Embed Size (px)
Citation preview

2012.11.30.
1
Overview of Radiation
Protection
Bálint Vecsei dr.
• Every day all over the world people are exposed to ionising radiation, almost all from natural sources in the environment or for medical reasons.
• Ionising radiation has enough energy to cause damage cells which can increase the risk of cancer later in life.
• In general the health effects of ionisingradiation are dependent on the dose received.
Background radiation
2,4-3,4 mSv/year
• Radiation is indispensable in modern
medicine.
• The radiographic examination is one of the
principal diagnostic methods used in all fields
of medical services
• The risk associated with low-level diagnostic
exposures could be expected to be low, but
greater than zero
• For this reason it is prerequisite to measure the dose to the patients in the diagnostic radiologyprecisely.
• the radiation dose to the patients should be as low as reasonably achievable, a principle knownas ALARA (International Commission on Radiological Protection)
• The number of diagnostic examinations shouldalso be taken into consideration because the risk is directly proportional to the frequency of X-ray exposure.

2012.11.30.
2
• Dental radiographic examinations are one of
the most frequently performed radiological
studies.
• The effective dose delivered to patients per
radiograph is low but the collective dose is
significant because of the large number of
radiographs made.
effects of radiation are grouped into
two categories
• Deterministic effects are based on cell killing and are
characterized by a threshold dose. Below the threshold dose
there is no clinical effect. With exposures above the threshold
dose the severity of the injury increases with dose.
• Stochastic effects, including cancer and heritable effects
are based on damage to DNA. There is no-threshold or ‘‘safe’’
dose.
�Persons are medically exposed as part of their diagnostic or treatment
�According to ICRP and BSS, two basic principles of radiation protection are to be complied with: justification and optimization
�Dose limits are not applicable, but a guidance is given on dose levels
� Investigation of exposures is strongly recommended
Three types of exposure
• Medical Exposure
(principally the exposure of
persons as part of their
diagnostic or treatment)
• Occupational Exposure
(exposure incurred at work,
and practically as a result of
work)
• Public Exposure (including all
other exposures)
1 : Overview of Radiation Protection in Diagnostic Radiolog 10
Framework of radiological protection
for medical exposure
• Justification
• Optimization
• The use of doses limits is NOT
APPLICABLE
– Dose constraints and guidance (or
reference) levels ARE RECOMMENDED
Three levels of justification
• General level: The use of radiation in medicine
is accepted as doing more good than harm
• Generic level: specific procedure with a
specific objective (eg. chest radiographs for
patients showing relevant symptoms)
• Third level: the application of the procedure to
an individual patient
12

2012.11.30.
3
Generic justification (I)
• It is a matter for national professional bodies, sometimes in conjunction with national regulatory authorities
• The exposures to staff (occupational) and to members of the public should be taken into account
• The possibility of accidental or unintended exposures (potential exposure) should also be considered
• The decisions should be reviewed from time to time as new information becomes available
13
Justification for an individual patient
(third level)
• To check that the required information is not yet available
• Once the procedure is generically justified, no additional justification is needed for simple diagnostic investigations
• For complex procedures (such as CT, IR, etc) an individual justification should be taken into account by medical practitioner (radiologist, referral doctor..)
14
The optimization of protection (I)
�Optimization is usually applied at two levels:– The design and construction of equipment and installations
– Day to day radiological practice (procedures)
�Reducing the patient dose may reduce the quantity as well as the quality of the information provided by the examination or may require important extra resources
�The optimization means that doses should be “as low as reasonably achievable, economic and social factors being taken into account” compatible with achieving the required objective
15
The optimization of protection (II)
• There is a considerable scope for dose reductions in diagnostic radiology (ICRP 60)
• Simple, low-cost measures are available for reducing doses without loss of diagnostic information (ICRP 60, 34)
• The optimization of protection in diagnostic radiology does not necessarily mean the reduction of doses to the patient
16
Risk and Dosislevels
Risk of different activities (not ordered)
• Atomenergy
• Smoking
• Antibiotics
• X-ray diagnostic
• Electrocity
• Cycling
• Food preservation
• Automobile
• Consumtion of alcoholic drinks

