Embed Size (px)
Citation preview
Kidney International, Vol. 59 (2001), pp. 718–724
Outpatient vancomycin use and vancomycin-resistantenterococcal colonization in maintenance dialysis patients
MOHAMED G. ATTA,1 JOSEPH A. EUSTACE,1 XIAOYAN SONG, TRISH M. PERL,and PAUL J. SCHEEL, JR.
Divisions of Nephrology and Infectious Diseases, Johns Hopkins University School of Medicine and School of Hygiene andPublic Health and the Johns Hopkins Hospital, Baltimore, Maryland, USA
Outpatient vancomycin use and vancomycin-resistant entero- Many nephrologists frequently use vancomycin for thecoccal colonization in maintenance dialysis patients. empiric treatment of dialysis-associated infections [1–3],
Background. Although outpatient vancomycin is widely used despite recommendations to the contrary [4, 5]. Vanco-as empiric therapy for dialysis-associated infections, its rela-mycin has the advantage of being highly effective againsttionship with vancomycin-resistant enterococcal (VRE) coloni-gram-positive organisms, including those resistant tozation is not established.
Methods. During a two-year prospective cohort study, rec- methicillin, and of having an extended duration of actiontal swabs obtained from patients at the start and finish of the in end-stage renal disease. Unfortunately, its increasedstudy period and during interim hospitalizations were cultured use has been associated with a dramatic increase in hospi-for VRE.
tal-acquired infections with vancomycin-resistant enter-Results. Ten of 124 patients initially grew VRE. Twenty-fourococci (VRE). This resistance is usually genetically medi-of the remaining patients had no follow-up cultures because of
patient death (62%), transfer to another dialysis facility (17%), ated and is potentially transferable between bacterialpatient’s refusal (7%), and transplantation (4%), and were species [6–8]. Moreover, the danger exists that resistancethus excluded. The remaining patients (N 5 90) had a median
may develop in more virulent organisms such as Staphy-age of 54.3 years and were 92% African American and 50%lococcus aureus, as has been described in several casemale. Fifty-eight percent were treated by hemodialysis. They
received 403 g of intravenous vancomycin over 157.2 patient- reports [9–14]. Much of the existing literature regardingyears of follow-up, 73% as outpatients. Sixteen of 90 patients VRE infection relates to in-hospital practice and thus may(17.8%) became colonized with VRE, an incidence rate of one not apply to the outpatient dialysis setting. In addition,case per 9.8 patient-years of follow-up. None of the 29 patients
several studies have failed to demonstrate an increase inwho did not receive vancomycin developed VRE comparedthe prevalence of VRE among dialysis patients, despitewith 26% of those treated with vancomycin (P 5 0.001). The
odds ratio (95% CI) for the association of outpatient vancomy- the widespread use of vancomycin [3, 15–18]. We con-cin (g per year) with VRE colonization was 1.23 (1.05, 1.44, P 5 ducted the following study to define the incidence of0.008). The association remained significant following adjust- VRE colonization in the dialysis population and to exam-ment in separate logistic regression analyses for relevant demo-
ine specifically the association between outpatient van-graphic, clinical, antimicrobial (inpatient vancomycin, oral orcomycin use and the development of VRE colonization.intravenous cephalosprins, aminoglycosides, quinalones, or anti-
anaerobics), and hospitalization exposures. The unadjusted rel-ative risk of death in patients growing VRE was significantly
METHODShigher than in those not colonized with VRE (P 5 0.005).Conclusions. VRE colonization is a relatively common and Study design
underrecognized problem among chronic dialysis patients. ItIn December of 1996, we conducted a cross-sectionalis strongly and independently associated with the outpatient use
