Pregnant and breast-feeding women. If NRT is deemed necessary, the 24 hour patch should be avoided.
Drug Interactions Tobacco smoking induces the cytochrome P450 isoenzyme CPY1A2 so that the clearance of some drugs in smokers is increased and their half-life shortened. Smoking cessation may lead to raised levels of some medication and increased risk of adverse effects. This needs to be monitored, and medication dose reduced as necessary. It is the chemicals in the smoke that are responsible for this interaction, not the nicotine, so substituting smoking with nicotine replacement products has no impact on the interaction. Patients taking the following groups of drugs should be monitored for any signs of increased drug levels:
clozapine*, olanzapine, fluvoxamine, tricyclic antidepressants (e.g. clomipramine, imipramine, amitriptyline), benzodiazepines, haloperidol, zotepine, phenothiazines, mirtazepine, duloxetine, caffeine, zolpidem
Theophylline
Insulin+
Adrenergic agonists and antagonists
Flecainide, Tacrine, Tamoxifen, Propranolol, Pentazocine, Warfarin, Verapamil
Warfarin
Methadone
Refer to the following documents for more detailed information: Oxford Health NHS FT Medicines Information Bulletin Vol 13 No 3 “Smoking Cessation -
the Effects on Psychotropic Medication” UKMI Q&A 136 “Which medicines need adjustment when a patient stops smoking?”
*Clozapine toxicity may lead to seizures therefore quit attempts should be closely monitored and clozapine plasma measured to avoid toxicity. + Insulin requirements may change and any plans for smoking reduction should be made in consultation with the diabetic clinic
Counselling The patient should be counselled on how to use the specific product given (see table of NRT products) plus the general advice on:
Withdrawal symptoms
Possible changes in the body on stopping smoking e.g. weight gain, and how to manage these
The effects of smoking tobacco whilst using NRT – particularly in vulnerable groups, e.g. pregnant women, clients with cardiovascular disease
Written information on products supplied, self-help leaflets and where to obtain more information
5
0
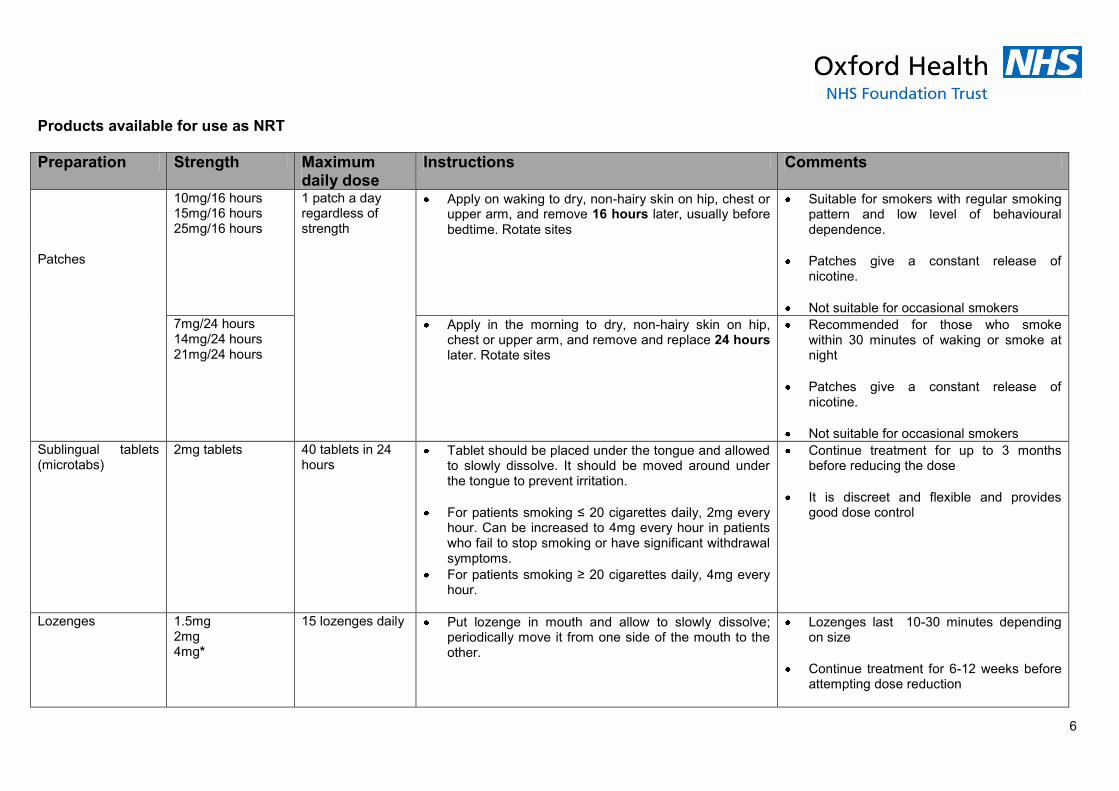
Products available for use as NRT
Preparation Strength Maximum daily dose
Instructions Comments
Patches
10mg/16 hours 15mg/16 hours 25mg/16 hours
1 patch a day regardless of strength
Apply on waking to dry, non-hairy skin on hip, chest or upper arm, and remove 16 hours later, usually before bedtime. Rotate sites
Suitable for smokers with regular smoking pattern and low level of behavioural dependence.
Patches give a constant release of nicotine.
Not suitable for occasional smokers
7mg/24 hours 14mg/24 hours 21mg/24 hours
Apply in the morning to dry, non-hairy skin on hip, chest or upper arm, and remove and replace 24 hours later. Rotate sites
Recommended for those who smoke within 30 minutes of waking or smoke at night
Patches give a constant release of nicotine.
Not suitable for occasional smokers
Sublingual tablets (microtabs)
2mg tablets 40 tablets in 24 hours
Tablet should be placed under the tongue and allowed to slowly dissolve. It should be moved around under the tongue to prevent irritation.
For patients smoking ≤ 20 cigarettes daily, 2mg every hour. Can be increased to 4mg every hour in patients who fail to stop smoking or have significant withdrawal symptoms.
For patients smoking ≥ 20 cigarettes daily, 4mg every hour.
Continue treatment for up to 3 months before reducing the dose
It is discreet and flexible and provides good dose control
Lozenges
1.5mg 2mg 4mg*
15 lozenges daily Put lozenge in mouth and allow to slowly dissolve; periodically move it from one side of the mouth to the other.
