Embed Size (px)
Citation preview

Dr. Karthik Ramasamy
Consultant Hematologist, Oxford University Hospitals
OVERVIEW OF RRMM TREATMENT IN THE REAL-WORLD SETTING
GLOIXA2019-00011h. December 2019.

YOUR CHOICE OF THERAPY FOR RRMM PATIENTS IS OFTEN DRIVEN BY:
1. Data from RCTs
2. Real-world evidence data
3. Patient choice
4. Fitness and comorbidities
RCT, randomized controlled trial; RRMM, relapsed/refractory multiple myeloma

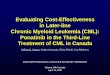
SURVIVAL IN RRMM
*Number of patients at risk at each time point reflects the number of patients with follow-up available for evaluation at those time pointsMM, multiple myeloma; No., number
©2015 by American Society of HematologyCook G, et al. Blood 2015;126(23):abstract 2093.
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36
Died due to MM
Patients alive
Died due to other reason
Pro
po
rtio
n o
f p
atie
nts
aliv
e
Pro
po
rtion
of p
atien
ts wh
o d
ied
Visit (months)
No. at risk* 627 558 451 356 268 191 146 91 54 21 6
0.0

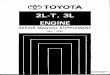
LARGE PROPORTION OF PATIENTS ARE LOST AT EACH LINE OF THERAPY
Yong K et al. Br J Haematol 2016;175:252–64.
• Real-world, retrospective study shows that 15% of patients reach the 4th line of treatment
• Currently only 61% of patients reach 2nd line of treatment
100%
95%
61%
38%
15%
1%
Mean (95% CI): diagnosis, 2 m (1.60, 2.40); 1L, 8 m (7.74, 8.26); 1L maintenance, 9 m (7.78, 10.22)
Mean (95% CI): 2L–3L, 11 m (10.22, 11.78); 3L, 8 m (7.63, 8.37)
Mean (95% CI): 1L–2L, 16 m (15.0, 17.0); 2L 9 m (8.64, 9.36)
Mean (95% CI): 3L–4L, 7 m (5.9, 8.1); 4L, 6 m (5.5, 6.5)
Mean (95% CI): 4L–5L, 3 m (1.8, 4.2); 5L, 4 m (3.15, 4.85)
Median durations in months shown
Start1L
End 1L induction
End 1L maintenance
Start2L
Start4L
Start5L
End 2L
End 3LStart 3L
End 4L
End 5L
1L
2L
3L
4L
5L
1 m 6 m 6 m
5 m 6 m
3 m
1 m 4 m
Active treatment
Treatment-free interval
Maintenance treatment
5 m
Diagnosis
10 m 7 m
CI, confidence interval; L, line (of therapy); m, months

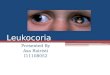
A SUBSTANTIAL PROPORTION OF REAL-WORLD PATIENTS ARE NOT ELIGIBLE FOR CLINICAL TRIALS, DRIVING DIFFERENCES IN OUTCOMES
• Clinical trial eligibility criteria may exclude many patients from trial participation1
• 40% of NDMM patients from the Connect MM registry are ineligible for enrollment in RCTs, based on common RCT exclusion criteria from published studies*,1
• 3-year OS rate significantly lower in RCT-ineligible versus RCT-eligible patients (63% vs 70%; p<0.05)1
• Thus, clinical trial findings may not reflect the overall MM population1
*Common RCT exclusion criteria included: M-protein ≤1.0 g/dL, creatinine >2.5 mg/dL (13.9%), low absolute neutrophil count (≤1.5 x 109/L), and low hemoglobin (≤8 g/dL)HR, hazard ratio; NDMM, newly diagnosed multiple myeloma; OS, overall survival 1. Shah JJ, et al. Clin Lymphoma Myeloma Leuk 2017;17:575–83.
Su
rviv
al
pro
bab
ilit
y1
0.2
0.4
0.6
0.8
1.0
Duration (months)No. at risk
RCT-eligible 820 758 699 636 479 291
RCT-ineligible 548 491 431 391 280 165
HR: 0.81
95% CI: 0.67‒0.99
p=0.03920
0 12 36 7224 66605448426 18 30
RCT-eligible
RCT-ineligible

