Embed Size (px)
Citation preview

Clark 2017
1
©2016 MFMER | slide-1
Motor SpeechIn Acute and Degenerative Conditions
Heather M Clark, Ph.D. CCC/SLP, BC-ANCDS
Iowa Conference on Communicative DisordersApril 2017
©2016 MFMER | slide-2
Disclosures
• Financial and non-financial conflicts of interest• Salary from Mayo Clinic• Book royalties received from Pro-Ed (book topic unrelated to this talk)
• Grant support• National Institute of Neurological Disorders and Stroke
• National Institute on Deafness and Other Communication Disorders
• National Institutes of Health
©2016 MFMER | slide-3
Outline
• Overview of Dysarthria and AOS
• Clinical features• Neurologic substrates
• Motor Speech Assessment
• Overview of assessment
• Consideration of chronicity
• Motor Speech Treatment• Guiding frameworks• Consideration of
chronicity• Standardized
treatment protocols• Comprehensibility
strategies
©2016 MFMER | slide-4
Overview of Motor Speech Disorders
©2016 MFMER | slide-5
Dysarthria
©2016 MFMER | slide-6
Dysarthria
Neurologic speech disorder reflecting abnormalities in the strength, speed, range, steadiness, tone, or accuracy of movements required for respiratory, phonatory, resonatory, articulatory, or prosodic aspects of speech production
Duffy, 2013

Clark 2017
2
©2016 MFMER | slide-7
Flaccid Dysarthria
• Features relate to muscle weakness• Often asymmetric
• Specific features depend on LMNs involved and/or pathophysiology
• Consistent features vs rapid fatigue/recovery with rest
©2016 MFMER | slide-8
Flaccid dysarthria
CranialNerve
Speech Features
V Does not typically impact speech unless severe bilateral deficit
VII Unilateral: unlikely to significantly impact speech, perhaps subtle
XPh Hypernasality
XSL Low pitch, monopitch
XRL Breathiness, diplophonia, short phrases
XII Imprecise articulation
©2016 MFMER | slide-9
Spastic dysarthriaSubsystem/Domain Speech Features
Respiration Short phrases
Phonation Strained, strangled
Resonance Hypernasality
Articulation Imprecise
Prosody Slow rateMonopitch, monoloudness
©2016 MFMER | slide-10
Ataxic dysarthriaSubsystem/Domain
Speech Features
Respiration Excessive loudness variation
Phonation May be harsh
Resonance Often normal, otherwise may be variable
Articulation Irregular articulatory breakdowns
Prosody Slow rateScanning speechExcess and equal stress
Other “drunken” quality
©2016 MFMER | slide-11
Hypokinetic dysarthriaSubsystem/Domain
Speech Features
Respiration Reduced loudness
Phonation Tight breathiness
Resonance Often normal
Articulation Imprecise, usually with reduced ROM during speech movements
Prosody Rapid rateShort rushes of speechMonopitch, monoloudness
Other Palilalia“Mumbling” quality
©2016 MFMER | slide-12
Hyperkinetic dysarthriaSubsystem/Domain
Speech Features
Respiration InterruptionsExcessive loudness variations
Phonation StrainTremorVoice interruptions
Resonance Constant or variable
Articulation DistortionsInterruptions
Prosody Often slow
Other Visual features often prominent

Clark 2017
3
©2016 MFMER | slide-13
UUMN dysarthriaSubsystem/Domain Speech Features
Respiration Reduced loudness*
Phonation Weak, strained, or hoarse
Resonance Hypernasal*
Articulation ImpreciseIrregular breakdowns
Prosody Slow (or normal) rateReduced stress*
Other*Particularly in the context of reduced background physiologic effort
Can be perceptually similar to flaccid, spastic, and/or ataxic dysarthria
©2016 MFMER | slide-14
Mixed dysarthria
• Any combination of the above
©2016 MFMER | slide-15
Apraxia of Speech
©2016 MFMER | slide-16
Apraxia of Speech
• AOS is a disturbance in the programming of movements for speech
• muscles are capable of normal functioning (right-sided weakness secondary to UMN dysarthria may be seen)
• appropriate message has been formulated
©2016 MFMER | slide-17
Most agree that…
• AOS is distinct from dysarthria• Which involves impairments in speed,
strength, coordination, or muscle tone affecting all movements
• AOS is distinct from aphasia• Which involves impairments in manipulation
(comprehension & expression) of linguistic symbols
• AOS is distinct from nonverbal oral apraxia
©2016 MFMER | slide-18
Speech Characteristics (Duffy 2013)
• Articulatory
• Rate and Prosody
• Fluency

Clark 2017
4
©2016 MFMER | slide-19
Articulatory Characteristics
• Consonant and vowel distortions (imprecise articulation)
• Distorted substitutions• Perseverative• Anticipatory
• Distorted additions
• Distorted sound prolongations
• Voicing errors
• Relatively consistent error type and location
©2016 MFMER | slide-20
Rate and Prosodic Characteristics
• Slow overall rate, especially for longer utterances
• Prolonged but variable vowel duration and inter-word intervals
• Syllable segmentation
• Errors of stress assignment
• Reduced words per breath group relative to MPT
• Decreased phonetic accuracy with rate increases
©2016 MFMER | slide-21
Fluency Characteristics
• Attempts to self-correct articulatory errors
• False starts and restarts
• Visible and audible groping for articulatory postures
• Sound and syllable repetitions
©2016 MFMER | slide-22
Influence of Task Variables
• Syllabicity effects• Increased errors
• Low frequency syllables• Syllables with more phonemes• Consonant clusters within syllables
• Increased errors with more phonemes and/or more syllables (complexity)
• Volitional/purposeful utterances have more errors than automatic/reactive utterances
©2016 MFMER | slide-23
Influence of Task Variables
• Higher error rates in nonsense syllables
• Higher error rates in consonant clusters
• Initiation of utterances is particularly difficult
• Imitation does not generally elicit more errors than are present in spontaneous speech of equal complexity
©2016 MFMER | slide-24
Severe AOS
• Limited repertoire of speech sounds
• Limited variety of utterances
• May be reflected by muteness
• Usually accompanied by severe aphasia and nonverbal oral apraxia

Clark 2017
5
©2016 MFMER | slide-25
Motor Speech Assessment
©2016 MFMER | slide-26
Differential diagnosis
“When do you give
an aphasia battery?
When you already know the patient has aphasia”
- Joe Duffy
©2016 MFMER | slide-27
Motor Speech Assessment for Differential Diagnosis
• History
• Perceptual assessment of continuous speech
• Speech-like tasks
• Examination of oral structure and function
©2016 MFMER | slide-28
Medical HistoryInformation Key Indicators or
FindingsRelevance for Communication
Current diagnosis and past medical history (PMH)
1. Neurologic2. Pulmonary3. ENT
1. Predict impairments and inform prognosis and tx plan
2. May account for respiratory impairments affecting speech
3. May account for voice impairments affecting speech
Medications 1. Sedatives2. Antihypertensives,
antihistamines, diuretics
3. Carbidopa levadopa
1. Lethargy may influence communication function
2. May affect vocal quality
3. Timing of medication may influence performance
Imaging 1. Head CT or MRI 1. Site of lesion may predict impairments and differential diagnosis
Reports from other disciplines
1. Nursing2. Physical medicine
1. Usually indicate level of alertness and ability to communicate basic needs
2. May indicate ability to participate in therapeutic intervention
©2016 MFMER | slide-29
Interview – Onset & CourseQuestion Purpose
Describe the changes in your speech
Some descriptions occur more frequently in with specific motor speech disorders• “Mumbling” – hypokinetic• Slow and effortful – spastic dysarthria, AOS• Tongue is thick – flaccid• Can’t pronounce words, “trip” over words – AOS • Sound drunk - ataxic
When did the problem start?Gradual or sudden?
Suggests possible etiologies
Change since onset? Improving or worsening symptoms suggests possible etiologies
Improvement with therapy Responsiveness to intervention may suggest underlying impairment
Duffy, 2013
©2016 MFMER | slide-30
Interview – Associated Deficits
Question Purpose
Other symptoms (beginning at the same time, prior to, or after development of speech difficulties)?• Cognitive/linguistic• Swallowing/drooling• Gait/balance• Weakness/coordination
“Company it keeps” may suggest etiology
• Changes in emotional expression Flattened affect: hypokinetic dysarthriaPseudobulbar affect: spastic dysarthria
Duffy, 2013

