Embed Size (px)
Citation preview

724
Overdrive
Refractoriness
f
s
r
Disease
PABLO A. CHIALE, MD, RUBEN A. SANCHEZ, MD, DAVID A. FRANCO, MD,
MARCELO V. ELIZARI, MD, FACC, MAURICIO B . ROSEN AUM, MD, FACC
Buenos Aires, Argentina
Obj °ves . The alm of this study was to the response ofrefrmt 1n,,% In n and diseased human bundle branches tochanges In cycle length, well as during a long period ofcontinuous overdrive pacing.
Background. The ante rode refractory period of the bundlebranches in patients with functional bundle branch block shortensas the rate is Increased . The rate-dependent response of re cto-
in
bundle branches is quite different. However,this diftrence has not been precisely delineated, and its physio-
is Uncertain .M
. R
of the bundle branches was measuredby the a
plus technique in 16 patients with tacbyc la-ndent bundle b block and 10 patients with functional
bundle b block, both after basic trains of 8 atria[-pacedImpulses at different cycle lengths and du
a 10-min period oftin
overdrive pacing.Results . The baseline refractory period in the bundle branches
Functional bundle branch block occurs when prematuresupraventricular impulses reach the normal intraventricularconduction system at a time when one of the bundlebranches is not fully recovered from the effect of thepreceding beats (1-9) . In contrast to functional bundlebranch block, permanent bundle branch block implies asevere degree of bundle branch disease, resulting in com-plete interruption of conduction . However, this advancedstage of bundle branch block is often preceded by a period ofvariable duration during which the block is intermittent andrate dependent (10-13) . Although functional bundle branchblock is the model for studying anterograde refractoriness innormal human bundle branches, rate-dependent and partic-ularly tachycardia-dependent bundle branch block is proba-bly the best model for studying the electrophysiologic
From the Division of Cardiology, Ramos Mejia Hospital, Buenos Aires,Argentina. This work was supported in part by the Fundacion de investiga-ciones Cardiologicas Einthoven, the Fundacion Alberto J . Roemmers and theConsejo Nacional de Investigaciones Cientificas y Tecnicas (CONICET),Buenos Aires, Argentina .
Manuscript received March 4,1993 ; revised manuscript received October4, 1993, accepted October 14, 1993 .
Address for corr gdenec: Dr. Pablo A . Chiale, Division of Cardiology,Ramos Mejia Hospital, t •c .:iza 609, Ist floor, Buenos Aires (1221),Argentina .
1994 by the American College of Cardiology
JACC Vol. 23, No. 3March 1 . 1994 :724-32
of patients with functional bundle branch block measured Q ±32 (mean ± SD) and shortened to 368 ± 30 at the shortestcycle length . The maximal effect was reached within the 1st min ofoverdrive pacing . The baseline refractory period of the bundlebranches was significantly longer in patients with tachyca la-de dent bundle branch block (611 ± 1 ms) and demonstrateda cumulative overdrive prolongation in 15 (83%) of 18 studies withtypkl manifestations of fatigue. In two other studies, this oc .cur
o.Ay after ajmaline administration .Conclusem c. A rate- and time-dependent prolongation of re-
fractoriness frequently occurs in diseased human bundlebranches. When absent, this response may be induced under theeffects of sodium channel blockers . This would suggest that anabnormality in the recovery from inactivation of the sodiumchannel might underlie the early stages of bundle branch disease .
(J Am Coil Cardiol 1994,23 :724-32)
changes underlying the early stages of disease of the bundlebranches . Although both functional and tachycardia-dependent bundle branch block are rate-dependent phenom-ena, observations from our laboratory strongly suggest thatthe response of tachycardia-dependent bundle branch blockto an increased rate of stimulation is different and oftenopposite to that occurring in functional bundle branch block .The purpose of our study was to delineate these differencesand their physiologic meaning . To that effect, we usedprogrammed atrial stimulation to study 16 patients withtachycardia-dependent and 10 patients with functional bun-dle branch block, with particular emphasis on rate-relatedchanges of refractoriness in the bundle branches .
Methods
Patients with tachycardia-dependent bundle branch block .We studied 16 patients with previously documented bundlebranch block during spontaneous sinus rhythm in at leastone electrocardiogram (ECG) recorded at rest (Table 1) .Eighteen electrophysiologic studies were performed . In 14studies, two 6F bipolar electrode catheters were introducedthrough the right or left femoral veins. One of the twocatheters was positioned against the lateral wall of the rightatrium for atrial pacing, whereas the tip of the second
0735-1097/941$7.00

JACC Vol . 23, No . 3March 1, 1994:724-32
Table 1 . Clinical Characteristics of 16 Patients With Tachycardia-Dependent Bundle Branch Block
F = female : LBBB ~- left bundle branch block ; M = male ; Pt = patient ;RDBB = right bundle branch block .
catheter was placed across the tricuspid valve for Its bundlerecording. His bundle electrograms were recorded at paperspeeds of 50 and 100 mm/s . Stimuli during atrial pacing weretwice the diastolic threshold and 2 ms in duration. In fourother studies, transesophageal atrial pacing was used, withstimuli 10 to 20 ms in duration . The smallest pulse strengthallowing stable atrial capture was used to minimize thepatients' discomfort .
Pacing protocols . The refractory period of the bundlebranches was measured with the extrastimulus technique .Two different pacing protocols were used according to theabsence or presence of a bundle branch block pattern duringspontaneous sinus rhythm (Fig . 1). When bundle branch
A,
•
9 weN
81
as
a&
52
as
Iss
•
WM412as
at
91
at
a
S1
as
~1
111 .
