Embed Size (px)
Citation preview

SPECIAL ARTICLE
Overweight and obesity: Pharmacotherapeutic considerationsNancy Balkon, PhD, ANP-C, NPP, FAANP (Clinical Associate Professor)1, Craig Balkon, PharmD, RPh(Pharmacist)2, & Bruce S. Zitkus, EdD, ANP-BC, FNP-BC, CDE (Clinical Associate Professor)1
1 Stony Brook University School of Nursing, Stony Brook, New York2 Rite Aid Corporation
KeywordsObesity; pharmacology; pharmacotherapy;
weight management.
CorrespondenceNancy Balkon, PhD, ANP-C, NPP, FAANP, Stony
Brook University School of Nursing, Level 2,
Health Sciences Center, Stony Brook, NY
11794-8240.
Tel: 631-444-3270;
Fax: 631-444-3136;
E-mail: [email protected]
Received: November 2010;
accepted: November 2010
doi: 10.1111/j.1745-7599.2010.00587.x
DisclosureThe authors report no competing interests.
Abstract
Purpose: This article reviews current trends for using pharmacotherapy incombination with other weight loss modalities and offers points for considera-tion by clinicians in practice.Data sources: Selected evidence-based articles and government websites.Conclusions: Pharmacotherapy as a strategy for managing overweight, obese,and extremely obese individuals remains controversial. Risk versus benefit andoverall safety of prescription drugs for weight loss management remains a pri-mary focus for consideration among clinicians and a viable topic for evidence-based outcomes research.Implications for practice: Overweight and obesity are well accepted as crit-ical risk factors and predictors of morbidity and mortality in individuals of allages from childhood to senescence. In the United States, overweight and obe-sity exist in epidemic proportions. It is critical that primary care providers beknowledgeable about pharmacologic factors related to obesity.
Overweight and obesity are well accepted as critical riskfactors and predictors of morbidity and mortality in in-dividuals of all ages from childhood to senescence. Inthe United States, overweight and obesity exist in epi-demic proportions (Sherry et al., 2010). In this eraof health policy that defines and implements strategiesto promote health and prevent disease or its progres-sion, overweight and obesity are primary concerns. Asphysical findings identified during health assessment,overweight and obesity deserve the close attention ofclinicians as they make diagnoses, consider actual andpotential co-morbidities, and select interventions to op-timize therapeutic outcomes.
Overweight and obesity
Interpretation of data collected during physical exam-ination allows the clinician to move forward in clinicalreasoning and decision making to formulate a plan ofcare that is best suited for each individual as a uniqueentity. These data are interpreted against what is consid-ered “normal” for the data set. Established parameters ex-ist for determining whether one is of normal weight or
deviates to below normal or above normal. The standarddata points of height and weight are supplemented withadditional data, such as body mass index (BMI), waist cir-cumference, skin fold thickness, fluid intake versus out-put determination, and other laboratory findings, in aneffort to improve accuracy of diagnosis and underlyingfactors contributing to an individual’s weight. These pa-rameters are useful in determining deviations above andbelow normal body weight. The first three parametersmentioned are suited for evaluation of fat-related weightchanges, while fluid balance and others are suited to eval-uate weight changes associated with other causes like re-sponse to illness.
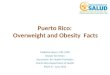
BMI has become the “gold standard” for weight as-sessment when one is concerned with assessing changesin body fat content above and below what is typicallyconsidered normal (Figure 1). Measuring waist circum-ference provides additional morbidity and mortality dataespecially for cardiac and diabetes-related disease statesbecause they are associated with a high prevalence of corebody fat, which translates to increased abdominal girth(Figure 2). Skin fold thickness assessment has diminishedin popularity.
61Journal of the American Academy of Nurse Practitioners 23 (2011) 61–66 C©2011 The Author(s)Journal compilation C©2011 American Academy of Nurse Practitioners
Overweight and obesity N. Balkon et al.
Extreme obesity (Class III) >/= 40
Obesity (Class II) 35.0-39.9
Overweight (Class I) 30.0-34.9
Normal 18.5-24.9
Underweight <18.5
Anorexia nervosa </=17.5
Note: BMI = Weight (kg)/Height (meters) = kg/m2
Figure 1 Body mass index (BMI).
