Embed Size (px)
Citation preview

International Journal of Law and Psychiatry, Vol. 22, No. 5–6, pp. 581–601, 1999Copyright © 1999 Elsevier Science LtdPrinted in the USA. All rights reserved
0160-2527/99 $–see front matter
PII S0160-2527(99)00027-8
581
Overall Pattern of Health Care and Social Welfare Use by Injured Workers in the British Columbia Cohort
Clyde Hertzman,* Kimberlyn McGrail,† and Bob Hirtle‡
Introduction
In British Columbia (BC), workers injured during the course of their jobs re-ceive financial compensation, but through a process that is separate from thehealth care system and other elements of the social safety net, such as employ-ment insurance or social assistance. The distinct functioning of the workers’compensation system in BC, and similar systems in other jurisdictions, has itsorigins in the historic trade-off of workers giving up the right to sue their em-ployers, in return for fair compensation for work-related injuries. Though it isa separate piece, the experience of injured workers may have a great deal incommon with other people who are (temporarily or permanently) dependenton other parts of the social safety net.
This article is based upon a pioneering record linkage study that was carriedout to support the inquiries of the Royal Commission on Workers’ Compensa-tion in British Columbia, 1997–98 (Hertzman, McGrail, & Hirtle, 1998). Someof the questions raised by the inquiry were: What are some of the characteris-tics of the workers’ compensation population with respect to socioeconomicstatus (SES), and general experience with the compensation system? What isthe pattern of use of health and social services before and after a reportedworkplace injury? How do these patterns compare to a population matched byage and sex? If there are differences, how might they be explained based on
*Professor, Department of Health Care and Epidemiology, Faculty of Medicine, University of BritishColumbia, Vancouver, British Columbia, Canada.
†Research Associate, Centre for Health Services and Policy Research, University of British Columbia,Vancouver, British Columbia, Canada.
‡Research Associate, Department of Health Care and Epidemiology, University of British Columbia,Vancouver, British Columbia, Canada.
Address correspondence and reprint requests to Clyde Hertzman, Department of Health Care and Epi-demiology, Faculty of Medicine, University of British Columbia, Mather Building, 5804 Fairview Avenue,Vancouver, British Columbia, V6T 1Z3, Canada; E-mail: [email protected]

582 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
existing knowledge about workplace injury and related topics such as unem-ployment? And, does the workers’ compensation operate as an integratedpiece of the social safety net? This article addresses these issues by analyzingthe experience of workers who applied for and/or received workers’ compen-sation benefits in terms of their use of other types of health and social services;and evaluates whether these individuals differed from an age- and gender-matched comparison group who did not make claims to the Workers’ Com-pensation Board (WCB).
Methods
The data used here were derived from three sources: the WCB, the Ministryof Human Resources, and the BC Linked Health Database (BCLHD). In BC,the WCB system is funded exclusively by payroll levies on industry, and coversmore than 90% of the paid workforce. It is the only system through which em-ployees can make claim for compensation for a workplace injury. The WCBprovided computerized records of all injured workers claims from 1986 to1996. These files gave information on each successful claim: short-term disabil-ity, long-term disability (pension), fatality, or health care only, as well as thefact and date of all unsuccessful or incomplete claims. More than 800,000 indi-vidual claimants made more than 2 million claims to the WCB during those 11years.
The Ministry of Human Resources provided approximately 1.6 million In-come Assistance (welfare) records. These included all individuals (BC resi-dents) and their dependents who were awarded welfare benefits, as well asthose who applied but were deemed ineligible, between 1990 and 1997. If anyof these individuals had
also
made application for welfare between 1980 and1989, these events were retained as well.
1
The BCLHD, developed under contract with the BC Ministry of Health,makes six key transaction files in the province “linkable” to one another forthe purposes of research (Chamberlayne et al., 1998). These include: the birthfile, the death file, Medical Services Plan claims file (i.e., fee-for-service pay-ments to physicians and alternative providers), hospital discharge file, long-term care client file, and the Pharmacare A plan file (i.e., the provincial drugpayment plan for BC residents over 65 years of age). More than 95% ofrecords in each file, going back to fiscal year 1985/86, have been probabilisti-cally linked to a unique individual recorded on the Registration and PremiumBilling file maintained by the Medical Services Plan of BC.
2
BC, as all Cana-dian provinces, has a universal system of health care coverage, and there are
1
The (relatively) low linkage rate may imply that the true prevalence of welfare use among WCBclaimants is underreported here. However, there is good reason to believe that the linkage rate for thosewho actually received assistance, as opposed to those who applied for it but were turned down, is muchhigher than 75%.
2
The data in the BCLHD are owned by various stewards in and outside by the Ministry of Health, andare accessible to researchers under an access protocol that complies with BC’s Freedom of Information andProtection of Privacy Act.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 583
no copayments required for physician or hospital services. Thus the BCLHDrepresents a comprehensive, population-based linked data set.
Using “personal identifier fields” (names, birth dates, and postal codes) andsimilar probabilistic linkage methods, we were able to “link” 97.2% of WCBclaims and 75% of Income Assistance applications (successful and unsuccess-ful) to the BCLHD. A link was created when the personal identifier fieldsfrom the WCB and welfare files were successfully matched to an individual onthe Registration and Premium Billing file. Creation of such links meant thatresearchers could merge individuals’ specific claims histories from the WCBand welfare files with their history of use of health care services covered byBC’s universal access medicare system.
For the purposes of this project, a principal linked file was created as follows:
• All individuals who filed a claim with the WCB in 1991 were identified(herein, the “1991 injury cohort”).
• The WCB records of these individuals for the full period available to us(1986–1996) were merged.
• This file was linked with the Medical Services Plan (MSP) and hospitaldischarge records for the same time period.
• This file was then further linked with the Income Assistance file (herein,“welfare”).
• Using these linked files, we created individual “trajectories” for the 1991cohort, organized in time sequence, of all medical and hospital encoun-ters funded by the WCB and the BC Ministry of Health, as well as all in-jury claims and encounters with the welfare system.
• By matching on age and gender, we created a comparison population ofpeople who were registered for health benefits, but who did not file aWCB claim over the period 1986 to 1996. The limited information avail-able on the registration file made it impossible to consider matching onmore than these two variables.
To limit the size of the analysis cohort, most analyses—except some re-stricted to the WCB file alone—included only the 1991 injury cohort. The 1991injury cohort includes people who were also injured in other years, peoplewho made multiple claims in 1991, and people who reported injuries to theWCB in 1991 but were not compensated for them. This latter situation canarise when a claim is incomplete—that is, not all paperwork is filed, or theclaimant decides not to follow up—as well as when the claim is adjudicatedand turned down by the WCB. There is no way within these data to separatethese two groups. Unless otherwise noted, the analyses include the entire 1991injury cohort, not just those who were awarded claims by the WCB.
In some cases, there were limits put on the 1991 injury cohort. For example,to eliminate the effects of prior claims (at least as far as possible given data be-tween 1986 and 1996), a subgroup of “first claimants” was identified. Theseare individuals who reported an injury to the WCB for the first time in 1991.The text notes whenever such subgroups were created and used.
The analysis of linked data is usually based on the construction of trajecto-ries of care for individuals. In this case, all fee-for-service payments to physi-