81
81
as
CHIALE ET AL .
725PROLONGED REFRACTORINESS iN THE BUNDLE BRANCHES
as
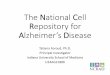
block was absent (Fig . IA), the refractory period of thebundle branches (necessarily shorter than the sinus nodecycle length) was measured by delivering progressivelyshorter (in 10-ms steps) atrial extrastimuli after a basic trainof atrial paced impulses at a preselected cycle length(15 studies) . If bundle branch block was present duringspontaneous sinus rhythm (Fig. I B), the refractory period ofthe bundle branch (necessarily longer than the sinus nodecycle length) was estimated by delivering the atrial extra-stimuli at progressively longer intervals after a basic train ofatrial paced impulses at a preselected cycle length (threestidies, in all of which sinus node activity after the basictrain was sufficiently depressed to allow for introduction ofthe postmature atrial extrastimuli) .
The refractory period of the bundle branches was definedas the longest H IH2 interval (R jR2 in the four transesopha-geal pacing studies) resulting in a bundle branch blockpattern with a QRS width a 120 ms . To assess the effects ofchanges in the driving rate, the refractory period of thebundle branches was measured after trains of 8 basic atrialpaced impulses separated by 9-s intervals during which thesinus node was allowed to reassume control of the heart rate(Fig. I, A and B, top panels) . The baseline refractory periodwas determined at the slowest rate of pacing resulting instable atrial capture . The measurements were repeated attwo or more shorter cycle lengths (in 50- to 100-ms steps)
Figure 1 . Pacing protocols . A, In patients with normal intraventric-ular conduction during spontaneous sinus rhythm, the refractoryperiod of the bundle branches was measured by means of prematureatrial extrastimuli . B, When a bundle branch block pattern wasalready present during spontaneous sinus rhythm, postmature (in-stead of premature) atrial extrastimuli were applied to obtain nor-malization of conduction to measure the refractory period of thebundle branches. See text for details . S I = basic atrial pacedimpulses ; S2 = atrial extrastimuli .
to _as
at
t
10
Pt No.Age (yr)/Gender Diagnosis
ConductionDisturbance
1 52/F Systemic hypertension LBBB2 56/F Systemic hypertension LBBB3 28/F Systemic hypertension LBBB4 50/F Unknown RBBB5 551F Chagas heart disease LBBB6 48/F Idiopathic dilated cardiomyopathy LBBB7 75/F Postradiation cardiomyopathy LBBB8 381F Systemic hypertension LBBB9 58/M Ischemic heart disease RBBB10 54/F Idiopathic dilated cardiomyopathy LBBB11 42/F Unknown LBBB12 57/M Systemic hypertension LBBB13 48/M Systemic hypertension LBBB14 62/M Chronic obstructive lung disease RBBB15 71/F Systemic hypertension LBBB16 70M Unknown RBBB

JACC Vol. 23, No. 3PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES
March 1 . 1994:724-32726
CHIALE ET AL.
and compared with the baseline values . To evaluate theeffects of the duration of overdrive pacing, the refractoryperiod of the bundle branches was measured at 1, 3, 5, 8 and10 min of a single 10-min period of continuous atrial pacingat a selected cycle length (Fig1, A and B, bottom panels) byintroducing the mama] extrastimulus after every 8 consecutivebasic paced impulses .* These values were compared withthe baseline value obtained after trains of eight paced beatsat the same cycle length separated by 9-s intervals of sinusrhythm . The measurements of the refractory period weremade at least three times for reproducibility and the valuefound in most (two of three or three of four) of the successivemeasurements was taken as representative . In two patients,the study was repeated under different baseline conditions .Fj&.as with functional bundle branch block . We also
studied 10 patients (five men and five women, aged 18 to 35years) without any evidence of structural heart disease andwith a negative ajmaline test resuitt to exclude any latent orinapparent conduction disturbance in the bundle branches(14). All had been referred for evaluation of frequent supraventricular premature beats (n = 4) or recurrent parox-ysmal supraventricular tachycardias (n = 6) . All showed abundle branch block pattern exclusively in early prematureatrial impulses, complying with the rules of functional bun-dle branch block (2,5,6) . The six patients with supraventric-ular tachycardia underwent intracardiac pacing recordings,whereas the remaining four patients were studied by trans-esophageal atrial pacing. The same pacing protocol de-scribed for patients with tachycardia-dependent bundlebranch block and normal ventricular conduction during sinusrhythm (Fig . IA) vas used. The response of the refractoryperiod of the bundle branches to changes in the driving rateas well as during the 10-min period of overdrive pacing wasalso assessed after the intravenous administration of ajmaeline in all patients with functional bundle branch block, aswell as in three patients with tachycardia-dependent bundlebranch block (reasons for this are explained later) . In pa-tients with functional bundle branch block, ajmaline wasadministered in a single dose of I mg/kg body weight(without exceeding 70 mg), whereas relatively low doses (25to 50 mg) were given to patients with tachycardia-dependentbundle branch block.
All procedures were performed with patients in thepostabsorptive nonsedated state . Cardioactive drugs werediscontinued for ?_-5 half-lives before the study . None of thepatients was suffering from any acute illness or electrolyteabnormality . The study was approved by the Ethical Boardof the Ramos Mejia hospital . Each patient was informed
* To abbreviate the assessment of the refractory period of the bundlebranches at 1, 1 5, 8 and 10 min of continuous pacing, S I S2 intervals wereselected in every case, according to the results of the baseline studies .
t A negative ajmaline test result implies the absence of a bundle branchblock pattern at the peak effect of the drug (I to 3 min after intravenousadministration) (14) .
about the details o.,' the study and signed a written consentform .