OSPFS
0 12 24 36 48 60 72 84
Time (months)
0
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n o
f p
atie
nts
wit
ho
ut
eve
nt
(%)
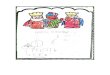
Trial-eligibleTrial-ineligible
No. at risk194 120 73 45 24 15 3 091 40 20 8 5 1 0
Trial-eligible
Trial-ineligible
27.3 (23.3–33.0)
16.2 (11.1–20.4)
105 (54.1)
60 (65.9)
EventsN (%)
Median PFSMonths (95% CI)
0 12 24 36 48 60 72 84
Time (months)
0
10
20
30
40
50
60
70
80
90
100
Pro
po
rtio
n o
f p
atie
nts
wit
ho
ut
eve
nt
(%)
Trial-eligibleTrial-ineligible
No. at risk194 157 133 110 83 62 10 091 61 46 30 27 15 4
Trial–eligible
Trial–ineligible
91 (46.9)
57 (62.6)
58.6 (48.6–64.4)
34.2 (21.6–48.1)
EventsN (%)
Median OSMonths (95% CI)
0
GERMAN REGISTRY DATA – NTE NDMM PATIENTS
NTE, non-trial-eligible; PFS, progression-free survival Knauf W, et al. Ann Hematol 2018;97:2437–45.

TYPES OF RWE: DATA GENERATED FROM MULTIPLE REAL-WORLD SOURCES
Multiple types of RWE,1 comprising data from the real-world setting generated from sources other than prospective, interventional clinical trialsEHR, electronic health records; EMR, electronic medical records; RWE, real-world evidence 1. Richardson et al. Blood 2017;130(Suppl 1):abstract 3149 (poster presentation).
• Registry-based studies (broad, population-based observational studies collecting uniform data) and analyses of registry data
• Also, data from registries specific to prospective/retrospective research projects
Prospective/retrospective local/national clinical registry studies
• Observational and non-interventional studies with specific eligibility criteriaProspective/retrospective formal
observational studies
• Analyses of data from programs with specific patient eligibility criteriaNamed-patient/compassionate use
programs
• Analyses of patient chart data/records from 1 or more treatment centersSingle-/multi-center,
retrospective/longitudinal chart reviews
• Retrospective analyses of data based on EHR/EMR or claims databasesData from electronic health/medical records
(EHR/EMR) or billing/insurance claims databases
• Analyses of data from national databases, programs, or centralized initiativesRetrospective national program analyses

A NUMBER OF MM PATIENT POPULATIONS ARE TYPICALLY UNDER-REPRESENTED IN CLINICAL TRIALS
1. Shah JJ, et al. Clin Lymphoma Myeloma Leuk 2017;17:575–83.2. Costa L, et al. Leuk Lymphoma 2016;57:2827–32.3. Fiala MA, et al. Leuk Lymphoma 2015;56:2643–9.
4. Pulte E, et al. Blood Advances 2018;2:116–9.
Patients with comorbidities1
or advanced disease1,2
Elderly, frail patients1,2
Patients from lower
socio-economic backgrounds3
Ethnic or racial minorities1,2,4
These characteristics are linked to worse outcomes to treatment1–4

• Patient selection: elderly patients and patients with comorbidities under-represented
• Less prone to bias – good internal validity
• Under-representation of community centers
• Stringent inclusion/exclusion criteria
• Protocol-driven dose modification may lead to better tolerability and longer duration of therapy
FACTORS POTENTIALLY CONTRIBUTING TO THE GAP BETWEEN REAL-WORLD EFFECTIVENESS AND CLINICAL TRIAL EFFICACY
1. Richardson et al. Blood 2017;130(Suppl 1):abstract 3149 (poster presentation).
• Higher toxicity burden among trial-ineligible patients; e.g. elderly patients and patients with more comorbidities
• Patient and physician preference and motivation
• Different distribution of academic versus community centers
• Healthcare access issues
• Good generalizability of results to wider MM population
• Other factors contributing to premature discontinuation of treatment regimens, e.g. mobility, patient distance from hospital, number of visits required during treatment
Clinical trial factors Real-world factors