Lozenges last 10-30 minutes depending on size
Continue treatment for 6-12 weeks before attempting dose reduction
6
5
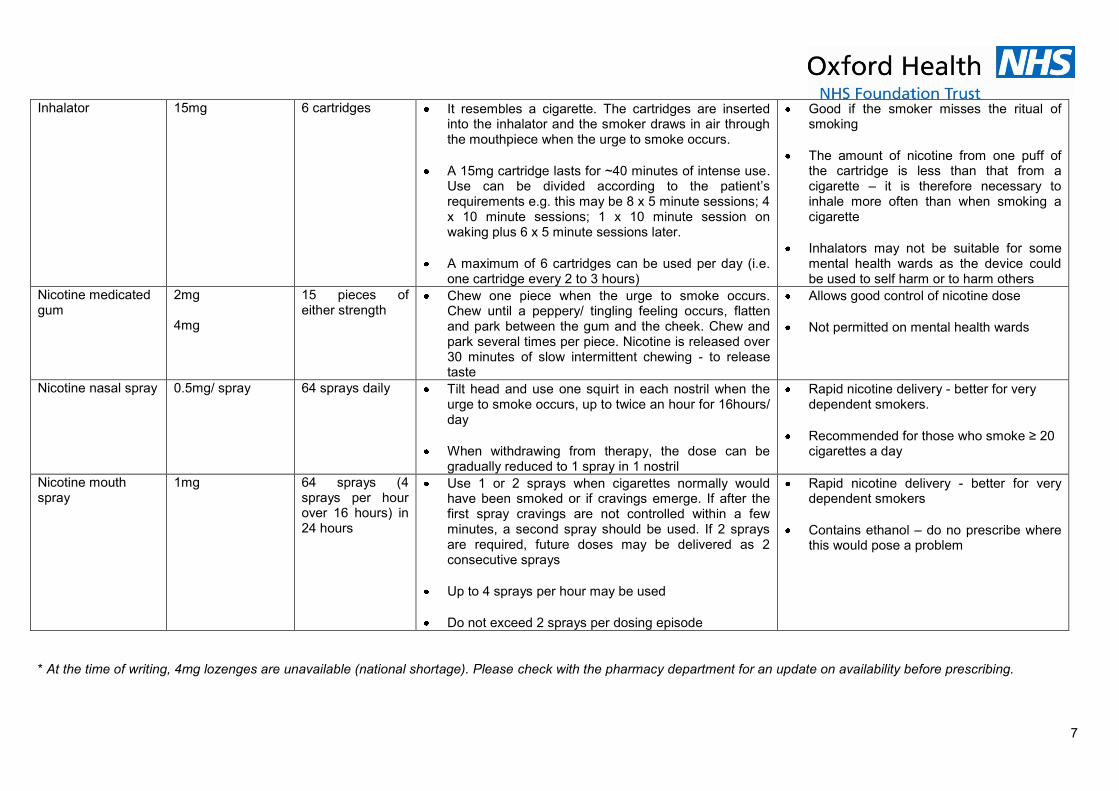
Inhalator 15mg 6 cartridges It resembles a cigarette. The cartridges are inserted into the inhalator and the smoker draws in air through the mouthpiece when the urge to smoke occurs.
A 15mg cartridge lasts for ~40 minutes of intense use. Use can be divided according to the patient’s requirements e.g. this may be 8 x 5 minute sessions; 4 x 10 minute sessions; 1 x 10 minute session on waking plus 6 x 5 minute sessions later.
A maximum of 6 cartridges can be used per day (i.e. one cartridge every 2 to 3 hours)
Good if the smoker misses the ritual of smoking
The amount of nicotine from one puff of the cartridge is less than that from a cigarette – it is therefore necessary to inhale more often than when smoking a cigarette
Inhalators may not be suitable for some mental health wards as the device could be used to self harm or to harm others
Nicotine medicated gum
2mg 4mg
15 pieces of either strength
Chew one piece when the urge to smoke occurs. Chew until a peppery/ tingling feeling occurs, flatten and park between the gum and the cheek. Chew and park several times per piece. Nicotine is released over 30 minutes of slow intermittent chewing - to release taste
Allows good control of nicotine dose
Not permitted on mental health wards
Nicotine nasal spray 0.5mg/ spray 64 sprays daily Tilt head and use one squirt in each nostril when the urge to smoke occurs, up to twice an hour for 16hours/ day
When withdrawing from therapy, the dose can be gradually reduced to 1 spray in 1 nostril
Rapid nicotine delivery - better for very dependent smokers.
Recommended for those who smoke ≥ 20 cigarettes a day
Nicotine mouth spray
1mg 64 sprays (4 sprays per hour over 16 hours) in 24 hours
Use 1 or 2 sprays when cigarettes normally would have been smoked or if cravings emerge. If after the first spray cravings are not controlled within a few minutes, a second spray should be used. If 2 sprays are required, future doses may be delivered as 2 consecutive sprays
Up to 4 sprays per hour may be used
Do not exceed 2 sprays per dosing episode
Rapid nicotine delivery - better for very dependent smokers
Contains ethanol – do no prescribe where this would pose a problem
* At the time of writing, 4mg lozenges are unavailable (national shortage). Please check with the pharmacy department for an update on availability before prescribing.
7

0
WHICH NICOTINE REPLACEMENT THERAPY PRODUCT?
Any product may be effective but take into account the following when selecting a suitable preparation:
o Quantity smoked o Level of dependence (highly dependent indicated by the need to smoke
within 30 minutes of waking) o Likelihood of missing physical sensation of smoking o Patient preference
Heavy smokers or those who are highly dependent may benefit from a 24 hour patch.
Patients likely to miss the physical sensation of smoking may benefit from an inhalator
A combination of two forms of NRT is often necessary e.g. a patch plus an inhaled, oral or nasal preparation
See table on previous pages for more details about available products
Dosages NRT dosages may depend on the number of cigarettes smoked per day. Use should normally be restricted to the licensed duration of the form of NRT used and be discontinued if the user restarts smoking. Side Effects The most common side effects are localised reactions & unlikely to lead to discontinuation e.g. Patches - skin irritation and sleep disturbances with patches Nasal spray - irritation of the nose, throat and eyes with nasal spray Oral preparations - If nausea, indigestion, hiccups occur it is possible that the product is not being used properly Withdrawal: Users should be encouraged to stop NRT usage within 3 months, but if it is necessary to use NRT beyond this time, they could do so if advised by a healthcare professional.
NRT ASSESSMENT AND SUPPLIES
Each ward/CMHT should have trained smoking cessation advisors to help support the smoking cessation programme. Where there is no-one that has had the appropriate training the named-nurse should follow guidance in Appendix A.
NRT can be prescribed by the patient’s medical team, non medical prescriber, GP or local Smoking Cessation Services and should be recorded in the medical notes
Oxford Health NHS FT allows a registered nurse to supply NRT products to newly admitted patients for a period of up to 24 hours
Inpatients wishing to quit/cut down smoking
1. For inpatients the named nurse/smoking advisor should complete a smoker’s questionnaire (Appendix B) with the patient if they plan to quit. This questionnaire identifies level of smoking and contraindications to NRT and guides NRT prescribing process
8

5
2. The patient will be assessed for suitability to receive NRT and, from their smoking history and preferences, appropriate NRT will be recommended
3. Any requests for named-patient NRT supplies should be accompanied by an Oxfordshire smoking advice service form completed by a trained advisor or evidence of smoking assessment e.g. questionnaire and ongoing support.