584 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
cians and alternative providers, as well as all hospital separations, were assem-bled for the 1991 injury cohort and the matched cohort. Various measures ofhealth services utilization, such as the proportion of each group that visited aGeneral Practitioner (GP) during a given year, were developed from these tra-jectories. The intent was to look at their use of health and social services,based on the BCLHD and welfare data, and to describe any recurring pat-terns.
Results
Between 1986 and 1996, the WCB recorded 2,236,624 total claims, repre-senting 874,334 unique individuals (an average of approximately 2.5 claims perclaimant). Of these, we were able to link 2,172,984, or 97.2%. There were203,898 unique claims with a 1991 injury year, of which 198,255 were linked(97.2%), a rate consistent with overall linkage rates. These claims were madeby 163,338 unique people, for an average of 1.2 claims per person
in 1991.
Thisimplies both that there are workers who make multiple claims within 1 calen-dar year, and that some of these workers also made claims in other years. Thelatter is reinforced if one considers that more than 19% of total claimants overthe period 1986 to 1996 make a claim in 1991 (163,338 out of 874,334).
There were 8,126 workers who reported injuries in 1991 who filed 12 ormore claims between 1986 and 1996. These workers (the “repeat claimants”)represented 5% of the total 1991 injury cohort, and made 124,209 uniqueclaims between 1986 and 1996. Throughout the entire study period, each ofthese workers filed an average of 1.9 claims per year. This value peaked at 2.0in 1989 and 1990.
The total number of claims made over the study period by the 1991 injurycohort is highly skewed. Just over 20% of workers reported only one injury tothe WCB between 1986 and 1997, and nearly three quarters of the cohort re-port five or fewer. The remaining 25% reported between 6 and 50 claims overthis 12-year period.
It should be emphasized that these numbers represent
different
injuries inother years—that is, this is not a carryover of the 1991 injury event to subse-quent years. There are probably a small proportion of injuries that are as-signed different claim numbers, but upon review are determined to be thesame. However, that would have little effect on the numbers here.
The average age of the 1991 injury cohort is 35.6 years and the majority ofinjuries take place in the 20s, 30s, and 40s. There is no significant difference inaverage age comparing short-term disability/long-term disability/pension,medical care only, and “other” claimants (calculations not shown).
Distribution of Injury Claims by Gender and Socioeconomic Status, 1986to 1996
Combined gender and socioeconomic data were available for 92% of 1986and 1991 awarded claims, and 77% of 1996 awarded claims. (Presumably, 1996was still being updated when we were given the file). SES is determined eco-logically based on the decile of average family income of the injured worker’s