2012.11.30.
4
Risk of different activities (increasing risk)
• Smoking
• Consumtion of alcoholic drinks
• Automobile
• Electrocity
• X-ray diagnostic
• Cycling
• Atomenergy
• Food preservation
• Antibiotics
1 micro-risk
• 2500 km travel by train
• 2000 km flight
• 80 km by bus
• 65 km by car
• 12 km by bike
• 3 km by motor bike
• smoke of one cigarette
• 2 month living together with a smoker
• eat one more bread and butter for a fat man
• breath 1 hour in Budapest
• sleep in a house one week
• to be stroked by thunder in 10 years
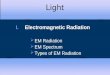
Risk
• Monument in gardenof St. Georg Hospitalin Hamburg, Germany
• Fast spread of x-raymachines
• Use of the technique without knowing the nature of this radiation
• Why?
(EMF, Nano)
Application of x-ray.
• „It is safer to see, than feel.” (Motto)
►Shoe-store►Advertisement
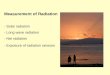
Development in Radiology
Veins on a segmented CT 3D image
Development in Radiology
• 16 slices CT
(best: over 256 slices)
1917

2012.11.30.
5
Development in Radiaton protection
Benifit
Benifit and risk
Benifit Risk
Benifit and riskOverview of dose quantities
Physical
effect
Chemical
effect
Bio-chemical
effect
Biological
effect
Radiation
Absorbed dosis
Equivalent dose
Effective dose
RISK
• Reflects the combined detriment from stochastic effects due to
the equivalent doses in all the organs and tissues of the body
• The combination of probability and severity of harm is called
“detriment”.
Estimated lifetime risk as a function of ageRisk
• Risk = (amount of harm) x (probability of harm)

2012.11.30.
6
Risk
• We always run a risk for some benifit
• There is hardly any activity without risk
Risk
• We always run a risk for some benifit
• There is hardly any activity without risk
Risk
• Risk = (amount of harm) x (probability of harm)
Example: Having a job
Benifit: basis for the existence
Loss: harms, accidences, death at work place
Can we know the risk of our job/profession?
Probability ~ number of accidents / all workers
of an acciedent
Risk ~ Probability of an acciedent x losses per accident
Risk in industry
manufacture of clothes, shoes
<0,00001
Paper-, food-, metal-, textile-, shipping, building industry
0,00001-0,0001
Coal industry and pottery 0,001-0,001
Airplan crew, marine fisherman
0,001-0,01
Mustard-gas-, naphtylamin producer
>0,01
Extra-risk of Chernobyl in Hungary
Plus dose: 0,2 mSv / 30 Years
Probability of plus cancer: 0,00001
• First way to communicate:"30 years of it's radiation in Hungary is as much as 1 month of natural background radiation."
• Second way to communicate:"The extra-risk is as much as to smoke 1 cigarette, or 60 km of auto-driving."
• Third way to communicate:"The radiation of Chernobyl killed 100 people in Hungary.”
(0,00001*10 000 000 = 100)
We live with1-3 mSv
Can kill4000 mSv
Radiation
Where to stop, where is the safe point?What are the effects of radiation?

2012.11.30.
7
• Medical Exposure
(principally the exposure of persons as
part of their diagnostic or treatment)
• Occupational Exposure
(exposure incurred at work, and practically
as a result of work)
• Public Exposure
(including all other exposures)
Three types of exposure Medical exposure
• Medical Exposure
– Exposure of persons as part of their diagnostic or treatment
– Exposures (other than occupational) incurred knowingly and willingly by individuals such as family and close friends helping either in hospital or at home in the support and comfort of patients
– Exposures incurred by volunteers as part of a program of biomedical research
Changes in Dose Limit (ICRP)
mSv
Year
Dose constraints for medical exposure
• For medical exposure dose constraints should
only be used in optimizing the protection of
persons exposed for medical research
purposes, or of persons, other than workers,
who assist in the care, support or comfort of
exposed patients.
40
Dose constraints
• for medical research purposes
• for individuals helping in care, support or comfort of patients, and visitors
– 5 mSv during the period of the examination or treatment
– 1 mSv for children visiting
1 : Overview of Radiation Protection in
Diagnostic Radiology41
PUBLIC - Optimization under
Constraints
• DOSE LIMITS
• effective dose of 1 mSv in a year
• in special circumstances, effective dose of 5 mSv in a single year, provided that the average over five consecutive years in less than 1mSv per year
• equivalent dose to lens of the eye 15 mSv in a year
• equivalent dose to skin of 50 mSv in a year.
42

