Embed Size (px)
Citation preview
Clinical Trial Billing Compliance
Overview
September 2014
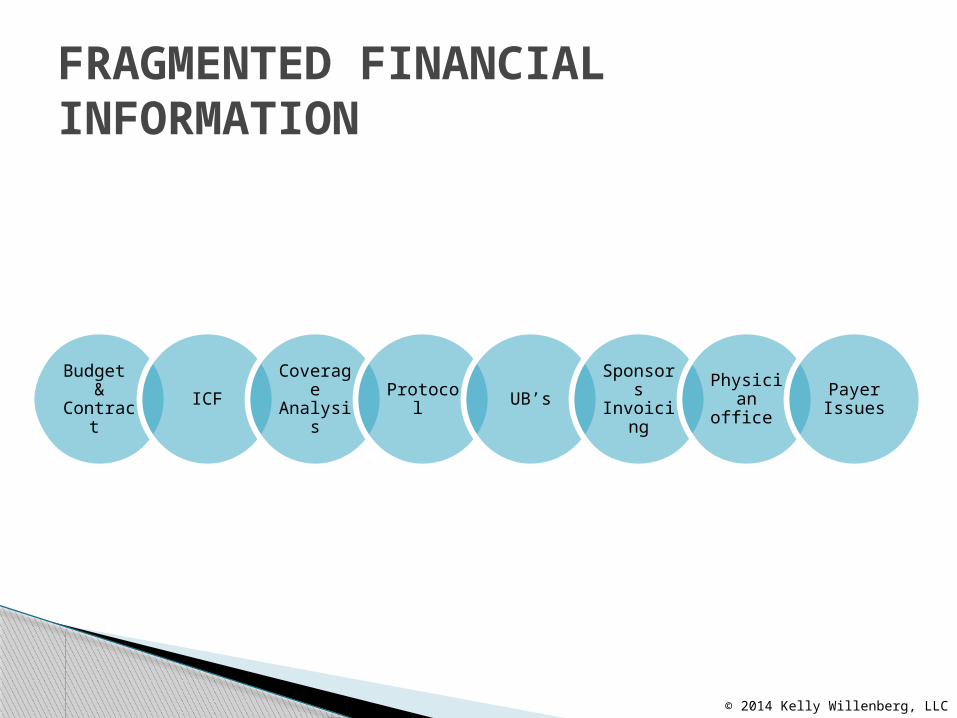
FRAGMENTED FINANCIAL INFORMATION
Budget &
Contract ICF
Coverage
AnalysisProtocol UB’s Sponsors
InvoicingPhysician office
Payer Issues
© 2014 Kelly Willenberg, LLC
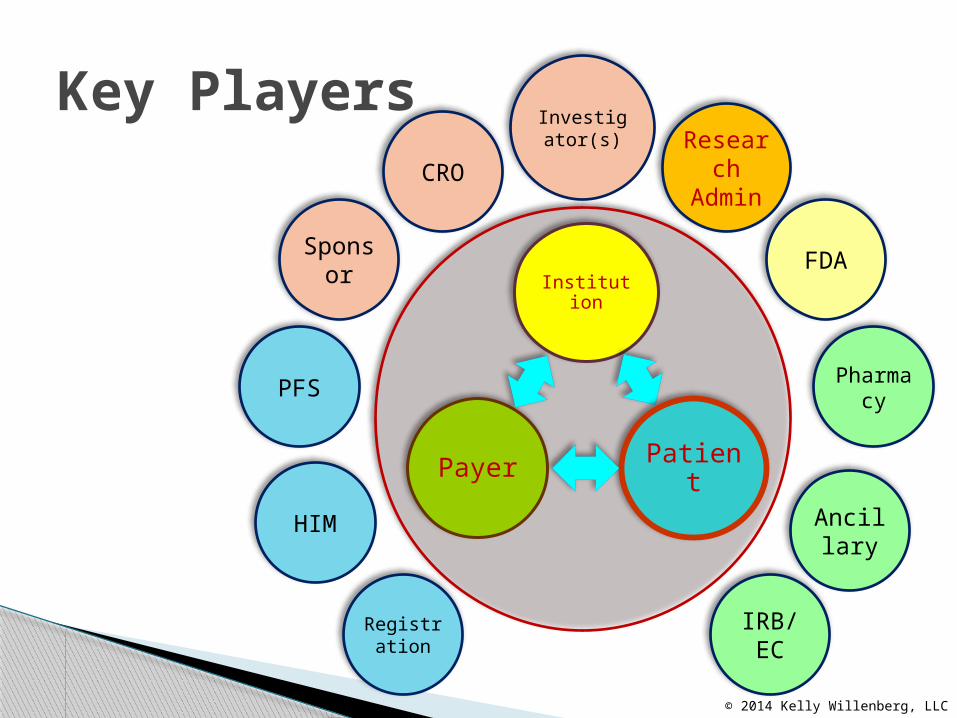
Institution
PatientPayer
Sponsor
CRO
Investigator(s)
FDA
Ancillary
IRB/EC
PFS
HIM
Registration
Key Players
© 2014 Kelly Willenberg, LLC
Pharmacy
ResearchAdmin
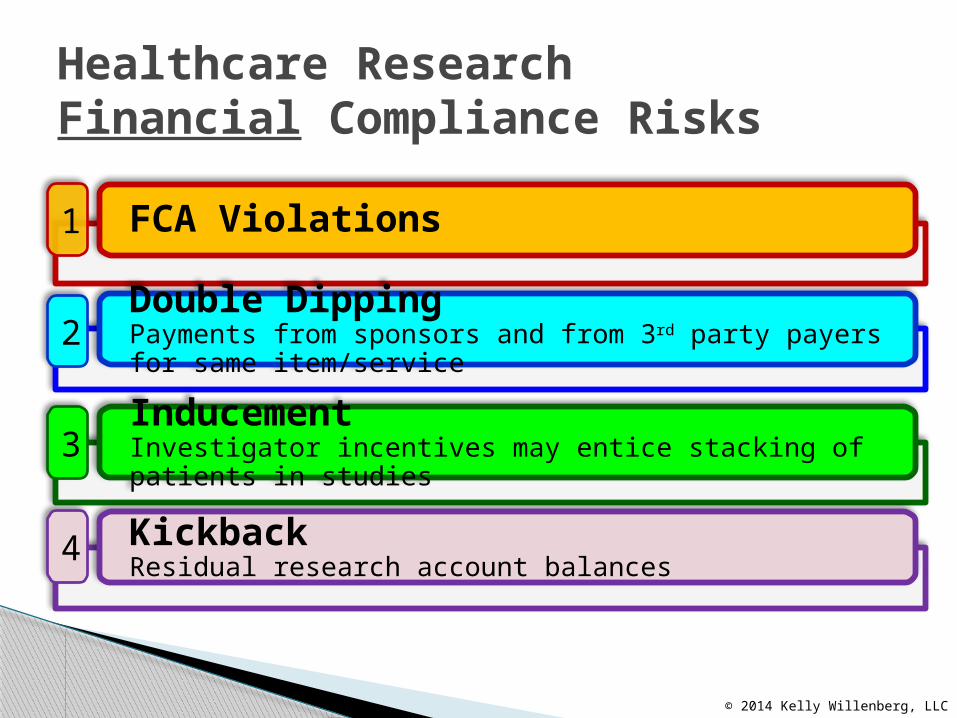
Healthcare ResearchFinancial Compliance Risks
© 2014 Kelly Willenberg, LLC
FCA Violations
Double DippingPayments from sponsors and from 3rd party payers for same item/service
InducementInvestigator incentives may entice stacking of patients in studies
KickbackResidual research account balances
1
2
3
4

Common Current State of Research in Community Hospitals
© 2014 Kelly Willenberg, LLC
Physicians/InvestigatorsAre conducting Clinical Trials independent of Hospitals
Reasons:• Independence • Lack confidence in Hospital’s ability • Control of grants/study funds • Circumvent hospital bureaucracy• Decrease paperwork conducting Clinical Trials independent of Hospitals
HospitalsResearch financial compliance programs may not be operationally effective and/or efficient Causes:• Ownership & Accountability • Policies and Procedures • Centralization • Resources • Physicians trust lacking• Management of grant/study funds research billing compliance Programs may not be operationally effective and/or efficient
External Parties Are approaching the investigator directly
Goals:• The PI knows sooner • Immediate results • Decrease paperwork • Decrease costs• Maintain control• Reduce accountability and scrutiny• Circumvent the hospitalapproaching the investigator directly
Frequent Issues Investigators will use the IRB submission as
the protocol◦ Calendar of events “loose” which makes budgeting
a challenge, coverage analysis impossible Assume that everything in the protocol is
conventional care or “standard of care” and therefore billable
Confusion about drug supplies◦ In IIT trials the drugs are sometimes not billable
and reimbursable Collaborating with team to decide on budget
© 2014 Kelly Willenberg, LLC
Read the protocol and review the proposed budget sent by the sponsor
Determine if the trial is qualified under Medicare guidelines
Decide what are considered patient services that are standard of care and what are research patients services
Do a Coverage Analysis
September 2014
What should you do First?