PROLONGED DURATION OF THERAPY APPEARS TO BEASSOCIATED WITH IMPROVED OUTCOMES IN CLINICAL TRIALS
CT, continuous therapy; FDT, fixed-duration therapy; IMiD, immunomodulatory drug; PD-1, first disease progression; PI, proteasome inhibitor
1. Robinson D, et al. Blood 2014;124:5676.2. Gandolfi S, et al. Cancer Metastasis Rev 2017;36:561–84.
3. Palumbo A, et al. J Clin Oncol 2015;33:3459–66.
• With the introduction and widespread use of multiple novel agents and the emerging treatment paradigm of long-term, continuous therapy, clinical outcomes have improved substantially in the past ~20 years, with a shift in the median OS from ~3 to ~5 years1,2
Pooled analysis of IMiD and PI-based regimens: longer PFS and OS with continuous therapy versus fixed-duration therapy3
n PD-1 Death
CT 417 219 9
FDT 410 308 13
HR: 0.47; 95% CI: 0.40‒0.56; p<0.001
PF
S(p
rob
ab
ilit
y)
Time (months)
0
0.2
0.4
0.6
0.8
1.0
0 12 36 6024 48
n Death
CT 417 111
FDT 410 143
HR: 0.69; 95% CI: 0.54‒0.88; p=0.003
OS
(pro
bab
ilit
y)
Time (months)
0
0.2
0.4
0.6
0.8
1.0
0 12 36 6024 48

PROLONGED DOT ASSOCIATED WITH IMPROVED OS IN RRMM PATIENTS IN ROUTINE CLINICAL CARE
• Large, retrospective US study evaluating the effect of the length of 2LT on OS in a heterogeneous cohort of RRMM patients treated between 2008‒20151
• Longer duration of 2LT significantly associated with improved 1-year OS1
2LT, 2nd-line therapy; DoT, duration of treatment; OR, odds ratio 1. Hari P, et al. Clin Lymphoma Myeloma Leuk 2018;18:152–60.
Percentage of increase in 1-year OS relative to median DoT of 2nd-line therapy1
OR: 0.78; 95% CI: 0.77‒0.83; p<0.01Pro
ba
bilit
yo
f s
urv
iva
l
(at
12
mo
nth
s)1
0
0.2
0.4
0.6
0.8
1.0
0 1 92 123 4 5 6 7 8 10 11
Duration of 2LT (months)
Do
Tin
2LT
(m
on
ths
)
0 2 10 1684 6 12 14
Percentage increase in 1-year OS
relative to median DoT in 2LT (months)
14%
12.7%
11.1%
9.2%
6.7%
3.7%
11 to <12 10 to <11
9 to <10 8 to <9 7 to <8
≥12

PFS/TTNT AND OS FOR PI-BASED REGIMENS IN RRMM: PHASE 3 CLINICAL TRIAL RESULTS VERSUS REAL-WORLD DATA
Ixazomib, in combination with lenalidomide and dexamethasone, is approved for the treatment of adult patients with MM who have received at least one prior therapy*Real-world data are shown as ranges of PFS/TTNT or OS. †OS data not reported in TOURMALINE-MM122 and for real-world ixazomib-based regimens.23,24 IV, intravenous; Kd, carfilzomib, dexamethasone; NR, not reported; RW, real-world; SC, subcutaneous; TTNT, time to next therapy; Vd, bortezomib, dexamethasone
1. Arnulf B, et al. Haematologica 2012;97:1925–8. 2. Richardson PG, et al. Blood 2007;110:3557–60. 3. Richardson PG, et al. N Engl J Med 2005;352:2487–98. 4. Durie B, et al. Haematologica 2017;102(s2):520.
5. Romanus D, et al. Clin Lymphoma Myeloma Leuk 2017;17:e81–e82. 6. Jagannath S, et al. Expert Rev Hematol 2016;9:707–17. 7. Nooka A, et al. Blood 2017;130(Suppl):3093. 8. Chari A, Blood 2017;130(Suppl):1818.
9. Hajek R, et al. Haematologica 2016;101(s1):532. 10. Dimopoulos MA, et al. Lancet Oncol 2016;17:27–38. 11. Dimopoulos MA, et al. Lancet Oncol 2017;18:1327–37. 12. Stewart AK, et al. N Engl J Med 2015;372:142–52. 13. Siegel DS, et al. J Clin Oncol 2018;36:728–34. 14. Chen CC, et al. J Manag Care Spec Pharm 2017;23:236–46.
15. Rifkin RM, et al. Blood 2017;130(Suppl):3433. 16. Rifkin RM, et al. Blood 2017;130(Suppl):3434. 17. Potluri R, Blood 2017;130(Suppl):1844. 18. Sevindik OG, et al. Blood 2017;130(Suppl):5405.
19. Hobbs M, et al. Blood 2016;128(Suppl):3337. 20. Danhof S, et al. Clin Lymphoma Myeloma Leuk 2015;15(Suppl 3):e284. 21. Cerchione C, et al. Haematologica 2017;102(s2):804. 22. Moreau P, et al. N Engl J Med 2016;374:1621–34.
23. Ziff M, et al. Haematologica 2017;102(s2):786–7. 24. Terpos E, et al. Blood 2017;130(Suppl):3087.
9.4
9.3
8.4
RW bortezomib-based regimens4-
9 5.7‒13.6
NRAPEX2,3
MMY-3021 V IV1
MMY-3021 V SC1
ENDEAVOR Vd10,11
26.3
18.7
RW carfilzomib-based regimens4-6,14-21
3.2‒25.3
ENDEAVOR Kd10,11
ASPIRE12,13
20.6
RW ixazomib-based regimens23,24
0 5 10 15 20 25 30
19.2‒27.6
Median PFS/TTNT (months)*
TOURMALINE-MM122
RW bortezomib-based regimen7,9
40
29.8
16.2‒27.3
NR
NR
APEX2
MMY-3021 V IV1
MMY-3021 V SC1
ENDEAVOR Vd11
RW carfilzomib-based regimens18-
21
Median OS (months)*,†
48.3
47.6
0 10 20 30 40 50
3.0‒16.1
ENDEAVOR Kd11
ASPIRE13