Statislics. One-way analysis of variance (ANOVA) andTukey Honest Significant Difference for unequal sample sizetest were used to assess comparatively the duration of therefractory period of the bundle branches both in patientswith functional and in those with tachycardia-dependentbundle branch block . The baseline values were comparedwith those obtained at the shortest cycle length and thoseshowing the maximal prolongation or shortening of refracto-riness, irrespective of the elapsed time of pacing during the10-min period of continuous overdrive pacing . The relationbetween the variables at baseline and after a 10-min period ofcontinuous overdrive pacing was studied by the Pearson(product moment) correlation coefficient . Significance refersto a value of p < 0.05 .
Results
At the longest basic cycle length (mean 7 10 ms in patientswith funtional bundle branch block and 811 ms in those withtachycardia-dependent bundle branch block), the refractoryperiod of the bundle branches in the patients with functionalbundle branch block measured 430 ± 32 ms (range 390 to460) (Table 2, Fig. 2A [bottom panel]) . Refractoriness wassignificantly longer in the patients with tachycardia-dependent bundle branch block (611 ± 184 ms in 17 studies*(range 450 to 1,060, p < 0.01) (Table 3, Fig. 2A [top panel]) .This prolongation of refractoriness is one of the earliestmanifest electrophysiologic abnormalities caused by diseasein the bundle branches . However, there was some overlap inthe duration of the refractory period between the two groupsof patients
Effects of Increased rates of pacing . In all 10 patients withfunctional bundle branch block, shortening of the cyclelength consistently shortened refractoriness in the bundlebranches, from 430 ± 32 ms (at the longest cycle length) to368 ± 30 ms (at the shortest cycle length) (Table 2, Fig . 2A,bottom panel) . The refractory period at the shortest basiccycle length was overestimated because it was shorter thanthe shortest H 1 H2 interval in 8 of these 10 cases . In contrast,in the 16 patients (17 studies)* with tachycardia-dependentbundle branch block, , atrial overdriving resulted in a slightmean prolongation of the refractory period from 611 ± 184 to631 ± 246 ms (Table 3), whereas in 5 of the 17 studies (Fig .2A [top panel]) overdrive pacing was shown to shortenrefractoriness as in those with functional bundle branchblock. However, when the remaining 12 studies were ana-lyzed separately, shortening of the cycle length resulted in amarked prolongation of the refractory period from 666 ± 193to 750 ± 220 ms (p < 0.0002 compared with cases of
* In one study (Patient 9, study b), the rate-dependent response could notbe assessed because the refractory period of the bundle branches was shorterthan the shortest HIH 2 interval that could be obtained at every basic cyclelength .

Rate-Dependent Changes in Bundle Branch Refractoriness i
functional bundle branch block) . Thus, values for refracto-riness of the bundle branches in patients with functional andtachycardia-dependent bundle branch block clearly divergedfrom each other as cycle length was shortened (Fig . 2A) .
Effects of the duration of overdrive pacing . A furtherdifference in the response to rapid atria] pacing between thepatients with functional and tachycardia-dependent bundlebranch block was observed when the overdrive pacing lastedfor several minutes. At baseline, no significant differenceswere found in the refractory period of patients with eitherfunctional or tachycardia-dependent bundle branch block(Tables 2 and 4, Fig . 2B) . However, a slight shortening of therefractory period (from 410 ± 25 to 392 ± 21 ms, r = 0 .85,p = NS) occurred in all five patients with functional bundlebranch block whereas a clear-cut prolongation (from 656 ±208 to 774 ± 228 ms, r = 0 .94, p < 0.0001) was demonstratedin 15 of 18 studies of patients with tachycardia-dependent
bundle branch block . This resulted again in a larger differ-ence in the duration of the refractory period in both groupsof patients (p < 0.02). Furthermore, although the maximal
shortening of the refractory period was reached within the1st min with a flat response thereafter in patients withfunctional bundle branch block, the overdrive prolongationof refractoriness occurring in patients with tachycardia-dependent bundle branch block developed more graduallyover several minutes in 15 of 18 studies. In 6 of the studies inwhich the changes could be assessed throughout the 10-minperiod of continuous pacing, the steady state duration ofrefractoriness was reached within 3 to 8 min in 5 of the 6studies, whereas in the remaining study the refractory period
Patients with Functional BBB
* Control bundle branch refractory period (ms) . 1, Time for the maximal observed change (min), BBB = bundle branch block ; BBRP = bundle branch blockrefractory period ; BCL = basic cycle length ; LAH = left anterior herniblock ; LPH = left posterior hemiblock ; LBBB = left bundle branch block ; Pt = patient ;RBBB = right bundle branch block .
was found to be longer at 10 min than at 8 min . Thiscumulative or time-dependent prolongation of refractorinessat a fixed rate of pacing results in abnormal bundle branchconduction occurring at progressively longer cycle lengths(Fig . 3 and 4) and is essentially similar to the response that inother cardiac tissues is often referred to as "fatigue" (15,16) .