Clark 2017
6
©2016 MFMER | slide-31
Speech Functions
©2016 MFMER | slide-32
Speech Functions - Tasks
• Connected speech• Reading• Picture description• Conversation
• Repetition• Single words• Sentences
• Automatic sequences
©2016 MFMER | slide-33
Speech-like Tasks
©2016 MFMER | slide-34
Speech-like tasks
• Alternate motion rates (AMRs)
• Sequential motion rates (SMRs)
• Prolonged vowel (maximum phonation time/MPT)
©2016 MFMER | slide-35
AMRs
Feature Relevance for Differential Diagnosis
Slow and regular Spastic
Irregular (slow or normal rate) Ataxic
Rapid/blurred Hypokinetic
Normal rate, imprecise Flaccid
Voicing errors Spastic
©2016 MFMER | slide-36
AMRs

Clark 2017
7
©2016 MFMER | slide-37
SMRsFeature Relevance for Differential Diagnosis
Better than AMRs Ataxic
Worse than AMRs AOS
©2016 MFMER | slide-38
Nonspeech Tasks
©2016 MFMER | slide-39
Nonspeech FeaturesFeature Relevance for Differential Diagnosis
Weakness Most apparent in LMN (flaccid) & UMN (UUMN/spastic)Subtle in hypokineticUnusual in ataxic
0
10
20
30
40
50
60
70
80
Pre
ssu
re (
kPa)
©2016 MFMER | slide-40
Nonspeech FeaturesFeature Relevance for Differential Diagnosis
Reduced ROM During isolated movements: can reflectweakness or spasticity
Only during rapid alternating movements: common in hypokinetic
Reduced speed Most apparent in spasticityPossible but not typical in flaccid
Atrophy LMN
Fasciculations LMN
Pathologic or exaggerated reflexes
UMN
Hypomimia Hypokinetic
Adventitious movements Hyperkinetic, functional
©2016 MFMER | slide-41
Assessment Consideration of Chronicity
©2016 MFMER | slide-42
Assessment across the continuum of care
• Timing/setting influences many aspects of assessment
• Purpose• Time available• Patient and family insight• Nature of confounding factors
Clark 2017
8
©2016 MFMER | slide-43
Assessment in Acute Care
©2016 MFMER | slide-44
Acute Care: Purpose
• Differential diagnosis
• Identification of reliable mode of communication
• Discharge planning
©2016 MFMER | slide-45
Acute Care: Time Available
• Patient available for assessment
• Patient awake and alert for assessment
©2016 MFMER | slide-46
Acute Care: Patient and family insight
• Description of the problem by patient and family not necessarily particularly helpful at this point
• May have identified an effective mode of communication
• Concern will be survival and (later) disability
• This may be the first time the patient or family has ever heard of dysarthria or AOS
©2016 MFMER | slide-47
Acute Care: Confounding factors
• Coma, delirium, encephalopathy, somnolence
• Baseline cognitive impairments
• Pain
• Hemiplegia
• Visuo-perceptual deficits
• Hearing loss
• Positioning
• Presence of NG, endotracheal tubes, trachs
©2016 MFMER | slide-48
Assessment in Chronic Phase
Clark 2017
9
©2016 MFMER | slide-49
Purpose
• Confirm diagnosis
• Obtain a thorough characterization of the motor speech disorder
• Probe for facilitating contexts
©2016 MFMER | slide-50
Purpose
• Develop a prognosis for improvement with therapy and/or
• Develop recommendations for maximizing communicative effectiveness
©2016 MFMER | slide-51
Purpose
• The task is usually to address communication difficulties that
• Have never been treated• Have been treated inappropriately• Have been treated appropriately but may
benefit from a different approach• Have been treated optimally but patient and
family have not effectively adapted to the “new normal”
©2016 MFMER | slide-52
Chronic: Time Available
• Often relatively extensive
Although probably never as much as is available in training settings
©2016 MFMER | slide-53
Chronic: Patient and family insight
• Description of the problem by patient and family is invaluable at this point
• Impact on work, personal, and social interactions
• Effective strategies• Challenging contexts
©2016 MFMER | slide-54
Chronic: Patient and family insight
• What have they been told the communication problem is called?
• Question is usually whether additional therapy could be helpful
• They may or may not have experience yet with ICF-guided therapy (more on this later)

Clark 2017
10
©2016 MFMER | slide-55
Chronic: Confounding factors
• Concomitant deficits• Pain• Hemiplegia• Visuo-perceptual deficits• Hearing loss• Aphasia• Cognitive impairments• Fatigue
• Maladaptive patterns
©2016 MFMER | slide-56
Chronic: Confirm Diagnosis
• Thorough motor speech exam and evaluation for common co-occurring difficulties
• If you are confident about previously established diagnoses, it may be possible to screen for other deficits and then use most of the time for comprehensive assessment of motor speech
• Consider the relative contribution of motor speech disorders to overall communicative effectiveness
©2016 MFMER | slide-57
Assessment of Progressive Motor Speech Disorders
©2016 MFMER | slide-58
Progressive: Purpose
• Differential diagnosis
• Characterization of concomitant communication disorders
©2016 MFMER | slide-59
Progressive AOS: Characterization
• Classifying Type of Progressive AOS
• Articulatory distortions predominate
• Segmentation predominates
• Distortions and segmentation are of equal severity
©2016 MFMER | slide-60
Progressive: Time Available
• Initial session for differential diagnosis
• Subsequent sessions likely needed for further characterization
Clark 2017
11
©2016 MFMER | slide-61
Progressive: Patient and family insight
Description of the problem by patient and family is invaluable
• Nature• Complaints of change in voice, difficulty with
pronunciation or enunciation, “tripping” over words, “can’t get words out”
• With or without complaints of aphasia• Gradual onset and worsening over time
• Impact on work, personal, and social interactions
• Effective strategies• Challenging contexts
©2016 MFMER | slide-62
Progressive: Patient and family insight
• What have they been told the communication problem is called?
• They will want to know if therapy can reverse the problem.
©2016 MFMER | slide-63
Progressive: Confounding factors
• Concomitant aphasia and/or cognitive communicative deficits
• Limb apraxia
©2016 MFMER | slide-64
Treatment of Motor Speech Disorders
©2016 MFMER | slide-65
General Considerations
• Concomitant conditions• NVOA may be present but likely will not
warrant treatment• Nonspeech oral motor activities not used at
all except to shape towards speech in the setting of muteness
• Severity
• Guiding frameworks
©2016 MFMER | slide-66
Management of Motor Speech DisordersConsidering Chronicity

Clark 2017
12
©2016 MFMER | slide-67
Acute Care
• Goals• Identifying or establishing reliable mode of
communication• Discharge planning
• For prolonged stays• On-going assessment as medical status
fluctuates• May be able to move forward with
rehabilitative goals
©2016 MFMER | slide-68
Early rehabilitation
• Goals• Restoration of function• Optimizing activity, participation, quality of
life• Comprehensibility strategies• Home and work modifications• Conversation partner training
©2016 MFMER | slide-69
Chronic Motor Speech Disorders
• One task is to justify treatment • Involves identifying communication
difficulties that• Have never been treated
• Have been treated inappropriately
• Have been treated appropriately but may benefit from a different approach
• Have been treated optimally but patient and family have not effectively adapted to the “new normal”
• Much of the highest quality evidence supporting treatment of dysarthria & AOS is the setting of chronic conditions
©2016 MFMER | slide-70
Chronic Motor Speech Disorders
• Goals• Restoration of function• Optimizing activity, participation, quality of life
• Comprehensibility strategies• Home and work modifications• Conversation partner training
©2016 MFMER | slide-71
Progressive Motor Speech Disorders
• Goals• Restoration (?), maintenance, and slowed decline, of
function• Optimizing activity, participation, quality of life
• Comprehensibility strategies• Home and work modifications• Conversation partner training
©2016 MFMER | slide-72
Frameworks Guiding Decision Making