ANALYSIS OF THE OPTUM EHR DATABASE: I-/B-/C-/D-BASED TRIPLETS
1. Davies F, et al. Hemasphere 2019;3(S1):abstract PS1419 (poster presentation).
• Real-world comparative effectiveness analysis of triplet regimens containing bortezomib (B), carfilzomib (C), daratumumab(D), or ixazomib (I) in RRMM patients
Objective
• Retrospective cohort study design
• Patients who initiated I-/B-/C-/D-based triplet therapy after ≥1 prior line on or after January 2014 in the Optum US-based EHR database were identified
• Database covers clinical practice in the US
Study design
• Duration of therapy
• Time to next therapy
• Kaplan-Meier analyses; stratified by line of therapy, ± confounder-adjusted Cox proportional hazards model
• Separate analyses of all triplet regimens and of Rd-based triplets
Outcomes
Rd, lenalidomide-dexamethasone

ANALYSIS OF THE OPTUM EHR DATABASE: I-/B-/C-/D-BASED TRIPLETS
CRAB, hypercalcemia, renal impairment, anemia, or bone lesions; IQR, interquartile range 1. Davies F, et al. Hemasphere 2019;3(S1):abstract PS1419 (poster presentation).
B-based C-based D-based I-basedN 746 522 418 216Median age, years (IQR) 70 (61–77) 65 (57–73) 68 (61–74) 69 (62–79)Age ≥75 years, % 33.0 20.1 24.9 38.4Median follow-up, months (IQR) 16.3 (6.8–28.6) 13.3 (5.6–23.7) 7.9 (3.5–12.4) 10.2 (5.4–16.1)Charlson Comorbidity Index score 0 / 1 / ≥2, % 28.7 / 10.7 / 60.6 24.9 / 12.8 / 62.3 25.6 / 12.4 / 62.0 40.3 / 11.6 / 48.2High-risk cytogenetics, % 15.7 25.9 20.3 13.9Any CRAB symptoms, % 81.8 86.8 81.8 63.9Line of treatment, %2 59.3 34.5 22.7 36.63 21.9 25.3 20.8 26.94 10.2 19.2 21.5 17.1≥5 8.7 21.1 34.9 19.4
Prior treatment exposure, %IMiD and PI 40.6 74.9 77.8 61.6PI only 36.9 19.7 11.2 11.6IMiD only 20.2 4.4 9.3 25.5
Refractory to IMiD and PI / IMiD only / PI only / Neither, %
10.3 / 23.3 / 4.0 / 62.3 40.4 / 12.3 / 31.2 / 16.1 50.0 / 17.5 / 17.2 / 15.3 27.3 / 13.9 / 23.6 / 35.2
Refractory to prior line of therapy, % 73.7 85.1 83.3 74.5Prior stem cell transplant, % 19.7 33.5 37.1 20.8Median time from diagnosis, months (IQR) 22.3 (10.8–43.1) 26.2 (13.0–47.6) 37.9 (22.4–58.8) 35.8 (20.7–57.1)