of vancomycin, which should be avoided whenever possible. prevalence study of VRE colonization in our outpatientdialysis center, a freestanding unit located in East Balti-more (MD, USA). Using a standardized protocol, peri-
1 Drs. Atta and Eustace contributed equally to this study. rectal swabs (culturette; Becton Dickinson Microbiologysystem, Cockeysville, MD, USA) were obtained from allKey words: end-stage renal disease, infection, chronic dialysis, dialysis-
related infection, gram-positive organisms, bacteria. consenting patients and were cultured for VRE. Patientswhose initial cultures did not grow VRE were enteredReceived for publication May 5, 2000into a cohort study and followed for up to a maximumand in revised form August 31, 2000
Accepted for publication September 5, 2000 of 25 months. During follow-up, patients hospitalizedat the Johns Hopkins Hospital were also intermittently 2001 by the International Society of Nephrology
718

Atta et al: Outpatient vancomycin and VRE colonization 719
cultured for VRE colonization, as part of routine hospital time of study entry (December 1996) until the time oftheir first positive VRE rectal culture or until the lastpractice. Standard infection control measures in the dial-
ysis unit included the use of universal precautions and recorded negative culture either at the end of the studyor prior to the subject exiting the cohort. Patients exitedthe cleaning of all dialysis equipment and the dialysis
chair between uses with 2% bleach solution. No specific the cohort prior to study’s termination due to trans-plantation, transfer to another dialysis unit, or patientprocedures were in place for dialyzing patients with a
history of VRE infection or colonization. In-hospital death. Patients who had no repeat rectal culture duringthe course of the study and whose follow-up VRE statusmanagement included the use of gowns and gloves and
the isolation or cohorting of known VRE colonized or was thus unknown were, by necessity, excluded from theprimary analysis. Patients who had a positive VRE rectalinfected patients. These infection control measures were
unchanged over the period of the study. At the end of the swab obtained within 48 hours of hospitalization wereassumed to have had VRE colonization prior to hospital-study period (December 1998), we conducted a second
cross-sectional prevalence study of VRE rectal coloniza- ization and did not have this last hospitalization countedamong their exposure data. As the duration of follow-tion in all surviving cohort members.up was different for different subjects, exposure data
Outcome ascertainment were expressed in terms of a subject’s average exposureper year.Patients were defined as being colonized with VRE
only if a cultured rectal swab grew VRE without clinicalPrimary analysisinfection. Rectal swabs were cultured using an identical
technique throughout the study period. In brief, speci- In the primary analysis, the effects of vancomycin ad-ministered in the chronic dialysis unit were studied sepa-mens were plated on agar appropriate for each body site
and on selective trypticase soy agar media containing rately from that administered within the hospital. The5% sheep’s blood, 10 mg/mL vancomycin, and 8 mg/mL influence of topical antimicrobial preparations and of pro-gentamicin. Colonies consistent with enterococcus, which phylactic use of cotrimoxazole among HIV patients—onhydrolyze PYR and were gram positive, were speciated which we had incomplete data—was not examined. Ausing motility, pigment production, and 10% lactose subgroup analysis was, however, performed excludingtests. Final speciation occurred according the scheme of HIV seropositive patients.Facklam and Collins [19]. Vancomycin susceptibility was