Clark 2017
13
©2016 MFMER | slide-73
ICFFrameworks Guiding Decision Making
©2016 MFMER | slide-74
International Classification of Function: ICF
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
World Health Organization, 2001
©2016 MFMER | slide-75
Health Condition
Disorder or disease
Informs• Prognosis
• Predicted comorbidities
• Tolerance for specific modalities
Treatment of motor speech disorders associated with neurodegenerative disease may differ from acute or chronic disease
• Goals
• Time course• Relatively frequent during
establishment of skills or strategies
• Relatively infrequent re-evaluation with updated recommendations
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
©2016 MFMER | slide-76
Body Functions and Structures
Underlying impairments of or changes to anatomical structures or physiologic functions
In motor speech disorders, impairments are often described at the level of muscle or nerve impairment (e.g., weakness) or at the level of subsystem (e.g., impairments of voice)
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
©2016 MFMER | slide-77
Activity and Participation
Describes the impact of health conditions, impairments, and contextual factors on performance of and participation in functional activities
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
©2016 MFMER | slide-78
Contextual Factors
Personal factors• Age
• Life experiences
• Personality
• Co-morbidities‒ Speakers with dysarthria often
have concomitant impairments in speech praxis, language, cognition, and/or swallowing functions
Environmental factors• Technology
• Geography
• Support and relationships
• Attitudes
• Services
• Systems and policies
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
Clark 2017
14
©2016 MFMER | slide-79
Application: ICF
• Differential diagnosis• Mixed hypokinetic-hyperkinetic-spastic
dysarthria• Apraxia of speech• Cognitive communicative impairment
• Medical diagnosis• Corticobasal syndrome
©2016 MFMER | slide-80
Application: ICF
Recommendation Rationale
Environmental modifications to maximize signal to noise ratio
• Increasing loudness exacerbated phonatory strain
Conversation partner strategies
• Cognitive deficits make it difficult for patient to use intentional strategies
• Include strategies addressing reduced output related to cognitive deficits
©2016 MFMER | slide-81
Motor Speech Treatment HierarchyFrameworks Guiding Decision Making
©2016 MFMER | slide-82
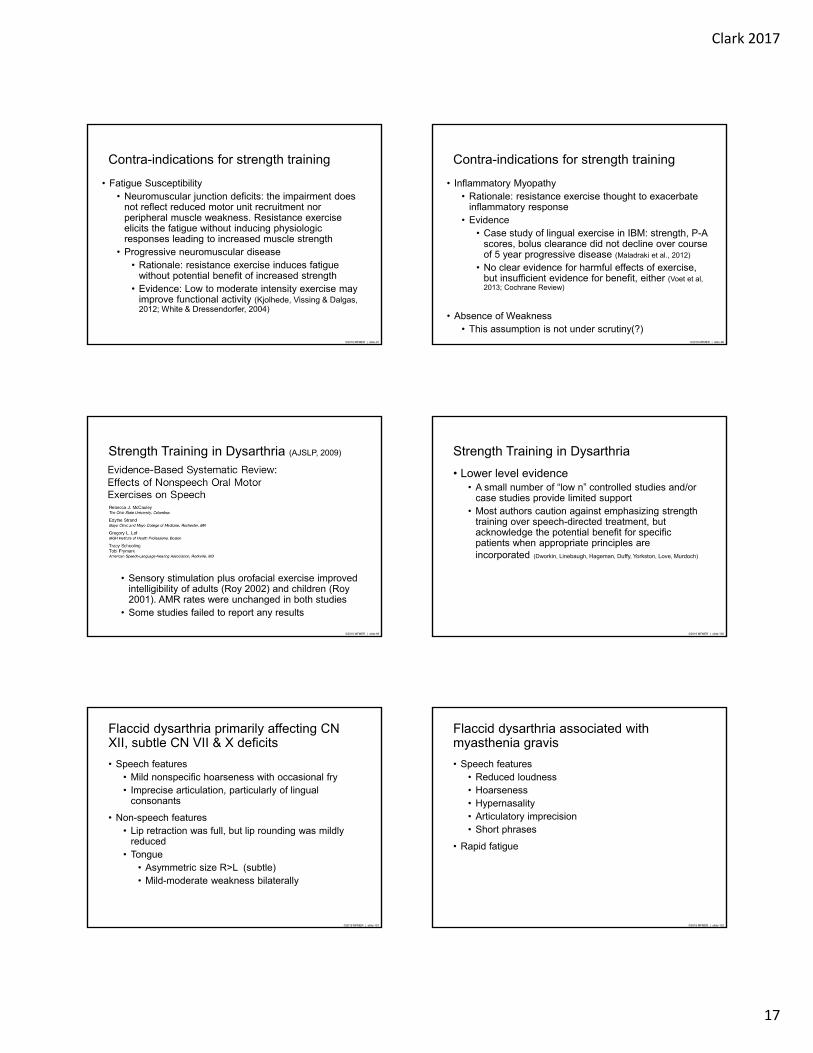
Speech Subsystems
Respiration
Phonation
ResonationArticulation
Prosody
©2016 MFMER | slide-83
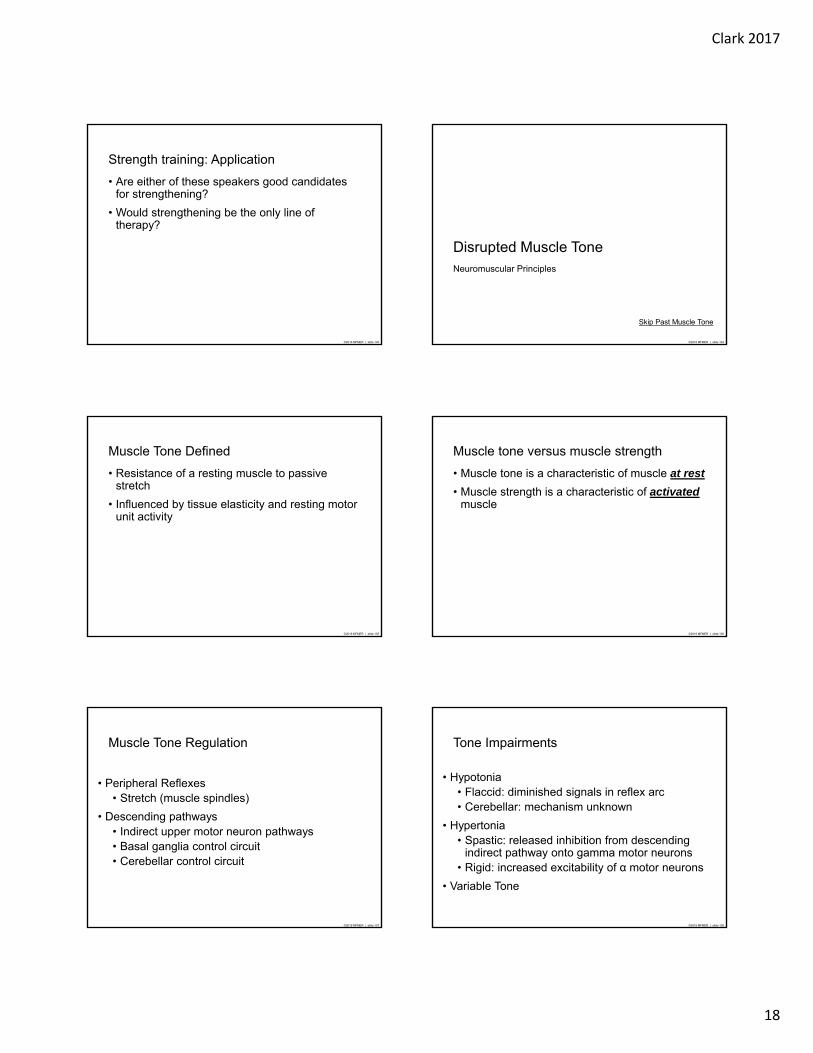
Motor Speech Treatment Hierarchy
• The speech subsystems do not act independently
• Adequate respiratory support and velopharyngeal valving supports phonation
• Articulatory precision is supported by respiratory, resonatory, and phonatory competence
Dworkin, 1991©2016 MFMER | slide-84
First Order Targets
Second Order Targets
Third Order Targets
Articulation
Phonation
Respiration Resonation
Prosody
Motor Speech Treatment Hierarchy
Dworkin, 1991

Clark 2017
15
©2016 MFMER | slide-85
First Order Targets: Respiratory support
(diaphragmatic breathing)
Loudness (e.g.,LSVT)
Third Order Targets: Overenunciation Articulation
Phonation
Respiration Resonation
Prosody
Application: Motor Speech Treatment Hierarchy
Prosody targets: Lexical stress
Slow rate
©2016 MFMER | slide-86
Neuromuscular Treatment PrinciplesFrameworks Guiding Decision Making
©2016 MFMER | slide-87
Strength
• Weakness• Maximum force (strength;1Rmax)• Sustained/repeated submaximal force
(endurance)• Power (near maximal forces at high speed)
• Causes• UMN lesion (UUMN and spastic dysarthria)• LMN lesion (flaccid dysarthria)• Disuse atrophy & deconditioning (all
dysarthrias)
©2016 MFMER | slide-88
Strength Training Principles
• Overload & Progression
• Intensity
• Recovery
• Reversibility
• Specificity of Training
©2016 MFMER | slide-89
Overload & Progression
• Overload• Taxing the muscles beyond typical
functioning• Results in
• Hypertrophy of muscle tissue• Increased motor unit recruitment
• Progression• Systematic overload• Implies need for regular reassessment of
maximum performance
©2016 MFMER | slide-90
Intensity
• Strength training• 60-80% 1Rmax
• 10 repetitions per set• 2-3 sets
• Endurance training
• 40-60% 1Rmax
• High number of repetitions (e.g., 60)

