Embed Size (px)
Citation preview

Canadian Association of Radiologists Journal xx (2014) 1e8www.carjonline.org
Computed Tomography / Tomodensitom�etrie
Outside the Inside: A Review of Soft-Tissue Abnormalities Seenon Thoracoabdominal Computed Tomography
Susan J. Frank, MD, Shari Friedman, MD, Milana Flusberg, MD, Ellen L. Wolf, MD,Marjorie W. Stein, MD*
Department of Radiology, Montefiore Medical Center, Bronx, New York, USA
Abstract
In this review, we illustrate the computed tomographic features of thoracoabdominal soft-tissue abnormalities, which may be easilyoverlooked and often can provide important information regarding systemic processes. Examples include necrotizing fasciitis, heterotopicossification, fat necrosis, benign and malignant neoplasms, endometriosis, and collagen vascular disease as well as systemic and congenitalpathology.
R�esum�e
Cette revue permet d’illustrer les caract�eristiques tomodensitom�etriques des anomalies des tissus mous, lesquelles peuvent facilementpasser inapercues et souvent s’av�erer une source de renseignements importants sur les processus syst�emiques. Elle porte notamment sur lafasciite n�ecrosante, l’ossification h�et�erotopique, la st�eaton�ecrose, les tumeurs b�enignes et malignes, l’endom�etriose, la collag�enose avecmanifestations vasculaires et les affections syst�emiques et cong�enitales.� 2014 Canadian Association of Radiologists. All rights reserved.
Computed tomography (CT) is routinely ordered for theevaluation of thoracic, abdominal, and pelvic pathology.Soft-tissue abnormalities, often incidental, are frequent andeasily overlooked. It is important that the radiologist befamiliar with the appearance and differential diagnosis ofsoft-tissue abnormalities on CT. This pictorial essay willreview the CT features of common and uncommon soft-tissue infections; postoperative complications; benign andmalignant neoplasms; endometriosis; and vascular, congen-ital, and systemic conditions.
Infections
Abdominal-wall infections include cellulitis, necrotizingfasciitis, and abscesses. Infections may be primary, post-operative, or posttraumatic, or associatedwith foreign bodies, ordue to extension of intra-abdominal infection. CT findings incellulitis include subcutaneous fat stranding and skin and fascial
* Address for correspondence: Marjorie W. Stein, MD, Department of
Radiology, Montefiore Medical Center, 111 East 210th Street, Bronx, New
York 10467, USA.
E-mail address: [email protected] (M. W. Stein).
0846-5371/$ - see front matter � 2014 Canadian Association of Radiologists. A
http://dx.doi.org/10.1016/j.carj.2013.09.005
thickening. Necrotizing fasciitis is life threatening and may bedifficult to distinguish from cellulitis, particularly in its earlystages. Subcutaneous gas is diagnostic in the appropriate clin-ical setting but is only reported in 55% of cases [1]. CT is usefulin determining the extent of involvement, particularly when theinfection involves the deep subcutaneous tissues (Figure 1) orintra-abdominal space. Fournier gangrene is a subtype of severenecrotizing fasciitis that involves the perineum, frequently seeninmale patientswith diabetes [2]. Pilonidal sinus disease resultsfrom chronic hair follicle infection with subcutaneous abscessformation and discharge through a midline draining sinus(Figure 2). Imaging is helpful to differentiate pilonidal sinusdisease,whichoriginates subcutaneously, fromperianal fistulas,which communicate with the anus or the rectum [3]. CT ishelpful in demonstrating these abscesses and fistulas.
Postoperative Appearances
There are normal and abnormal postoperative appearancesof the subcutaneous tissues. Mild skin thickening, subcu-taneous oedema, seromas, small hematomas, and gas withinthe soft tissues may be seen in the immediate postoperativeperiod. Infection in this setting is suggested when fever or
ll rights reserved.

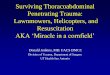
Figure 1. (A) A 67-year-old woman after a ventral hernia repair with mesh
(arrow). Axial noncontrast computed tomography (CT), demonstrating a large
fluid collection with gas in the anterior abdominal wall typical of infection.