4. A stop date should be identified. In the case of nicotine assisted reduction - dates should be set for the planned reduction
5. The quit attempt should be monitored closely when the smoker is on psychotropic medication to assess any changes in psychotropic medication required, or if the smoker needs further help with withdrawal symptoms and urges to smoke
6. When NRT is recommended, the patient’s medical team will be asked to prescribe the relevant NRT product on the prescription chart.
7. If there is any doubt about the patient’s suitability to receive NRT, this should be discussed with the Stop Smoking Service, ward doctor or pharmacist attached to that team.
8. If NRT is supplied the advisor will counsel the patient on how to use it. Inpatients NOT wishing to quit smoking but who have to abstain due to the smoke-free environment First 24 hours of admission: OH NHSFT allows a registered nurse to supply NRT products to newly admitted patients for a period of up to 24 hours. Refer to the “enforced abstinence protocol for nursing staff” in appendix E. Within first 24 hours of admission: A doctor should review a patient’s NRT requirements and any effect that smoking abstinence may have on prescribed medication within 24 hours of admission (see section on interactions). The clinical management plan should be documented in the patient’s notes. It may be necessary to take into account a patient’s leave when selecting NRT e.g. patients having regular leave may be less suitable for NRT patches. Patients prescribed patches who have occasional leave should have the patch removed prior to going on leave if they intend to smoke. The choice of NRT should be risk assessed. A ward’s own policy should be referred to e.g. gum is not used on mental health wards and an individual risk assessment may also be necessary e.g. it may not be suitable for patients at risk of self harm or harm to others to be given inhalator devices. If it is appropriate for a patient to be in possession of a small supply of NRT (e.g. a pot of lozenges, or an inhalator device and a cartridge) this should be documented in their notes. NRT should be prescribed on the drug chart or NRT chart in appendix D. PRESCRIBING NRT Planned quit: The prescription for NRT for patients with a target stop date should be sufficient to last only until 2 weeks after the target date. Only patients who show commitment to smoking cessation or reduction should continue to receive NRT. For smokers who have been unsuccessful with a single form of NRT or show a high level of
dependence, consider offering a combination of nicotine patches and another form of NRT (such as gum, inhalator, lozenge or nasal spray). Enforced abstinence:
9
5
For patients who are abstaining, but not attempting to quit, the prescription can continue indefinitely during an inpatient admission. NRT should not be prescribed as a TTO. When abstinence is no longer necessary, NRT should be stopped, unless the patient requests support for smoking reduction or cessation.
HOW TO WRITE THE NRT PRESCRIPTION PATCHES:
Patches are written on the regular side of the drug chart. For 24 hour patches a new patch is put on at the same time the old one is removed. However, for 16 hour patches it is good
practice to indicate on the prescription when the patch should be removed, so that nursing staff can sign the chart when it is put on and also sign 16 hours later when it is taken off. PRNs (e.g. inhalator, lozenge, microtab etc) This should be prescribed on the PRN NRT chart in appendix D. It should be attached to the main drug chart with reference to it from the main chart.
CMHT
In Buckinghamshire staff should refer patients to the CCG Stop Smoking Services or refer to one of the local GP or Pharmacy clinics as advertised on their website
http://www.smokescape.org/support/support-centres-in-bucks/
In Oxfordshire smoking advisors with level 2 training can write to GPs asking them to prescribe the appropriate NRT preparation(s) or patients can be referred to the CCG Stop Smoking Services. http://www.smokefreeoxfordshire.nhs.uk/
In Wiltshire staff should refer patients to a stop smoking advisor at their local GP surgery, or they can ask at their local pharmacy or one of the stop smoking clinics advertised on their website: http://www.wiltshirestopsmoking.co.uk/
MANAGEMENT AND MONITORING OF NRT PRESCRIPTIONS for PLANNED QUIT
NRT prescribing-review will be determined by the advisor and will normally be as follows:
1 week after stopping [to avoid wastage of prescribing products which are unused]
If patients are successful in stopping smoking after week 4 (preferable with carbon monoxide validation, where this is available) treatment may be given for another four weeks before reassessment.
If the smoker continues to abstain from smoking at week 8 then a further four weeks treatment may be offered and NRT gradually withdrawn over the next 4 weeks unless there is a strong likelihood of relapse without continuing treatment.
NRT should be gradually withdrawn by 12 weeks unless there is a strong likelihood of relapse without continuing treatment.
If the smoker is unsuccessful in stopping then discontinue treatment and make a fresh start when they are ready again (NICE recommends waiting 6 months unless special circumstances have hampered the person’s initial attempt to stop smoking). Sometimes hospital admission may not be the easiest time for an individual to successfully stop smoking and this should be followed up post-discharge when it is less stressful.
10
5
On discharge from hospital an NRT supply will be given until the next review appointment is due. This should be arranged with the local CCG smoking cessation advisor (see contact details section)
DISCHARGE The GPs of all patients who have attempted to quit smoking whilst in hospital should be informed of their quit attempt and their use of NRT if necessary. CONTACT DETAILS The Local Stop Smoking Services can be contacted:
Oxfordshire Tel. 0845 40 80 300 email [email protected]
Bucks Tel. 0845 27 07 222 email [email protected]
Wiltshire Tel. 0300 0034562 email [email protected]
NHS Helpline Tel. 0800 022 4 332 http://smokefree.nhs.uk/
REFERENCES
1. NICE Public Health guidance No 48. November 2013 https://www.nice.org.uk/guidance/ph48
2. NICE Public Guidance 45. Tobacco: harm reduction approaches to smoking. June 2013 http://www.nice.org.uk/guidance/ph45
3. NICE Public Health guidance No 10. February 2008 http://www.nice.org.uk/guidance/ph10
4. NICE public health intervention guidance – brief interventions and referral for smoking cessation in primary care and other settings. March 2006 http://www.nice.org.uk/guidance/ph1
5. Health Development Agency; Smoking and patients with mental health problems. April 2004 http://www.gserve.nice.org.uk/nicemedia/documents/smoking_mentalhealth.pdf
6. White paper Choosing Health; making healthier choices easier (November 2004) http://webarchive.nationalarchives.gov.ukCQC.
7. Essential Standards of Quality and Safety. March 2010 http://www.cqc.org.uk/sites/default/files/documents/gac_-_dec_2011_update.pdf
8. NICE TA 123. Smoking Cessation- Vareniclene. July 2007. https://www.nice.org.uk/guidance/ta123
9. MHRA. Drug Safety Update Vol 2, Issue 4. Nov 2008 10. MHRA. Drug Safety Update Feb 2010, vol 3 issue 7: 6 11. DoH. Local Stop Smoking Services: Service Delivery and Monitoring Guidance 2011/12
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213755/dh_125939.pdf 12. BNF 68. September 2014 – March 2015; section 4.10.2 13. UKMI Q&A136.4 Which medicines need a dose adjustment when a patient stops smoking. August 2012.
11

5
APPENDIX A: SMOKING CESSATION ADVICE FOR NAMED NURSE
1. All smokers should be offered advice about the benefits of quitting and recommended to stop. This should be entered in the care plan.