B-based C-based D-based I-basedN 746 522 418 216
Combination regimen, %
+Lenalidomide-dexamethasone 46.8 41.8 23.7 71.3
+Cyclophosphamide-dexamethasone 35.8 25.5 NR 5.1
+Pomalidomide-dexamethasone 7.0 28.0 35.6 20.8
+Bortezomib-dexamethasone NR NR 28.7 NR
+Carfilzomib-dexamethasone NR NR 4.5 NR
Other 10.5 4.8 7.4 2.8
ANALYSIS OF THE OPTUM EHR DATABASE: I-/B-/C-/D-BASED TRIPLETS
DoT, duration of treatment; Pom, pomalidomide 1. Davies F, et al. Hemasphere 2019;3(S1):abstract PS1419 (poster presentation).
• I-based regimens had the longest median DoT among all patients receiving ≥2nd-line therapy and among those receiving 2nd- and 3rd-line therapy (unadjusted analyses)
All patients receiving ≥2nd-line therapy Patients receiving 2nd- or 3rd-line therapy
Regimen Median DoT, months Regimen Median DoT, months
I-based 8.4 I-based 8.4
D-based 6.2 B-based 8.4
B-based 6.0 C-based 6.3
C-based 6.0 D-based NR (short follow-up)
P=0.0084 P=0.0748

ANALYSIS OF THE OPTUM EHR DATABASE: I-/B-/C-/D-BASED TRIPLETS
• Median TTNT was longer with I-based (11.1 months) versus B-based (9.8 months), C-based (6.7 months), and D-based (7.2 months) triplets (left-hand figure)– In this unadjusted analysis, the risk of next treatment initiation or death was significantly reduced in the I-based regimen group versus the
B-based group (reference); HR 0.80 (p=0.0299)– In the adjusted analysis, differences versus the B-based group were not significant
• In a stratified analysis of Rd-based regimens, TTNT appeared similar with IRd, BRd, and DRd but shorter with CRd (right-hand figure)– On adjusted analyses, no regimen was significantly different in terms of next treatment initiation or death versus B-based triplets that utilized
an Rd backbone
B/C/D/I-Rd, bortezomib/carfilzomib/daratumumab/ixazomib plus lenalidomide-dexamethasone 1. Davies F, et al. Hemasphere 2019;3(S1):abstract PS1419 (poster presentation).
Month from start index line of therapy0 3 6
75
Eve
nt–
fre
e s
urv
ival
(%
)
9 12 15 18 21 24
427746 579 332 253 180 139 103 82B–based256522 376 185 130 96 67 53 38C–based161418 251 102 57 28 18 5 1D–based119216 163 81 49 32 17 7 2I–based
No. at risk
100
50
25
0
Risk of event, HR (95% CI), UnadjustedB–based <reference>C–based 1.15 (1.00, 1.33); p=0.0529D–based 1.04 (0.87, 1.25); p=0.6567I–based 0.80 (0.65, 0.98); p=0.0299
Adjusted<reference>1.00 (0.85, 1.18); p=0.99690.86 (0.70, 1.05); p=0.14090.84 (0.68, 1.04); p=0.1055
TTNT with all triplet regimens
6
75
Eve
nt–
fre
e s
urv
ival
(%
)
Month from start index line of therapy0 3 9 12 15 18 21 24
224349 282 180 144 107 82 61 47B–Rd119218 168 86 61 46 32 26 20C–Rd5499 77 38 19 7 5 0 0D–Rd87154 116 60 37 27 14 5 1I–Rd
No. at risk
100
50
25
0
Risk of event, HR (95% CI), UnadjustedB–Rd <reference>C–Rd 1.33 (1.06, 1.66); p=0.0133D–Rd 0.75 (0.52, 1.10); p=0.1368I–Rd 0.99 (0.76, 1.30); p=0.9544
Adjusted<reference>1.20 (0.90, 1.60); p=0.21240.68 (0.44, 1.06); p=0.08710.95 (0.70, 1.30); p=0.7649
TTNT with Rd-based triplet regimens