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 585
postal code area, using a ranking method developed at Statistics Canada (Ng,Wilkins, Pole, & Adams, 1997). These data were processed separately formales and females. Similar patterns were found in both, so the results only formales are shown below.
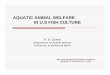
Figure 1 presents these data. For all 3 years, the number of claims peakedwithin the third SES decile and declined as SES decile increased (decile 1
5
lowest SES, 10
5
highest SES). The percentage of claims falling into each ofthe 4 lowest deciles increased continuously across the 3 study years. Con-versely, there was a continuous downward trend for the three highest deciles.The single largest change was the decline in awarded claims between 1991 and1996 for the highest SES decile. The rate of claims in this highest decile wasless than half that of the third decile (where claims are highest).
Injury Claims and Months on the Job, 1986 to 1996
There is a strong inverse relationship between length of time on the job andinjury rate (Figure 2). This is punctuated by an apparent tendency to round“duration on the job” to the nearest half year. The following trends were ap-parent for each of the three study years: (a) More than 30% of all injuries oc-curred within the first 5 months of employment, 50% within the first 18months, (b) Ignoring the half year figures, injury rates declined steadily overthe first 5 months.
One explanation for this phenomenon is that younger workers, who aremore prone to injury because of inexperience, are also more likely to be in thefirst few months of a job. The relationship between 1991 injuries, months onthe job, and age group are graphed in Figure 3. For workers aged 15 to 24,22.8% of compensated injuries occurred in the first month on the job. This fig-
FIGURE 1. Percentage of male claims attributable to socioeconomic (SES) decile.

586 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
ure was 16.2% for 25- to 34-year-olds and 10.7% for those over 35. Among 15-to 24-year-olds, over 50% of all compensated injuries occurred within the first5 months. Among those aged 25 to 34, the 50% mark was passed in the twelfthmonth. For those over 35, it took 3 years to reach the 50% mark. Thus, agetends to attenuate but not eliminate the risks of injury during the first fewmonths of a new job.
FIGURE 2. The relationship between injury incidence and months on the job.
FIGURE 3. The relationship between age-specific 1991 injury incidence and months on the job.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 587
The likelihood of injury within the first month on the job varies widely byindustry, from 2% in health and social services to 41% in construction. Almostthree quarters of injuries in construction, in fact, occur within 6 months on thejob. This trend may relate both to the nature of the work (i.e., high propensityfor injury) and the fact that each construction site can be counted as a new job(i.e., there is a greater proportion of the workforce in their first 6 months ofemployment on a particular site). Yet, more than half of all worker injuries oc-cur within the first 2 years on the job in all industries except government, edu-cation, and health and social services.
Repeat Claimants and Months on the Job
Number of months on the job was available for about the same proportionof the 1991 “repeat claimants” group as for the entire injury cohort. Between1986 and 1990, more than 40% of the claims awarded to “repeat claimants”were for injuries occurring during the first year on a job. After 1991, this num-ber dropped to approximately 30% (Figure 4).
The high likelihood of injury for these “repeat claimants” in the first yearon a job over an 11-year time frame implies a propensity for frequent jobchange among this group. One interpretation of these numbers is that the re-ported injury effectively ends employment, is then followed by re-employmentat a different location, and then another injury. While this is likely not the onlypattern that would be found with a closer examination of these high users, thefact of repeated claims and the high proportion of injuries early in the cycle ofemployment suggests that it does fit for some proportion of this group.
FIGURE 4. Percentage of repeat claimants injured during their first 12 months on a job, by year,1986–1996.

