Embed Size (px)
Citation preview

Overview of Changes to SNF Part A Payment
David R. Gifford MD MPHSr VP for Quality & Regulatory Affairs

Improving Lives by Delivering Solutions for Quality Care
Three Rs Impacting SNFs
Reimbursement• Hospital payments
o HRRP, VBP & HACo CJR (hip & Knee replacement)o Episodic paymentso Bundle Payment demoso ACOs
• Managed Care Plans• SNF
o SNF PPS Changing to PDPMo SNF VBP (rehospitalization)o Bundle Payment demos
Reporting• SNF QRP • Payroll Based Journal
(staffing)Regulatory • Requirements of
Participation• Emergency
Preparedeness
Workforce Shortage

SNF VBP

Improving Lives by Delivering Solutions for Quality Care
CMS Medicare SNF VBP Program
HOW IT WORKS• Step 1
o Calculate your rehospitalization RATE• Step 2
o Calculate your SCORE based on your rehospitalization rate OR improvement, whichever is better.
• Step 3o Link your SCORE to payment adjustment for Medicare Part A
claimso Simultaneously reduce everyone’s Part A rate by 2% o Increase your Part A rate by up to 3% based on your SCOREo Assign Incentive Payment Multiplier ranges from 0.980 to 1.0165

Improving Lives by Delivering Solutions for Quality Care
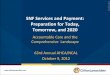
The Rehospitalization Score Yr 2
• Better of your achievement or improvement score• Achievement score year 2:
o If SNFRM rate < 16.3%, then achievement score is 100o If SNFRM rate > 19.8%, then achievement score is 0o Else: see formula
• Improvement score year 2:o If SNFRM rate < 16.3%, then improvement score is 90o If SNF RM CY2017 rate > CY2015 rate, then improvement
score is 0o Else: see formula

100 points
0 points
10 20 30 40 50 60 70 80 90
Baseline Period CY 2015
Perfo
rman
ce P
erio
d CY
201
7Scenario: Baseline rate is 24 and you improve to a performance rate of 20. What is your rehospitalization score? Plot baseline and performance rate; where they lines intersect you read the points.
Points
POIN
TS

Improving Lives by Delivering Solutions for Quality Care
CMS Propose Exchange Function(Graph is representation: NOT exact)
.98
0.9
9
1.0
1
.65
2.
0
= 18.3%

Improving Lives by Delivering Solutions for Quality Care
Incentive Payment Multiplier
Range: 0.9800 to 1.0165• 60% cut >1% to 2%• 13% cut 0 to 1%• 12% increase 0 to 1%• 15% increase >1% to 1.6%
Payment Cut Payment Increase73% 27%

Patient Driven Payment Model PDPMImplementation - October 1, 2019 (FY 2020)

Q4 2018 Q1 2019 Q2 2019 Q3 2019 Q4 2019
CMS: Draft MDS & data specs updates
CMS: Proposed rule—some modifications expected (i.e.. IPA) CMS: Final
Rule
PDPM Go-Live 10/1
CMS Schedule for PDPM Changes and Updates
CMS Plan for Education and Training as Yet Unclear – AHCA is
Moving Ahead As Possible

PDPM is a New Medicare Part A Fee-for-Service Payment System
Per Diem Payment*Budget-neutral
Therapy Minutes No
Longer Drive
Payment
Patient Characterist
ics Drive Payment
Total Therapy Delivery
Capped at 25% for
Group and Concurrent
MDS Coding
Now Drives
Payment
All Elements Included in Proposed Rule with Few Changes in Final

PDPM Overview§ The proposed PDPM is based on SIX components; with Five case mix adjusted based
on resident clinical characteristics1. PT2. OT3. SLP4. Non-therapy Ancillary (NTA)5. Nursing6. Non-case mix
§ Within components 1-5, residents assigned to a group which is attached to a CMI§ Calculate a payment for each component by
o multiplying the CMI for the resident’s group first by the component’s federal base payment rate
o then multiply PT, OT and NTA component by the variable per diem adjustmento for residents with HIV/AIDS indicated on their claim, the nursing component of payment
would be multiplied by 1.18
§ Added payments from each component plus the non-case-mix component payment rate to create a resident’s total SNF PPS per diem rate under the proposed PDPM.