Different responses to overdrive pacing in tachyeardia-dependent bundle branch block . Although the patients withfunctional bundle branch block had a response to overdrivepacing that uniformly consisted of a rapid shortening of therefractory period, three different response patterns wereobserved in those with tachycardia-dependent bundlebranch block. A cumulative (rate and time-dependent) pro-longation of refractoriness was documented in 12 of 17studies (type I response) (Fig . 3). In two other studies, therefractory period demonstrated a rate-dependent shorteningand a time-dependent prolongation (type II response) (Fig .4). In the remaining three studies, there was a rapid short-ening response similar to that occurring in all cases offunctional bundle branch block and normal bundle branchesand this was called type N response .
Prima facie, a type II response is "less abnormal" than atype I response and although the bundle branches are proneto fatigue in both circumstances, these two different re-sponses may indicate two different degrees of bundle branchinvolvement. Conversely, a type N response, which isindistinguishable from that occurring in patients with normalbundle branches, may be related to an even lesser degree ofbundle branch involvement . To test this possibility, ajmalinewas administered to the three patients with a type N response .
12345
678910
700700700800700700600800700700
420440390480
460450390460400410
RBBBRBBBRBBB
RBBB + LABRBBB
RBBB + LAHLBBBRBBBRBBBRBBB
500
500
400500
450600400500500
550
<390<380330
<360<410400
<320<370<340<380
RBBB + LPH
RBBB + LAH
-7 .1-13 .6-15 .4-25-10 .8-11 .1-17 .9-19 .5-15
-13
Time-Dependent Changes in Bundle Branch Refractoriness in Patients with Functional BBB
1 600 400* RBBB 390 RBBB -2 .52 600 420* RBBB 400 RBBB -4 .73 600 370* RBBB I t. 360 RBBB -2 .74 600 430* RBBB + LAH 31 390 RBBB + LAH -9 .35 600 430* RBBB It 420 RBBB -2 .3
JACC Vol, 23, No . 3March 1, 1994 :724-32 Ct-HALE ET AL .
PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES 727
Table 2 . Overdrive-Induced Changes of Refractoriness of the undle Branches in Patients With Functional Bundle Branch BlockLongest ShortestBCL Control BCL
Pt No. (ms) BBRP (ms) QRS Cortigurabon (ms)
BBRP (ms)
QRS Configuration % Change

728
CHIALE ET AL .PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES
TD 44NOW
soon
A .P.
AT .
JACC Vol . 23, No. 3March 1, 1994 :724-32
Figure 2 . Rate- (A) and time- (B) related responses of the refractory
three patients as well as a further cumulative prolongationperiod of the bundle branches in patients with tachycardia-
induced by overdrive pacing (Fig . 5). This conversion of adependent bundle branch block (TD-BBB) and functional bundle
type N response into a type I response strongly suggestsbranch block (F-BBB) . In patients with functional bundle branchblock, the refractory period of the bundle branches shortened
that, although of minor degree, some abnormality was stillconsiderably as the basic cycle length (BCL) was decreased,
present in the bundle branches of these two patients .whereas a minor shortening occurred during a 10-min period ofcontinuous overdriving, In contrast, the refractory period of thebundle branches (BBRP) in patients with tachycardia-dependentbundle branch block showed a rate-dependent (12 of 17 studies) and
Table 3. Rate-Dependent Changes in Bundle Branchtime-dependent (15 of 18 studies) prolongation . However, a rate-
Refractoriness in Patients With Tachycardia-Dependent Bundleand time-dependent shortening similar to that occurring in cases of
Branch Blockfunctional bundle branch block was obtained in five and threepatients, respectively, with tachycardia-dependent bundle branchblock . Note that this shortening occurred in those patients who hada refractory period of the bundle branches as short as that in patientswith functional bundle branch block, A .P . = atrial pacing .
Effects of ajmaline. In all 10 cases of functional bundlebranch block, ajmaline caused a mild (10 to 40 ms) butconsistent shortening of the refractory period in accordancewith the effect of this drug on action potential duration ofisolated normal Purkinje fibers (17) and in contrast to itseffects on patients with tachycardia-dependent bundlebranch block, in whom ajmaline generally causes a markedprolongation of refractoriness (18) . In addition, the type Nresponse to overdrive pacing was unaffected by ajmalineadministration in all 10 patients with functional bundlebranch block .
When ajmaline was administered to the three patientswith tachycardia-dependent bundle branch block and a typeN re onse (Patients , 8 a d 12 , a s stan l pr ongation
a) and b) are results from two different studies performed in Patients 9 andof the baseline refractory period was observed in two of the
14, 4 and 2 months apart, respectively . Abbreviations as in Table 2 .
Pt No .
LongestBCL(ms) BBRP (ms)
ShortestBCL(ms) BBRP (ms) % Change
1 600 450 500 >500 +112 750 560 500 650 +163 800 570 650 600 +5 .34 850 690 750 2!750 +8.75 800 460 450 380 -17 .46 800 460 450 380 -17 .47 700 460 600 550 +19.68 NXI 460 500 40) -139 a) 60) 490 500 L-500 +2
b) 700 <470 500 <470 -10 900 930 600 970 +4 .3I 1 800 870 500 950 +9 .212 1000 520 700 450 -13 .513 900 610 600 700 +14 .714 a) 900 1060 600 1240 +16 .9
b) 900 490 400 370 -2515 850 620 700 800 +4 .816 850 690 700 800 +15 .9

JACC Vol . 23, No . 3March I, 1994 :724-32
Table 4. Time-Dependent Changes in Bundle BranchRefractoriness in Patients With Tachycardia-DependentBundle Brar,;h Block
a) and b) as in Table 3 . Abbreviations as in Table 2 .