Statistical methodstested using agar dilution technique and concentrationsof vancomycin of 1, 2, 4, 16, and 64 mg/mL. If the organ- Outlying values for the distribution of each variableism had a minimal inhibitory concentration (MIC) of were identified using boxplots, and their validity wasgreater than 16 but less than 64, the E test was used to checked against the original clinical record. The VRE-confirm according to the National Committee for Clini- positive and -negative groups were compared using thecal Laboratory Standards [20]. Mann-Whitney U test for continuous and the Fisher’s
exact test for categorical data. The association of outpa-Exposure assessment tient vancomycin use with the development of VRE was
Baseline demographic information and clinical charac- examined using unconditional logistic regression. Theteristics of the participating subjects were abstracted influence of individual potential confounders was exam-from the patients’ medical records. The dose of vancomy- ined, one at a time, in separate logistic regression analy-cin, as well as any additional antibiotics, administered ses. Because of the limited available sample size, moreor prescribed in the dialysis unit was obtained from dial- extensive regression modeling was not attempted. Pa-ysis unit records. These antibiotics were prescribed ac- tient survival was examined using the Kaplan–Meiercording to the discretion of the attending physician and method and compared using the log rank test. Patientswithout use of standing orders. In-patient antibiotic use were censored at the time of transplantation or at losswas obtained from the hospital’s pharmacy record, and to follow-up. For all analyses, a type I error rate of 0.05details regarding the in-patient hospital stay and inten- was used. Statistical analysis was performed using SPSSsive care unit admissions were obtained from the Johns software, version 7.5 (Chicago, IL, USA).Hopkins Hospital case-mix database, a database thatrecords the duration and location of patients’ stay in the
RESULTShospital. Information on orally prescribed antibiotics wasOne hundred twenty-four of the 147 patients (84.4%)checked by cross-referencing data from the hospital out-
attending our dialysis unit in December 1996 agreedpatient pharmacy. As this pharmacy delivers medicineto participate in the study. Seventy-four patients weredirectly to the dialysis unit, it is widely, although nottreated with hemodialysis and the remaining 50 withexclusively, used by our dialysis patients.
Exposure data were obtained for all patients from the peritoneal dialysis. Ten of the 124 (8%) patients were
Atta et al: Outpatient vancomycin and VRE colonization720
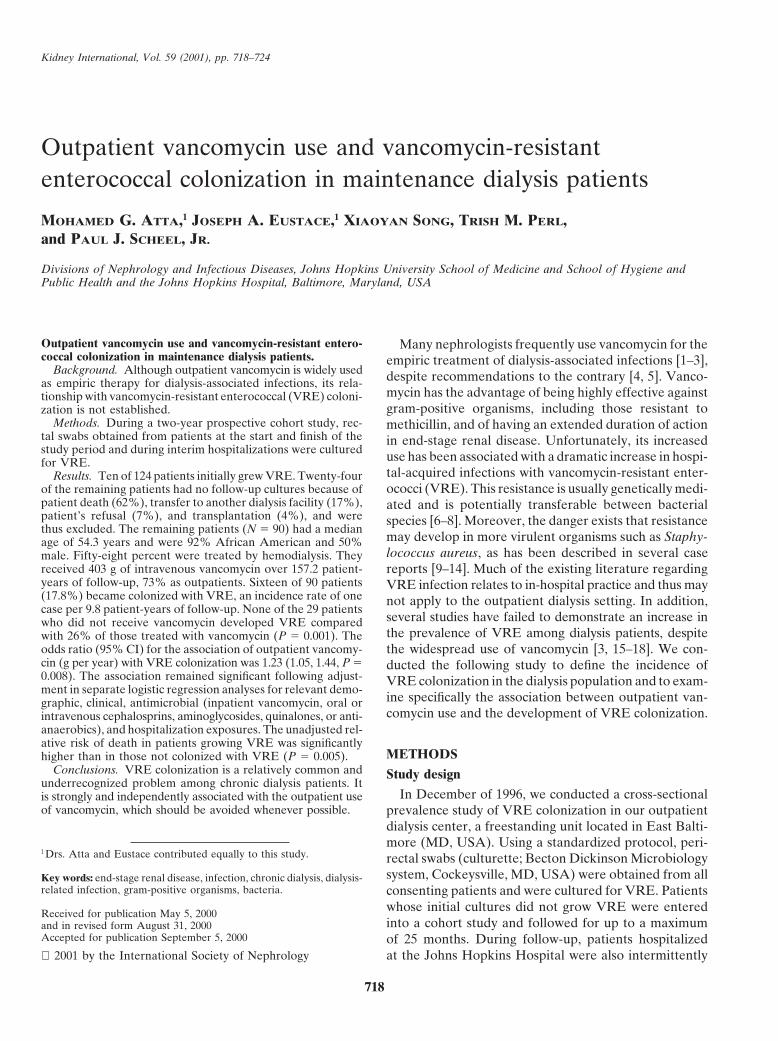
Table 1. Comparison of baseline demographics and clinical two groups’ antibiotics and hospitalization exposure arecharacteristics by follow-up vancomycin resistant enterococcal
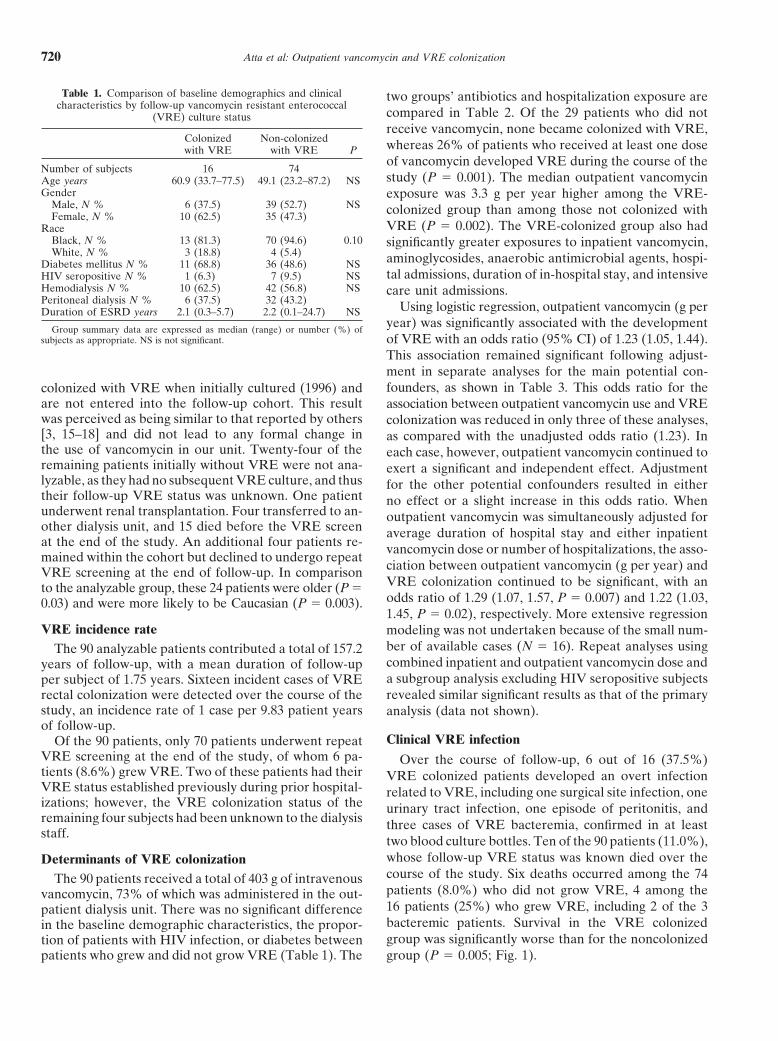
compared in Table 2. Of the 29 patients who did not(VRE) culture statusreceive vancomycin, none became colonized with VRE,
Colonized Non-colonized whereas 26% of patients who received at least one dosewith VRE with VRE Pof vancomycin developed VRE during the course of the
Number of subjects 16 74study (P 5 0.001). The median outpatient vancomycinAge years 60.9 (33.7–77.5) 49.1 (23.2–87.2) NS
Gender exposure was 3.3 g per year higher among the VRE-Male, N % 6 (37.5) 39 (52.7) NS colonized group than among those not colonized withFemale, N % 10 (62.5) 35 (47.3)
VRE (P 5 0.002). The VRE-colonized group also hadRaceBlack, N % 13 (81.3) 70 (94.6) 0.10 significantly greater exposures to inpatient vancomycin,White, N % 3 (18.8) 4 (5.4) aminoglycosides, anaerobic antimicrobial agents, hospi-Diabetes mellitus N % 11 (68.8) 36 (48.6) NS