ANALYSIS OF THE HUMEDICA EMR DATABASE: VRD, KRD, AND IRD IN RRMM
• DoT and TTNT of VRd, KRd, IRd in patients with RRMM: clinical practice in the US versus clinical trial experience
– Retrospective cohort study design: patients who initiated KRd, VRd, or IRd (index regimen) as treatment line 2, 3, or 4 between Jan 2008 and Dec 2016 in Humedica, a large US-based EMR database, were identified
– Endpoints: DoT, TTNT, discontinuation rates
KRd, carfilzomib, lenalidomide, dexamethasone; VRd, bortezomib plus Rd 1. Chari A, at al. Blood 2017;130(Suppl 1):abstract 1818 (poster presentation).
VRd KRd IRd
n 343 139 49
Median age (years) 69 65 73
Median follow-up (months) 17.3 8.3 5.2
Median DoT (months)
PI component alone 5.4 6.1 NR
Entire regimen 8.7 6.3 NR
Median TTNT (months) 12.9 8.7 NR

DoT (PI component)
Month from start of regimen
100
80
60
40
20
00 6 12 21 24
Tre
atm
en
t co
nti
nu
atio
n
pro
bab
ility
(%
)
3 9 15 18
IRdKRdVRd
TTNT
Month from start of regimen
100
80
60
40
20
00 6 12 21 24
Eve
nt-
fre
e p
rob
abili
ty (
%)
3 9 15 18
IRdKRdVRd
• This US-based EMR analysis of 531 patients treated with VRd, KRd, or IRd indicated that patients were able to stay on the PI component of an oral PI-Rd triplet for longer than patients receiving intravenous PI-Rd triplets; this may translate into improved TTNT
ANALYSIS OF THE HUMEDICA EMR DATABASE: VRD, KRD, AND IRD IN RRMM
1. Chari A, at al. Blood 2017;130(Suppl 1):abstract 1818 (poster presentation).
Updated data to be presented at ASH 2019
• Chari A, et al: Comparative Effectiveness of Triplets Containing Bortezomib (V), Carfilzomib (K), or Ixazomib (I) Combined with a Lenalidomide and Dexamethasone Backbone (Rd) in Patients with Relapsed/Refractory Multiple Myeloma (RRMM) in Routine Care in the United States (US)
• Program: Oral and Poster Abstracts• Session: 653. Myeloma: Therapy, excluding Transplantation: Poster I
• Saturday, December 7, 2019, 5:30 PM-7:30 PM• Hall B, Level 2 (Orange County Convention Center)

POOLED ANALYSIS FROM THE GREEK, CZECH, AND UK NAMED-PATIENT PROGRAMS
1. Terpos E, et al. Blood 2017;130(Suppl 1):abstract 3087 (poster presentation).
Ixazomib
Aims
Endpoints
Methodology
IMWG, International Myeloma Working Group; ORR, overall response rate
• First oral proteasome inhibitor approved by US Food and Drug Administration and European Medicines Agency• Data limited from real-world environment in Europe
• Evaluate effectiveness and safety of IRd in real-world setting in RRMM patients
• Primary: ORR per IMWG criteria• Secondary: treatment and response duration, adverse events, discontinuation, progression-free survival/time to progression
• Retrospective, observational study of data collected from Greece, the Czech Republic, and the UK• Simple and multiple regression model constructed to determine associations of factors of interest with ORR

POOLED ANALYSIS FROM THE GREEK, CZECH, AND UK NAMED-PATIENT PROGRAMS
RRMM patients who had received ≥1 cycle of IRd N=138
Country, n (%)Greece 35 (25)UK 46 (33)Czech Republic 57 (41)
Median age, years (range) 68 (40–92)Male/female, n (%) 85 (62) / 53 (38)ECOG PS 0–1/2–3, % 72/27Median number of previous therapies, n (range) 1.5 (1–7)1/2/3/4–7 prior lines, n (%) 69 (50) / 42 (30.4) / 20 (14.5) / 7 (5.1)Prior therapies, %
Bortezomib 89.1Thalidomide 46.4Lenalidomide 26.1Pomalidomide 1.4
Prior ASCT, % 26.1
ASCT, autologous stem cell transplant; ECOG PS, Eastern Cooperative Oncology Group performance status 1. Terpos E, et al. Blood 2017;130(Suppl 1):abstract 3087 (poster presentation).