Fat-related weight gain develops from exogenous andendogenous causes. Exogenous weight gain occurs froman imbalance between calories ingested and caloriesneeded to maintain normal weight due to overeating oras an expected but undesirable side effect of prescribedpharmacotherapy. Overeating is managed solely by dietmodification. Management of weight gain associated withpharmacotherapy is a unique challenge for clinicians.Close monitoring during therapy with modifications asneeded is essential for individuals receiving antidiabetictherapy, certain antiseizure/mood stabilizing drugs, andcertain atypical antipsychotics. With endogenous weightgain, there is a recognized underlying metabolic alter-ation associated with the disease state, for example, di-abetes mellitus. Optimal weight is achieved and main-tained in this case by managing the causative conditionin combination with diet modification.
Pharmacologic considerations
Pharmaceuticals, prescribed and over-the-counter(OTC), are used in weight management for promotingweight loss or weight gain and as supplements to ensuremaintenance of adequate nutrient, vitamin, and mineralbalance to meet an individual’s established nutritionalrequirements. That is, individuals at both ends of theweight continuum, the overweight and the underweight,may benefit from pharmaceutical intervention when it isindicated and used appropriately.
The BMI categories of overweight (Class I), obese (ClassII), and extremely obese (Class III) pose significant chal-lenges for the clinician. Weight management algorithmstypically focus on diet, controlled weight loss, exercise,
Male > 40 inches (102 cm)
Female > 35 inches (88 cm)
Figure 2 Waist circumference (obesity).
and behavioral modification as first-line interventions forall three categories.
Prescribed pharmacotherapy is certainly considered forindividuals whose weight gain falls into obese and ex-tremely obese categories. Those who are identified asoverweight (Class I) typically respond to the first-line in-terventions of diet, controlled weight loss, and behavioralmodification. Whenever a prescribed pharmacotherapeu-tic regimen is considered for use within this patient popu-lation it must be with careful consideration of risk versusbenefit. Increased body weight beyond what is consid-ered normal alters the body’s response to the drug. Po-tential changes in pharmacokinetics (absorption, distri-bution, metabolism, excretion) and pharmacodynamics(the effect of the drug) must be considered and plannedfor. A more detailed discussion is outside the scope of thisarticle.
There is reluctance to add pharmaceuticals to treat-ment regimens for weight loss until an individual’s re-sponse to first-line interventions have been evaluatedand deemed unsuccessful following an adequate trialperiod, typically reported as 6 months. Continued ac-tive debate surrounds the risk/benefit of pharmaceuti-cal use for weight loss since undesirable effects associ-ated with certain drugs and drug categories exist. Thereis no doubt that potential risks of pharmaceutical in-tervention must be weighed against the benefits. Forexample, fenfluramine-phentermine (fen-phen), dexfen-fluramine (Redux), and, more recently, sibutramine(Meridia) are no longer prescribed in the United Statesby recommendation of the Food and Drug Administra-tion (FDA). Fenfluramine-phentermine and dexfenflu-ramine were voluntarily withdrawn from market in 1997because of increased risk for cardiac valvular disease(FDA, 2010a). Phentermine (Aciphex), a related drug, re-mains available. Sibutramine (Meridia), a noradrenergic/serotonergic agent, was voluntarily withdrawn from U.S.and Canadian markets in October 2010. Data from a post-marketing study, the Sibutramine Cardiovascular Out-comes (SCOUT) Trial, prompted the withdrawal of sibu-tramine (Meridia; FDA, 2010b). Of most concern was thatindividuals with cardiovascular disease were shown tohave increased risk of heart attack and stroke with thisdrug (Clinicaltrials.gov, 2010; FDA, 2010b; James et al.,2010).