DiscussionBundle branch refractoriness in patients with functional
bundle branch block. In three previous studies (6,8,9), theduration of refractoriness ranged torn <305 to 500 ms forcycle lengths varying between 380 and 1,000 ms . Similarfigures were obtained in our 10 patients with Functionalbundle branch block, in whom we also confirmed that atrial
Figure 3. Patient M Rate- (A) and time- (B) depen-dent prolongation of refractoriness of the right bun-dle branch (type I response) in a patient withtachycardia-dependent right bundle branch block .The refractor) period of the right bundle branchlasted 1,060 ms at a basic cycle length (BCL) of900 ms and increased to 1,240 ms as the basic cyckelength was decreased to 600 ms (A) . The refractoryperiod of the right bundle branch was also pro-longed from 1,090 ms at baseline to 1,320 ms after3 min of continuous atrial pacing at a basic cyclelength of 800 ms ,B) . Thereafter, long enough dia-stolic intervals could not be obtained to assessfurther changes in the refractory period . Note that asmall degree of right bundle branch block doespersist after expiration of the refractory period .HBE = His bundle electrogram .
CHIALE ET AL,
729PROLONGED REFRACTORINESS IN THE BUNDLE BRAWHES
overdrive pacing consistently and uniformly shortened therefractcry period of the bundle branches (type N response) .In addition, we also showed that this effect reaches a steadystate within the 1st min of overdrive pacing (19) and that theadministration of ajmaline also results in shortening of therefractoriness .
Bundle branch refractoriness in patients with tachyeardia-dependent bundle branch block. Our results in 16 patients(18 studies) with tachycardia-dependent bundle branch blockshowed that 1) overdrive pacing caused a cumulative pro-longation of the refractory period of the diseased bundlebranch in 83% of studies, with typical manifestations offatigue; 2) overdrive prolongation of refractoriness wasfound to be both rate- and time-dependent (type I response)in 70 .611/o of studies, whereas in 12 .4% it was criticallydependent on the duration of overdrive pacing (type 11response); and 3) in two of three patients with a type Nresponse, the administration of ajmaline, a potent sodiumchannel blocking drug (I'), resulted in the conversion of thetype N response into a type I response, suggesting that-sodium channel dysfunction" was a possible pathogeniccomponent of the prolongation of the refractory period .
Fatigue in the intraventricular conducting system. Theconcept of fatigue was originally developed in relation toconductivity in the atrioventricular (AV) node (20) anddefined as the prolongation of the nodal conduction time thatdevelops slowly during a fast rate and dissipates slowly afterits termination (16) . It has been attributed to a cumulativeeffect on refractoriness and an increase in the diastolicthreshold for electrical excitability (15,16,21) . Fatigue orfatiguelike effects have also been demonstrated in the intactinjured His-Purkinje system (22) and depressed Purkinjefibers (23-25) . In all these studies, fatigue was associated
CONTROL SCL 800 msI
V, -ij
HBEH-t4 ,
1100
V, --i-A
HBE -14 'H-H ; 05901
-Ar-i13 '0:2
J'L_
Pt No.BCL(ms)
ControlBBRP(ms)
Time for theMaximalObservedChange
BBRP(ms) Change
I 4111 450 5 min 5 0 +112 500 650 8 min 800 +233 650 600 5 min 840 +404 750 750 3 min 850 +135 600 420 5 min 390 -7 .16 500 400 8 min L-500 +257 600 550 30s X600 +98 600 410 5 min 380 -7.39 a) 600 490 5 min 740 -151
b) 500 <470 10 Olin 2!500 +6.410 600 970 5 min 1,030 +5 .111 800 870 5 min 1,0W +14.912 806 480 5 min 440 -8 .313 60 700 3 min 750 +7 .414 a) 800 1090 3 min 1 .320 +21
b) 600 410 1 min -600 +4b .315 700 650 2 min 700 +7.616 7PO 800 3 min 890 +11 .2

730
CHIALE ET AL.PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES
rANW CONTROL BCL 800 ma t min
OCL 800 me
H ~ WSE 4f41H-H
470
3 min
with postrepolarization refractoriness . Some reports (12,26-.30) have suggested the occurrence of fatigue in humandiseased bundle branches, but the underlying mechanismwas not studied in detail in any of these latter reports . Ourstudy appears to be the first in which fatigue in humanbundle branches was systematically investigated by measur-ing rate- and time-dependent changes in refractoriness dur-ing orthograde (atrial) stimulation and in the presence of aminimal or modest degree of bundle branch disease . Under
800 me
I
600 me
5 min
430
1
3941
L
VI
HaE -441'
J# '.
I :
AJMALINE 25 mg IV
®00 m® so me
Rn
JACC Vol. 23, No. 3March 1,1994:724-32
Figure 4 . Patient 6. Biphasic re-sponse of refractoriness of the leftbundle branch during continuousatrial pacing. At a basic cyclelength (BCL) of 500 ms, a gradualand mild shortening of the refrac-tory period of the left bundlebranch from 400 to 380, 370 and360 ms occurred after 1, 3 and5 min, respectively, of continuouspacing (A). However, 2 :1 left bun-dle branch block was elicited after8 min of pacing, indicating that therefractory period of the left bundlebranch had been prolonged to500 ms (B) . Soon after that, a 3 :1left bundle branch block disclosingan additional prolongation of re-fractoriness of the left bundlebranch was observed. HBE m His
s
bundle electrogram .
such conditions, overdrive pacing was shown to result in arate- and time-dependent deterioration of conduction in mostof our patients with tachycardia-dependent bundle branchblock, and this form of fatigue was shown to be related to acumulative prolongation of the refractory period .