Clark 2017
16
©2016 MFMER | slide-91
Recovery
• Optimal interval between training sessions to allow recovery yet avoid reversal
• In large muscle groups, optimal interval is > 24 hrs
• Tongue strengthening studies: 3-7 days/week
• Respiratory muscle strengthening studies: 3-5 days/week
©2016 MFMER | slide-92
Reversibility
• “Use it or lose it”
• Levels of strength must be used to be maintained
©2016 MFMER | slide-93
Specificity of Training
• The effects of strength training are highly specific to the trained behaviors
• Transference refers to the gains in function for tasks that do not perfectly match the exercise
©2016 MFMER | slide-94
Movement factors subject to specificity
• Force
• Contraction velocity
• Duration
• Dynamics
• Integration
©2016 MFMER | slide-95
Integration
• Results of motor learning experiments suggest that motor programs (specific patterns of motor unit recruitment) are highly specific
• Predicts that exercises that incorporate the entire movement pattern (e.g., all articulators) will result in greatest carryover
©2016 MFMER | slide-96
Contra-indications for strength training
• Hypertonia• Rationale: High resistance exercise presumed to
increase spasticity, arose from principles of the Bobathapproach
• Evidence has failed to support this presumption• Stroke (Pak & Patten, 2008)
• Cerebral palsy (Dodd, Taylor & Damiano, 2002; Scholtes et al, 2012)
• MS (in combination with anti-spasticity medications; Motl, Snook & Hinkle, 2007)
• ALS (Ashworth, Satkunam, & Deforge, 2012 Cochrane Review)
Clark 2017
17
©2016 MFMER | slide-97
Contra-indications for strength training
• Fatigue Susceptibility• Neuromuscular junction deficits: the impairment does
not reflect reduced motor unit recruitment nor peripheral muscle weakness. Resistance exercise elicits the fatigue without inducing physiologic responses leading to increased muscle strength
• Progressive neuromuscular disease• Rationale: resistance exercise induces fatigue
without potential benefit of increased strength• Evidence: Low to moderate intensity exercise may
improve functional activity (Kjolhede, Vissing & Dalgas, 2012; White & Dressendorfer, 2004)
©2016 MFMER | slide-98
Contra-indications for strength training
• Inflammatory Myopathy• Rationale: resistance exercise thought to exacerbate
inflammatory response• Evidence
• Case study of lingual exercise in IBM: strength, P-A scores, bolus clearance did not decline over course of 5 year progressive disease (Maladraki et al., 2012)
• No clear evidence for harmful effects of exercise, but insufficient evidence for benefit, either (Voet et al, 2013; Cochrane Review)
• Absence of Weakness• This assumption is not under scrutiny(?)
©2016 MFMER | slide-99
Strength Training in Dysarthria (AJSLP, 2009)
• Sensory stimulation plus orofacial exercise improved intelligibility of adults (Roy 2002) and children (Roy 2001). AMR rates were unchanged in both studies
• Some studies failed to report any results
©2016 MFMER | slide-100
Strength Training in Dysarthria
• Lower level evidence• A small number of “low n” controlled studies and/or
case studies provide limited support• Most authors caution against emphasizing strength
training over speech-directed treatment, but acknowledge the potential benefit for specific patients when appropriate principles are incorporated (Dworkin, Linebaugh, Hageman, Duffy, Yorkston, Love, Murdoch)
©2016 MFMER | slide-101
Flaccid dysarthria primarily affecting CN XII, subtle CN VII & X deficits
• Speech features• Mild nonspecific hoarseness with occasional fry • Imprecise articulation, particularly of lingual
consonants
• Non-speech features• Lip retraction was full, but lip rounding was mildly
reduced • Tongue
• Asymmetric size R>L (subtle)• Mild-moderate weakness bilaterally
©2016 MFMER | slide-102
Flaccid dysarthria associated with myasthenia gravis
• Speech features• Reduced loudness• Hoarseness• Hypernasality• Articulatory imprecision• Short phrases
• Rapid fatigue
Clark 2017
18
©2016 MFMER | slide-103
Strength training: Application
• Are either of these speakers good candidates for strengthening?
• Would strengthening be the only line of therapy?
©2016 MFMER | slide-104
Disrupted Muscle ToneNeuromuscular Principles
Skip Past Muscle Tone
©2016 MFMER | slide-105
Muscle Tone Defined
• Resistance of a resting muscle to passive stretch
• Influenced by tissue elasticity and resting motor unit activity
©2016 MFMER | slide-106
Muscle tone versus muscle strength
• Muscle tone is a characteristic of muscle at rest
• Muscle strength is a characteristic of activated muscle
©2016 MFMER | slide-107
Muscle Tone Regulation
• Peripheral Reflexes• Stretch (muscle spindles)
• Descending pathways• Indirect upper motor neuron pathways• Basal ganglia control circuit• Cerebellar control circuit
©2016 MFMER | slide-108
Tone Impairments
• Hypotonia• Flaccid: diminished signals in reflex arc• Cerebellar: mechanism unknown
• Hypertonia• Spastic: released inhibition from descending
indirect pathway onto gamma motor neurons• Rigid: increased excitability of α motor neurons
• Variable Tone

Clark 2017
19
©2016 MFMER | slide-109
Muscle Spindle Action in Speech/Swallowing Muscles
• Jaw closing muscles• High density muscle spindles• Strong stretch reflex
• Face & lips• Low density or lack of muscle spindles• Do not exhibit stretch reflexes
©2016 MFMER | slide-110
Muscle Spindle Action in Speech/Swallowing Muscles
• Tongue • Muscle spindle density similar to limbs• Do not exhibit typical stretch reflexes • (Neilson et al., 1979)
• Palate, Pharynx, Larynx• Presence of muscle spindles varies across muscles• No studies to date have demonstrated stretch reflexes in the
human larynx (Ludlow, 2005) or pharynx
©2016 MFMER | slide-111
Assessment of Muscle Tone: Clinical
• Passive displacement of relaxed limb• Modified Ashworth Scale (6-point scale)
• Muscle palpation• Feel for resistance to tissue deformation
©2016 MFMER | slide-112
Clinical Assessment ofMuscle Tone: Speech musculature
• Observation of resting position• Facial droop• Lip retraction
• Orofacial tone assessments• Dworkin & Culatta (1996)• Beckman (1988)
©2016 MFMER | slide-113
Proximal Muscle Groups
Velum and pharynx• Slow, symmetrical movements may indicate
hypertonia• Droop, often asymmetrical, may indicate
hypotonia
• Larynx• Hypertonicity typically has bias for
hyperadduction (strained, strangled vocal quality)
©2016 MFMER | slide-114
Evidence for Tone Impairments inDysarthriaDysarthria Hypothesized (Darley,
Aronson, Brown, 1969)
Data
Flaccid Flaccid hypotonia Flaccid: hypotonia (Solomon & Clark, 2010)
Spastic Spastic hypertonia Spastic: No hyperactive stretch reflexes in the tongue in spastic dysarthria (Nielson et al., 1979)
Ataxic Normal None
Hypokinetic Rigid hypertonia Hypokinetic: Increased lip stiffness (Hunker, Abbs, & Barlow, 1982; Chu et al., 2010)
Hyperkinetic Dystonic/variable None

Clark 2017
20
©2016 MFMER | slide-115
Management of Tone Impairments
• Pharmacologic• Spasticity
• Muscle relaxants (e.g., Baclofen)
• Muscle paralytics (e.g., botulinum toxin)
• Rigidity• Levodopa
• Surgical• Spasticity
• Tendon lengthening • Rhizotomy
• Rigidity• Pallidotomy• Deep brain stimulation
Effects on speech tend to be less dramatic than on postural and limb musculature
©2016 MFMER | slide-116
Behavioral Management of Tone Impairments• Target sensory endings or afferent pathways of
reflex loops
• Examples• Slow stretch – inhibit stretch reflex• Quick stretch/tapping – stimulate stretch
reflex• Vibration – stimulate tonic vibratory reflex
(stimulates agonist, inhibits antagonist)
• Related modalities• Cold• Massage
©2016 MFMER | slide-117
Muscle tone in the speech musculature:Summary
• Perceptual assessment methods have not been validated with instrumental measures
• Instrumental measures are under exploration but have not yet met validity standards even in the research setting
• Muscle tone in the orofacial muscles is regulated in ways unique from the limb musculature
©2016 MFMER | slide-118
Muscle tone in the speech musculature:Summary
• It is unclear how resting muscle tone affects speech movements
• Treatments described to address muscle tone in the limbs unlikely to affect speech muscles other than jaw closing muscles
• No evidence to demonstrate efficacy of tone altering treatments for speech
©2016 MFMER | slide-119
Motor Learning PrinciplesFrameworks for Guiding Decision Making
©2016 MFMER | slide-120
Motor learning
• Learning produces relatively permanent changes in the capability for performance
• Separate from factors that temporarily change performance (e.g., motivation, warm-up)
• Implications• Performance during training is not a
measure of learning• Factors that result in better performance
during rehearsal/training may not have the same effect on permanent learning and/or carryover