588 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
Lag Times Between Injury and Payment Dates
A major issue with any compensation system is the time it takes betweenmaking a claim and receiving payment for that claim. There are 81,180 uniqueclaim numbers associated with awarded claims for lost time on the job in 1991.Lag times between month/year of injury and month/year of the first paymentwere calculated for 80,082 records (99.6%) for which sufficient data wereavailable. The median wait for payment was 1 month. Payment was made for90% of all claims within 4 months. Ninety-seven percent received paymentwithin 10 months. 3,402 pension records (awarded for permanent disability ordeath) were analyzed to determine the wait time between injuries and finan-cial awards. In this analysis, the compensation date was taken as the earlier ofpension effective date or award payment date.
Sixty-five percent of 1991 pensioners received interim compensation awardsprior to their pension being effective. Seventeen percent received compensa-tion awards around the same time as their pension became effective and 18%had pensions become effective before receiving other compensation awards.The median wait for compensation was 4 months. Ninety percent of pension-ers received compensation within 10 months. Six and one half percent waited ayear or more, 1.6%, 2 years or more, and 0.5%, more than 3 years.
Physician Services Utilization
Many individuals who report injuries to the WCB also require health careservices provided through the BC medical system. It was expected that use ofthese services, outside what may be compensated by the WCB related to aworkplace injury, would not be significantly greater than a population similar
FIGURE 5. Percentage of 1991 injury cohort and cohort matched by age and gender who visit ageneral practitioner at least once per year, 1986–1995. WCB 5 Workers’ Compensation Board.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 589
in age and gender who did not report injuries to the WCB. If anything, itwould have been anticipated that health services utilization would be less, dueto the frequently observed “healthy worker effect” (Checkoway, Pearce, &Crawford-Brown, 1989). All use of MSP, unless otherwise noted, excludespayments to providers made by the WCB. In other words, the trends seen hereshould represent patterns of care for the injury cohort for medical problemsthat are unrelated to compensable WCB injuries.
Figure 5 shows the proportion of the 1991 injury cohort and the matched co-hort that visited GPs during each year from 1986 through 1995. The propor-tion of the injury cohort that visited GPs increased to the injury year (1991),peaked during 1991, and then decreased somewhat, though not to former lev-els. In comparison, there was a slow but steady (age-related) increase in theproportion of the matched cohort who visited GPs during these years, thoughthe number remained lower throughout. WCB claimants were far more likelythan nonclaimants to make a GP visit in any given year. The minimum differ-ence was about 50%, but was closer to 100% in 1991, the injury year. A similarpattern was observed for visits to specialists (data not shown).
The trend in these charts implies two conclusions. First, individuals whomake claims to the WCB are more frequent users of physician services thanthe general population. Second, some individuals appear to permanently in-crease their use of physician services following an injury claim to WCB. Onedifficulty with the latter conclusion is that many people in the 1991 injury co-hort also made claims to the WCB in previous years. As a result of these inju-ries, they may have chronic conditions that now require more constant atten-tion from physicians.
In order to assess this effect we re-analyzed the data limiting the 1991 injurycohort to “first claimants” (first, at least, since 1986, which is the first year for
FIGURE 6. Percentage of 1991 injury cohort first claimants and cohort matched by age and gen-der who visit a general practitioner at least once per year, 1986–1995. WCB 5 Workers’ Compen-sation Board.

590 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
which we have linked WCB data). This restriction limits the cohort size to68,924 individuals. Figure 6 shows patterns of GP contact for these individuals,by year (the pattern for specialists is again similar, so is not shown). The differ-ence between the injury cohort and matched cohort persists.
“Acute” and “Chronic” Injuries
The use of physician services by the WCB injury cohort exhibits patternsthat are different from the group matched for age and gender. To more fullyexplore the potential reasons for these differences, we created two subsets ofthe injury cohort; one including people with “acute” injuries, and one includ-ing those with more chronic injuries. The hypothesis was that the “acute”group would be more similar in use of physician services to the matched co-hort, while the “chronic” group, because of the nature of their injuries, wouldhave higher use. For both groups, a subset of the matched cohort was defined,again based on age and gender characteristics of each group. The acute and re-volving door groups were then further divided into “repeat claimants” and“first claimants,” as above.
The “acute injury” group was defined as having a 1991 Nature of Injurycode, in the short-term disability file, of 100 (amputation or enucleation), 160(contusion, crushing, or bruising), 170 (cut, laceration, or puncture—openwound), or 210 (fracture). The “chronic” group were those whose 1991 ICDcode was 724, 846, or 847—codes for back conditions. In both cases, it is onlythe 1991 injury that was used to make this determination; that is, the “acute in-
FIGURE 7. Percent of “acute” injury group and a cohort matched for age and gender, who visita general practitioner at least once, by year, 1986–1995. WCB 5 Workers’ CompensationBoard.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 591
jury” group may include people who have made “chronic” claims in otheryears, and vice versa.
Figures 7 and 8 show the proportion of 1991 injury and matched cohortswho visit GPs by year. The patterns on these graphs are very similar to eachother (and again, the patterns for specialists were similar), and to the patternsseen previously for the full cohorts. This strongly suggests that there is a com-ponent of increased health services utilization among injured workers that isnot directly related to the type of injury reported. Moreover, this effect per-sists after taking into account continuous enrollment in the BC medical plan.The most promising approach here is to consider the developmental factorsthat lead individuals into work that is dangerous (i.e., has high injury rates)and consider how these selection factors may also select for poorer health sta-tus in other domains of health.
Workers’ Compensation Board Medical Aid Costs
Table 1 shows total number, total people and total amount of medical aidpayments made by the WCB on behalf of the 1991 injury cohort, for 1991 in-jury claims only, from 1991 through 1996. These numbers include payments tophysicians, clinics/hospitals, and alternative providers.
Missing from Table 1, however, are the medical claims paid on behalf of thiscohort for WCB claims made in years other than 1991. These claims are signif-icant, and Table 2 shows total number of payments, number of people, totalamount of payments, and average payment per person for ALL claims paid byWCB for the 1991 injury cohort (including the payments in Table 1).
FIGURE 8. Percent of the “chronic” injury group and a cohort matched for age and gender whovisit a general pracitioner at least once, by year, 1986–1995. WCB 5 Workers’ CompensationBoard.