2012.11.30.
8
Occupational dose limits
• 100 mSv/5 years effective dose
• BUT does not allowed over 50 mSv in any
year!
Occupational Public
Effective dose 20 mSv/yr averaged* 1 mSv in a yr
over 5 yrs.
Annual equivalent
dose to
► Lens of eye 150 mSv 15 mSv
► Skin 500 mSv 50 mSv
► Hands & Feet 500 mSv
N.B.: M.P.D. 1931 = 500 mSv, 1947=150 mSv, 1977=50 mSv &
in 1990=20 mSv
Dose Limits (ICRP 60)
Students, trainee
Effective dose 1 mSv/yr averaged*
Annual equivalent
dose to
► Lens of eye 150 mSv
► Skin 50 mSv
► Hands & Feet 150 mSv
N.B.: M.P.D. 1931 = 500 mSv, 1947=150 mSv, 1977=50 mSv &
in 1990=20 mSv
Dose Limits (ICRP 60) Guidance levels for diagnostic radiography (typical adult patient)
ExaminationEntrance surface dose per radiograph (mGy)
Thoracic spine AP 7
Thoracic spine LAT 20
Dental peri-apical 7
Dental AP 5
46
Guidance levels for diagnostic radiography (typical adult patient)
ExaminationEntrance surface dose per radiograph (mGy)
Skull AP 5
Skull LAT 3
Dose values are in air with backscatter. They are for conventional film-screen combination (200 speed class). For higher speed film-screen combinations (400-600), the
values should be reduced by a factor of 2 to 3.
1 : Overview of Radiation Protection in Diagnostic
Radiology47
Typical effective doses from diagnostic
medical exposures
48
From: Referral Criteria For Imaging. CE, 2000.
Diagnostic
procedure
Typical effective dose
(mSv)
Equiv. no. of chest x-rays
Approx. equiv. period of natural background
radiation
Chest (single PA film)
0.02 1 3 days
Skull 0.07 3.5 11 days
Thoracic spine 0.7 35 4 months
Lumbar spine 1.3 65 7 months

2012.11.30.
9
Typical effective doses from diagnostic
medical exposures
1 : Overview of Radiation Protection in
Diagnostic Radiology49
Diagnostic
procedure
Typical effective dose
(mSv)
Equiv. no. of chest x-rays
Approx. equiv. period of natural background
radiation
CT head 2.3 115 1 year
CT chest 8 400 3.6 years
CT Abdomen or pelvis
10 500 4.5 years
From: Referral Criteria For Imaging. CE, 2000.
Comparison of doses from sources of exposure
Source of Exposure Dose
Dental X-ray 0.005 mSv
135g bag of Brazil nuts 0.005 mSv
Chest X-ray 0.02 mSv
Transatlantic flight 0.07 mSv
Nuclear power station worker average annual occupational exposure 0.18 mSv
UK annual average radon dose 1.3 mSv
CT scan of the head 1.4 mSv
UK average annual radiation dose 2.7 mSv
USA average annual radiation dose 6.2 mSv
CT scan of the chest 6.6 mSv
Average annual radon dose to people in Cornwall 7.8 mSv
Whole body CT scan 10 mSv
Annual exposure limit for nuclear industry employees 20 mSv
Level at which changes in blood cells can be readily observed 100 mSv
Acute radiation effects including nausea and a reduction in white blood cell count 1000 mSv
Dose of radiation which would kill about half of those receiving it in a month 5000 mSv
Summary
• Exposure of patients as part of their diagnostic or treatment, has to be justified
• Optimization of patient exposures means keeping doses to a minimum without loss of diagnostic information
• Guidance dose levels are defined to serve as a reference for medical practitioners: if a level is exceeded some specified action or decision should be taken
• Guidance (reference) levels are not dose limits.
1 : Overview of Radiation Protection in
Diagnostic Radiology51
Personal Dosimetry
�Personal dosimetry provides the means tomeasure and record radiation doses received byindividual workers.
�Personal dosemeters should be worn byoperators who take more than 100 intra-oralfilms or 50 panoramic films per week.
�In practice, the majority of dentists and supportstaff do not need to wear dosemeters althoughmany do so as a reassurance measure.