Clark 2017
21
©2016 MFMER | slide-121
Select Principles of Motor Learning
• Skill presentation techniques
• Task sequencing
• Providing feedback
Schmidt & Lee, 2011
©2016 MFMER | slide-122
Evidence Supporting the Application of Motor Learning Principles in Motor Speech Disorders
©2016 MFMER | slide-123
Take-home Messages on Motor Learning
• Measuring Motor Learning• Performance during the treatment session is
not a sensitive measure of learning (retention/transfer)
• To best serve our patients and our profession, we need to diligently report progress/treatment success based on outcomes obtained outside of rehearsal (treatment sessions or at least targeted practice)
©2016 MFMER | slide-124
Take-home Messages on Motor Learning
• Many training factors that enhance learning result in slower acquisition
• Random practice• Varied practice• Reduced feedback
• The more movement trials the better
• All evidence suggests that motor learning is highly specific
• Underlying ability cannot be improved by drills targeting speed or coordination
©2016 MFMER | slide-125
Take-home Messages on Motor Learning
• Excessive verbal processing will direct attentional resources away from motor control processing
• Visual models• Reduced verbal feedback
• Reducing feedback allows the learner to attend to sensory consequences (more similar to the target context)
©2016 MFMER | slide-126
Application: Motor learning
• Treatment targets• Loudness• Slow rate• Over-enunciation• Lexical stress
• Skill presentation• Direct and indirect modeling• “Loud” requires limited
verbal description
• Practice• Random and variable
(assuming the skill has been acquired but not generalized)
• Nonverbal feedback (sound level meter)
• Summary feedback

Clark 2017
22
©2016 MFMER | slide-127
Read the phrase
• Go for it
• Are you sure?
• The cat’s out of the bag
• Enormous hippopotamus
• I’m in!
• Don’t count your chickens before they’re hatched
• Coffee?
LOUD
SLOW
ENUNCIATE
CAREFUL STRESS
©2016 MFMER | slide-128
Specific Dysarthria Treatments
©2016 MFMER | slide-129
Respiratory Treatments
©2016 MFMER | slide-130
Respiratory Impairments
Impairments
• Reduced inspiratory capacity
• Reduced expiratory pressure
• Reduced control • Checking action• Involuntary
movements
Associated Speech Changes
• Reduced overall loudness
• Loudness decay
• Excessive loudness variation
©2016 MFMER | slide-131
Supporting Respiratory Function
• Postural adjustments• Sitting upright or standing typically better
than lying supine• Avoid excess flexion
• Trunk/abdomen• Neck
• External supports• Expiratory boards
©2016 MFMER | slide-132
Inspiratory Muscle Training
• Diaphragm is primary target (belly breathing)
• Discourage excess use of accessory muscles (shoulder breathing)
• Goal is to establish strong, quick inspiration followed by slow, controlled exhalation
• Early training may incorporate slowed and controlled inhalation and exhalation, discussed on next slide
• Strength training requires overload, which may be best achieved with an inspiratory training device
Sapienza, C. & Troche, M. (2012). Respiratory muscle strength training: Theory and practice. Plural Publishing.

Clark 2017
23
©2016 MFMER | slide-133
Diaphragmatic breathing
• Promotes solid respiratory support
• May help inhibit excessive activation of accessory inspiratory muscles and laryngeal musculature
• Visual and tactile feedback (“belly breathing”) often helpful
• Applications on hand-held devices can support independent practice
©2016 MFMER | slide-134
Controlled Expiration (Inspiratory Checking)
• Can be combined with diaphragmatic breathing
• Focus on quick, strong inhalation
• Followed by slow, steady exhalation
Netsell, R & Hixon, T. J. (1992). Inspiratory checking in therapy for individuals with speech breathing dysfunction. ASHA 34: 152.
©2016 MFMER | slide-135
• Pressure threshold trainer
• Resistance set at 75% maximum expiratory pressure
• Rule of 5’s• 5 repetitions• 5 times per day• 5 days per week
• 4-8 weeks
Expiratory Muscle Strength Training (EMST)
©2016 MFMER | slide-136
• Training outcomes• Increased expiratory pressures• Reduced hypophonia• Improved intelligibility
• Patient groups studied• Parkinson disease• Multiple sclerosis• Ataxic disorders
Expiratory Muscle Strength Training (EMST)
©2016 MFMER | slide-137
Phrase Grouping
• Targets strategic pauses for inhalation
• Phrase length selected according to• Respiratory support• Syntactic boundaries
©2016 MFMER | slide-138
Resonatory Treatments