2. People who are not ready to quit should be asked to consider the possibility and encouraged to seek help in the future.
3. Patients who are based in the community should be referred to the CCG Stop Smoking Services
4. In-patients should be referred to a trained Stop Smoking Advisor. If there are no trained smoking cessation personnel available the named nurse should carry out a smoking cessation questionnaire (Appendix B) and assess the patient’s smoking history and suitability for NRT.
5. The assessment should indicate any risk factors, and the smoking-dependence of the patient
6. The suitability of NRT should be reviewed with the relevant medical & pharmacy staff to see if there are any significant risk factors. The assessment can then be used to decide which product to prescribe following NRT product (details on pages 6&7) and flow chart (page 8)
7. For inpatients a nicotine replacement therapy (NRT) prescription chart (appendix D) may be attached to the main drug chart and an entry made in the ‘prn’ section of the latter as indicated.
8. If NRT is accepted, it should be offered immediately [NICE 2014] 9. Brief interventions and group behaviour therapy should be offered as appropriate to each
‘quitter’. 10. The smoking status of those who are not ready to stop should be recorded and reviewed
with the individual once a year, where possible 11. The smoking status of successful quitters needs to be updated on patient records
NB Attention should be given to monitoring weight gain as sometimes smoking cessation may lead to increased carbohydrate intake and weight issues. Health eating and exercise should be encouraged.
12
5
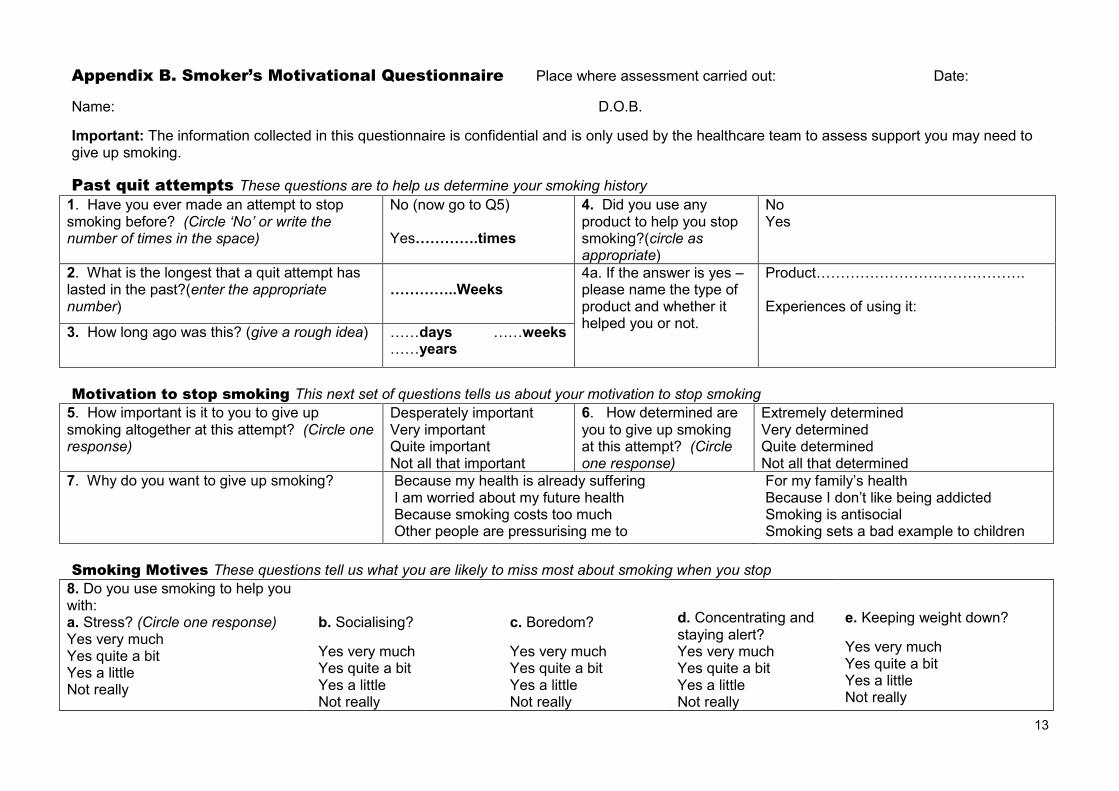
Appendix B. Smoker’s Motivational Questionnaire Place where assessment carried out: Date:
Name: D.O.B.
Important: The information collected in this questionnaire is confidential and is only used by the healthcare team to assess support you may need to give up smoking.
Past quit attempts These questions are to help us determine your smoking history
1. Have you ever made an attempt to stop smoking before? (Circle ‘No’ or write the number of times in the space)
No (now go to Q5) Yes………….times
4. Did you use any product to help you stop smoking?(circle as appropriate)
No Yes
2. What is the longest that a quit attempt has lasted in the past?(enter the appropriate number)
…………..Weeks
4a. If the answer is yes – please name the type of product and whether it helped you or not.
Product……………………………………. Experiences of using it:
3. How long ago was this? (give a rough idea) ……days ……weeks ……years
Motivation to stop smoking This next set of questions tells us about your motivation to stop smoking
5. How important is it to you to give up smoking altogether at this attempt? (Circle one response)
Desperately important Very important Quite important Not all that important
6. How determined are you to give up smoking at this attempt? (Circle one response)
Extremely determined Very determined Quite determined Not all that determined
7. Why do you want to give up smoking? Because my health is already suffering I am worried about my future health Because smoking costs too much Other people are pressurising me to
For my family’s health Because I don’t like being addicted Smoking is antisocial Smoking sets a bad example to children
Smoking Motives These questions tell us what you are likely to miss most about smoking when you stop
8. Do you use smoking to help you with: a. Stress? (Circle one response) Yes very much Yes quite a bit Yes a little Not really
b. Socialising?
Yes very much Yes quite a bit Yes a little Not really
c. Boredom?
Yes very much Yes quite a bit Yes a little Not really
d. Concentrating and staying alert? Yes very much Yes quite a bit Yes a little Not really
e. Keeping weight down?