An individual’s progression along the weight contin-uum, from overweight (Class I) to obese (Class II) to ex-tremely obese (Class III), correlates with increased healthrisk and potential development of life-threatening com-plications. Overweight is a health risk and the first iden-tified on the increased body weight continuum. It is of-ten associated with inactivity, alterations in lipid profile,and changes in carbohydrate metabolism if it persists over
62
N. Balkon et al. Overweight and obesity
1. Pre-Therapy AssessmentA. Perform detailed history and physical B. Obtain detailed medication history: C. Identify existing or previous medical history for conditions that require cautious
prescribing or contraindicate the use of a drug; specifically: allergy to drug or drug family, patient age, medical history, pregnancy, lactation
2. Appropiate medication selection (medication, dose, route, frequency)
3. Surveillance During TherapyA. Always monitor the dose being administered.
- Rationale: Insure that dose is within acceptable limits for the diagnosis and patient being treated.
B. Compare current status with previous status to detect improvements or deterioration in patient's condition. These include weight, BMI, waist circumference, and other anthropometric measures.Comparisions of self-reported intake and exercise should also be performed
C. Monitor for therapeutic drug effect(s). D. Monitor for adverse effects, toxicity, interactions E. Monitor for hypersensitivity reactions which might require drug's discontiuation. F. Order, monitor, and interpret diagnostic tests that assist in assessment of
therapeutic response. G. Monitor for actual and/or potential interactions:
- drug-drug - drug-nutrient - drug-laboratory test
4. Education: (Patient/Significant Other) Instruct about:
A. drug action B. indications for use C. dose, frequency and route of administration D. adverse effects (expected and undesirable) E. guidelines for dose adjustment F. appropriate action to take if adverse effects occur:
1. how to manage symptoms of expected adverse effects. 2. when to notify practitioner/prescriber. 3. under which conditions to hold/omit dose before notifying
practitioner/prescriber. 4. under which conditions to seek immediate medical attention.
G. importance of completing the full course of therapy as prescribed; i.e., don't discontinue drug once signs and symptoms have
subsided. H. consequences of not taking or abruptly discontinuing a prescribed
drug.I. that drug is to be taken only in the manner and for the condition for
which it is prescribed. J. that all medications are to be kept out of reach of children
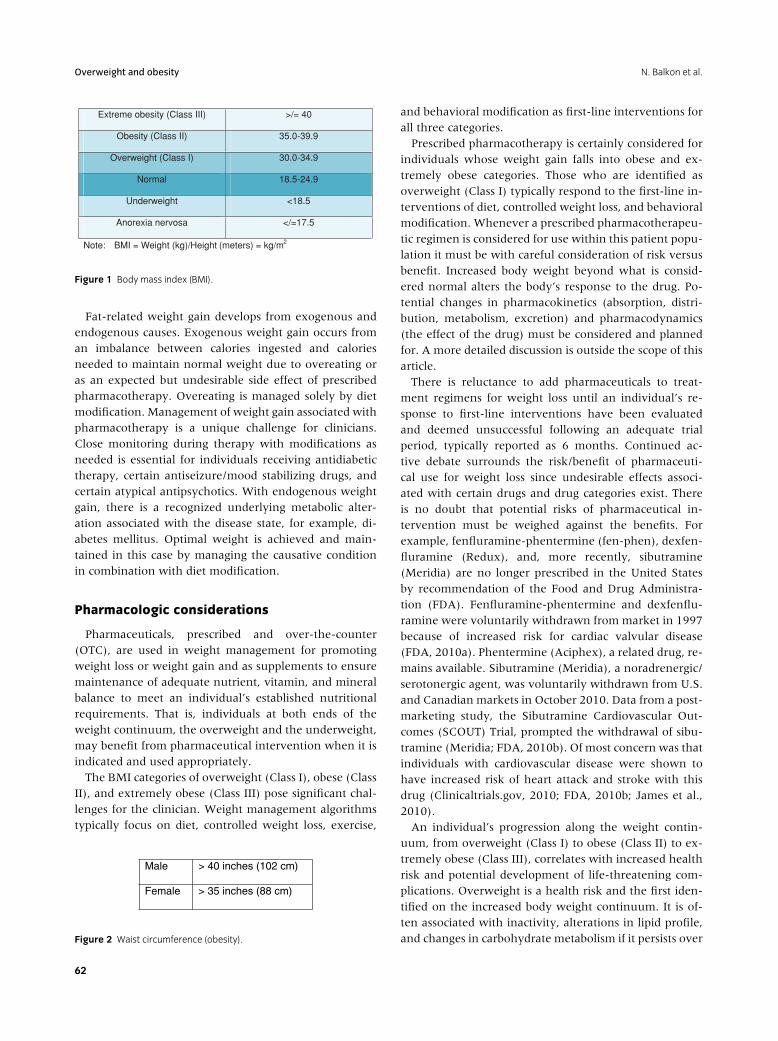
Figure 3 Components of pharmacotherapeutic management. Data from Malseed, R.T., Goldstein, F.J., and Balkon, N.B. (1994). Pharmacology: Drug
therapy and nursing considerations. Philadelphia: J.B. Lippincott. pp. 3–11.