Clark 2017
24
©2016 MFMER | slide-139
Resonatory Impairments
Impairments
• Velar weakness
• Slowness of velar elevation
• Reduced control • Incoordination• Involuntary
movements
Associated Speech Changes
• Hypernasality
• Nasal emission
• Weak articulatory contacts
• Hyponasality
• Alternating resonance
©2016 MFMER | slide-140
• Nonspeech exercise• Examples
• Horn-blowing• Straw-sucking
• No evidence for carry-over to speech tasks
• Speech exercise• Continuous positive airway pressure (CPAP)• Overloads the velopharyngeal musculature
during speech tasks
Velopharyngeal Exercise
Cahill, L. M., Turner, A. B., Stabler, P. A., Addis, P. E., Theodoros, D. G., & Murdoch, B. E. (2004). An evaluation of continuous positive airway pressure (CPAP) therapy in the treatment of hypernasality following traumatic brain injury: a report of 3 cases. [Case Reports]. The Journal of head trauma rehabilitation, 19(3), 241-253.
©2016 MFMER | slide-141
Speech-based Resonatory Treatment
• Emphasis of appropriate oral and/or nasal resonance
• May incorporate augmented feedback• Nasal mirror • SeeScape• Nasometry
• May incorporate progressive difficulty• Vowels • Liquids• Plosives and fricatives• Phonetic context
©2016 MFMER | slide-142
Prosthetic Management
• Palatal lift• Assessment and implementation in
collaboration with prosthodontist• Will be most helpful for speakers with
isolated hypernasality or nasality disproportionate to other features
• Keeping in mind that adequate velopharyngeal valving may support the benefit of interventions targeting phonation or articulation
• Behavioral intervention usually still neededYorkston, K. M., Spencer, K. A., Duffy, J. R., Beukelman, D.R., Golper, L. A., Miller, R. M., Strand, E. A., & Sullivan,M. (2001). Evidence-Based Practice Guidelines for Dysarthria: Management of Velopharyngeal Function. Journal of Medical Speech-Language Pathology, 9(4), 257-273.
©2016 MFMER | slide-143
Prosthetic Management
• Nose plugs
• Nasal obturator• Occlude the nares to prevent excess nasal
air escape• Short term solution while a palatal lift is being
fabricated• Long term option for patients who are not
candidates for palatal lift
Hakel, Marshall, & McHenry (2009). Understanding palatal lifts and nasal obturators. Presented at the ASHA Convention (http://www.asha.org/events/convention/handouts/2009/1915_hakel_mark/) ©2016 MFMER | slide-144
Surgical Management
• Examples• Pharyngeal flap• Injection augmentation
• Candidacy issues• Stable velopharyngeal impairment• Patency of airway
• Behavioral intervention may still be needed
Clark 2017
25
©2016 MFMER | slide-145
Phonatory treatments
Speyer, R. (2008). Effects of voice therapy: A systematic review. Journal of Voice, 22(5), 565-580.
©2016 MFMER | slide-146
Phonatory Impairments
Impairments
• Hypo-adduction
• Hyper-adduction
• Reduced flexibility
• Reduced stability
Associated Speech Changes
• Strained voice
• Breathiness
• Reduced loudness
• Monopitch/monoloudness
• Tremor
• Flutter
©2016 MFMER | slide-147
Supporting Phonatory Function
• Hypo-adduction• Head turn to facilitate approximation of vocal
cords• Manual lateralization of the thyroid cartilage• Surgical management
• Vocal cord injection augmentation• Thyroplasty
• Hyper-adduction• Relaxation• Massage
©2016 MFMER | slide-148
Reducing Laryngeal Strain
• Direct speaker’s attention to somatosensory aspects of excess muscle tension
• Some aspects of laryngeal tension/strain may not respond completely to behavioral approaches
• dystonia in hyperkinetic dysarthria• strain-strangled quality in spastic dysarthria –
but may overcorrect!
• Excess laryngeal tension may result from poor respiratory support or poor coordination with respiration (see Respiratory Treatments)
©2016 MFMER | slide-149
Laryngeal Exercise
• Increasing medial compression (adduction)• Push-pull• Grunt• Cough
• Increasing pitch range and control• Pitch glides and/or steps• Pitch matching
©2016 MFMER | slide-150
Loudness Treatment
• Lee Silverman Voice Treatment (LSVT)• Systematic hierarchy of exercises, focusing
on a single goal “speak LOUD!”• Targets respiratory, laryngeal and articulatory
subsystems• Incorporates high intensity, high frequency
practice
• SPEAK OUT with LOUD Crowd
• Non-standardized loudness treatment
Smith, M. & Ramig, L. (2014). Neurologic disorders and the voice. In J.S. Rubin, G. Korovin & R. T. Sataloff (Eds.), Diagnosis and Treatment of Voice Disorders. Plural Publishing
Clark 2017
26
©2016 MFMER | slide-151
Coordinating Respiration & Phonation
• Potential targets• Lung volume at onset of phonation• Initiating phonation at the top of inhalation• Phrase grouping (ceasing phonation before
respiratory support wanes)• Rapid inhalation between phrases
Spencer, K. A., Yorkston, K. M., & Duffy, J.R. (2006). Practice guidelines for dysarthria: evidence for the behavioral management of the respiratory/phonatory system.Academy of Neurologic Communication Disorders and Sciences, Technical Report No. 3, 50 pages. ©2016 MFMER | slide-152
Articulatory treatments
©2016 MFMER | slide-153
Articulatory Impairments
Impairments
• Weakness and/or fatigue
• Reduced range of motion
• Reduced speed
• Reduced coordination
• Involuntary movements
Associated Speech Changes
• Articulatory imprecision
• Slow rate
©2016 MFMER | slide-154
Supporting Articulatory Function
• Velopharyngeal support (see Resonatory Treatments)
• Jaw support (bite block)
• Sensory tricks (hyperkinetic dysarthria –dystonia)
• Stretching/massage• Hyper-reflexia (spasticity) in jaw muscles• Would not be expected to facilitate muscle
functions in lips, face, tongue
©2016 MFMER | slide-155
Articulatory Exercise
• Candidates for exercise• Detectable weakness is a primary contributor
to articulatory imprecision• Weakness may be detectable in spastic
dysarthria, but slowness of movements may be the greater detriment
• No contra-indications for resistance exercise (e.g., susceptibility to fatigue)
• Tongue strengthening programs well studied for dysphagia outcomes; speech evidence is less compelling, even in dysarthria
McCauley, R. J., Strand, E., Lof, G. L., Schooling, T., & Frymark, T. (2009). Evidence-based systematic review: effects of nonspeech oral motor exercises on speech. American Journal of Speech-language Pathology, 18(4), 343-360. ©2016 MFMER | slide-156
Articulatory Treatments
• Exaggerated articulation (over-articulation)
• Alternative place/manner/voicing
• Coordination of complex phonetic sequencing• Be mindful of task specificity• Often targeted in concert with lexical stress
(see Prosody treatment)
Clark 2017
27
©2016 MFMER | slide-157
PROSODY TREATMENTS
©2016 MFMER | slide-158
Prosody Targets
• Speaking rate
• Lexical stress
• Sentential stress
• Phrase groupings (see respiratory treatments)
©2016 MFMER | slide-159
Speaking Rate
• Even for patients with slow rate, increasing overall speaking rate is almost never an appropriate target
• Reducing speaking rate, even for patients with normal or slow rate, typically improves intelligibility
• Speakers with hypokinetic dysarthria often have rapid rate, but may have difficulty intentionally reducing rate
©2016 MFMER | slide-160
Rate Reduction Strategies
• Pacing board/hand tapping
• Metronome
Yorkston, K. M., Hakel, M., Beukelman, D. R., & Fager, S. 2007). Evidence for effectiveness of treatment of loudness, rate or prosody in dysarthria: A systematic review. Journal of Medical Speech-Language Pathology, 15(2), xi-xxxvi
©2016 MFMER | slide-161
Rate Reduction Strategies
• Delayed auditory feedback
• Indirect strategies• Increased loudness (see phonatory
treatments)• “Clear” speech (see intelligibility treatments)
Yorkston, K. M., Hakel, M., Beukelman, D. R., & Fager, S. 2007). Evidence for effectiveness of treatment of loudness, rate or prosody in dysarthria: A systematic review. Journal of Medical Speech-Language Pathology, 15(2), xi-xxxvi ©2016 MFMER | slide-162
Lexical and Sentential Stress
• Visual cueing/feedback• Hand gestures signalling change in
loudness, pitch, and/or duration• Acoustic software
• Activities/stimuli• Contrastive stress• Metric pattern across various word lengths• Verbal repair

Clark 2017
28
©2016 MFMER | slide-163
Standardized Treatments for AOS
©2016 MFMER | slide-164
Treatment Programs
©2016 MFMER | slide-165
AOS Treatment Programs
• Articulation Focused
• Prosody Focused
• Utterance Focused
• Gestural / Aug Comm
©2016 MFMER | slide-166
AOS Treatment
• Articulation Focused• 8 Step Continuum• DTTC• PROMPT• Sound Production Treatment
• Utterance Focused
• Prosody Focused
• Gestural / Aug Comm
©2016 MFMER | slide-167
8 Step Continuum
• AKA Integral Stimulation
• Designed to provide “threshold” level cueing so the patient receives stimulation just adequate to elicit a correct response without over-cueing
©2016 MFMER | slide-168
Suggested Cue Hierarchy
• (Tactile Cues)
• Simultaneous Production
• Mimed Production
• (Immediate Repetition)
• Successive Repetition

Clark 2017
29
©2016 MFMER | slide-169
Suggested Cue Hierarchy
• Delayed Repetition
• Reading
• Reading with Delay
• Answering Questions
• Role Playing
©2016 MFMER | slide-170
Dynamic Temporal and Tactile Cueing
©2016 MFMER | slide-171
Dynamic Temporal and Tactile Cueing
©2016 MFMER | slide-172
Dynamic Temporal and Tactile Cueing
©2016 MFMER | slide-173
Dynamic Temporal and Tactile Cueing
©2016 MFMER | slide-174
Dynamic Temporal and Tactile Cueing
Clark 2017
30
©2016 MFMER | slide-175
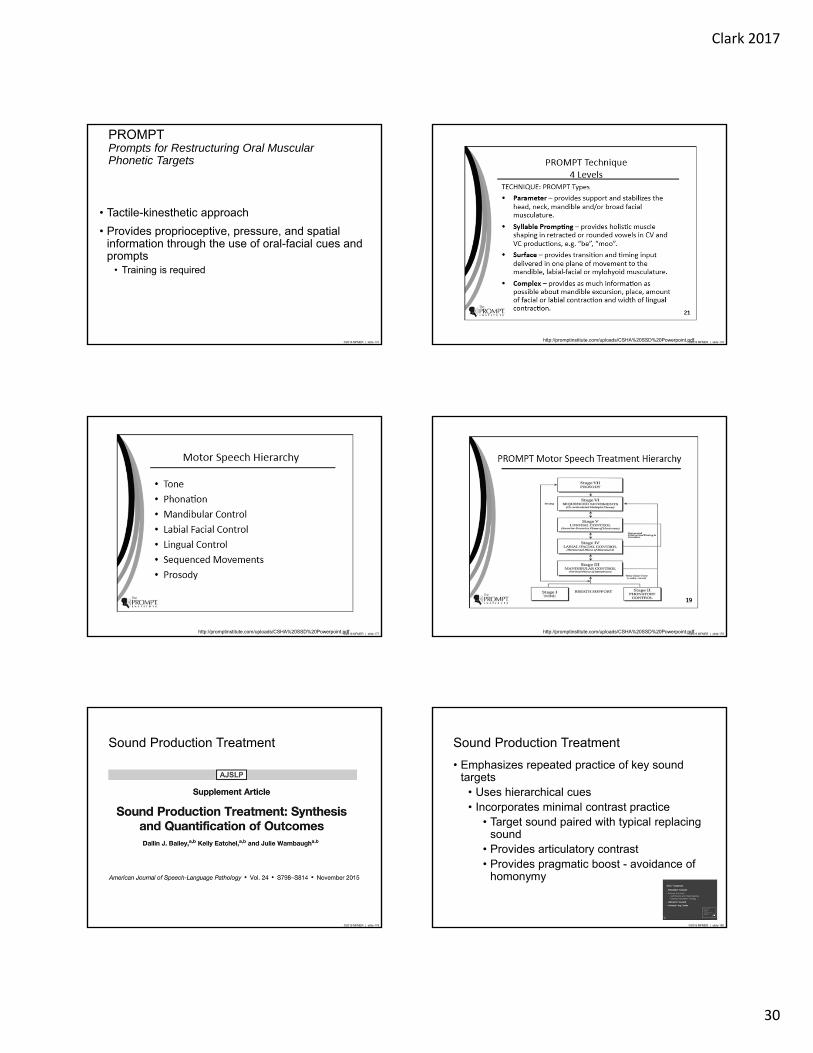
PROMPTPrompts for Restructuring Oral Muscular Phonetic Targets
• Tactile-kinesthetic approach
• Provides proprioceptive, pressure, and spatial information through the use of oral-facial cues and prompts
• Training is required
©2016 MFMER | slide-176http://promptinstitute.com/uploads/CSHA%20SSD%20Powerpoint.pdf
©2016 MFMER | slide-177http://promptinstitute.com/uploads/CSHA%20SSD%20Powerpoint.pdf ©2016 MFMER | slide-178http://promptinstitute.com/uploads/CSHA%20SSD%20Powerpoint.pdf
©2016 MFMER | slide-179
Sound Production Treatment
©2016 MFMER | slide-180
Sound Production Treatment
• Emphasizes repeated practice of key sound targets
• Uses hierarchical cues• Incorporates minimal contrast practice
• Target sound paired with typical replacing sound
• Provides articulatory contrast• Provides pragmatic boost - avoidance of
homonymy

