Embed Size (px)
Citation preview

Arch Gynecol Obstet (2012) 285:1759–1761
DOI 10.1007/s00404-011-2167-4LETTER TO THE EDITOR
Ovarian hyperstimulation syndrome in a patient with frozen–thawed embryo transfer and dichorionic diamniotic pregnancy
Funda Gungor Ugurlucan · Ahmet Cem Iyibozkurt · Bulent Baysal
Received: 7 August 2011 / Accepted: 28 November 2011 / Published online: 28 December 2011© Springer-Verlag 2011
Dear Sir,
Ideal treatment outcome in assisted reproduction is optimumovarian stimulation with minimal rate of severe ovarianhyperstimulation syndrome (OHSS) or multiple pregnan-cies. However, there is still no precise method to com-pletely prevent severe OHSS, except by withholding theovulation-inducing trigger of human chorionic gonadotro-pin (hCG) [1].
Individualization of treatment according to the speciWcrisk factor and the speciWc response in the current cyclewith the option of freezing all embryos, or transfer of only asingle embryo, has the potential of reducing the risk and theseverity of the syndrome in susceptible cases [2]. But, stillin some situations, these strategies do not prevent ovarianhyperstimulation.
We report a case in which cryopreserved and thawedembryo transfer in a spontaneous cycle led to ovarianhyperstimulation. Five weeks after the embryo transfer, thepatient was admitted to the hospital with marked enlarge-ment of the ovaries, ascites, and dyspnea. The diagnosiswas OHSS and she was treated accordingly.
A 32-year-old nulligravida nulliparous woman with ahistory of primary infertility for 12 years was admitted forassisted reproduction. She had oligomenorrhea with occa-sional ovulatory cycles and features of hyperandrogenism,and polycystic ovaries on the transvaginal ultrasound scanand was diagnosed with polycystic ovary syndrome,
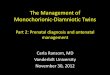
according to 2003 Rotterdam consensus criteria [3]. Herheight was 167 cm, weight 64 kg, and body mass index(BMI) 23 kg/m2. She had no other illnesses or operations.She had a history of three ovulation induction cycles withclomiphene citrate and intrauterine inseminations. Ovula-tion induction for assisted reproduction was performedusing long protocol. Leuprolide acetate 1 mg was started onday 21 of the previous cycle and reduced to 0.5 mg on day3 of the next cycle and ovulation induction was begun onday 3 with 150 IU recombinant FSH. The FSH and estra-diol (E2) levels on day 3 were 6.7 mIU/ml and 16 pg/ml,respectively, and the duration of stimulation was 10 days.hCG was used for ovulation triggering; 30 follicles wereaspirated and 27 oocytes were retrieved. Embryo transferwas performed on day 3 of oocyte retrieval. Three 8-cellembryos were transferred and 16 embryos were cryopre-served, but the �-hCG on day 12 was negative. No ovarianhyperstimulation symptoms developed. Following this, twocycles of cryopreserved–thawed embryo transfer withoutovulation induction was conducted 6 and 11 months afterthe Wrst negative result. Three cryopreserved embryos werethawed and transferred in each trial. In both of these cycles,transdermal 17-� estradiol and micronized progesteronewere given for endometrial preparation; transdermal 17-�estradiol was started on day 1 of the cycle, micronized pro-gesterone was added on day 14, and embryo transfer wasperformed on day 17. The appearance of the ovaries at thetime of embryo transfer is documented in Fig. 1. The FSHand E2 levels on day 3 were 7.8 mIU/ml and 34 pg/ml; theFSH, LH, and E2 levels on day 14 were 8.0 mIU/ml,7.1 mIU/ml, and 32 pg/ml, respectively. Micronized pro-gesterone was continued for luteal phase support. The lastcycle was successful, �-hCG was positive on day 12 and adichorionic diamniotic pregnancy was diagnosed at thetransvaginal ultrasound scan 21 days after the embryo
F. Gungor Ugurlucan (&) · A. C. Iyibozkurt · B. BaysalDepartment of Obstetrics and Gynecology, Istanbul Faculty of Medicine, Istanbul University, Atakoy 9-10. Kisim, B 7 Blok, Daire: 48, Atakoy/Bakirkoy, 34156 Istanbul, Turkeye-mail: [email protected]
123
1760 Arch Gynecol Obstet (2012) 285:1759–1761
transfer. Five weeks after the embryo transfer, the patientwas admitted to the hospital with marked enlargement ofthe ovaries, ascites, and dyspnea, and the diagnosis ofOHSS was made. Her hematocrit was 47%, leukocyte40,000/ml, and platelets 400,000/ml. Biochemical valueswere normal except for potassium which was 5.5. Thepatient was hospitalized and supportive treatment wasgiven. By 4 weeks, all the symptoms regressed and labora-tory values normalized. The pregnancy continued withoutany complications.
Ovarian hyperstimulation syndrome is an iatrogenic con-dition resulting from an excess response to ovulation induc-tion. The main features of this syndrome are markedenlargement of the ovaries and acute third space Xuidextravasation due to increased capillary permeability, suchas ascites, pulmonary edema, and peripheral edema [4].
Factors inXuencing the incidence of OHSS includeyounger age, lean BMI, polycystic ovary disease, hypogo-nadotropic hypogonadism, human menopausal gonadotro-pin or puriWed FSH, use of GnRH agonists, gonadotropindosage, and use of hCG to trigger ovulation [5]. Thesyndrome has two forms with probably two diVerent path-ophysiologies. Early onset form presents 3–7 days afterhCG administration, whereas the late onset form presents12–17 days after hCG administration. Early onset OHSScan be predicted by the preovulatory ovarian response toovulation induction. For the prevention of early onsetOHSS, controlled ovarian stimulation with GnRH antago-nists with GnRH agonist to trigger ovulation is performed.If more than 20 oocytes or 10 embryos are obtained, thenthe patient should be followed for 5 days for the signs ofearly OHSS, such as ascites in ultrasonography or
Fig. 1 Transvaginal ultraso-nography of the ovaries at the time of frozen–thawed embryo transfer. Upper left ovary, lower right ovary
123