tal admissions, duration of in-hospital stay, and intensiveHIV seropositive N % 1 (6.3) 7 (9.5) NSHemodialysis N % 10 (62.5) 42 (56.8) NS care unit admissions.Peritoneal dialysis N % 6 (37.5) 32 (43.2) Using logistic regression, outpatient vancomycin (g perDuration of ESRD years 2.1 (0.3–5.7) 2.2 (0.1–24.7) NS
year) was significantly associated with the developmentGroup summary data are expressed as median (range) or number (%) of
subjects as appropriate. NS is not significant. of VRE with an odds ratio (95% CI) of 1.23 (1.05, 1.44).This association remained significant following adjust-ment in separate analyses for the main potential con-founders, as shown in Table 3. This odds ratio for thecolonized with VRE when initially cultured (1996) and
are not entered into the follow-up cohort. This result association between outpatient vancomycin use and VREwas perceived as being similar to that reported by others colonization was reduced in only three of these analyses,[3, 15–18] and did not lead to any formal change in as compared with the unadjusted odds ratio (1.23). Inthe use of vancomycin in our unit. Twenty-four of the each case, however, outpatient vancomycin continued toremaining patients initially without VRE were not ana- exert a significant and independent effect. Adjustmentlyzable, as they had no subsequent VRE culture, and thus for the other potential confounders resulted in eithertheir follow-up VRE status was unknown. One patient no effect or a slight increase in this odds ratio. Whenunderwent renal transplantation. Four transferred to an- outpatient vancomycin was simultaneously adjusted forother dialysis unit, and 15 died before the VRE screen average duration of hospital stay and either inpatientat the end of the study. An additional four patients re- vancomycin dose or number of hospitalizations, the asso-mained within the cohort but declined to undergo repeat
ciation between outpatient vancomycin (g per year) andVRE screening at the end of follow-up. In comparisonVRE colonization continued to be significant, with anto the analyzable group, these 24 patients were older (P 5odds ratio of 1.29 (1.07, 1.57, P 5 0.007) and 1.22 (1.03,0.03) and were more likely to be Caucasian (P 5 0.003).1.45, P 5 0.02), respectively. More extensive regression
VRE incidence rate modeling was not undertaken because of the small num-ber of available cases (N 5 16). Repeat analyses usingThe 90 analyzable patients contributed a total of 157.2combined inpatient and outpatient vancomycin dose andyears of follow-up, with a mean duration of follow-upa subgroup analysis excluding HIV seropositive subjectsper subject of 1.75 years. Sixteen incident cases of VRErevealed similar significant results as that of the primaryrectal colonization were detected over the course of the
study, an incidence rate of 1 case per 9.83 patient years analysis (data not shown).of follow-up.
Clinical VRE infectionOf the 90 patients, only 70 patients underwent repeatVRE screening at the end of the study, of whom 6 pa- Over the course of follow-up, 6 out of 16 (37.5%)tients (8.6%) grew VRE. Two of these patients had their VRE colonized patients developed an overt infectionVRE status established previously during prior hospital- related to VRE, including one surgical site infection, oneizations; however, the VRE colonization status of the urinary tract infection, one episode of peritonitis, andremaining four subjects had been unknown to the dialysis three cases of VRE bacteremia, confirmed in at leaststaff.
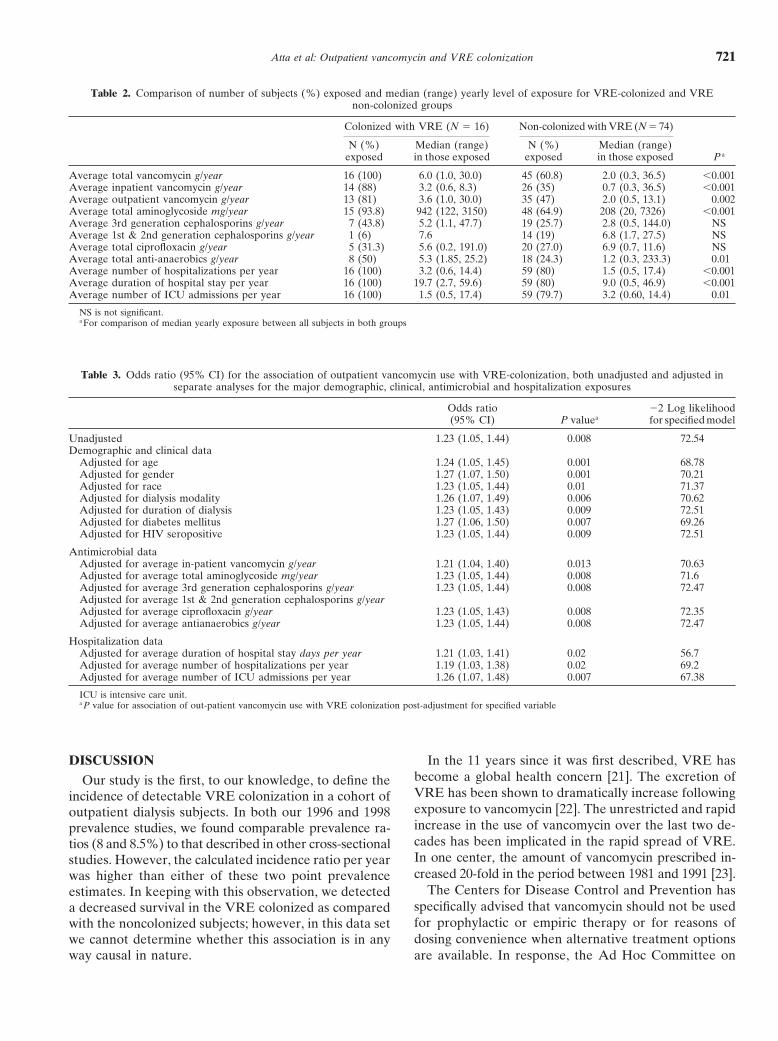
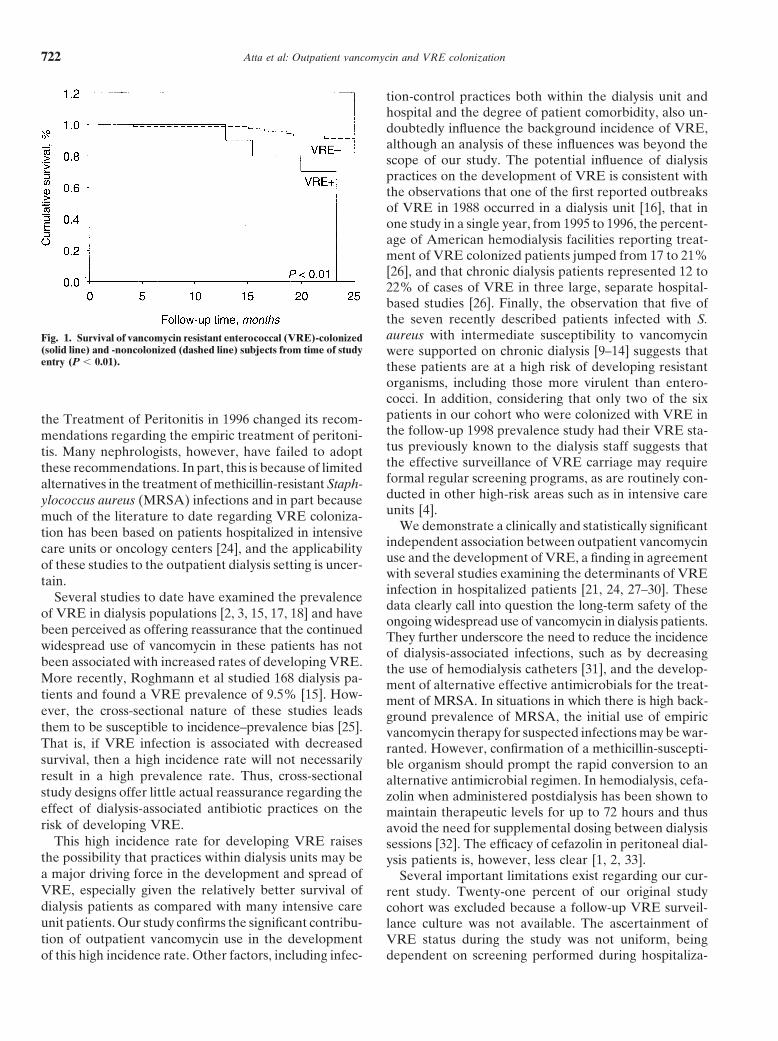