592 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
TA
BL
E 1
Med
ical
Aid
Pay
men
ts f
or
1991
Co
ho
rt R
elat
ed t
o 1
991
Inju
ries
No.
of
peop
le
No.
rece
ivin
gM
D s
ervi
ces
No.
rece
ivin
got
her
serv
ices
No.
of M
Dpa
ymen
ts
Am
ount
of M
Dpa
ymen
ts($
)
No.
of o
ther
paym
ents
Am
ount
of o
ther
paym
ents
($)
MD
paym
ents
/pe
rson
MD
amou
nt/
pers
on($
)
Tot
alam
ount
/pe
rson
($)
1991
117,
147
108,
449
69,9
6334
5,28
116
,001
,788
138,
460
17,1
17,7
213.
214
7.55
282.
7219
9216
,813
14,1
2810
,042
103,
929
8,36
7,32
136
,544
7,97
9,78
77.
459
2.25
972.
2919
934,
379
3,14
22,
692
26,9
101,
670,
039
9,86
32,
754,
580
8.6
531.
521,
010.
4219
943,
032
1,78
52,
065
13,6
7979
1,84
36,
992
1,65
8,36
77.
744
3.61
808.
1219
952,
281
1,27
61,
549
9,65
090
3,19
85,
109
915,
931
7.6
707.
8479
7.51
1996
1,60
392
81,
042
6,43
665
2,04
03,
071
766,
859
6.9
702.
6388
5.15
MD
5
med
ical
.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 593
TA
BL
E 2
To
tal M
edic
al A
id P
aym
ents
fo
r 19
91 C
oh
ort
No.
of
peop
le
No.
rece
ivin
gM
D s
ervi
ces
No.
rece
ivin
got
her
serv
ices
No.
of M
Dpa
ymen
ts
Am
ount
of M
Dpa
ymen
ts($
)
No.
of o
ther
paym
ents
Am
ount
of o
ther
paym
ents
($)
MD
paym
ents
/pe
rson
MD
amou
nt/
pers
on($
)
Tot
alam
ount
/pe
rson
($)
1986
21,3
0620
,577
6,52
960
,951
2,70
6,95
614
,224
1,99
5,79
13.
013
1.55
220.
7219
8725
,160
24,1
238,
686
75,0
984,
134,
550
20,1
323,
018,
757
3.1
171.
3928
4.31
1988
30,3
4128
,371
19,8
2191
,593
4,99
9,44
240
,298
4,49
0,22
73.
217
6.22
312.
7719
8934
,719
32,7
2420
,690
104,
682
5,35
9,89
042
,346
4,60
1,62
93.
216
3.79
286.
9219
9039
,203
36,8
1124
,710
119,
075
6,14
6,50
153
,959
5,61
5,90
53.
216
6.97
300.
0419
9111
8,88
311
0,22
771
,561
362,
848
17,5
66,1
2514
6,85
318
,395
,900
3.3
159.
3630
2.50
1992
47,9
9143
,827
27,5
5727
7,32
415
,166
,749
82,5
3513
,401
,864
6.3
346.
0659
5.29
1993
36,2
4833
,763
19,0
0021
4,67
610
,272
,483
59,1
0410
,417
,808
6.4
304.
2557
0.80
1994
33,0
6630
,707
16,9
3120
2,23
88,
326,
450
55,2
9711
,826
,064
6.6
271.
1660
9.46
1995
33,3
0731
,192
14,9
9620
4,58
810
,581
,183
41,5
649,
127,
286
6.6
339.
2359
1.72
1996
30,4
6228
,903
13,2
2019
6,74
89,
947,
388
37,7
028,
120,
001
6.8
344.
1659
3.11
MD
5
med
ical
.