Mechanism of the overdrive prolongation of refractoriness.The rapid shortening of the refractory period caused byoverdrive pacing in the patients with functional bundlebranch block should be attributed to a parallel shortening of
Figure S. Prolongation of refractori-ness of the left bundle branch andconversion of a type N to a type Iresponse by ajmaline . In the controlstudy (A), the refractory period of theleft bundle branch measured 460 msat a basic cycle length (BCL) of800 ms and shortened to 420 and380 ms as the cycle length was de-creased to 600 and 500 ms, respec-tively . A mild shortening of refracto-riness of the left bundle branch alsooccurred during a 10-min period ofcontinuous atria] pacing (not shown).After a low dose of ajmaline (25 mgintravenously [IV]) (B), the refrac-tory period of the left bundle branchwas prolonged by 210 ms (from 460 to670 ms) at a basic cycle length of800 ms. A marked lengthening to>970 ms occurred when the basiccycle length was shortened to 600 ms .Likewise, a substantial prolongationof the refractory period of the leftbundle branch was also obtained af-ter 3 min of continuous pacing (notshown). HBE = His bundle electro-gram.

JACC Vol . 23, No . 3 CHiALE ET AL .
731March 3, 1994:724-32
PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES
the action potential duration (250102). The changes inconductance and ion concentrations underlying this shorten-ing are well known (33) . However, little is known about themechanism of the slow prolongation of the refractory periodin the patients with tachycardia-dependent bundle branchblock. Because there is no apparent reason why the changesin conductancec and ion concentrations caused by overdrivepacing should be any different from those occurring in thenormal bundle branches, it must be assumed that in diseasedbundle branches, overdrive pacing shifts the action potentialand refractoriness durations in opposite directions, resultingin the occurrence (or magnification) of postrepolarizationrefractoriness (25,34) . Conversely, in a previous study (35),procainamide caused a large prolongation of refractorinessin diseased bundle branches, whereas verapamil (whichincreases or facilitates fatigue in the AV node [36]) failed toproduce any significant change . Moreover, in the presentstudy, the administration of aijwaline resulted in conversionfrom a type N (normal) response to a type I (rate- andtime-dependent prolongation of refractoriness) response intwo of three patients with tachycardia-dependent bundlebranch block . In addition, Takahashi et al . (22) found thatlidocaine increased whereas verapamil reduced the degree ofoverdrive suppression of conduction induced in the "invivo" injured canine His-Purkinje system . The corollary isthat sodium channel blockers promote or facilitate fatigue indiseased bundle branches, whereas calcium antagonists fa-cilitate fatigue in the AV node, strongly suggesting a differ-ent ionic basis for these two forms of fatigue .
Is there a selective involvement of sodium channels? Sev-eral selective sodium channel blockers are known to slowrecovery from inactivation and cause by themselves post-repolarization refractoriness (37-40) that is also rate- andtime-dependent (38-42) and therefore remarkably similar tothe overdrive prolongation of refractoriness occurring inpatients with tachycardia-dependent bundle branch block .This similarity suggests that both effects-one caused bydisease and the other by the drugs-might be exerted at thesame locus within the molecular structure of the sodiumchannel . This locus might be in or close to the inactivation"gate," which has been implied as the drug receptor site(43,44) . A selective involvement of ionic channels may beviewed as an attractive hypothesis that . deserves furtherinvestigation .
Paced versus natural acceleration of the heart rate . Pacingstudies suffer from the limitation that they cannot be directlyextrapolated to the clinical setting. Under natural condi-tions, cardiac acceleration is due to a predominance ofsympathetic tone, which by itself shortens refractoriness(4,45) . Actually, if the cardiac rate is accelerated eitherby exercising or atropine administration in patients withtachycardia-dependent bundle branch block, the result isgenerally shortening of refractoriness in the bundle branches(46) . Unpublished studies from our laboratory show thatoverdrive prolongation of the refractory period can beentirely reversed or prevented by administration of isopro-
terencl . Catecholamines have also been shown (47) to re-verse the prolongation of refractoriness induced by sodiumchannel blockers .
Implications. The rate- and time-dependent prolongationof the refractory period of ' :eased bundle branches dem-onstrated in our study sheds new light on several apparentlypuzzling observations, such as the "nonrate-related" bundlebranch block and paroxysmal infra-His AV block occurringafter several or many cycles of equal length (48,49) and the"unexpected" or "unpredictable" drop of a single beat incases of Mobitz 11 block (50) . It is also conceivable thatoverdrive prolongation of refractoriness may develop indiseased cardiac tissues at the same time that shorteningoccurs in normal adjacent tissues, setting the stage for theoccurrence of reentrant activity . Conversely, the prolonga-tion of refractoriness could explain the self-limited characterof some cardiac tachyarrhythmias and be involved in theantiarrhythmic effects of overdriving . Overdrive pacing maybe used to differentiate functional from pathologic bundlebranch block in cases in which the clinical significance of theconduction disturbance is uncertain. However, it must bestressed that at critically rapid rates, perpetuation of func-tional bundle branch block may occur as a result of con-cealed retrograde invasion into the bundle branch .
We are grateful to Brian F. Hoffman. MD for valuable and constructivecomments on this work, Julio D . Pastori, MD, M . Susana Halpern, MD andMarisa M . Martin, MD for help in the preparation of the manuscript andUlises Questa, PhD for the statistical analysis of results . The secretarial skillof Cecilia Mc Keon is also appreciated .
References
I . Lewis T. Observations upon disorders of the heart's action . Heart1912 ;3 :279-309 .