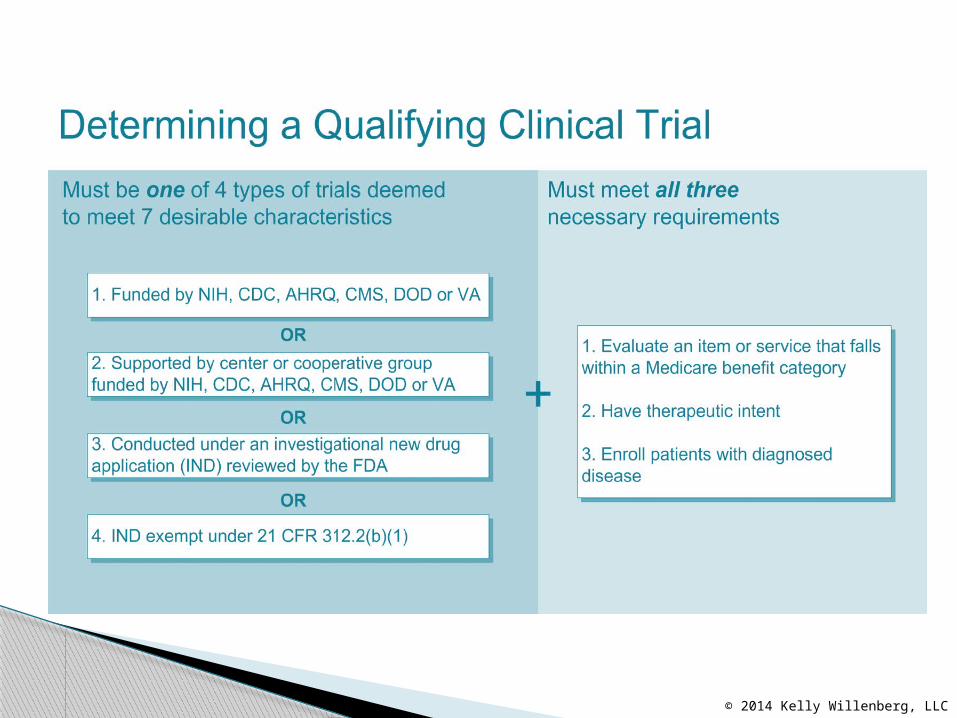
Perform Qualifying Clinical Trial (QCT) Analysis
Develop grid to match schedule of events Identify items or services “hard-wired” free
into protocol Determine items and services that are
routine costs Determine if routine costs are covered by
Medicare
General Order of steps
© 2014 Kelly Willenberg, LLC
Check proposed contract to determine if offered budget covers items and services that are not billable
Negotiate contract/budget against the Coverage Analysis
Finalize necessary sections of informed consent
Finalize and lock grid once study approved to be used as translation tool for billing and reimbursement.
General order of steps
© 2014 Kelly Willenberg, LLC
© 2014 Kelly Willenberg, LLC
Clinical Trials Policy – CMS Policy (July 2007) that provides guidance regarding Medicare beneficiaries participating in Clinical Trials and routine costs http://www.cms.gov/Medicare/Coverage/ClinicalTrialPolicies/index.html
Routine Costs: items and services that are provided to the patient even if s/he was NOT in a clinical trial, conventional care
Routine Costs are defined, specified and documented in the Trial documents prior to the beginning of the Trial: a thorough coverage analysis
September 2014
Assessing Routine Costs
What is an Coverage Analysis? A Coverage Analysis will determine whether
any procedures may be billed to Medicare (and by extension to other insurance companies)
This presentation does not cover MCA’s but demonstrates why doing an MCA important when completing a budget
This is the first step to doing a proper budget
© 2014 Kelly Willenberg, LLC
Coverage Analysis
Is the study “qualifying” under the guidelines?
What are the “routine” costs?
Which of the above are covered by Medicare?
How is the costs worded in the contract and consent?