Clark 2017
31
©2016 MFMER | slide-181
Selection of Treatment Targets
• Derived in the process of thorough characterization of speech sound accuracy
• Impact on intelligibility• % in error• Homonymy• Frequency of occurrence in language
• Level of success
• Trial therapy - stimulability
©2016 MFMER | slide-182
Selection of Exemplars of Targets
• 10 exemplars should be sufficient
• Real words when possible
• One word-position suggested
• Variety of vowels should be represented
• Minimal contrast word selected for each exemplar
• Real word• Contains replacing sound or approximation• Key…tea• Cap…tap
©2016 MFMER | slide-183
Hierarchy of Cues (Word Level)
Step 1 – Modeling/Imitation at Word Level
Step 2 – Modeling + Written letter cue/Imitation
Step 3 – Integral Stimulation
Step 4 – Articulatory Placement + Modeling
Step 5 – Production of target sound in isolation
©2016 MFMER | slide-184
Treatment Sequence
• Each Session (45 minutes to 1 hour)• hierarchy applied to each word pair• 10 words presented in random order = 1 trial• attempt to complete at least 7 trials (70
words) per session
• Three sessions per week recommended
©2016 MFMER | slide-185
Treating More than One Sound At a Time with SPT
• Select minimal contrast words across the sounds
• “low” “mow” “know”
• Select the contrast word to reflect errors on all sounds (may need more than one)
• “dough” “though”
©2016 MFMER | slide-186
Targeting Multiple Sounds
• Generally recommended only after single phoneme targets are produced with relatively high levels of accuracy (e.g., 40% +)
• Number of trials is greatly reduced – probably would be difficult to “establish” sounds
• Recall Motor Learning Principles• Blocked trials - better for initial acquisition• Randomized trials - better for learning / maintenance
Clark 2017
32
©2016 MFMER | slide-187
AOS Treatment
• Articulation Focused
• Prosody Focused• Metronome and Hand-tapping• Melodic Intonation Therapy
• Utterance Focused
• Gestural / Aug Comm
©2016 MFMER | slide-188
Metronome Training
• Focuses on rate reduction, not on accurate phonetic productions
• Multisyllabic targets
• Benefit ↓ ___ ___
• Spaghetti ___ ↓ ___
• Represent ___ ___ ↓
©2016 MFMER | slide-189
Metronome Training – Multisyllabic Words
• Hierarchical levels vary the availability of a model, speed of metronome, and nature of rhythm
• Level 1: Clinician Model, Unison Production, Patient Production
• Level 2: Faded Clinician Model• Level 3: No Clinician Model• Level 4: Increased Production Rate• Level 5: Syncopated Rhythm
©2016 MFMER | slide-190
Feedback
• Tapping accuracy
• # syllables
• Production to the beat (not about sound production)
©2016 MFMER | slide-191
Why Might Rate Control/Pacing Facilitate Articulation?
• Increased time to reach articulatory postures
• Improved functioning of central pattern generators
• Decreased degrees of freedom in speech production
• Increased allocation of resources
• Motoric “spillover”
• Increased afference
©2016 MFMER | slide-192
Melodic Intonation Therapy
• MIT has been applied to the management of AOS and nonfluent aphasia
• Emphasizes both melody and rhythm of productions

Clark 2017
33
©2016 MFMER | slide-193
Level 1
• Step 1: Humming• Clinical models melody and taps rhythm• Next adds word to melody and rhythm
• Step 2: Unison
• Step 3: Unison with clinician fading out
• Step 4: Immediate repetition
• Step 5: Response to probe question
©2016 MFMER | slide-194
Level 2
• Step 1: Clinician models target while tapping (no patient response required)
• Step 2: Unison with fading
• Step 3: Delayed repetition
• Step 4: Response to probe question
©2016 MFMER | slide-195
Level 3 (Speech Song)
• Step 1: Delayed repetition
• Step 2: Introduce speech song • Exaggerated rhythm and stress
• Step 3: Speech song with fading
• Step 4: Delayed repetition of normal speech prosody
• Step 5: Response to probe question
©2016 MFMER | slide-196
AOS Treatment Programs
• Articulation Focused
• Prosody Focused
• Utterance Focused• Response Elaboration Training• Voluntary Control of Involuntary Utterances• Script Training
• Gestural / Aug Comm
©2016 MFMER | slide-197
Utterance Focused Treatments
• Emphasize effective volitional communication regardless of phonetic accuracy
©2016 MFMER | slide-198
Response Elaboration TrainingKearns and colleagues
• Loose training procedure designed to increase length and content of verbal productions
• Patient-initiated utterances• guided by pictures• NOT specified by therapist
• Modeling & forward chaining procedures

Clark 2017
34
©2016 MFMER | slide-199
RET Sequence1. Present picture stimuli & elicit a response
2. Repeat patient’s production & reinforce
3. Ask a question to elicit an elaboration of the original response
4. Repeat & reinforce the new production; model combined productions (1 + 3)
5. Model combined production and request a repetition
6. Reinforce repetition and model again
©2016 MFMER | slide-200
Modifications to RET• Provision of 2 phrase level models (NP & VP)
in the event of no response (initial response & elaboration)
• Provision of integral stimulation upon incorrect or no response (following previous models)
• Repeated practice of elaborated utterances
• Use of a time delay prior to final repetition
©2016 MFMER | slide-201
Modified Version of RET
1. Present picture stimuli & elicit a response• model 2 response options (e.g., “you could say NP
or VP”)• model a 1-word response - request repetition• use integral stimulation
2. Repeat patient’s production & reinforce
3. Ask a question to elicit an elaboration of the original response
• model as in step 1
©2016 MFMER | slide-202
Modified Version Cont.
4. Repeat & reinforce the new production; model combined productions (1 + 3)
5. Model combined production and request a repetition
• if correct - 3 more productions• if incorrect - use integral stimulation to elicit multiple
productions
6. Remove picture for 5 seconds - request repetition of description
• Feedback as in step 5
©2016 MFMER | slide-203
RET Applied to Personal Recount• no picture stimuli
• patient instructed to “Tell something about anything that you would like to talk about.”
• treatment hierarchy applied as before
• at least 14 topic attempts elaborated upon per session
©2016 MFMER | slide-204
Summary of RET• Provides models and scaffolding to increase
length and informativeness of verbal expression
Clark 2017
35
©2016 MFMER | slide-205
Script training
• Goal is to produce islands of fluent speech in conversation
• Isolated or sequenced phrases and sentences with specific conversational purposes are practiced extensively
©2016 MFMER | slide-206
Voluntary Control of Involuntary Utterances (VCIU)
• For patients with limited verbal expression
• Attempts to expand the communicative uses of spontaneous productions
©2016 MFMER | slide-207
VCIU Sequence
• Clinician notes any spontaneous utterances and writes them each on a card
• Patient reads card • (spontaneous -> volitional)
• Utterances that can be produced volitionally are targeted in other contexts
• Picture naming• Sentence completion• Discourse
©2016 MFMER | slide-208
VCIU Principles
• Target stimuli can be added continually
• Emphasis is on expanding use of spontaneous utterances, not on correct productions (either phonetic or semantic) during any given trial
©2016 MFMER | slide-209
Management of Motor Speech DisordersComprehensibility Strategies & AAC
©2016 MFMER | slide-210
Operational Definitions
Intelligibility
The listener’s success in understanding the acoustic signal produced by a speaker
Comprehensibility
The listener’s success in understanding the message/meaningproduced by a speaker
• Both intelligibility and comprehensibility are influenced by the communication environment and the behaviors of the speaker and listener.
• Comprehensibility strategies include behaviors that improve intelligibility