Yes very much Yes quite a bit Yes a little Not really
13
5
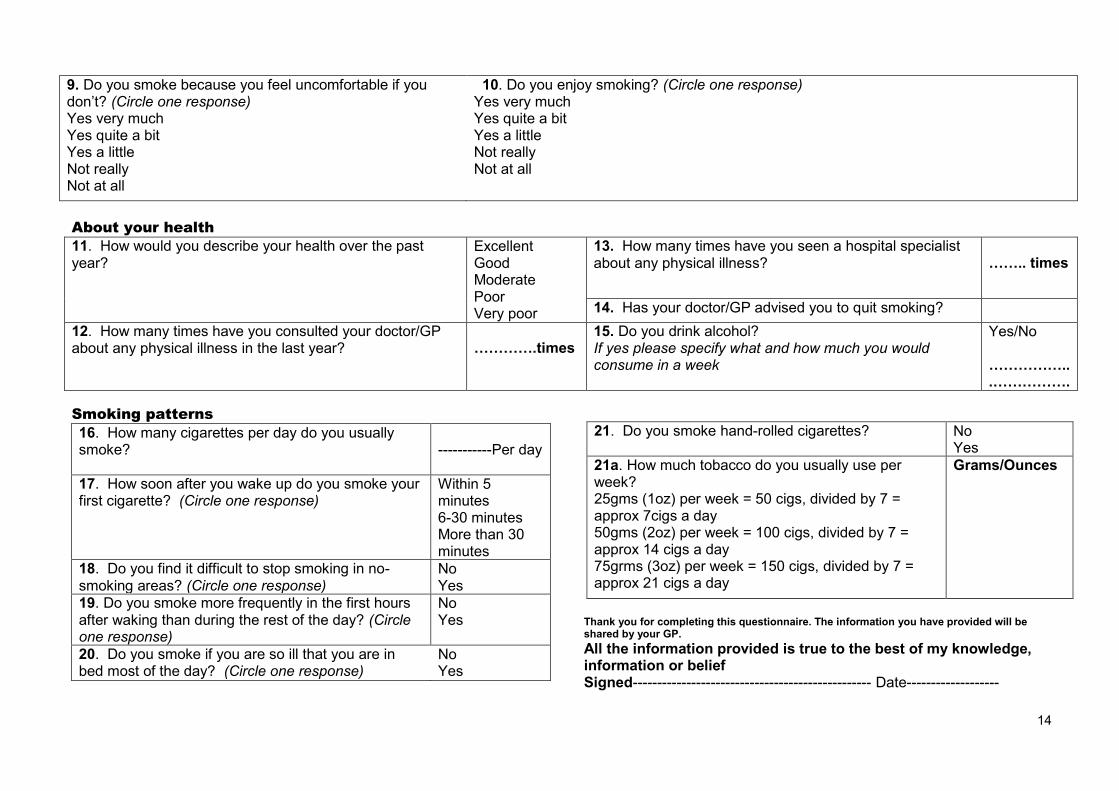
9. Do you smoke because you feel uncomfortable if you don’t? (Circle one response) Yes very much Yes quite a bit Yes a little Not really Not at all
10. Do you enjoy smoking? (Circle one response) Yes very much Yes quite a bit Yes a little Not really Not at all
About your health
11. How would you describe your health over the past year?
Excellent Good Moderate Poor Very poor
13. How many times have you seen a hospital specialist about any physical illness?
…….. times
14. Has your doctor/GP advised you to quit smoking?
12. How many times have you consulted your doctor/GP about any physical illness in the last year?
………….times
15. Do you drink alcohol? If yes please specify what and how much you would consume in a week
Yes/No ……………...…………….
Smoking patterns
16. How many cigarettes per day do you usually smoke?
-----------Per day
17. How soon after you wake up do you smoke your first cigarette? (Circle one response)
Within 5 minutes 6-30 minutes More than 30 minutes
18. Do you find it difficult to stop smoking in no-smoking areas? (Circle one response)
No Yes
19. Do you smoke more frequently in the first hours after waking than during the rest of the day? (Circle one response)
No Yes
20. Do you smoke if you are so ill that you are in bed most of the day? (Circle one response)
No Yes
Thank you for completing this questionnaire. The information you have provided will be shared by your GP.
All the information provided is true to the best of my knowledge, information or belief Signed------------------------------------------------- Date-------------------
21. Do you smoke hand-rolled cigarettes?
No Yes
21a. How much tobacco do you usually use per week? 25gms (1oz) per week = 50 cigs, divided by 7 = approx 7cigs a day 50gms (2oz) per week = 100 cigs, divided by 7 = approx 14 cigs a day 75grms (3oz) per week = 150 cigs, divided by 7 = approx 21 cigs a day
Grams/Ounces
14
5
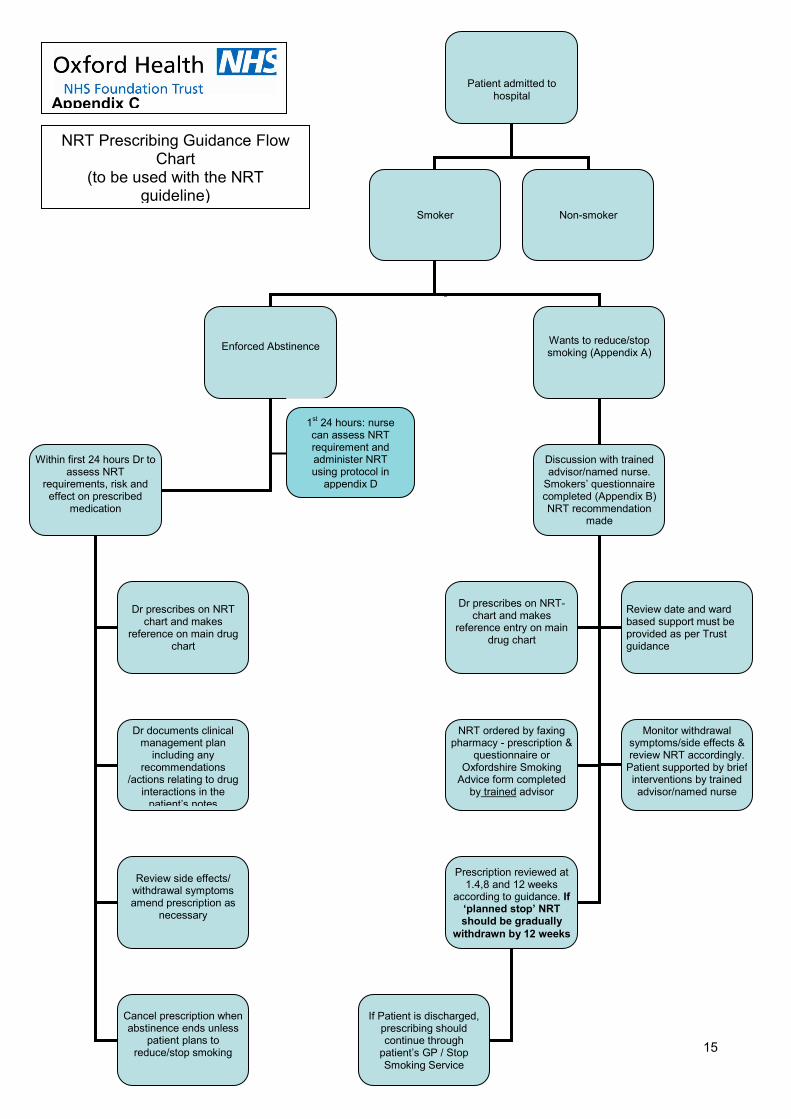
Patient admitted to hospital
Smoker Non-smoker
Enforced Abstinence
Does not want to give up smoking
Wants to reduce/stop smoking (Appendix A)
Within first 24 hours Dr to assess NRT
requirements, risk and effect on prescribed
medication
No Further action. Consider providing
literature/ details of PCT Stop Smoking Service.