© 2014 Kelly Willenberg, LLC
POSSIBLE CLINICAL TRIAL BILLING ERRORS
14
• Billing for services not rendered• Billing for services that are already paid by the
sponsor or promised free in the informed consent• Billing for services that are for research-purposes
only or are part of a non-qualifying clinical trial• Billing Medicare for device trials without MAC
approval letter in hand• Bill Medicare Advantage Plans (Part C) when claims
should be directed to the Medicare Administrative Contractor
©Kelly Willenberg, LLC 2014
POSSIBLE CLINICAL TRIAL BILLING ERRORS
15
• Billing for items or services not supported by required documentation• A proper, signed order• Adequate documentation of medical necessity for the
item or service• Documentation of study participation, as required
• Billing without proper codes, modifiers or NCT #• Waiving/paying/reimbursing subject co-pay or
deductible obligations
©Kelly Willenberg, LLC 2014
© 2013 Kelly Willenberg, LLC16
The 8-digit clinical trial number must be reported on all claims (Medicare beneficiaries, Traditional and Managed Care) associated with clinical trial participation
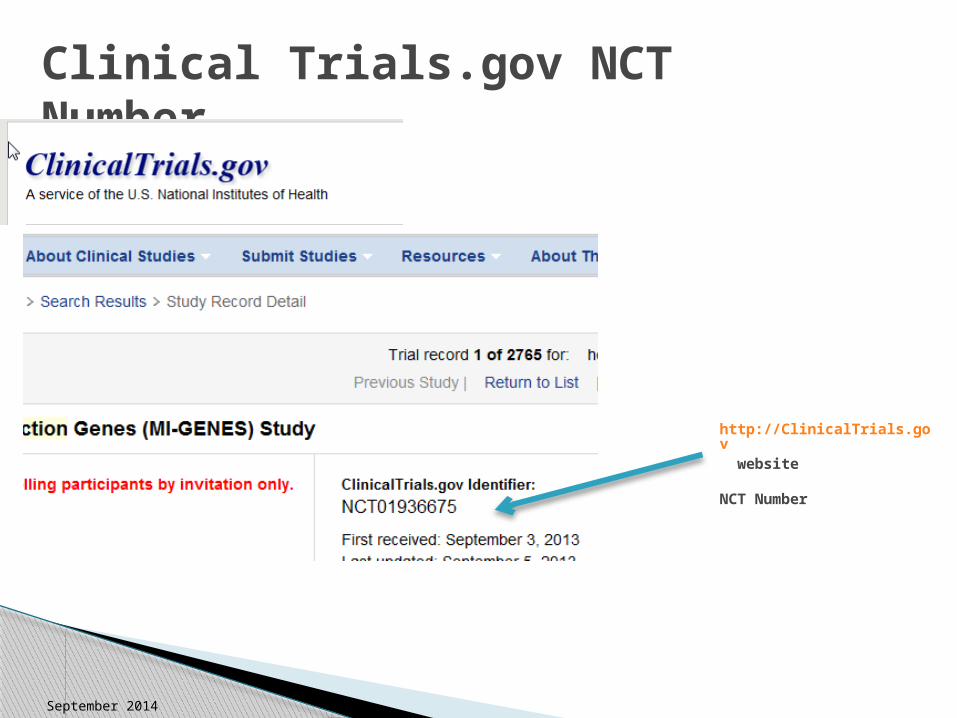
• National Clinical Trial (NCT) number NCT12345678• Also known as the Clinicaltrials.gov Identifier
Effective Date: Services on/after January 1, 2014• Voluntarily reported since January 2008
Claim types: Both hospital/technical and professional
September 2014
Mandatory Reporting of NCT Number – MM8401
CMS will use this number to identify all items and services provided to Medicare beneficiaries (Traditional and Managed Care) during their participation in a Medicare qualifying clinical trial, study, or registry
Permits CMS to:• Better track payments• Ensure that the information gained from the research
is used to inform coverage decisions• Make certain that the research focuses on issues of
importance to the Medicare population
September 2014
Why?
September 2014
Clinical Trials.gov NCT Number
http://ClinicalTrials.gov website
NCT Number
ICD-9-CM Diagnosis Code V70.7 (Examination of a participant in a clinical trial); ICD-10 coming 2015
Revenue Code 0624 for FDA Investigational Devices, as applicable
Condition Code 30
Q0 and Q1 modifiers, as applicable (outpatient claims only)
NCT number
Report in UB-04 Form Locators 39-41
September 2014
Required data Elements for reporting: Hopsitals
ICD-9-CM Diagnosis Code V70.7 (Examination of a participant in a clinical trial); ICD-10 coming in 2015
Revenue Code 0624 for FDA Investigational Devices, as applicable
Q0 and Q1 modifiers, as applicable (outpatient claims only)
NCT number
Report in CMS-1500 Field 19
September 2014
Required Data Elements for Reporting: Physician Practices
• If some, but not all of the required elements (NCT #, ICD-9 code, modifiers, revenue codes, condition codes) are reported, the claim will be stopped and returned to the provider (RTP)
• Possible RTP statements:• “Claim lacks information which is needed for adjudication
…..”• “Missing/incomplete/invalid Investigational Device
Exemption number for FDA-approved clinical trial services”• “Your claim contains incomplete and/or invalid information,
and no appeal rights are afforded because the claim is unprocessable ….”
September 2014
What happens if we don’t report?
Questions
Kelly Willenberg, MBA, BSN, CHRC, [email protected]
864-473-7209
© 2014 Kelly Willenberg, LLC


















![(4) Masama,B - Willenberg,C [D94] - Chess Western Province](https://img.pdfslide.us/doc/110x75/61969d21a1cc9770721a84d9/4-masamab-willenbergc-d94-chess-western-province.jpg)