Improving Lives by Delivering Solutions for Quality Care
PDPM vs RUG Components
RUGsTherapy
Non-Case-Mix Therapy
Nursing
Non-Case-Mix
PDPM PT
OT
SLP
Nursing
NTAS
Non-Case-Mix

PDPM CMI Components Summary PT OT SLP Nursing NTAS
# of
Groupers 16 16 12 25 6
Clinical
Condition
Primary reason for
SNF Care - Section I
Primary reason for
SNF Care - Section I
Acute Neurologic
Condition
Clinical Condition –
section I
Comorbidities -
Section I
Functional
Status
Section GG Early
and Late Loss
Section GG Early and
Late Loss
None Section GG Early and
Late Loss
None
Cognitive
Status
None None BIMS & CPS None None
Other None None • Swallowing disorder or mechanically altered diet
• Other SLP-Related comorbidities
• Extensive Services Received
• Depression • Restorative nursing
services received
Extensive Services
Received -
sections K, M, & O
CMI range 1.08 to 1.92 1.09 to 1.68 0.68 to 4.19 0.66 to 4.04 0.72 to 3.25
Per Diem
Adjustor
Taper after day 20 Taper after day 20 No Tapering No Tapering Taper after day 3

Improving Lives by Delivering Solutions for Quality Care
Example Calculator – PDPM
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per
diem)PT $59.33 x x x =OT $55.23 x x x =SLP $22.15 x x x =NTA $78.05 x x x =Nursing $103.46 x x 1.00* x =Non-Case-Mix Component
$92.63 x x x =
Total =*Except when resident has HIV/AIDS, then variable per diem adjustment = 1.18Note: Rates are for urban facilities, CMS estimated if program went into effect FY19

Base Federal Rate

PT & OT Per Diem Adjustment Factors

NTA Per Diem Adjustment Factors

Example Resident – PDPM (Day 4-20)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 1.00 = $91.96OT $55.23 x 1.55 x x 1.00 = $85.61SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 1.00 = $144.39Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $625.81

Variable Per-Diem
Day 4 - NTAS rates drop 2/3
Day 21 and every 7 days - PT and OT rates drop 2%
Interim Payment Assessment Optional
Variable Payments Do Not Reset to Day-One

PDPM Impact on MDS

Fewer MDS Assessments
Day 5 MDS
Day 14 MDS
Day 30 MDS
Day 60 MDS
Day 90 MDS
Discharge MDS
RUGs IV
PDPM
Day 5/
Admission MDS
Discharge MDS with Therapy Codes
Interim Payment
Adjustment
Therapy OMRAs
1. Elimination of MDS Schedule 2. Elimination of Other Medicare Required Assessment (OMRA)

Therapy Time No Longer Impacts Payments But Must Still Be Reported
• Therapy services are only to be reported on SNF PPS discharge MDS• The following PT/OT/SLP service delivery items are to be reported
separately by discipline o Start and end dateso Total treatment days during entire stayo Total individual 1:1 therapy minutes during entire stayo Total concurrent therapy minutes during entire stayo Total group therapy minutes during entire stay
• There is a 25% limit on the total amount of concurrent and or group therapy permitted per stay within each discipline o CMS will issue a non-fatal warning edit on validation report if limit surpassedo CMS will monitor and flag providers for audits, and revise policy if abused

Many More MDS Items Impact PDPM than Under RUGs
Under RUGs• Over 90% of resident days
reported via Rehab RUGs• Rehab RUG rates determined
by 20 MDS item fields o Therapy minutes – 12 itemso ADLs – 8 items
Under PDPM• All PDPM component rates
independently determined• 161 MDS item fields
• PT – 14 MDS items• OT – 14 MDS items• SLP – 33 MDS items• Nursing – 129 MDS items• NTAS – 33 MDS items

Other MDS Considerations
• Many PDPM MDS items also impact SNF QRP o101 MDS items impact SNF QRP 2% adjustment
for reporting • Uncertainty regarding whether, or how quickly,
Medicaid, Medicare Advantage, ACO Conveners, CJR Bundle Holders, or other payers will transition to PDPM