Clark 2017
36
©2016 MFMER | slide-211
Helpful resources
Yorkston, K. M., Beukelman, D., Strand, E., & Hakel, M. (2010). Management of motor speech disorders in children and adults (3 ed.). Austin, TX: Pro-Ed.
©2016 MFMER | slide-212
Comprehensibility Strategies
• Seek to improve activity and participation
• Include• Optimization of
environmental factors• Exploiting facilitating
personal factors• Compensating for limiting
personal factors
Health Condition
Activity and Participation
Contextual Factors
(Personal and Environmental)
Body Functions and
Structures
©2016 MFMER | slide-213
Introducing Comprehensibility Strategies
• Initial visit• Providing recommendations• In order to obtain history
©2016 MFMER | slide-214
Comprehensibility Strategies
Optimizing the environment
Speaker behaviors
Listener behaviors
©2016 MFMER | slide-215
Optimizing the environment
pixshark.com
©2016 MFMER | slide-216
Reducing background noise
• Obvious, controllable sources• TV, radio, computer, etc
http://www.susieburrell.com.au/rise-nutrition-haters/

Clark 2017
37
©2016 MFMER | slide-217
Reducing background noise
• Obvious, not-so-controllable sources• Crowd noise
• Move away
• Take advantage of barriers
©2016 MFMER | slide-218
Reducing background noise
• Not-so-obvious controllable sources• Appliances• Open windows
• Turn ‘em off
• Close ‘em
• Move away
©2016 MFMER | slide-219
Reducing background noise
• Not-so-obvious not-so-controllable sources• Road/traffic noise
• May require other strategies
©2016 MFMER | slide-220
Optimizing lighting
• Avoid backlighting
• Avoid dim lighting
©2016 MFMER | slide-221
Optimizing the environment
• Be in the same environment!
• Avoid communication over a distance
©2016 MFMER | slide-222
Optimizing the environment
• Reduce distractions
• Auditory and visual distractions
• Multi-tasking

Clark 2017
38
©2016 MFMER | slide-223
Optimizing the environment
• Choose the time and place for communication
Avoid important conversations when the speaking or listening will be difficult
©2016 MFMER | slide-224
Speaker Behaviors
©2016 MFMER | slide-225
Speaker behaviors
• Speech-focused
• Language-focused
• Communication-focused
©2016 MFMER | slide-226
Speaker behaviors: Speech-focused
• Speak slowly
Clinician Pearls• Acknowledge this is challenging • Suggest “tricks”
• Speak loudly• Speak clearly
©2016 MFMER | slide-227
Speaker behaviors: Speech-focused
• Speak very slowly* • Pause briefly between each word• Pay attention to the small words• Do not separate syllables within words• Include every syllable• Maintain intonation (may have to slow even
further)
*when intelligibility is more dramatically impacted
©2016 MFMER | slide-228
Speaker behaviors: Speech-focused
• Speak clearly• Imagine you’re speaking to someone who is
hard of hearing or doesn’t understand your language very well
• Over-enunciate• Speak carefully
Tjaden, K., Sussman, J. E., & Wilding, G. E. (2014). Impact of clear, loud, and slow speech on scaled intelligibility and speech severity in Parkinson's disease and multiple sclerosis. Journal of speech, language, and hearing research : JSLHR, 57(3), 779-792.
Instructions may focus on over-articulation (hyper-articulation), but effects are broader
Slow rateWider loudness and pitch variation

Clark 2017
39
©2016 MFMER | slide-229
Speaker behaviors: Speech-focused
• Speak up!• Not just for hypokinetic dysarthria• Great in the context of reduced background
physiologic effort• Often improves articulatory precision• May reduce rate
©2016 MFMER | slide-230
Speaker behaviors: Language-focused
• Use complete, simple sentences
• Use predictable wording
©2016 MFMER | slide-231
Speaker behaviors: Language-focused
• When repeating• The first repetition, say it exactly as you said
it the first time• Rephrase, but make sure the listener knows
you’re rephrasing
©2016 MFMER | slide-232
Speaker behaviors: Communication-focused
• Get the listener’s attention
• Call his/her name• Wait until the listener is watching
your face
©2016 MFMER | slide-233
Speaker behaviors: Communication-focused
• Help the listener predict what you’re going to say
• Identify the general topic• Take advantage of contextual cues
(point to objects in the environment, headlines, etc.)
• Signal topic changes
©2016 MFMER | slide-234
Speaker behaviors: Communication-focused
• Use all modalities available• Speak• Point• Gesture• Facial expression• Pictures (points or draw)• Write• Text• Type
Clark 2017
40
©2016 MFMER | slide-235
Speech Supplementation
• Incorporated during spoken expression
• Strategies provide listeners with additional information to help make sense of the spoken message
• Typically involves “signal-independent” information about the message
• Includes gestures
Hanson, E., Yorkston, K., & Beukelman, D. (2004). Speech supplementation techniques for dysarthria: A systematic review. Journal of Medical Speech-Language Pathology, 12(2), ix-xxix.
©2016 MFMER | slide-236
Alphabet Supplementation
• Point to initial letter of word as each word is spoken
• Also serves as a pacing strategy
• Identification of initial letter facilitates word prediction by listener
A B C DE F G HI J K L M NO P Q R S TU V W X Y Z
Example of alphabet board with vowels aligned on left margin.
©2016 MFMER | slide-237
Semantic/Topic Supplementation
• Identifies the topic of discussion to help listener’s word prediction and comprehension
• Topics can be identified through• Spoken expression• Written expression• Photographs/pictures• Other artifacts
• Calendars• Souvenirs• Newspapers
©2016 MFMER | slide-238
Speaker behaviors: Communication-focused
• Interact
• Use turn-taking signals• Visible• Audible• Conspirator• Let listeners know “the rules”
©2016 MFMER | slide-239
Listener Behaviors
©2016 MFMER | slide-240
Listener behaviors
• Give your undivided attention
• Move close to the speaker• Watch the speaker

Clark 2017
41
©2016 MFMER | slide-241
Listener behaviors
• Know (ask for) the topic
• Watch for topic-changing signals
©2016 MFMER | slide-242
Listener behaviors
• Piece together the clues• Speech• Gestures• Facial expression• Pointing• Writing• Texting
©2016 MFMER | slide-243
Listener behaviors
• Signal to the speaker as soon as you don’t understand
A nonverbal signal is often best so the speaker doesn’t feel interrupted
©2016 MFMER | slide-244
Listener behaviors
• Avoid the least helpful question in the English language
http://propercourse.blogspot.com
©2016 MFMER | slide-245
Listener behaviors
• Avoid the least helpful question in the English language
http://propercourse.blogspot.com
• Repeat the part of the message you heard
• Ask yes/no questions for clarification
©2016 MFMER | slide-246
Listener behaviors
• Know the rules
• How does the speaker signal a turn?
• Should you “word predict”?• What is the back-up plan?

Clark 2017
42
©2016 MFMER | slide-247
Speaker & Listener Behavior
• Glossing• Listener repeats each word as the speaker
says it• Speaker has to pause briefly between words
so listener can repeat• Correct breakdowns as they occur• Combine with alphabet supplementation
©2016 MFMER | slide-248
Instruction in Comprehensibility Strategies and Developing Recommendations
©2016 MFMER | slide-249
Presenting Comprehensibility Strategies
• Explain that the goal is successful exchange of information, not word for word intelligibility
• Highlight the value of being understood the first time
• Emphasize that successful communication is the responsibility of all participants
• “Good advice for all of us” philosophy
©2016 MFMER | slide-250
Presenting Comprehensibility Strategies
• Allow speaker and family members to practice and respond
• Troubleshoot obstacles• Listeners who “can’t hear”• Listeners who only talk• “Fast talkers”
• Give feedback and additional guidance
©2016 MFMER | slide-251
Evaluate success
• Some patients may be proficient after initial session
• Some may need additional instruction• Follow-up consultation• Component of on-going therapy
• Value of individual strategies may vary across recovery, progression, and/or context
©2016 MFMER | slide-252
AAC
• Augmentative and alternative communication (AAC) is an appropriate option for speakers with poor intelligibility
• Temporary as speech improves• Introduced early in degenerative disease
Clark 2017
43
©2016 MFMER | slide-253
Evidence-Based Practice Resources
©2016 MFMER | slide-254
EBP Resources
©2016 MFMER | slide-255 ©2016 MFMER | slide-256
EBP Resources
www.ancds.org
©2016 MFMER | slide-257
EBP Resources
www.speechbite.com©2016 MFMER | slide-258
EBP Resources
• Clinical Aphasiology Conference Proceedings• www.clinicalaphasiology.org
• Conference on Motor Speech• http://www.madonna.org/res_conferences• Proceedings published in JMSLP
• ASHA• Special Interest Division 2
• UpToDate ®

Clark 2017
44
©2016 MFMER | slide-259
Mayo ClinicLocations
©2016 MFMER | slide-260
Questions & Discussion