2 . Gonaux JL, Ashman R . Auricular fibrillation with aberration simulatingventricular paroxysmal tachycardia. Am Heart 11947;34 :366-73 .
3 . Langendorf R . Aberrant ventricular conduction . Am Heart J 1951 ;41 :700-15 .
4 . Moe OK, Mendez C, Han J . Aberrant impulse propagation in the dogheart: a study of functional bundle branch block . Circ Res 1%5;16 :261-86.
5 . Cohen SI, Lau S11, Haft JI, Damato AN . Experimental production ofaberrant ventricular conduction in man . Circulation 1967 ;36 :673-85 .
6. Denker S, Shenasa M, Gilbert CJ, Akhtar M . Effects of abrupt changes incycle length on refractoriness of the His-Purkinje system in man . Circu-lation 1983 ;67 :60-8.
7. Rosenbaum MB, Sanchez RA, Goicoechea R. Aberrant ventricularconduction during atria[ fibrillation . In : Touboul P, Waldo AL, editors .Atrial Arrhythmias : Current Concepts and Management . St . Louis, MO:Mosby-Year Book, 1990:163-8 .
8. Schuilenburg RM, Durrer 1) . Rate-dependency of functional block in thehuman His-bundle and bundle branch-Purkinje system . Circulation 1973~48 :526-40,
9. Denes P, Wu D, Dhingra R, Pietras RJ, Rosen KM . The effects of cyclelength on cardiac refractory periods in man . Circulation 1974;49 :32-41 .
10. Lazzari JO, Chiale PA, Halpern MS, Elizari MV, Rosenbaum MB . The"making" of a bundle branch block . In : Rosenbaum MB, Elizari MV,editors . Frontiers of Cardiac Electrophysiology . The Hague : MartinusNihjoff, 1983 :657-68 .
IL Rosenbaum MB, Elizari MV, Lazzari JO, Halpern MS, Nau GJ, Levi RJ .The mechanism of intermittent bundle branch block : relationship to

732
CHIALE ET AL .
prolonged recovery, hypopolarization and spontaneous diastolic depolar-ization . Chest 1973;63:666-72 .
12 . Fisch C, Zipes DP, McHer.ry PL. Rate-dependent aberrancy . Circulation1973-,49:714-24 .
13 . Dents P, Wu D, Dhingra R, Amat Y Leon F, Wyndham C, Rosen KM .Electrophysiologic observations in patients with rate-dependent bundlebranch block . Circulation 1975 ;51 :244-50 .
14 . Chiale PA, Przybylski JO, Wan RA, et al . Usefulness of the ajmaline testin patients with latent bundle branch block. Am J Cardiol 1982:49:21-5 .
15. Merideth J, Mendez C, Mueller WJ, Moe GK . Electrical excitability ofatrioventricular nodal cells . Circ Res 1968 ;23 :69-85 .
16. Billete J, Metayer R, St-Vincent M . Selective functional characteristics ofrate-induced fatigue in rabbit atrioventricular node . Circ Res 1968-,62 :790-9.
17. Pillat B, Heistracher P. Elektrophysiologische Unterschrigen uber dieWirkung von Ajmallne auf Reizleitungsfasern . Naunyn SchmiedebergsArch Pharmakal 1964,246 :375-88
19. Chiale PA, Przybylski J, Halpern MS . Lazzari 10, Elizari MV, Rosen-baum MB. Comparative effects of ajmaline on intermittent bundle branchblock and the Wolf-Parkinson-White syndrome. Am J Cardiol 1977;39 :651-7.
19. Miles WM, Prystowsky EN . Alteration of human right bundle branchrefractoriness by changes in duration of the atrial drive train . Circulation196603 :2444
20. Lewis T. Master AM . Observations upon conduction in the mammalianheart : AV conduction . Heart 1925 :12 :209-69 .
21 . Simwn MB, Spear JE Moore EN . Electrophysiologic studies on atrio-ventricular nodal Wenekebach cycles . Am J Cardiol 1978-,41 :244-58.
22 . Takahashi N, Gilmour Rl Jr . Zipes DP. Overdrive suppression ofconduction in the canine His-Purki* system after occlusion of theanterior septal artery . Circulation 1994;70:495-505 .
23 . Gilmour RF Jr, Salata A Zipes DP. Rate-related suppression andfacilitation of conduction in isolated canine cardiac Purkinje fibers . CircRes 1985 ;57:35-45.
24 . Anuelevitch C . Jalife J . Moe GK. Frequency-dependent alterations ofconduction in Purkirije fibers . In Ref 10:397-415 .
25 . Davidenko JM, Antzelevitch C . Electrophysiologic mechanisms underly-ing rate dependent changes of refractoriness in normal and segmentallydepressed canine PurkiNe fibers: the characteristics of postrepolarizationrefractoriness . Circ Res 191150 :257-68 .
26 . Range M, NarulaOS. "Fatigue phenomenon" in the human His-Purkinjesystem [abstract] . Circulation 1973;48Suppi IV : 103 .
27 . Narula OS, Runge M. Accommodation of A-V nodal conduction andfatigue phenomenon in the His-Purkinje system . In : Wellens HJJ, Lit KI,Jam MJ, editors: The Conduction System of the Heart . Leiden : StenfertKroese, 1976:529-44 .
28 . Fisch C . Bundle branch block after ventricular tachycardia : a manifesta.bon of *Iatigue" or "overdrive suppression ." J Am Coll Cardiol 1994 .3 :1562-4.