time. While there are multiple etiologies for medical diag-noses like hypertension, hyperlipidemia, type 2 diabetesmellitus, and osteoarthritis, overweight is a common co-existing (comorbid) condition. As overweight progressesto obesity and extreme obesity, consequences of long-standing hypertension, hyperlipidemia, and changes incarbohydrate metabolism may also progress and expressthemselves as coronary artery disease, stroke, type 1 dia-betes mellitus, metabolic syndrome, and a cadre of phys-ical and end-organ changes that put individuals at risk
for chronic debilitating illness or death. For these reasons,weight management is a public health and public policyissue for health promotion, disease prevention, and keep-ing down healthcare costs.
Pharmacotherapeutic management strategy
Pretherapy assessment, appropriate medication selec-tion, surveillance during therapy, and education arecomponents of safe and effective pharmacotherapeutic
63

Overweight and obesity N. Balkon et al.
management and prescribing (Figure 3; Malseed, Gold-stein, & Balkon, 1994). Individuals who are overweighthave multiple health problems, medical comorbidities,and often complex medication histories, and thereforepose unique pharmacotherapeutic challenges.
Prescribed and OTC medications, herbal/natural prod-ucts, food supplements, vitamins, and minerals are allused in weight management protocols. They all havepharmacotherapeutic properties; however, while herbaland food supplements often have pharmacologic activity,their efficacy cannot be assumed to be equivalent to thatreported for FDA-approved compounds because theirmanufacture and labeling are not regulated by the FDA.
Pharmacotherapeutic categories
Identification of physiologic and biochemical mecha-nisms that stimulate weight gain have led to selectionof drugs from certain drug categories to facilitate weightloss. What has resulted over time is selection of agentsfor short-term and long-term use. Formulations approvedby the FDA include noradrenergic agents as appetitesuppressants and the lipase inhibitor orlistat, which isavailable in prescribed and OTC forms (Xenical and Alli,respectively). Sibutramine (Meridia) was the only nora-drenergic/serotonergic agent and is no longer available.Compounds with serotonergic activity (SSRI antidepres-sants) and stimulants such as caffeine and ephedrine arebeing studied and used off-label (i.e., no FDA indicationfor weight loss). Leptin and other endogenous peptidesare also being researched for efficacy in weight man-agement. Botanicals (herbals) and nutraceuticals are alsoused by some to stimulate weight loss but safety and effi-cacy of these agents have not been documented.
Achieving the desired therapeutic outcome of weightloss is closely linked to clearly defining factors that con-tribute to weight gain for each individual. Regardingpharmacotherapy and weight loss, identifying underlyingfactors that contribute to an individual’s weight gain willfacilitate the selection of the most appropriate pharmaco-logic agent or agents. For example, if anxiety or depres-sion is a stimulus for overeating, then it might be rea-sonable to select a medication that has been proven topromote weight loss while also managing the underly-ing depression. It should be no surprise that antidepres-sants are included among the drugs used for weight loss.In this scenario, selection of a drug that increases nore-pinephrine, serotonin, or both might be the most appro-priate. Use of antidepressants in this manner are not FDAapproved and therefore off-label uses, as in the case offluoxetine (Prozac) and sertraline (Zoloft), which havebeen studied, are subject to professional prescribing reg-ulations. The text and figures that follow provide exam-
ples of drugs with current FDA approval for weight loss.Readers are encouraged to consult additional resourcesfor greater detail.