Median DoT 7.2 months (range, 1.0–27.5)
ORR 68.5% (95% CI: 60.5–76.4)
• 76.6% (95% CI: 66.2–86.9) at 2nd line• 60.6% (95% CI: 48.8–72.4) at ≥3rd line• 84.%, 87.0%, and 94.2% in patients receiving IRd for ≥6, ≥7, or
≥8 months, respectively• Odds of achieving ≥PR were 9.5 times greater in patients
receiving IRd for ≥6 versus <6 months• Median time to best response 1.3 months
POOLED ANALYSIS FROM THE GREEK, CZECH, AND UK NAMED-PATIENT PROGRAMS
16.9
10
4.6
39.2
18.5
8.5
2.3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Best response
Pat
ien
ts (
%)
Best response to IRd (N=130): ORR 68.5% (29.3% ≥VGPR)
sCR
CR
VGPR
PR
MR
SD
PD
CR, complete response; MR, minimal response; PR, partial response; sCR, stringent CR; SD, stable disease; VGPR, very good partial response 1. Terpos E, et al. Blood 2017;130(Suppl 1):abstract 3087 (poster presentation).
• Median follow-up 9.1 months

POOLED ANALYSIS FROM THE GREEK, CZECH, AND UK NAMED-PATIENT PROGRAMS
• Median TTP 27.6 months (95% CI: 15.2–27.6)
TTP, time to progression 1. Terpos E, et al. Blood 2017;130(Suppl 1):abstract 3087 (poster presentation).
Median PFS 27.6 months (95% CI: 11.3–27.6)
15Overall PFS time (months)
0 5 10 20 25
3137 80 27 22123 55 19 1299 35 10 0
0
0.2
0.4
0.6
0.8
1.0S
urv
iva
l p
rob
ab
ilit
y
Product–limit survival estimate
with number of subjects at risk
No. at risk
Censored95% confidence limits

POOLED ANALYSIS FROM THE GREEK, CZECH, AND UK NAMED-PATIENT PROGRAMS: SAFETY
AE, adverse event; DVT, deep vein thrombosis 1. Terpos E, et al. Blood 2017;130(Suppl 1):abstract 3087 (poster presentation).
Safety findings N=138
Treatment interruptions, n (%) 12 (8.7)Due to AEs 9 (6.5)
Treatment discontinuation, n (%) 19 (13.7)Due to AEs 10 (7.2)For second ASCT 5 (3.6)For administrative reasons 4 (2.9)
Median time to discontinuation among patients who discontinued, months (IQR) 4.0 (2.4–7.4)Peripheral neuropathy, n (%) 39 (28.3)
Sensory 25 (18.1)Motor 2 (1.4)Unknown type 13 (9.4)Events resolved/continuing (grade 1 or 2), n/39 (%) 15 (38.5) / 24 (61.5)
Pneumonia, n (%) 11 (8.0)Hypertension, n (%) 8 (5.8)DVT, n (%) 5 (3.6)Herpes zoster, n (%) 4 (2.9)Cataracts, n (%) 2 (1.4)Deaths during the study, n (%) 11 (8)
Due to PD, n (%) 4 (2.9)

CONCLUSIONS
• The emerging treatment paradigm of long-term, continuous therapy is improving OS/PFS in the context of MM clinical trials
– However, poorer long-term clinical outcomes have been reported in real-world settings
• Multiple factors affect the translation of clinical trial findings into real-world benefits, including patient burden, burden of administration, access to care, and treatment toxicity
• Real-world findings on the use of novel MM agents are emerging:
– Shorter clinical outcomes for parenteral PI-based combinations have been reported in real-world versus clinical trial settings
• Patient- and disease-related factors should be considered when choosing therapy for RRMM patients in the real-world setting
• There is an ongoing need to further understand the factors affecting the translation of clinical trial efficacy into real-world treatment effectiveness in RRMM