Arch Gynecol Obstet (2012) 285:1759–1761 1761
hemoconcentration. If signs develop, it is recommended tocryopreserve all the embryos and postpone the embryotransfer [6]. In our case, despite stimulation with low-doserecombinant FSH, 27 oocytes were retrieved, but symp-toms of OHSS did not develop.
In contrast to the early onset form, the late onset OHSSis not strongly related to the pre-ovulatory ovarianresponse; therefore, measures for the prevention of lateonset OHSS are usually unsuccessful [5]. Our particularcase had oligomenorrhea with occasional ovulatory oranovulatory cycles. Hence, one can speculate that ovulationprior to thawed embryo transfer may be the reason for theseen OHSS. However, we did not observe any folliculardevelopment during ultrasonography scans in the cryopre-served embryo cycle.
The eVectiveness of embryo cryopreservation for theelimination of OHSS was evaluated in a Cochrane review,but according to this there was insuYcient evidence to sup-port routine cryopreservation [7]. There is a lack of ran-domized controlled trials on this subject.
In the literature, the late form was observed only incycles with multiple gestations, with a trend toward anincrease in the severity of disease with an increase in thenumber of gestational sacs [6, 8]. And it was suggestedthat, when there is serious risk of severe OHSS, cryopreser-vation of all embryos may prevent the development of lateonset OHSS, but not early onset OHSS, which is related tothe trigger hCG dose [8, 9]. If early OHSS does notdevelop, the transfer of one blastocyst will reduce thechance of multiple pregnancy and thereby eliminate the riskof late onset OHSS.
Although cryopreservation has been advocated as a suc-cessful way to prevent severe OHSS, our patient developedsevere OHSS after thawed embryo transfer. Multiple preg-nancy may be the main reason for the development of this
syndrome in our patient. Probably single thawed embryotransfer could decrease the probability of development ofsevere OHSS in patients at risk.
ConXict of interest None declared.
References
1. The Practice Committee of the American Society for ReproductiveMedicine (2008) Ovarian hyperstimulation syndrome. Fertil Steril90:B188–B193
2. Orvieto R (2005) Can we eliminate severe ovarian hyperstimulationsyndrome? Hum Reprod 20(2):320–322
3. The Rotterdam ESHRE/ASRM-Sponsored PCOS consensus work-shop group (2004) Revised 2003 consensus on diagnostic criteriaand long-term health risks related to polycystic ovary syndrome(PCOS). Hum Reprod 19:41–47
4. Navot D, Bergh PA, Laufer N (1996) The ovarian hyperstimulationsyndrome. In: Adashi E, Rock JA, Rosenwaks Z (eds) Reproductiveendocrinology, surgery, and technology. Lippincott–Raven Pub-lishers, Philadelphia, pp 2215–2232
5. Mathur RS, Akande AV, Keay SD et al (1997) Late onset OHSSafter ovarian stimulation is poorly predicted by peak oestradiol con-centration and number of oocytes collected. Hum Reprod 12(AbstrBook 1):R-229
6. Lyons CA, Wheeler CA, Frishman GN, Hackett RJ, Seifer DB,Hanning RVJ (1994) Early and late presentation of the ovarianhyperstimulation syndrome: two distinct entities with diVerent riskfactors. Hum Reprod 9:792–799
7. Angelo AD, Amso NN (2002) Embryo freezing for preventingovarian hyperstimulation syndrome: a Cochrane review. HumReprod 17(11):2787–2794
8. Mathur RS, Joels LA, Jenkins JM, Hunt LP, Jenkins JM (1995)Ovarian hyperstimulation syndrome may be more likely if multiplepregnancy follows assisted conception. Acta Genet Med Gemellol44:233–235
9. Queenan JT, Veeck LL, Toner JP, Oehninger S, Muasher SJ (1997)Cryopreservation of all prezygotes in patients at risk of severehyperstimulation does not eliminate the syndrome, but the chancesof pregnancy are excellent with subsequent frozen-thaw transfers.Hum Reprod 12:1573–1576
123


![A monochorionic diamniotic twin pregnancy with selective ... · fetoscopy, a sequential Laser placental ablation was performed, identifying 6 anastomoses (5 arteriovenous [AV] and](https://img.pdfslide.us/doc/110x75/5f2d79ce00b49e3aa72f885c/a-monochorionic-diamniotic-twin-pregnancy-with-selective-fetoscopy-a-sequential.jpg)