594 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
Total Cost of Physician Services
Figure 9 displays physician payments made by MSP and by WCB for the1991 injury cohort, and MSP payments for the matched cohort. In all years,MSP payments are higher for the injury cohort than for the matched cohort.This difference is increased if payments to physicians by the WCB are in-cluded, and further increased if other medical aid payments are included. Thedollars are not adjusted, so small increases over time for both groups were ex-pected, but the difference between the two groups was not.
Hospital Use
The 1991 injury cohort is approximately twice as likely to have a hospitalseparation compared to the matched cohort. As for physician services, this istrue even
before
the index injury year of 1991, though the difference does in-crease in 1991. The proportionate difference between the two groups is largerfor day surgery than it is for inpatient hospital care. The use of day surgery in-creases for both the WCB and non-WCB groups between 1986 and 1995,which is consistent with overall trends in hospital use.
Many of the people in the WCB 1991 injury cohort are known to have madeclaims in years prior to 1991, which might explain part of the difference in theuse of hospital services between these groups. Figure 10 eliminates this by re-stricting the WCB group to those who make their first claim in 1991. The ex-clusion of pre-1991 claimants slightly reduces the difference in use, but theWCB group remains far more likely to be admitted to hospital for either daysurgery or inpatient care—both before and after the 1991 injury claim.
FIGURE 9. Total expenditures on physician services for the 1991 Workers’ Compensation Board(WCB) injury cohort and a matched sample.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 595
Income Assistance
The linked welfare file included 1,226,466 individuals who were over theage of 18 in 1997. Of these, approximately 25% also made a WCB claim atsome point between 1986 and 1996. Among the 163,338 individuals in the 1991injury cohort, 54,552, or 33%, applied for welfare sometime between 1990 and1998.
Table 3 disaggregates the WCB 1991 injury cohort by “type” of claimant(medical care only, short-term disability, long-term disability/pension, andother) and “application status” for welfare benefits. Because of the years ofdata available, the information on this table relates to payments made eitherjust before or in the years after the 1991 injury. Approximately 30% of the1991 injury cohort who make application for welfare are not granted benefits.Though the differences are relatively small, individuals in the short-term dis-ability group are least likely to apply for welfare (62.9% of the total), but aremost likely to receive benefits (26.5% of the total group, or 71% of the appli-cants). This group of welfare recipients accumulated almost $600 million ofpayments between October 1990 and the end of 1997.
Table 4 restricts the injury cohort to “first claimants.” This restriction hadvery little effect on the distribution of individuals in these tables.
Famly Composition of Welfare Applicants
We were able to identify family composition only for applicants who re-ceived benefits, as family status is recorded on the welfare data only in relation
FIGURE 10. Percentage of 1991 first claimants and matched non-Workers’ Compensation Board(WCB) cohort who use hospital services (inpatient or day surgery) in British Columbia, 1986–1995.

596 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
TA
BL
E 3
Ind
ivid
ual
s in
th
e W
ork
ers’
Co
mp
ensa
tio
n B
oar
d 1
991
Inju
ry C
oh
ort
Wh
o A
pp
ly f
or
Inco
me
Ass
ista
nce
(IA
) B
enef
its
Bet
wee
n O
cto
ber
199
0 an
d F
ebru
ary
1997
No
appl
icat
ion
to IA
App
licat
ion
to IA
—no
bene
fits
App
licat
ion
to IA
—be
nefit
sre
ceiv
ed
Tot
alR
ow %
Col
. %R
ow %
Col
. %R
ow %
Col
. %
Med
ical
car
e on
ly41
,075
69.1
37.8
5,56
19.
434
.712
,777
21.5
33.2
59,4
13S
hort
-ter
m d
isab
ility
42,8
7662
.939
.47,
265
10.7
45.3
18,0
5826
.546
.968
,199
Long
-ter
m d
isab
ility
/pen
sion
2,84
170
.52.
635
88.
92.
283
320
.72.
24,
032
Oth
er21
,994
69.4
20.2
2,85
29.
017
.86,
848
21.6
17.8
31,6
94T
otal
108,
786
16,0
3638
,516
163,
338

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 597
TA
BL
E 4
Ind
ivid
ual
s w
ith
Fir
st R
epo
rted
Wo
rker
s’ C
om
pen
sati
on
Bo
ard
Inju
ry in
199
1 W
ho
Ap
ply
fo
r In
com
e A
ssis
tan
ce (
IA)
Ben
efit
sB
etw
een
Oct
ob
er 1
990
and
Feb
ruar
y 19
97
No
appl
icat
ion
to IA
App
licat
ion
to IA
—no
bene
fits
App
licat
ion
to IA
—be
nefit
sre
ceiv
ed
Tot
alR
ow %
Col
. %R
ow %
Col
. %R
ow %
Col
. %
Med
ical
car
e on
ly17
,568
67.9
38.7
2,36
29.
136
.45,
931
22.9
34.7
25,8
61S
hort
-ter
m d
isab
ility
15,3
9760
.933
.92,
594
10.3
40.0
7,27
728
.842
.625
,268
Long
-ter
m d
isab
ility
/pen
sion
1,18
373
.32.
612
57.
71.
930
719
.01.
81,
615
Oth
er11
,219
69.3
24.7
1,40
18.
721
.63,
560
22.0
20.8
16,1
80T
otal
45,3
676,
482
17,0
7568
,924