(B) A 28-year-old man with sacral decubitus ulcer. Contrast-enhanced axial
CT, demonstrating a large amount of gas within the gluteus muscles and
subcutaneous inflammatory stranding typical for necrotizing fasciitis.
2 S. J. Frank et al. / Canadian Association of Radiologists Journal xx (2014) 1e8
leukocytosis is present. Postsurgical heterotopic ossificationis a form of myositis ossificans traumatica and occurs only insubxiphoid, midline, vertical abdominal incisions. It is morecommon in men and has been reported as early as 11 days
Figure 2. A 42-year-old man with pilonidal sinus disease. Axial noncontrast
computed tomography, demonstrating a sinus tract (arrow) that extends from
the midline, which does not communicate with the rectum.
after surgery [4,5]. It is hypothesized to be due to eitherexcessive suture line tension, metaplasia of mesenchymalembryonal cells, or intraoperative seeding of perichondrialcells [5]. CT reveals ossification within an incision, betweenthe anterior abdominal fascia and the peritoneum (Figure 3)[5]. Heterotopic ossification can contain cartilage, bone, andfatty marrow [5e7]. The ability of CT to differentiate ossi-fication from calcification, which is due to dystrophic de-posits of calcium phosphate salts, is important because thetreatment for heterotopic ossification is often surgical. CTalso allows differentiation of heterotopic ossification fromother palpable soft-tissue masses, including a retainedforeign body, wound infection, and tumour seeding [5].
Fat Necrosis
Subcutaneous fat necrosis may be due to trauma, collagenvascular disease, myeloproliferative disease, pancreatitis,pancreatic cancer, or, rarely, exposure to cold [8,9]. Fat ne-crosis, when due to trauma, may occur long after the incitingevent. On CT, it typically appears as a well-defined subcu-taneous fat-density mass with peripheral enhancement andcalcification (Figure 4). Alternatively, it may be visualized asa globular soft-tissue density with central fat [8].
Soft-Tissue Neoplasms
Soft-tissue tumoursmay be benign ormalignant, primary ormetastatic. Although magnetic resonance imaging is the mo-dality of choice for soft-tissue tumour assessment, CT is alsohelpful in assessing matrix mineralization, bony involvement,and vascularity.
Benign Neoplasms
Lipomas are very common benign soft-tissue tumours,frequently seen incidentally, more often in women, and aremultiple in 5%. Typical locations include the back, shoulders,abdomen, and extremities. Lipomas are usually superficial but
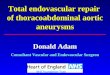
Figure 3. A 50-year-old woman after abdominal surgery. Contrast-enhanced
computed tomography, demonstrating heterotopic ossification of the midline
incision (arrow).

Figure 4. A 62-year-old woman after abdominal surgery. Contrast-enhanced
computed tomography, demonstrating foci of fat necrosis, with peripheral
enhancement and calcification in the anterior abdominal wall.
Figure 6. A 31-year-old man with periscapular fatty mass (arrow) seen on
contrast-enhanced computed tomography. The typical location and density
favors a hibernoma.
3Soft-tissue abnormalities on CT / Canadian Association of Radiologists Journal xx (2014) 1e8
may be intramuscular. On CT, lipomas measure fat density,often contain fibrous septations, and may contain calcifica-tions or induce cortical thickening in adjacent bone (Figure 5).Septations are usually thin, smooth, and nonenhancingcompared with their malignant counterparts, but imagingoverlap exists with well-differentiated liposarcomas [7,10].
A hibernoma, a variant of a lipoma, is a benign tumourcomposed of brown fat, often located in the thigh or near thescapula. On CT, it exhibits fatty, or slightly higher, attenu-ation, and may demonstrate serpentine vasculature and mildcapsular enhancement (Figure 6). Although fluorodeox-yglucose avid on positron emission tomographyeCT, it maybe distinguished from malignancy by its characteristiclocation and CT attenuation [10].