Review smoking status at later date/post discharge
Dr prescribes on NRT chart and makes
reference on main drug chart
Dr documents clinical management plan
including any recommendations
/actions relating to drug interactions in the
patient’s notes
Review side effects/ withdrawal symptoms amend prescription as
necessary
Cancel prescription when abstinence ends unless
patient plans to reduce/stop smoking
Discussion with trained advisor/named nurse.
Smokers’ questionnaire completed (Appendix B) NRT recommendation
made
Dr prescribes on NRT-chart and makes
reference entry on main drug chart
Review date and ward based support must be provided as per Trust guidance
NRT ordered by faxing pharmacy - prescription &
questionnaire or Oxfordshire Smoking
Advice form completed by trained advisor
Monitor withdrawal symptoms/side effects & review NRT accordingly.
Patient supported by brief interventions by trained advisor/named nurse
Appendix C
NRT Prescribing Guidance Flow Chart
(to be used with the NRT guideline)
Prescription reviewed at 1.4,8 and 12 weeks
according to guidance. If ‘planned stop’ NRT should be gradually
withdrawn by 12 weeks
If Patient is discharged, prescribing should continue through
patient’s GP / Stop Smoking Service
1st 24 hours: nurse
can assess NRT requirement and administer NRT using protocol in
appendix D
15
5
10
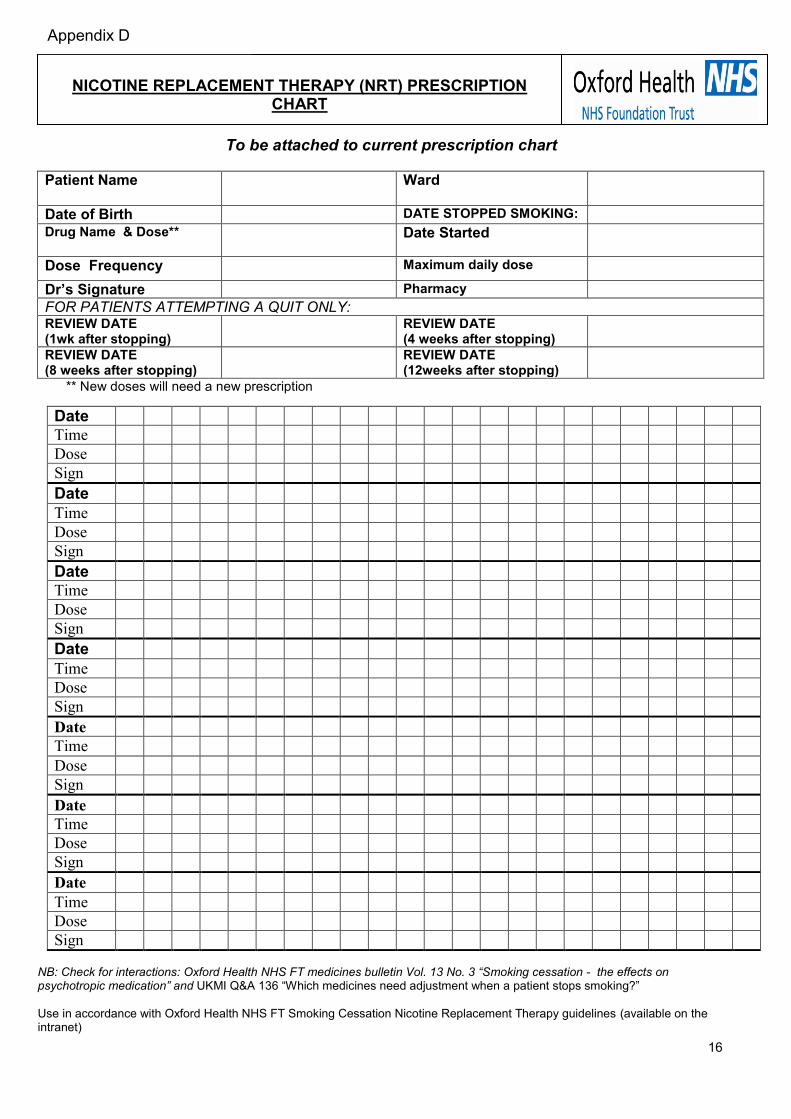
To be attached to current prescription chart
Patient Name
Ward
Date of Birth DATE STOPPED SMOKING: Drug Name & Dose**
Date Started
Dose Frequency Maximum daily dose
Dr’s Signature Pharmacy
FOR PATIENTS ATTEMPTING A QUIT ONLY: REVIEW DATE (1wk after stopping)
REVIEW DATE (4 weeks after stopping)
REVIEW DATE (8 weeks after stopping)
REVIEW DATE (12weeks after stopping)
** New doses will need a new prescription
Date
Time
Dose
Sign
Date
Time
Dose
Sign
Date
Time
Dose
Sign
Date
Time
Dose
Sign
Date
Time
Dose
Sign
Date
Time
Dose
Sign
Date
Time
Dose
Sign
NB: Check for interactions: Oxford Health NHS FT medicines bulletin Vol. 13 No. 3 “Smoking cessation - the effects on psychotropic medication” and UKMI Q&A 136 “Which medicines need adjustment when a patient stops smoking?”