two blood culture bottles. Ten of the 90 patients (11.0%),whose follow-up VRE status was known died over theDeterminants of VRE colonizationcourse of the study. Six deaths occurred among the 74The 90 patients received a total of 403 g of intravenouspatients (8.0%) who did not grow VRE, 4 among thevancomycin, 73% of which was administered in the out-16 patients (25%) who grew VRE, including 2 of the 3patient dialysis unit. There was no significant differencebacteremic patients. Survival in the VRE colonizedin the baseline demographic characteristics, the propor-group was significantly worse than for the noncolonizedtion of patients with HIV infection, or diabetes between
patients who grew and did not grow VRE (Table 1). The group (P 5 0.005; Fig. 1).
Atta et al: Outpatient vancomycin and VRE colonization 721
Table 2. Comparison of number of subjects (%) exposed and median (range) yearly level of exposure for VRE-colonized and VREnon-colonized groups
Colonized with VRE (N 5 16) Non-colonized with VRE (N 5 74)
N (%) Median (range) N (%) Median (range)exposed in those exposed exposed in those exposed P a
Average total vancomycin g/year 16 (100) 6.0 (1.0, 30.0) 45 (60.8) 2.0 (0.3, 36.5) ,0.001Average inpatient vancomycin g/year 14 (88) 3.2 (0.6, 8.3) 26 (35) 0.7 (0.3, 36.5) ,0.001Average outpatient vancomycin g/year 13 (81) 3.6 (1.0, 30.0) 35 (47) 2.0 (0.5, 13.1) 0.002Average total aminoglycoside mg/year 15 (93.8) 942 (122, 3150) 48 (64.9) 208 (20, 7326) ,0.001Average 3rd generation cephalosporins g/year 7 (43.8) 5.2 (1.1, 47.7) 19 (25.7) 2.8 (0.5, 144.0) NSAverage 1st & 2nd generation cephalosporins g/year 1 (6) 7.6 14 (19) 6.8 (1.7, 27.5) NSAverage total ciprofloxacin g/year 5 (31.3) 5.6 (0.2, 191.0) 20 (27.0) 6.9 (0.7, 11.6) NSAverage total anti-anaerobics g/year 8 (50) 5.3 (1.85, 25.2) 18 (24.3) 1.2 (0.3, 233.3) 0.01Average number of hospitalizations per year 16 (100) 3.2 (0.6, 14.4) 59 (80) 1.5 (0.5, 17.4) ,0.001Average duration of hospital stay per year 16 (100) 19.7 (2.7, 59.6) 59 (80) 9.0 (0.5, 46.9) ,0.001Average number of ICU admissions per year 16 (100) 1.5 (0.5, 17.4) 59 (79.7) 3.2 (0.60, 14.4) 0.01
NS is not significant.a For comparison of median yearly exposure between all subjects in both groups
Table 3. Odds ratio (95% CI) for the association of outpatient vancomycin use with VRE-colonization, both unadjusted and adjusted inseparate analyses for the major demographic, clinical, antimicrobial and hospitalization exposures
Odds ratio 22 Log likelihood(95% CI) P valuea for specified model
Unadjusted 1.23 (1.05, 1.44) 0.008 72.54Demographic and clinical data
Adjusted for age 1.24 (1.05, 1.45) 0.001 68.78Adjusted for gender 1.27 (1.07, 1.50) 0.001 70.21Adjusted for race 1.23 (1.05, 1.44) 0.01 71.37Adjusted for dialysis modality 1.26 (1.07, 1.49) 0.006 70.62Adjusted for duration of dialysis 1.23 (1.05, 1.43) 0.009 72.51Adjusted for diabetes mellitus 1.27 (1.06, 1.50) 0.007 69.26Adjusted for HIV seropositive 1.23 (1.05, 1.44) 0.009 72.51
Antimicrobial dataAdjusted for average in-patient vancomycin g/year 1.21 (1.04, 1.40) 0.013 70.63Adjusted for average total aminoglycoside mg/year 1.23 (1.05, 1.44) 0.008 71.6Adjusted for average 3rd generation cephalosporins g/year 1.23 (1.05, 1.44) 0.008 72.47Adjusted for average 1st & 2nd generation cephalosporins g/yearAdjusted for average ciprofloxacin g/year 1.23 (1.05, 1.43) 0.008 72.35Adjusted for average antianaerobics g/year 1.23 (1.05, 1.44) 0.008 72.47
Hospitalization dataAdjusted for average duration of hospital stay days per year 1.21 (1.03, 1.41) 0.02 56.7Adjusted for average number of hospitalizations per year 1.19 (1.03, 1.38) 0.02 69.2Adjusted for average number of ICU admissions per year 1.26 (1.07, 1.48) 0.007 67.38
ICU is intensive care unit.a P value for association of out-patient vancomycin use with VRE colonization post-adjustment for specified variable