598 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
to payments made. The number of children was not calculated, but was re-corded only as a “yes” or “no.”
The sex displayed on Table 5 reflects the gender of the WCB applicant. Forboth groups—all applicants, and those who were first claimants in 1991—sin-gle males accounted for more than 40% of the total. Single females are slightlymore predominant in the first claimant group compared to the overall group(12.4% vs. 8.9%, respectively) and married people (male or female) with kidsare slightly less predominant (23.5% vs. 26.5%).
Family Composition of the “Matched” Cohort that Receive Income Assistance Benefits
Just under 10% of the matched cohort receive welfare benefits in the period1991 to 1997, compared to 23% of the 1991 injury cohort (Table 3). The familycomposition of this group of beneficiaries is outlined in Table 6. When com-pared to Table 5, this suggests the matched welfare recipients are far morelikely to be single without kids, and far less likely to be married with kids, thanis the injury cohort. Since the principal group of welfare recipients in BC is sin-
TABLE 5Income Assistance Recipients (1991–1997) Among the 1991 Injury Cohort by Gender, Marital
Status, and Presence of Children
Single Married
No kids Kids No kids Kids
Male 15,769 1,949 2,853 8,191Female 3,271 2,463 803 1,566Total 19,040 4,412 3,656 9,757Male 42.8% 5.3% 7.7% 22.2%Female 8.9% 6.7% 2.2% 4.2%Total 51.6% 12.0% 9.9% 26.5%
TABLE 6Income Assistance Recipients (1991 and After) Among the Matched Cohort, by Gender, Marital
Status, and Presence of Children
Single Married
No kids Kids No kids Kids
Male 11,179 68 1,199 1Female 2,755 32 917 0Total 13,934 100 2,116 1Male 69.2% 0.4% 7.4% 0.0%Female 17.1% 0.2% 5.7% 0.0%Total 86.3% 0.6% 13.1% 0.0%

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 599
gle women with children, the injured workers appear to form a second distinctclient group, which has not been recognized in public policy until now.
Discussion
The preceding analyses utilized linked data to develop a better understand-ing of the experience of individuals who make injury claims to the WCB inBC. It was not an exhaustive exploration, but rather represented an initial at-tempt to test the abilities of these data to answer questions of policy interest,and to identify questions that merited further investigation. With respect tothe latter, this work did identify some patterns that should be of interest to in-vestigators in the future. The patterns of greatest interest are summarized asfollows.
More than 30% of all injuries in the injured workers file occurred within thefirst 5 months of first employment in a given job; and 50% occurred within thefirst 18 months. These findings suggest that serious consideration should begiven to directing preventive programs at those entering the labor force; mak-ing workplaces safer for new employees; focusing on the hazards of entry-leveljobs; and addressing the psychosocial factors in transition to work that maypredispose individuals to injury.
A large proportion of WCB claims are made by “frequent” WCB claimants.In other words, the repeat claimants seem to change jobs frequently, and arecaught in a “revolving door” of employment, injury, re-employment in a newjob, and re-injury.
Injured workers form a subset of the population who are high users of non-WCB-funded health care services. It was expected that use of non-WCB ser-vices would be similar to a population similar in age and gender did not reportinjuries to the WCB. Yet this was not the case. Between 1986 and 1995, mem-bers of the 1991 injured workers’ cohort visited General Practitioners and Spe-cialists at least 50% more frequently than the matched group. The proportionof the injury cohort that visit physicians increased up to the injury year (1991),peaked during 1991, and then decreased somewhat, though not to former lev-els. In comparison, there was a slow but steady (age-related) increase in theproportion of the matched cohort who visited GPs during these years, thoughthe number remained lower throughout.
The pattern for hospital use was similar to the one seen for use of physicianservices. The injury cohort was approximately twice as likely to have an inpa-tient hospital visit or day surgery encounter, compared to the matched group.Once again, this is true even
before
the index injury year of 1991, though thedifference did increase in 1991 and peaked in 1992.
What is the reason for this pattern? To some extent, the increases in healthservices utilization during and after the injury year may be work-related, eventhough they were not funded by the WCB. However, this is not the predomi-nant explanation for the pattern over the whole period, before, during, and af-ter injury. Further analyses showed that the pattern could not be explained asa long-term effect of injuries that occurred in 1986 or later; nor was it basedupon increased medical visits for chronic health problems which turned intoclaims later on.