29. Lagondod R, Pick A . Artificial pacing of the human heart : its contribu-tion to the understanding of arrhythmias . Am J Cardiol 1971-,28 :516-25.
30. Wald RW, Waxman MB . Case report : depression of distal AV conductionfollowing ventricular pacing. PACE 1"1 ;4:84-8.
31 . Holtman BF, Cranefleld PE Electrophysiology of the Heart . New York :McGraw-Hill . 1960 :222-7.
JACC Vol. 23, No . 3PROLONGED REFRACTORINESS IN THE BUNDLE BRANCHES
March 1, 1994 :724-32
32. Moore EN, Preston JB, Moe GK . Durations of transmembrane actionpotentials and functional refractory periods of the canine false tendon andventricular myocardium: comparison in single fibers . Circ Res 1%5 -,17:259-73 .
33 . Carmeliet E . Repolarization and frequency in cardiac cells. J Physiol1977 ;73 :903-23 .
34 . Lazzara R, El-Sherif N, Scherlag BJ . Disorders of cellular electrophysi-ology produced by ischemia of the canine His bundle. Circ Res 1975,36:444-54 .
35 . Chiale PA, Pastori JD, Sanchez RA, Elizari MV, Rosenbaum MB .Contrasting effects of verapamil and procainamide on rate-dependentbundle branch block : pharmacologic evidence for the role of depressedsodium channel responses . J Am Coll Cardiol 1990-.15:633-9.
36. Curtis AB, Ellenbogen K, Wharton JM, Strauss HC . The frequency-dependent effects of verapamil on anterograde refractory periods andconduction in the atrioventricular node in man . J Cardiovasc Electrophys-iol 1992-,3:21-33 .
37 . Singh BN, Hanswirth D. Comparative mechanisms of action of antiar-rhythmic drugs. Am Heart J l97 , ; :" - 67-82.
38. Campbell TJ . Subclassification of class I antiaffhythmic drugs . In :Vaugham Williams EM, editor. Handbook of Experimental Pharmacol-ogy. Vol . 89: Antiarrhythmic Drugs . Berlin : Springer-Verlag, 1989:135-55 .
39. Nattel S, Zeng FD : Frequency-dependent effects of antiarrhi , qhmic drugson action potential duration and refractoriness of canine cardiac Purkirtjefibers. J Pharmacol Exp Ther 1984 ;229 :28 .3-91 .
40. Franz MR, Costard A . Frequency-dependent effects of quinidine on therelationship between action potential duration and refractoriness in thecanine heart in situ . Circulation 1988-.77 :1177-84.
41 . Campbell U Resting and rate-dependent depression of maximum rate ofdepolarization (V max) in guinea-pig ventricular action potentials bymexiletine, disopyramide and encainide . J Cardiovasc Pharmacol 1983-.5 :291-6.
42. Varro A, Elharrar V, Surawicz B . Frequency-dependent effects of severalclass I amitiffhythmic drugs on Vmax of action potential upstroke incanine cardiac Purkinje fibers. J Cardiovasc Pharmacol 1985 ;7 :482-92 .
43 . Cahalan M, Shapiro BI, Almers W . Relationship between inactivation ofsodium channels and block by quaternary derivatives of local anestheticsand other compounds . In : Fin BR, editor. Molecular Mechanisms ofAnesthesia. New York : Raven, 1980:17-33 .
44 . Armstrong CM . Sodium channels and gating currents . Physiol Rev1981 .61 :644-83.
45. Halpern MS . Chiale PA, Nau GJ, et al . Effects of isoproterenol onabnormal ventricular conduction . Circulation 1980:62 :1357-64 .
46 . Nau GJ, Elizari MV, Rosenbaum MB . Recovery of impulse propagationin the bundle branches of the human heart : the different varieties of phase3 bundle branch block . In Ref 10 :416-26.
47 . Calkins H, Sousa J. El-Atari R, Schmaltz S . Kadisch A, Morady F .Reversal of antiarrhythmic drug effects by epinephrine : quinidine versusamiodarone. J Am Coll Cardiol 1992 ;19:347-52.
48 . Wallace AG, Laszlo J . Mechanisms influencing conduction in a case ofintermittent bundle branch block . Am Heart J 1%1,61 :548-54.
49 . Levi RJ, Elizari MV, Lazzari JO, Nau GJ, Rosenbaum MB . Las difer-entes variedades del bloqueo AV paroxistico . Rev Lat Cardiol 1980;1 :82 -95 .
50 . Halpern MS, Nau GJ, Chiale PA, Elizari MV, Rosenbaum MB . Mecha-nism of Mobitz II periodicities . In Ref 10:465-87 .










![· 2019-05-07 · (i) Refractoriness under load (ii) Refractoriness [9+6] 6.(a) Explain moving bed catalytic cracking method with a neat labeled diagram. (b) Explain the terms octane](https://img.pdfslide.us/doc/110x75/5e72a6512887ad35820f60f8/2019-05-07-i-refractoriness-under-load-ii-refractoriness-96-6a-explain.jpg)








![diet.edu.indiet.edu.in/Downloads/EEE_PREVIOUS_QUESTION_PAPERS/2012/EEE_I-II_REG.p… · (i) Refractoriness under load (ii) Refractoriness [9+6] 6.(a) Explain moving bed catalytic](https://img.pdfslide.us/doc/110x75/5e72a6512887ad35820f60f9/dietedu-i-refractoriness-under-load-ii-refractoriness-96-6a-explain.jpg)