DISCUSSION In the 11 years since it was first described, VRE hasbecome a global health concern [21]. The excretion ofOur study is the first, to our knowledge, to define theVRE has been shown to dramatically increase followingincidence of detectable VRE colonization in a cohort ofexposure to vancomycin [22]. The unrestricted and rapidoutpatient dialysis subjects. In both our 1996 and 1998increase in the use of vancomycin over the last two de-prevalence studies, we found comparable prevalence ra-cades has been implicated in the rapid spread of VRE.tios (8 and 8.5%) to that described in other cross-sectionalIn one center, the amount of vancomycin prescribed in-studies. However, the calculated incidence ratio per yearcreased 20-fold in the period between 1981 and 1991 [23].was higher than either of these two point prevalence
The Centers for Disease Control and Prevention hasestimates. In keeping with this observation, we detectedspecifically advised that vancomycin should not be useda decreased survival in the VRE colonized as comparedfor prophylactic or empiric therapy or for reasons ofwith the noncolonized subjects; however, in this data setdosing convenience when alternative treatment optionswe cannot determine whether this association is in any
way causal in nature. are available. In response, the Ad Hoc Committee on
Atta et al: Outpatient vancomycin and VRE colonization722
tion-control practices both within the dialysis unit andhospital and the degree of patient comorbidity, also un-doubtedly influence the background incidence of VRE,although an analysis of these influences was beyond thescope of our study. The potential influence of dialysispractices on the development of VRE is consistent withthe observations that one of the first reported outbreaksof VRE in 1988 occurred in a dialysis unit [16], that inone study in a single year, from 1995 to 1996, the percent-age of American hemodialysis facilities reporting treat-ment of VRE colonized patients jumped from 17 to 21%[26], and that chronic dialysis patients represented 12 to22% of cases of VRE in three large, separate hospital-based studies [26]. Finally, the observation that five ofthe seven recently described patients infected with S.aureus with intermediate susceptibility to vancomycinFig. 1. Survival of vancomycin resistant enterococcal (VRE)-colonized
(solid line) and -noncolonized (dashed line) subjects from time of study were supported on chronic dialysis [9–14] suggests thatentry (P , 0.01). these patients are at a high risk of developing resistant
organisms, including those more virulent than entero-cocci. In addition, considering that only two of the sixpatients in our cohort who were colonized with VRE inthe Treatment of Peritonitis in 1996 changed its recom-the follow-up 1998 prevalence study had their VRE sta-mendations regarding the empiric treatment of peritoni-tus previously known to the dialysis staff suggests thattis. Many nephrologists, however, have failed to adoptthe effective surveillance of VRE carriage may requirethese recommendations. In part, this is because of limitedformal regular screening programs, as are routinely con-alternatives in the treatment of methicillin-resistant Staph-ducted in other high-risk areas such as in intensive careylococcus aureus (MRSA) infections and in part becauseunits [4].much of the literature to date regarding VRE coloniza-
We demonstrate a clinically and statistically significanttion has been based on patients hospitalized in intensiveindependent association between outpatient vancomycincare units or oncology centers [24], and the applicabilityuse and the development of VRE, a finding in agreementof these studies to the outpatient dialysis setting is uncer-with several studies examining the determinants of VREtain.infection in hospitalized patients [21, 24, 27–30]. TheseSeveral studies to date have examined the prevalencedata clearly call into question the long-term safety of the
of VRE in dialysis populations [2, 3, 15, 17, 18] and haveongoing widespread use of vancomycin in dialysis patients.