PDPM Payment Drivers

Accuracy with Diagnosis & Coding on Admission MDS Critical
PTOTSLPNursingNTAS
Hospital Discharges • No new information
needed from hospital • Typical discharge
information sufficient
SNF Admits• SNF clinician diagnoses • MDS coordinator codes
based on assessment items & ICD-10 codes
Payment Classification• Case-Mix Group (CMG)
assigned for each component
• Patient characteristics for component CMGs differ

PT & OT Component Drivers
• Primary reason for SNF careo MDS section I: ICD-10
codes
• Function ADL Scoreo MDS section GG
16 payment groups each
4 clinical categories
4 functional score ranges


SLP Component Drivers
• Primary Diagnosis for SNF care o MDS section I: acute neurologic condition
• Secondary Diagnoseso MDS section I: SLP co-morbidities
or • Cognitive impairment
o MDS BIMS or CPS
• Dysphagiao Mechanically altered dietORo Swallowing disorderMDS items
12 payment groups
4 categories based on number of elements
3 categories based on number of elements

SLP CMI – Related Comorbidities

SLP CMI

Nursing Component Drivers
• Extensive Services• Clinical Conditions• Adjustors
oDepressionoRestorative nursingoFunction ADL
25 payment groups
3 base service categories5 base clinical categories
Used to modify extensive services and clinical conditions

Nursing CMI
Each resident is Assigned to 1 of 25 Groupings each with its own CMI based on
§ Primary Diagnosis grouping - MDS Section I
§ Functional Status - MDS Section GG
§ Presence of Depression – MDS PHQ
§ Extensive Services Received – MDS section O, K, M & I
§ Restorative nursing services received - MDS

RN CMI Groupings (1 of 3)

RN CMI Groupings (2 of 3)

RN CMI Groupings (3 of 3)

NTAS Component Drivers
Each Payment Group has its own CMI based on:• High NTAS cost conditions
o MDS Section I
• High NTAS cost extensive serviceso MDS sections K, M & O
6 payment groups

NTA CMI

NTA Scoring (1 of 2)

NTA Scoring (2 of 2)

Great! …But What Does That Mean?

Example Resident –Description
• Admitted with stroke • ADL 9 • Moderate cognitive impairment• Needs PT, OT, SLP – receives 730
minutes/week• Special requirements – dialysis, IV meds,
mechanically modified diet• Comorbidities – diabetes

Example Resident – DetailsResident Characteristics
Resident A Details
Rehab Received YesTherapy Minutes 730Extensive Services NoADL Score 9Clinical Category Acute NeurologicPT and OT Function Score 10Nursing Function Score 7Cognitive Impairment ModerateSwallowing Disorder NoMechanically Altered Diet YesSLP Comorbidity NoComorbidity Score 7 (IV meds, diabetes)Other Conditions/Services DialysisDepression No
RUGs category:
RUB
PDPM characteristics

EXAMPLE OF PDPM – PT/OT CMI
PDPM CMI IndexPT = ???OT = ???SP = RN = NTA =


EXAMPLE OF PDPM – PT/OT CMI
PDPM CMI IndexPT = 1.55OT = 1.55SP = RN = NTA =

EXAMPLE OF PDPM – SP CMI
PDPM CMI IndexPT = 1.55OT = 1.55SP = ???RN = NTA =

Example Resident: SLP CMI

EXAMPLE OF PDPM – SP CMI
PDPM CMI IndexPT = 1.55OT = 1.55SP = 2.85RN = NTA =

Example Resident – PDPM (Day 1-3)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 1.00 = $91.96OT $55.23 x 1.55 x x 1.00 = $85.61SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 3.00 = $433.18Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $914.60

EXAMPLE OF PDPM – All CMIs
PDPM CMI IndexPT = 1.55OT = 1.55SP = 2.85RN = 1.85NTA = 1.43

Example Resident – RUGs Rate
RUG Rate Calculation for RUB FY 2019 (Urban)Component Base Fed
Rate
Case-Mix
Index
Payment
(per
diem)
Therapy $136.67 x 1.87 = $283.05
Non-case-
mix therapyNA for RUB x = $0
Nursing $181.44 x 1.56 = $255.57
Non-case-
mix nursing$92.60 x = $92.60
Total = $631.22
$631.22 per diem
x 30 day stay
= $18,936.60

Example Resident – PDPM (Day 1-3)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 1.00 = $91.96OT $55.23 x 1.55 x x 1.00 = $85.61SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 3.00 = $433.18Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $914.60