600 C. HERTZMAN, K. MCGRAIL, and B. HIRTLE
Our conclusion is that WCB claimants are already predisposed to be highusers of health care services even before they become engaged in the WCBsystem. In order to understand this further, it will be necessary to learn moreabout the experiences of injured workers during their entire work history (i.e.,prior to 1986, and perhaps in other jurisdictions) as well as their experiencesbefore they enter the labor force.
Injury rates vary tremendously by industry. Thus, a white- collar worker,even one making the minimum wage, will not be at risk of amputation or frac-ture at work. The crucial question is: what are the common factors that lead in-dividuals (and social groups) into relatively dangerous work, which
also
serveas risk factors for other forms of ill health? Here, we have a rich literature onthe latent and pathway effects of child development and educational attain-ment which lead to lower health status in adulthood (Hertzman, 1998; Power& Hertzman, 1997). From this literature, our leading hypothesis would be thatrelative socioeconomic disadvantages at birth leading to low educational at-tainment will in turn increase the chances of employment in dangerous workbecause of decreased employment options. This hypothesis can be evaluatedwith linked and longitudinal data.
Injured workers are a distinct group of high consumers of welfare. Twenty-three percent of the WCB 1991 injury cohort received welfare benefits in theperiod 1991 to 1997, compared to less than 10% of the age- and gender-matched comparison group. Among the WCB applicants, those applying forshort-term disability benefits were more likely to apply for and receive welfarethan those applying for long-term disability/pension benefits or medical carebenefits only. In addition, welfare recipients who are not WCB applicants arefar more likely to be single without kids, and far less likely to be married withkids, than are the WCB applicants of the same age and gender. Thus, WCBapplicants seem to be at increased risk of becoming welfare recipients, follow-ing injury, compared to other British Columbians. This implies that WCB ap-plicants represent a population group that suffers higher than expected levelsof unemployment.
Unemployment is understood to have a deleterious effect on health status(Bartley, 1994; Martikainen & Valkonen 1996; Montgomery, Bartley, Cook, &Wadsworth 1996), although the exact pathway of the effect is not understood.Some theories include the financial stress of unemployment, the social andpsychological isolation, and a tendency toward self-destructive behaviors. Pe-riods of unemployment resulting from workplace injury carry all of these con-sequences, as well as the injury itself. Not all workplace injuries result in losttime on the job, but a sizable proportion do, and these are the most costly,both to the workers’ compensation system and the worker.
Longitudinal studies also suggest that there may be developmental factors,specifically early life and early labor force experiences, that may increase theprobability of prolonged unemployment (Montgomery et al., 1996). This mayalso be true of patterns of workplace injury. If true, it would offer additionalsupport for including workers’ compensation systems in our conception of thesocial safety net. Furthermore, a better understanding of the precursors ofworkplace injury has the potential to improve prevention strategies both in de-sign and population targeting.

HEALTH CARE AND SOCIAL WELFARE USE IN THE BC COHORT 601
Two conclusions follow from this. First, it would be worthwhile to measurethe welfare experience of an injury cohort prior to injury in a manner parallelto physician and hospital services utilization. Second, and most important,these data show that the WCB is part of the social safety net, regardless of thebeliefs of the principal stakeholders in Workers’ Compensation.
Conclusion
This research project points to a clear conclusion that workplace injuries shouldnot be considered as isolated events. Longevity on the job, age, SES, and previousinjury all appear to be related to subsequent accidents. Understanding life-coursetrajectories prior to initial workplace injury ought to be considered of primeimportance. This may include early childhood experiences in schools, commu-nities and at home, as well as prelabor and early labor market experiences.
Given this direction, it also makes sense to think of workers’ compensationsystems as part of the general social safety net. We should be concerned abouthow quickly the adjudication process takes place and what compensation isavailable while that process is occurring. We should also be concerned withthe interface between workers’ compensation and other payment systems,such as employment insurance and welfare, and where disability (temporaryor permanent) has occurred, the health care system as well. From a public ac-countability standpoint, it is important to know whether one system is off-loading “clients” onto another, thereby cost-shifting instead of dealing with is-sues of prevention. Finally, from a societal perspective, we ought to be con-cerned with the seamlessness of the system, and strive to prevent individualsfrom falling through the cracks.
References
Bartley, M. (1994). Unemployment and ill health: Understanding the relationship.
Journal of Epidemiologyand Community Health, 48
, 333–337.Chamberlayne, B., Green, B., Barer, M. L., Hertzman, C., Lawrence, W. J., & Sheps, S. B. (1998). Creating
a population-based linked health database: A new resource for health services research.
Canadian Jour-nal of Public Health, 89
, 270–273.Checkoway, H., Pearce, N. E., & Crawford-Brown, D. J. (1989).
Research methods in occupational epidemi-ology.
New York: Oxford University Press.Hertzman, C. (1998). The case for child development as a determinant of health.
Canadian Journal of Pub-lic Health, 89
(Suppl. 1), S14–S19.Hertzman, C., McGrail, K. M., & Hirtle, B. (1998).
Summary report of the incidence and prevalence ofworker injury and subsequent outcome in British Columbia: A record linkage study.
Report to the RoyalCommission on Workers’ Compensation in British Columbia, September 1998.
Martikainen, P. T., & Valkonen, T. (1996). Excess mortality of unemployed men and women during aperiod of rapidly increasing unemployment.
The Lancet, 348
, 909–912.Montgomery, S. M., Bartley, M. J., Cook, D. G., & Wadsworth, M. E. J. (1996). Health and social precursors
of unemployment in young men in Great Britain.
Journal of Epidemiology and Community Health, 50
,415–422.
Ng, E., Wilkins, R., Pole, J., & Adams, O. B. (1997). How far to the nearest physician?
Health Reports, 8
(4),19–31.
Power, C., & Hertzman, C. (1997). Social and biological pathways linking early life and adult disease.
BritishMedical Bulletin, 53
, 210–221.