been perceived as offering reassurance that the continued They further underscore the need to reduce the incidencewidespread use of vancomycin in these patients has not of dialysis-associated infections, such as by decreasingbeen associated with increased rates of developing VRE. the use of hemodialysis catheters [31], and the develop-More recently, Roghmann et al studied 168 dialysis pa- ment of alternative effective antimicrobials for the treat-tients and found a VRE prevalence of 9.5% [15]. How- ment of MRSA. In situations in which there is high back-ever, the cross-sectional nature of these studies leads ground prevalence of MRSA, the initial use of empiricthem to be susceptible to incidence–prevalence bias [25]. vancomycin therapy for suspected infections may be war-That is, if VRE infection is associated with decreased ranted. However, confirmation of a methicillin-suscepti-survival, then a high incidence rate will not necessarily ble organism should prompt the rapid conversion to anresult in a high prevalence rate. Thus, cross-sectional alternative antimicrobial regimen. In hemodialysis, cefa-study designs offer little actual reassurance regarding the zolin when administered postdialysis has been shown toeffect of dialysis-associated antibiotic practices on the maintain therapeutic levels for up to 72 hours and thusrisk of developing VRE. avoid the need for supplemental dosing between dialysis
This high incidence rate for developing VRE raises sessions [32]. The efficacy of cefazolin in peritoneal dial-the possibility that practices within dialysis units may be ysis patients is, however, less clear [1, 2, 33].a major driving force in the development and spread of Several important limitations exist regarding our cur-VRE, especially given the relatively better survival of rent study. Twenty-one percent of our original studydialysis patients as compared with many intensive care cohort was excluded because a follow-up VRE surveil-unit patients. Our study confirms the significant contribu- lance culture was not available. The ascertainment oftion of outpatient vancomycin use in the development VRE status during the study was not uniform, being
dependent on screening performed during hospitaliza-of this high incidence rate. Other factors, including infec-

Atta et al: Outpatient vancomycin and VRE colonization 723
authors acknowledge the assistance of Pam Babij, CNP; Martha Con-tions. This may have potentially introduced a bias associ-lon, RN; Nancy Feeley, CNP; Doreen Kuhn, CNP; and Shelly Malan,
ating VRE with hospitalization. However, it would not RN, BSN, for their help in the conduct of this study. They also thankSarah Dieter for her secretarial assistance and Professor Joseph Han-explain an association with the outpatient use of vanco-dler and Professor Neil R. Powe for their review of the manuscript.mycin, which in the majority of cases does not lead to
hospitalization. While our ascertainment of outpatient Reprint requests Mohamed G. Atta, M.D., Division of Nephrology,Johns Hopkins University, 1830 East Monument Street, Suite 416, Balti-vancomycin use is likely to be complete, as this wasmore, Maryland 21205, USA.exclusively used in the dialysis unit, we are unlikely toE-mail: [email protected]
have complete exposure information on several potentialrisk factors. In-hospital information was only available
REFERENCESfor patients hospitalized at Johns Hopkins Hospital;
1. Ng R, Zabetakis PM, Callahan C, et al: Vancomycin-resistanthowever, as our dialysis unit is situated adjacent to Johnsenterococcus infection is a rare complication in patients receiving
Hopkins Hospital and serves a local and largely unin- PD on an outpatient basis. Perit Dial Int 19:273–274, 19992. Sandoe JA, Gokal R, Struthers JK: Vancomycin-resistant enter-sured population, it is therefore the primary care facility
ococci and empirical vancomycin for CAPD peritonitis. (letter)for these patients. In a survey conducted in 1997, wePerit Dial Int 17:617–618, 1997
found that over 90% of our dialysis patients were either 3. Brady JP, Snyder JW, Hasbargen JA: Vancomycin-resistant en-terococcus in end stage renal disease. Am J Kidney Dis 32:415–418,hospitalized directly to Johns Hopkins Hospital or were1998subsequently transferred there following admission to
4. Hospital Infection Control Practices Advisory Committeeanother facility (Brigitte Sullivan, personal communica- (HICPAP): Recommendations for preventing the spread of vanco-
mycin resistance. Infect Control Hosp Epidemiol 16:105–113, 1995tion). We have, however, no reason to believe that in-5. Ad Hoc Advisory Committee on Peritonitis Management: Peri-complete ascertainment of the previously mentioned
toneal dialysis-related peritonitis treatment recommendations 1996variables should have introduced a bias leading to a update. Perit Dial Int 16:557–573, 1996
6. Leclerq R, Derlot E, Duval J, et al: Plasmid mediated resistancespurious association with the outpatient use of vancomy-to vancomycin and teicoplanin in Enterococcus faecium. N Englcin. Although our study shows a strong independentJ Med 319:157–161, 1988
association between outpatient vancomycin and VRE 7. Eliopoulos GM: Vancomycin-resistant Enterococci. Mechanismand clinical relevance. Infect Dis Clin North Am 11:851–865, 1997colonization, due to its observational nature, it is clearly
8. Arthur M, Molinas C, Depardieu F, et al: Characterization ofunable to prove that the demonstrated association isTn1546, a Tn3-related transposon conferring glycopeptide resis-
causative in nature. tance by synthesis of depsipeptide peptidoglycan precursors inEnterococcus faecium BM4147. J Bacteriol 175:117–127, 1993In conclusion, we demonstrate a high incidence of
9. Hiramatsu K, Artaka N, Hanaki H, et al: Dissemination in Japa-VRE among chronic dialysis subjects. There is a strong,nese hospitals of strains of Staphylococcus aureus heterogenously
statistically significant and independent effect of outpa- resistant to vancomycin. Lancet 350:1670–1673, 199710. Sieradzki K, Roberts RB, Haber SW, et al: The developmenttient vancomycin use on the development of VRE. Pend-
of vancomycin resistance in a patient with methicillin resistanting further results from larger prospective studies, weStaphylococcus aureus infection. N Engl J Med 340:517–523, 1999
believe that, in keeping with suggested recommendations 11. Centers for Disease Control and Prevention: Update: Staphylo-coccus aureus with reduced susceptibility to Vancomycin—United[4, 5], the outpatient use of vancomycin in the chronicStates, 1997. MMWR Morb Mortal Wkly Rep 46:813–815, 1997dialysis setting should be avoided whenever possible.