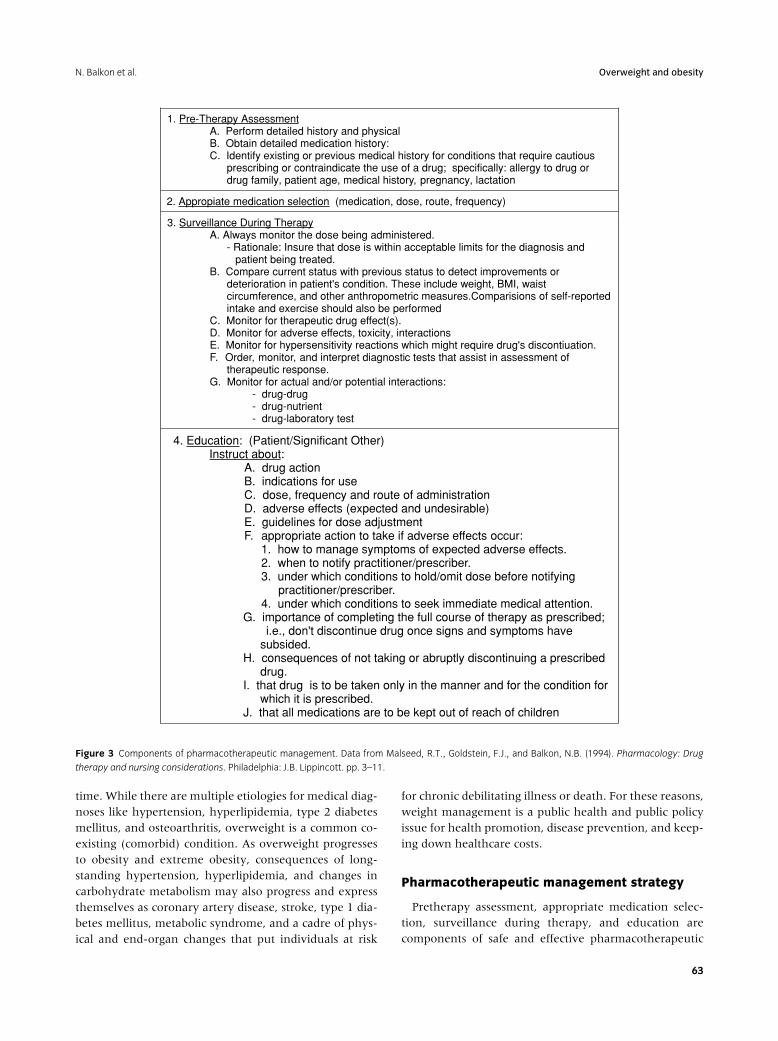
Noradrenergic agents are those compounds that arestimulated by or release norepinephrine. Most are pre-scribed. They are selected for their appetite suppres-sant (anorexiant) effect and not for stimulant (sympath-omimetic) effect. Most are recommended for short-termuse. Those with high abuse potential such as dextroam-phetamine are not recommended for weight loss. Theseagents are prescribed with caution in elders since they areknown to produce undesirable side effects in this popula-tion (Figure 4).