Use in accordance with Oxford Health NHS FT Smoking Cessation Nicotine Replacement Therapy guidelines (available on the intranet)
NICOTINE REPLACEMENT THERAPY (NRT) PRESCRIPTION CHART
Appendix D
16
5
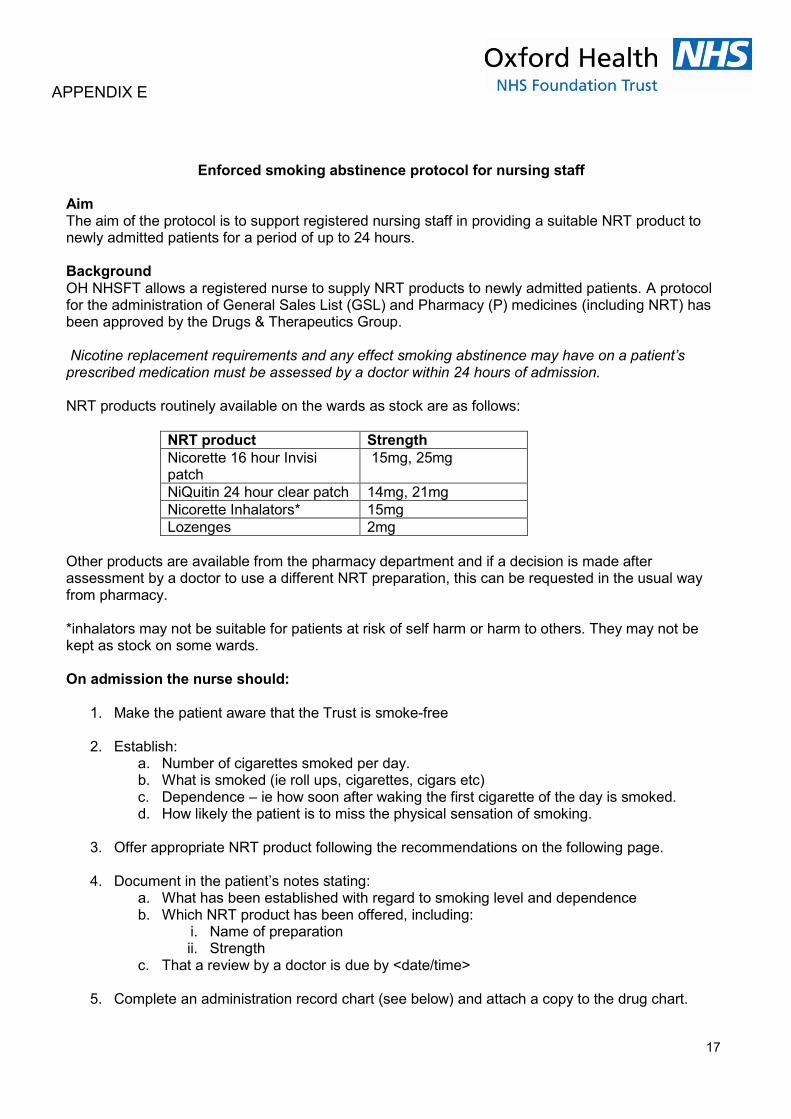
Enforced smoking abstinence protocol for nursing staff
Aim The aim of the protocol is to support registered nursing staff in providing a suitable NRT product to newly admitted patients for a period of up to 24 hours. Background OH NHSFT allows a registered nurse to supply NRT products to newly admitted patients. A protocol for the administration of General Sales List (GSL) and Pharmacy (P) medicines (including NRT) has been approved by the Drugs & Therapeutics Group. Nicotine replacement requirements and any effect smoking abstinence may have on a patient’s prescribed medication must be assessed by a doctor within 24 hours of admission. NRT products routinely available on the wards as stock are as follows:
NRT product Strength
Nicorette 16 hour Invisi patch
15mg, 25mg
NiQuitin 24 hour clear patch 14mg, 21mg
Nicorette Inhalators* 15mg
Lozenges 2mg
Other products are available from the pharmacy department and if a decision is made after assessment by a doctor to use a different NRT preparation, this can be requested in the usual way from pharmacy. *inhalators may not be suitable for patients at risk of self harm or harm to others. They may not be kept as stock on some wards. On admission the nurse should:
1. Make the patient aware that the Trust is smoke-free
2. Establish: a. Number of cigarettes smoked per day. b. What is smoked (ie roll ups, cigarettes, cigars etc) c. Dependence – ie how soon after waking the first cigarette of the day is smoked. d. How likely the patient is to miss the physical sensation of smoking.
3. Offer appropriate NRT product following the recommendations on the following page.
4. Document in the patient’s notes stating:
a. What has been established with regard to smoking level and dependence b. Which NRT product has been offered, including:
i. Name of preparation ii. Strength
c. That a review by a doctor is due by <date/time>
5. Complete an administration record chart (see below) and attach a copy to the drug chart.
APPENDIX E
17
5
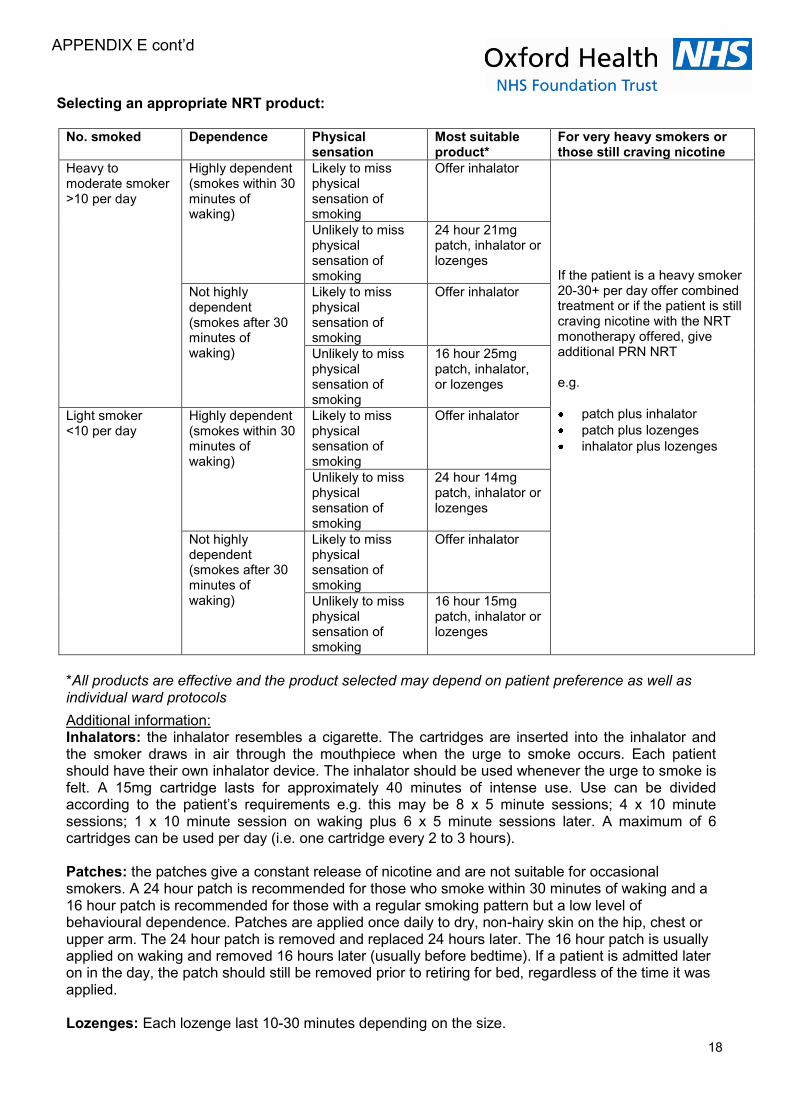
Selecting an appropriate NRT product: No. smoked Dependence Physical
sensation Most suitable product*
For very heavy smokers or those still craving nicotine
Heavy to moderate smoker >10 per day
Highly dependent (smokes within 30 minutes of waking)
Likely to miss physical sensation of smoking
Offer inhalator If the patient is a heavy smoker 20-30+ per day offer combined treatment or if the patient is still craving nicotine with the NRT monotherapy offered, give additional PRN NRT e.g.