Example Resident – PDPM (Day 4-20)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 1.00 = $91.96OT $55.23 x 1.55 x x 1.00 = $85.61SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 1.00 = $144.39Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $625.81

Example Resident – PDPM (Day 21-27)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 0.98 = $90.12OT $55.23 x 1.55 x x 0.98 = $83.89SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 1.00 = $144.39Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $622.26

Example Resident – PDPM (Day 28-30)
Component Base Fed Rate
Case-Mix Index
Special Adjustors
Variable per diem
Payment (per diem)
PT $59.33 x 1.55 x x 0.96 = $88.28OT $55.23 x 1.55 x x 0.96 = $82.18SLP $22.15 x 2.85 x x = $63.13NTA $78.05 x 1.85 x x 1.00 = $144.39Nursing $103.46 x 1.43 x 1.00 x = $148.10Non-Case-Mix Component $92.63 x x x = $92.63
Total = $618.71

Example Resident – PDPM 30 Days
Day 1-3 => 3 days @ $914.60 = $2,743.80
Day 4-20 => 17 days @ $625.81 = $10,638.77
Day 21-27 => 7 days @ $622.26 = $4,355.82
Day 28-30 => 3 days @ $618.71 = $1,856.13
Total = $19,594.52
(Reminder: RUGS Total Was $18,936.60)

Getting Ready for PDPM

Concerns in Preparing for PDPM
• Operational ConcernsoCapabilities MDS coding assessmentoRelationships with hospitalsoContracts assessment
§ Therapy vendors§ IT vendors

Concerns in Preparing for PDPM
• Front-Line ConcernsoClinical programsoCommunication processesoWorkflowoStaffingoTraining

What To Be Doing Now
62
1
2
3
4
Educate yourself about the new system
Develop accurate diagnostic and MDS coding capabilities
Evaluate and strengthen your ability to manage complex patients
Align resources

What Should I Do to
Prepare?
• CMS to provide grouper software
• MAKE SURE YOU ARE COMPLETING MDS ACCURATELY
o Sections GG, I, K, M, O
o [ICD-10 coding on section I is critical]
o BIMS and CPS
o PHQ (depression)
• Look to get an MDS coordinator trained in ICD-10 coding
o AHCA will be providing training

Understand New Payment Drivers’ Impact Accurate Collection of Clinical Information
Optimize Resources to Support PDPM Strengthen Care Delivery Process
ü Executive staff understands PDPM payment drivers and expected facility adjustment if no changes to patient mix
ü Executive staff understands organizational gaps that will affect implementation and subsequent payment under PDPM
ü Executive staff discussion on changes in organizational culture to support PDPM
ü Operational staff understands overall model goals and individual components relevant to role on team
ü Build ICD-10 coding capacity to ensure payment
Core Competencies for Success Under PDPM
64
PDPM Readiness
1 2
34
ü Staff understands importance of clinical documentation ü Ability to capture admission information quickly: clear
picture of hospitalization/surgeries, comorbidities, chronic illnesses, and social determinants of health
ü Highly proficient and accurate approach to determining ARD and coding initial diagnoses, comorbidities, and nursing and NTA services received throughout stay
ü Ability to capture functional status correctly – Section GG ü Process in place to complete Interim Payment Assessment*
ü Evaluation of MDS coordinators’ abilities and growth potential
ü Evaluation of need for / investment in additional clinical staff (e.g., NPs)
ü Evaluation and optimization of therapy contracts ü Evaluation of need for / investment in training to improve
coding accuracyü Evaluation of current business office capabilities ü Evaluation of internal / vendor software readiness
ü Evaluation of care planning team and processes ü Standup meetings and daily communication between
nursing and therapist staffs ü Understanding of how therapy practices may change to
ensure best outcomes for patient ü Exceptional restorative nursing program ü Ability to support complex patients ü Evaluation and development of specialized clinical programs
(e.g., cardiac, respiratory) and transitions program
*CMS has not yet finalized the Interim Payment Assessment Policy

Contact Information
David Gifford MD MPHSR VP for Quality & Regulatory Affairs
American Health Care Association1201 L St. NW
Washington DC [email protected]
202-898-3161www.ahcancal.org