Elastofibroma is a rare benign tumour composed of fibroustissue and fat, most frequently found in elderly women. Sixtypercent are bilateral and are characteristically located in theinfrascapular region, deep to the serratus anterior and latissimusdorsi muscles. On CT, the mass is typically soft-tissue attenu-ation, with dense striations and fatty streaks (Figure 7) [11].
Neurofibromas may be plexiform, localized, or diffuse.Theymay be associatedwith neurofibromatosis whenmultiple
Figure 5. A 47-year-old man with intramuscular fatty mass (arrow) seen
incidentally on this contrast-enhanced computed tomography.
or plexiform. On CT, a neurofibroma appears as a fusiformsoft-tissue mass in close proximity to a nerve and may erodebone (Figure 8). It is typically isodense to muscle on non-contrast CT, with a variable enhancement pattern after intra-venous contrast [10].
Desmoid tumour is a deep fibromatosis, which is benignbut notorious for local recurrence. It commonly occurs be-tween 25 and 35 years of age, and may be seen with familialadenomatous polyposis. Although 70% occur in the ex-tremities, women taking oral contraceptives or who arerecently postpartum have an increased incidence of desmoidsin the rectus abdominis and internal oblique muscles. On CT,desmoids are ill defined or spiculated, iso- or hyperdense,and enhance after intravenous contrast [12].
Malignant Neoplasms
Liposarcoma is seen in middle-aged and elderly patients,typically in the thigh, gluteal region, retroperitoneum, or lowerextremity. Features of fatty lesions that increase suspicion for
Figure 7. A 78-year-old man with classically located infrascapular elastofi-
broma (arrow) seen on noncontrast computed tomography.

Figure 8. A 27-year-old man with neurofibromatosis I and multiple intra-
abdominal and subcutaneous neurofibromas seen on contrast-enhanced
computed tomography.
Figure 10. A 33-year-old man with AIDS and Kaposi sarcoma. Contrast-
enhanced computed tomography, demonstrating an avidly enhancing sub-
cutaneous lesion in the right anterior chest wall. A lung mass is also present.
4 S. J. Frank et al. / Canadian Association of Radiologists Journal xx (2014) 1e8
malignancy include large size, thick septa, nodular solidcomponents, and contrast enhancement. Poorly differentiatedliposarcomas may not have visualized fat [7,10]. Malignantfibrous histiocytoma, also referred to as pleomorphic undif-ferentiated sarcoma, occurs most often in the lower extrem-ities, especially the thigh. It appears as a heterogeneouslyenhancing soft-tissue mass frequently causing adjacent bonedestruction. The mass may occasionally contain bone, carti-lage, fibrous tissue, hemorrhage, or necrosis [10]. Granulocyticsarcoma (chloroma) predominately occurs in a subcutaneousor intramuscular location, in patients younger than 15 yearswho have acute or chronic myelogenous leukaemia or othermyeloproliferative disorders. Chloromas characteristicallyappear as slightly hypodense masses compared with muscleand with homogeneous contrast enhancement (Figure 9) [13].Kaposi sarcoma, often an AIDS-defining illness, is linked toherpes virus type 8 infection. It most commonly presentsas hyperenhancing subcutaneous nodules (Figure 10) [14].
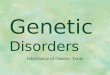
Figure 9. A 53-year-old man with chronic myelogenous leukaemia. Axial
contrast-enhanced computed tomography, demonstrating a hyperdense sub-
cutaneous chloroma (arrow), an unusual appearance because most chloromas
are hypodense to muscle.
Soft-tissue metastases are most often identified in the abdom-inal and chest wall, back, thigh, and shoulder (Figure 11). Lungcancer is the most common primary tumour to metastasize tosoft tissues followed by kidney, colon, and melanoma. Soft-tissue metastases may be the first sign of malignancy [15].
Endometriosis
Endometriosis is a common gynaecologic condition thatoccurs in 15% of menstruating women, almost exclusivelyin the pelvis. It may also form in a surgical scar aftercaesarean section, hysterotomy, hysterectomy, or laparotomy.The incidence of abdominal-wall endometriomas after acaesarean section varies from 0.03%e1% [16,17]. Endome-trial deposits have been reported in the dermal and subcu-taneous tissues, and, infrequently, in the rectus abdominismuscle and rectus sheath [18]. Scar endometriosis typicallypresents as a cyclically enlarging palpable abdominal-wall
Figure 11. A 35-year-old woman with metastatic cervical cancer. Contrast-
enhanced computed tomography, demonstrating multiple subcutaneous
metastases.