12. Smith TL, Pearson ML, Wilcox KR: Emergence of vancomycinFurther research is urgently required in order to examine resistance in Staphylococcus aureus. N Engl J Med 340:493–501,
1999and develop alternative regimens for the empiric treat-13. Staphylococcus aureus with reduced susceptibility to vancomycin-ment of suspected dialysis-associated infections. The role United States. MMWR Morb Mortal Wkly Rep 46:765–766, 1997
and optimal method of screening for VRE in dialysis 14. Staphylococcus aureus with reduced susceptibility to vancomycin-Illinois, 1999. MMWR Morb Mortal Wkly Rep 48:1165–1167, 2000patients also needs to be examined. Finally, the fre-
15. Roghmann MC, Fink JC, Polish L, et al: Colonization with vanco-quency with which cross-infection of VRE occurs within mycin resistant enterococci in chronic hemodialysis patients. Amthe dialysis unit requires investigation. To date there J Kidney Dis 32:254–257, 1998
16. Uttley AH, George RC, Naidoo J: High-level vancomycin-resis-are no specific guidelines on the management of VRE-tant enterococci causing hospital infection. Epidemiol Infect 103:colonized dialysis patients or formal recommendations 173–181, 1989
regarding infection control management of such patients 17. Koroff A, Larson E, Kumar P, et al: Vancomycin resistant entero-coccus in a hospital based dialysis unit. ANNA J 25:381–386, 1998in the setting of a dialysis unit. Limiting the spread of
18. Low CL, Eisele G, Cerda J, et al: Low prevalence of vancomycin-VRE represents a major challenge facing the dialysis resistant Enterococcus in dialysis outpatients with history of vanco-community; however, it is clearly essential in order to mycin use. Perit Dial Int 16:651–652, 1996
19. Facklam RR, Collins MD: Identification of enterococcus speciessafeguard both the public health and the health of pa-isolated from human infections by a conventional test scheme.tients treated by long-term maintenance dialysis. J Clin Microbiol 27:731–734, 1989
20. National Committee for Clinical Laboratory Standards: Meth-ods for Dilution Antimicrobial Susceptibility Tests for Bacteria ThatACKNOWLEDGMENTSGrow Aerobically (4th ed). Villanova, Approved Standard M7-A4,
Dr. Atta was supported by a grant from the National Kidney Foun- 1997dation of Maryland. Dr. Eustace was supported in part by a Johns 21. Boyce JM: Vancomycin-resistant enterococcus. Infect Dis Clin
North Am 11:367–384, 1997Hopkins University Clinical Scientist Career Development award. The

Atta et al: Outpatient vancomycin and VRE colonization724
22. Van der Auwera P, Pensart N, Korten V, et al: Influence of 28. Hafner A, Riley LW: Risk factors associated with vancomycinresistant Enterococcus faecium infection or colonization in 145oral glycopeptides on the fecal flora of human volunteers: Selectionmatched patients and control patients. Clin Infect Dis 23:767–772,of highly glycopeptide-resistant Enterococci. J Infect Dis 173:1129–19961136, 1996
29. Handwerger S, Raucher B, Altarac D, et al: Noscomial outbreak23. Ena J, Dick RW, Jones RN, et al: The epidemiology of intravenousdue to Enterococcus faecium highly resistant to vancomycin, peni-vancomycin use in a university hospital. JAMA 269:598–602, 1993cillin and gentamicin. Clin Infect Dis 16:750–755, 199324. Bhorade SM, Christenson J, Pohlman AS, et al: The incidence
30. Rubin LG, Tucci V, Cercenado E, et al: Vancomycin-resistantof and clinical variables associated with vancomycin-resistant en-Enterococcus faecium in hospitalized children. Infect Control Hospterococcal colonization in mechanically ventilated patients. ChestEpidemiol 13:700–705, 1992115:1085–1091, 1999
31. Powe RN, Jaar B, Furth SL, et al: Septicemia in dialysis patients:25. Sackett DL: Bias in analytical research. J Chronic Dis 32:51–63, Incidence, risk factors and prognosis. Kidney Int 55:1081–1090,1979 1999
26. Tokars IJ: Vancomycin use and antimicrobial resistance in hemo- 32. Marx MA, Frye RF, Matzke GR, et al: Cefazolin as empiricdialysis centers. Am J Kidney Dis 32:521–523, 1998 therapy in hemodialysis-related patients: Efficacy and blood con-
27. Morris JG, Shay DK, Hebden JN: Enterococci resistant to multi- centrations. Am J Kidney Dis 32:410–414, 1998ple antimicrobial agents including vancomycin: Establishment of 33. Vas S, Bargman J, Orepoulos DG: Treatment in PD patients ofendemicity in a university medical center. Ann Intern Med 123:250– peritonitis caused by gram-positive organisms with single daily
dose of antibiotics. Perit Dial Int 17:91–94, 1997259, 1995