patch plus inhalator
patch plus lozenges
inhalator plus lozenges
Unlikely to miss physical sensation of smoking
24 hour 21mg patch, inhalator or lozenges
Not highly dependent (smokes after 30 minutes of waking)
Likely to miss physical sensation of smoking
Offer inhalator
Unlikely to miss physical sensation of smoking
16 hour 25mg patch, inhalator, or lozenges
Light smoker <10 per day
Highly dependent (smokes within 30 minutes of waking)
Likely to miss physical sensation of smoking
Offer inhalator
Unlikely to miss physical sensation of smoking
24 hour 14mg patch, inhalator or lozenges
Not highly dependent (smokes after 30 minutes of waking)
Likely to miss physical sensation of smoking
Offer inhalator
Unlikely to miss physical sensation of smoking
16 hour 15mg patch, inhalator or lozenges
*All products are effective and the product selected may depend on patient preference as well as individual ward protocols
Additional information: Inhalators: the inhalator resembles a cigarette. The cartridges are inserted into the inhalator and the smoker draws in air through the mouthpiece when the urge to smoke occurs. Each patient should have their own inhalator device. The inhalator should be used whenever the urge to smoke is felt. A 15mg cartridge lasts for approximately 40 minutes of intense use. Use can be divided according to the patient’s requirements e.g. this may be 8 x 5 minute sessions; 4 x 10 minute sessions; 1 x 10 minute session on waking plus 6 x 5 minute sessions later. A maximum of 6 cartridges can be used per day (i.e. one cartridge every 2 to 3 hours). Patches: the patches give a constant release of nicotine and are not suitable for occasional smokers. A 24 hour patch is recommended for those who smoke within 30 minutes of waking and a 16 hour patch is recommended for those with a regular smoking pattern but a low level of behavioural dependence. Patches are applied once daily to dry, non-hairy skin on the hip, chest or upper arm. The 24 hour patch is removed and replaced 24 hours later. The 16 hour patch is usually applied on waking and removed 16 hours later (usually before bedtime). If a patient is admitted later on in the day, the patch should still be removed prior to retiring for bed, regardless of the time it was applied. Lozenges: Each lozenge last 10-30 minutes depending on the size.
APPENDIX E cont’d
18
5
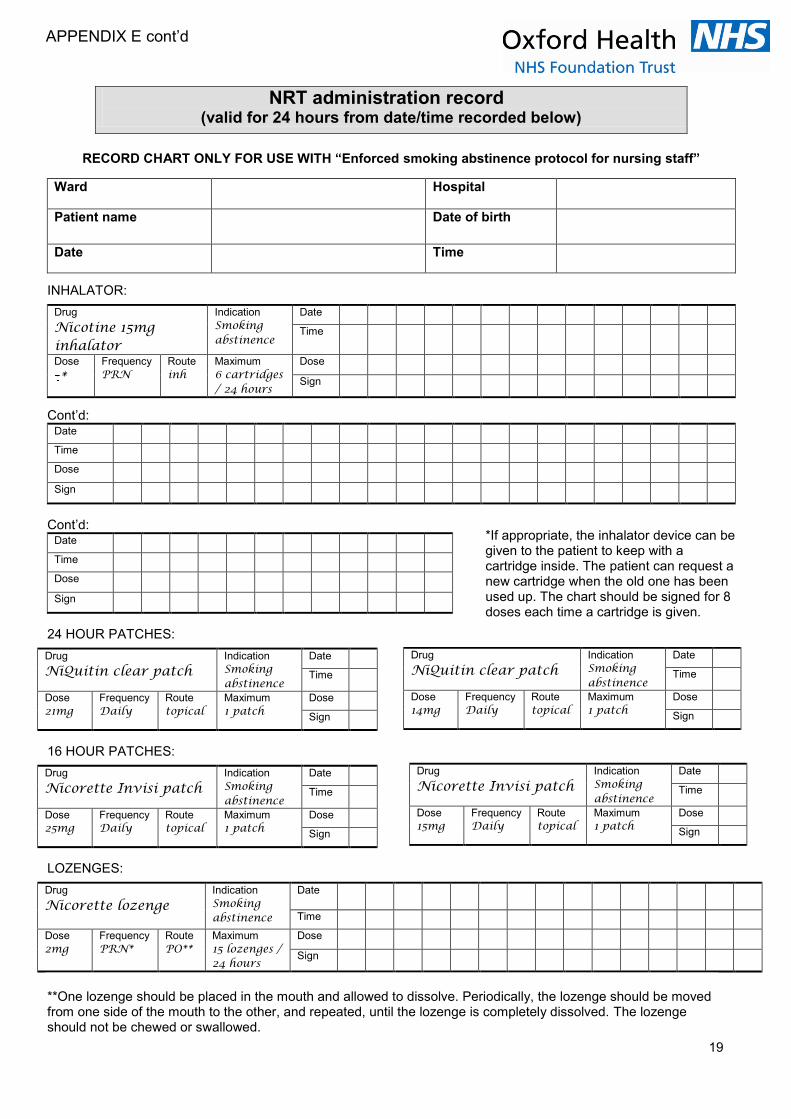
RECORD CHART ONLY FOR USE WITH “Enforced smoking abstinence protocol for nursing staff”
Ward Hospital
Patient name Date of birth
Date Time
INHALATOR:
Drug
Nicotine 15mg inhalator
Indication
Smoking abstinence
Date
Time
Dose
* Frequency
PRN Route
inh Maximum
6 cartridges / 24 hours
Dose Sign
Cont’d: Date
Time
Dose Sign
Cont’d: Date
Time
Dose Sign
24 HOUR PATCHES:
Drug
NiQuitin clear patch Indication
Smoking abstinence
Date
Time
Dose
21mg Frequency
Daily Route
topical Maximum
1 patch Dose
Sign
16 HOUR PATCHES:
Drug
Nicorette Invisi patch Indication
Smoking abstinence
Date
Time
Dose
25mg Frequency
Daily Route
topical Maximum
1 patch Dose
Sign
LOZENGES:
Drug
Nicorette lozenge Indication
Smoking abstinence
Date
Time
Dose
2mg Frequency
PRN* Route
PO** Maximum
15 lozenges / 24 hours
Dose Sign
**One lozenge should be placed in the mouth and allowed to dissolve. Periodically, the lozenge should be moved from one side of the mouth to the other, and repeated, until the lozenge is completely dissolved. The lozenge should not be chewed or swallowed.
NRT administration record (valid for 24 hours from date/time recorded below)
Drug
NiQuitin clear patch Indication
Smoking abstinence
Date
Time
Dose
14mg Frequency
Daily Route
topical Maximum
1 patch Dose
Sign
Drug
Nicorette Invisi patch Indication
Smoking abstinence
Date
Time
Dose
15mg Frequency
Daily Route
topical Maximum
1 patch Dose
Sign
*If appropriate, the inhalator device can be given to the patient to keep with a cartridge inside. The patient can request a new cartridge when the old one has been used up. The chart should be signed for 8 doses each time a cartridge is given.
APPENDIX E cont’d
19







![Oxford Health NHS Foundation Trust€¦ · Web view2017/04/26 · Meeting of the Oxford Health NHS Foundation Trust Board of Directors [DRAFT] Minutes of a meeting held on 26 April](https://img.pdfslide.us/doc/110x75/5f28ed3873da546efe3b3cb4/oxford-health-nhs-foundation-trust-web-view-20170426-meeting-of-the-oxford.jpg)





