Figure 13. A 28-year-old woman with steatocystoma multiplex. Noncontrast
computed tomography, demonstrating multiple fat and fluid density subcu-
taneous nodules.
5Soft-tissue abnormalities on CT / Canadian Association of Radiologists Journal xx (2014) 1e8
mass with increased tenderness during menses. CT typicallyreveals an enhancing solid mass in the abdominal wall, oftenwith adjacent inflammatory stranding (Figure 12). Theappearance varies, depending on the phase of the menstrualcycle, relative proportion of stroma, and the amount ofhemorrhage and fibrosis. Magnetic resonance imaging maybe useful to confirm the presence of blood products [16e18].Medical management with progestational agents is oftenunsuccessful, and endometriomas may recur when hormonaltreatment is terminated. Thus, surgery is the treatment ofchoice, and CT is useful in presurgical planning [16e18].
Sebaceous Cyst
The term ‘‘sebaceous cyst’’ includes epidermal inclusioncysts that occur in relatively hairless parts of the body, andpilar cysts, which are associated with hair follicles. Sebaceouscysts contain keratin but do not contain sebum. They occurdue to blocked sebaceous glands or hair follicles, or excessivetestosterone production. Common locations include the scalp,face, neck, trunk, back, and scrotum. They exhibit variable CTattenuation, depending on their content, and are characteris-tically located in the subcutaneous tissues just beneath theskin surface. Steatocystoma multiplex is a rare autosomaldominant disorder of the pilosebaceous unit. Patients withsteatocystoma multiplex present with numerous sebum andkeratin-containing intradermal cysts, often on the chest(Figure 13) [10,19].
Eagle-Barret Syndrome
Eagle-Barret or prune belly syndrome occurs exclusivelyin male patients and is characterized by congenital absenceor hypoplasia of the abdominal-wall muscles in associationwith genitourinary abnormalities (Figure 14). Cryptorchi-dism is always present. Varying degrees of urinary tractobstruction are seen, including urinary bladder enlargement
Figure 12. A 26-year-old woman with history of caesarean section. Non-
contrast computed tomography, demonstrating a pathologically proven
endometrioma that appears as a soft-tissue nodule (arrow) in the midline
abdominal wall caesarean section scar with adjacent stranding.
[20]. Pseudo-prune-belly syndrome is the term used when thesyndrome occurs unilaterally or in female patients [21].Treatment is directed towards relief of obstruction to preventinfection and kidney damage [20]. Cross-sectional imagingcan also be useful to determine the practicality of cosmeticrepair [21].
Acquired Muscle Atrophy
Acquired muscle atrophy of the abdominal-wall muscu-lature may result from disuse or denervation. On CT,muscular atrophy is seen as fatty replacement of muscle(Figure 15). The atrophy is typically diffuse when secondaryto muscular dystrophy, cerebral palsy, or quadriplegia, and isunilateral or asymmetric when due to cerebral vascular ac-cident, poliomyelitis, trauma, or surgery [10].
Figure 14. A 4-year-old boy with Eagle-Barret syndrome. Axial noncontrast
computed tomography, demonstrating characteristic absence of the
abdominal-wall musculature and marked hydroureteronephrosis.

Figure 17. A 61-year-old woman with end-stage renal disease. Contrast-
enhanced computed tomography, demonstrating metastatic calcification in
the soft tissues of the pelvis, with multiple fluid-calcium levels (arrow).
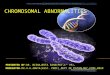
Figure 15. Muscle atrophy. (A) An 80-year-old man after a hip fracture with
unilateral gluteal muscle atrophy (arrow) due to disuse seen on noncontrast
computed tomography. (B) A 43-year-old man with muscular dystrophy with
diffuse muscle atrophy.