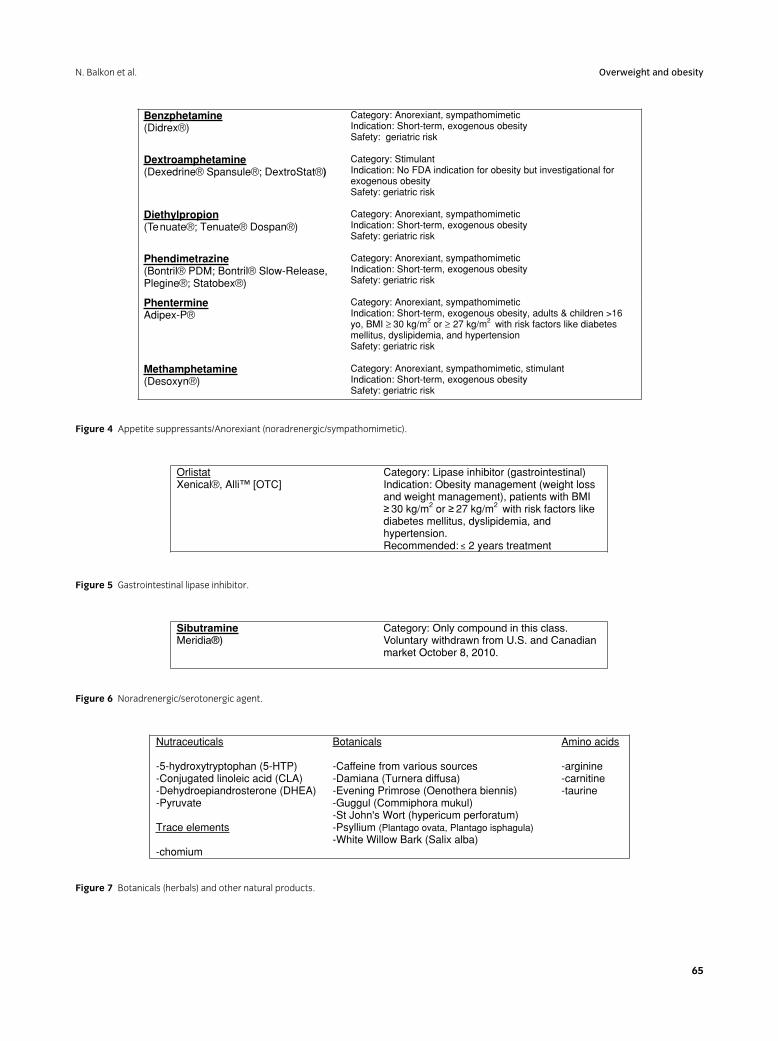
An FDA Safety Review of the gastrointestinal lipaseinhibitor orlistat (Xenical) was completed in May 2010following reports of liver-related adverse events (12 for-eign reports with Xenical; one U.S. report with Alli). Acausal relationship between this drug and severe liver in-jury has not been established; however, the FDA (2010c)has approved revised labeling for both drugs and recom-mends that clinicians consider the risk/benefits of phar-macotherapy with these drugs before prescribing or sug-gesting therapy with either formulation (Figure 5).
The only drug in the noradrenergic/serotonergic cat-egory, sibutamine (Meridia) was voluntarily withdrawnfrom U.S. and Canadian markets on October 8, 2010, inresponse to outcomes of SCOUT trial suggesting increasedcardiac risk (Figure 6; FDA, 2010b).
Botanicals (herbals), nutraceuticals, vitamins, miner-als, and amino acids all have found their way into theweight management-related pharmacotherapeutic litera-ture. Many claim weight management effects but to datehave not been studied in depth. Agents of particular in-terest are listed in Figure 7; however, detailed discussionis beyond the scope of this article.
In summary
The role of pharmacotherapeutics in the managementof weight gain has yet to be described fully.
Pharmacotherapy as a strategy for managing over-weight, obese, and extremely obese individuals remainscontroversial. Risk versus benefit and overall safety ofpharmacotherapy as an adjunct to weight loss manage-ment remains a primary focus for consideration amongclinicians and a viable topic for evidence-based outcomesresearch. While several pharmaceuticals in combina-tion with diet, exercise, and behavior modification havebeen shown to be a valuable adjunct in short-term andlong-term therapy several agents have voluntarily beenremoved from the U.S. marketplace or are prescribed andrecommended with caution due to adverse effect pro-files specifically related to alterations in cardiovascular or
64
N. Balkon et al. Overweight and obesity
Benzphetamine(Didrex®)
Category: Anorexiant, sympathomimetic Indication: Short-term, exogenous obesity Safety: geriatric risk
Dextroamphetamine(Dexedrine® Spansule®; DextroStat®)
Category: Stimulant Indication: No FDA indication for obesity but investigational for exogenous obesity Safety: geriatric risk
Diethylpropion(Tenuate®; Tenuate® Dospan®)
Category: Anorexiant, sympathomimetic Indication: Short-term, exogenous obesity Safety: geriatric risk
Phendimetrazine(Bontril® PDM; Bontril® Slow-Release, Plegine®; Statobex®)
Category: Anorexiant, sympathomimetic Indication: Short-term, exogenous obesity Safety: geriatric risk
PhentermineAdipex-P®
Category: Anorexiant, sympathomimetic Indication: Short-term, exogenous obesity, adults & children >16 yo, BMI ≥ 30 kg/m2 or ≥ 27 kg/m2 with risk factors like diabetes mellitus, dyslipidemia, and hypertension Safety: geriatric risk
Methamphetamine(Desoxyn®)
Category: Anorexiant, sympathomimetic, stimulant Indication: Short-term, exogenous obesity Safety: geriatric risk
Figure 4 Appetite suppressants/Anorexiant (noradrenergic/sympathomimetic).