6 S. J. Frank et al. / Canadian Association of Radiologists Journal xx (2014) 1e8
Collagen Vascular Disease
Autoimmune connective tissue disorders such as poly-myositis and dermatomyositis can demonstrate a sheet-like
Figure 16. A 46-year-old woman with mixed connective tissue disorder.
Axial noncontrast computed tomography, demonstrating subcutaneous cal-
cifications (arrow) and honeycombing at the lung bases.
pattern of calcification in the skin, subcutaneous tissues,and fascial planes termed calcinosis universalis [7]. Calci-nosis circumscripta refers to dermal papules, plaques, andsubcutaneous nodules seen in the early stages of polymyo-sitis, dermatomyositis, lupus, and scleroderma, which maycontain calcifications [22]. Interstitial lung disease may bevisualized (Figure 16).
Renal Disease
Patients with chronic renal failure commonly developperiarticular calcium deposits. Metastatic calcification refersto the deposition of calcium in normal soft tissues secondaryto elevated serum calcium from an abnormality of calciummetabolism [7]. These deposits can be mass-like with fluid-calcium levels that render them indistinguishable fromidiopathic tumoural calcinosis (Figure 17) [22].
Vascular Pathology
Vascular lesions are typically low density, with areas ofheterogeneity secondary to vascular, fibrous, and fatty
Figure 18. A 44-year-old man with right paraspinal hemangioma (arrow).
Noncontrast computed tomography, demonstrating classic appearance with
fat, vessels, and phleboliths.

Figure 19. A 59-year-old man with end-stage renal disease. Contrast-
enhanced computed tomography, demonstrating extensive collateral ves-
sels in the abdominal wall due to multiple central venous stenoses from
longstanding indwelling hemodialysis catheters.
7Soft-tissue abnormalities on CT / Canadian Association of Radiologists Journal xx (2014) 1e8
tissue. Low-flow lesions, such as venous malformations,are visualized as soft-tissue masses with phleboliths andvessels that enhance after contrast. Arteriovenous fistulasor malformations are high-flow lesions that typicallydemonstrate large feeding arteries and draining veins. CTangiography can aid in preoperative planning by delineatingthe anatomy and venous drainage patterns [7]. Hemangiomais a common benign vascular neoplasm, frequently seen inchildren. On CT, it appears as a soft-tissue mass, oftenwith calcified phleboliths and enhancing tortuous vessels(Figure 18). Cavernous intramuscular forms may have largefatty components. Patients with portal venous hypertensionor central venous obstruction can demonstrate collateralveins in the chest and abdominal wall (Figure 19). This isoften seen in association with subcutaneous oedema, char-acterized by stranding within the subcutaneous fat, moreprominent in the dependent tissues [21].
Figure 20. An 84-year-old woman on anticoagulation. Noncontrast computed
tomography, demonstrating moderate-sized left rectus sheath hematoma with
hematocrit level.
Rectus Sheath Hematoma
Rectus sheath hematoma (RSH) often presents with suddenonset of abdominal pain and a palpable abdominal mass. RSHis more frequent in women and may occur after minimaltrauma, such as coughing, or with exercise. RSH may be dueto damaged inferior or superior epigastric arteries or tears ofthe muscle. Anticoagulation is a predisposing factor [23]. OnCT, RSH appears as a lenticular-shaped mass when above thearcuate line and as a spherical mass when below the line. Thisdifference in shape is due to the different anatomic compo-sition of the posterior rectus sheath below the arcuate line.The density varies with the age of the hematoma, which isgenerally hyperdense acutely, may develop a hematocrit level,and becomes iso- or hypodense over time (Figure 20).
Conclusions
Soft-tissue abnormalities are common and easily overlookedon routine thoracoabdominal CT. Radiologists must carefullyevaluate the soft tissues, which can reveal unsuspected abnor-malities and provide information about systemic processes.Familiarity with CT features of soft-tissue lesions, includinglocation, the relationship to adjacent structures, attenuation andenhancement patterns, can aid in establishing the correctdiagnosis and in guiding optimal patient management.