OrlistatXenical®, Alli™ [OTC]
Category: Lipase inhibitor (gastrointestinal) Indication: Obesity management (weight loss and weight management), patients with BMI
30 kg/m2 or 27 kg/m2 with risk factors like diabetes mellitus, dyslipidemia, and hypertension. Recommended: – 2 years treatment <
Figure 5 Gastrointestinal lipase inhibitor.
SibutramineMeridia®)
Category: Only compound in this class. Voluntary withdrawn from U.S. and Canadian market October 8, 2010.
Figure 6 Noradrenergic/serotonergic agent.
Nutraceuticals
-5-hydroxytryptophan (5-HTP) -Conjugated linoleic acid (CLA) -Dehydroepiandrosterone (DHEA) -Pyruvate
Trace elements
-chomium
Botanicals
-Caffeine from various sources -Damiana (Turnera diffusa) -Evening Primrose (Oenothera biennis) -Guggul (Commiphora mukul) -St John's Wort (hypericum perforatum) -Psyllium (Plantago ovata, Plantago isphagula) -White Willow Bark (Salix alba)
Amino acids
-arginine-carnitine -taurine
Figure 7 Botanicals (herbals) and other natural products.
65

Overweight and obesity N. Balkon et al.
hepatic function. Despite ongoing research and recog-nition that obesity is on the rise in the United States,continued reluctance to initiate clinician-managed phar-macotherapy for weight loss as a first-line therapeuticintervention remains. Pharmacotherapy is typically rec-ommended to be considered when the BMI is ≥ 30 kg/m2
or ≥ 27 kg/m2 with risk factors for or comorbidities likediabetes mellitus, dyslipidemia, and hypertension. In allcases, it is recommended that risk/benefit of pharma-cotherapy be assessed.
References
Clinicaltrials.gov. 2010. A long term study of sibutramine and the role of
obesity management in relation to cardiovascular disease in overweight
and obese patients (SCOUT). Last updated May 6, 2010. Study completed
November 2009.
James, W. P., Caterson, I. D., Coutinho, W., Finer, N., Van Gaal, L. F.,
Maggioni, A. P., et al. (2010). SCOUT Investigators. Effect of sibutramine
on cardiovascular outcomes in overweight and obese subjects. New England
Journal of Medicine, 363(10):905–917.
Malseed, R. T., Goldstein, F. J., & Balkon, N. B. (1994). Pharmacology:
Drug therapy and nursing considerations (pp. 3–11). Philadelphia: J. B.
Lippincott.
Sherry, B., Blanck, H. M., Galuska, D. A., Pan, L., Dietz, H. W., & Balluz, L.
(2010). Vital signs: State-Specific obesity prevalence among
adults — United States, 2009. Morbidity and Mortality Weekly Reviews, August
3, 2010 Retrieved October 2010 from http:www.cdc.gov/mmwr/pdf/wk/
mm59e0803.pdf
U.S. Food and Drug Administration. (2010a). Postmarket drug safety
information–– Fen-Phen. Retrieved October 2010 from http://www.fda.
gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsand
Providers/ucm179871.htm
U.S. Food and Drug Administration. (2010b). Postmarket drug safety
information – Meridia. Retrieved October 2010 from http://www.fda.
gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsand
Providers/ucm191652.htm
U.S. Food and Drug Administration. (2010c). Safety information –
Orlistat. Retrieved October 2010 from http://www.fda.gov/Safety/
MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/
ucm213448.htm
66