References
[1] Wysoki MG, Santora TA, Shah RM, et al. Necrotizing fasciitis: CT
characteristics. Radiology 1997;203:859e63.
[2] Rajan DK, Scharer KA. Radiology of Fournier’s gangrene. AJR Am J
Roentgenol 1998;170:163e8.
[3] Taylor S, Halligan S, Bartram C. Pilonidal sinus disease: MR imaging
distinction from fistula in ano. Radiology 2003;226:662e7.[4] Rosa M, Amir M. Myositis ossificans traumatica of the abdominal wall.
Can J Surg 2009;52:e33e4.
[5] Jacobs JE, Birnbaum BA, Siegelman ES. Heterotopic ossification of
midline abdominal incisions: CT and MR imaging findings. AJR Am J
Roentgenol 1996;166:579e84.
[6] Balboni TA, Gobezie R, Mamon HJ. Heterotopic ossification: patho-
physiology, clinical features, and the role of radiotherapy for prophy-
laxis. Int J Radiat Oncol Biol Phys 2006;65:1289e99.[7] Subhawong TY, Fishman EK, Swart JE, et al. Soft-tissue masses and
masslike conditions: what does CT add to diagnosis and management?
AJR Am J Roentgenol 2010;194:1559e67.
[8] Chan LP, Gee R, Keogh C, et al. Imaging features of fat necrosis. AJR
Am J Roentgenol 2003;181:955e9.
[9] Lee SK, Lee JH, Han CH, et al. Calcified subcutaneous fat necrosis
induced by prolonged exposure to cold weather: a case report. Pediatr
Radiol 2001;31:294e5.
[10] Resnick D, Kransdorf M. Bone and Joint Imaging. 3rd ed. Philadelphia,
PA: Elsevier Saunders; 2005. pp. 1199e243.
[11] Ochsner JE, Sewall SA, Brooks GN, et al. Elastofibroma dorsi. Ra-
dioGraphics 2006;26:1873e6.
[12] Robbin M, Murphey M, Temple HT, et al. Imaging of musculoskeletal
fibromatosis. Radiographics 2001;21:585e600.
[13] Guermazi A, Feger C, Rousselot, et al. Granulocytic sarcoma (chlor-
oma) imaging findings in adults and children. AJR Am J Roentgenol
2002;178:319e25.
[14] Restrepo C, Martinez S, Lemos J. Imaging manifestations of Kaposi’s
sarcoma. Radiographics 2006;26:1169e85.

8 S. J. Frank et al. / Canadian Association of Radiologists Journal xx (2014) 1e8
[15] Plaza J, Perez-Montiel D, Mayerson J, et al. Metastases to soft tissues.
Cancer 2008;112:193e203.
[16] Hensen JJ, Vreisman ACV, Puylaert JBCM. Abdominal wall endo-
metriosis: clinical presentation and imaging features with emphasis on
sonography. AJR Am J Roentgenol 2006;186:616e20.
[17] Dwivedi AJ, Agrawal SN, Silva YJ. Abdominal wall endometriomas.
Dig Dis Sci 2002;47:456e61.
[18] Kafkasli A, Franklin RR, Sauls D. Endometriosis in the uterine wall
cesarean section scar. Gynecol Obstet Invest 1996;42:211e3.
[19] Sonnenblick E, Buchness R, Austin J. CT demonstration of steato-
cystoma multiplex. J Comput Tomogr 1986;10:357e9.
[20] Eagle JR, Barret GS. Congenital deficiency of abdominal musculature
with associated genitourinary abnormalities: a syndrome: report of nine
cases. Pediatrics 1950;6:721e36.
[21] Donnelly L, Frush D. Cross-sectional imaging of abnormalities of the
abdominal wall in pediatric patients. AJR Am J Roentgenol 2001;176:
1233e9.
[22] Olsen K, Chew F. Tumoral calcinosis: pearls, polemics, and alternative
possibilities. Radiographics 2006;26:871e85.[23] Berna JD, Garcia-Medina V, Guirao J, et al. Rectus sheath he-
matoma: diagnostic classification by CT. Abdom Imaging 1996;
21:62e4.