Embed Size (px)
Citation preview

Aortic Surgery Symposium 2010
New York, NYApril, 2010
Department of Cardiothoracic and Vascular Surgery
The University of Texas Medical School at HoustonMemorial Hermann Heart & Vascular
Institute
AL Estrera, MD, CC Miller III, PhD, TK Lee, MD, T Kaneko, MD, JC Walkes, MD, H Safi, MD
Outcomes of Acute Type A Aortic Dissection After Previous Cardiac Surgery

Purpose
• Since few data exist, we report outcomes of acute type A aortic dissection (ATAAD) after previous cardiac surgery (PCS).

Methods
330 Acute Type A Aortic Dissection
Jan. 1991 – March 2009
Median age: 62 (21-91)
69%
31%
281 Primary (85%) 49 PCS (15%)

Variable
Previous Cardiac Surgery
Group
Number (%)n=49
Primary Group
Number (%)n=49
P-Value
Age 63+12.8 57.9+13.9 <.02
Male Gender 40 (82) 187 (67) <.04
Chest Pain 40 (82) 256 (91) .07
Back Pain 36 (73) 215 (77) .72
Leg Weakness 10 (20) 48 (17) .55
Stroke 1 (2) 29 (10) .07
Paraplegia 4 (8) 17 (6) .53
Hypotension 10 (20) 70 (25) .59
Tamponade 6 (all CABG) (12) 48 (17) .42
Myocardial Ischemia 5 (10) 25 (9) .79
Al (Mod Sev) 15 (30) 132 (47) <.05Time Interval (Admission-OR) Hours 46.4+63.3 37.1+73.1 .40
Aortic Size 5.7+1.4 5.0+0.8 .0001
PA Rupture/Fistula 2 (4) 0 (0) <.03
Preoperative Variables in Acute Type A Aortic Dissection with/without PCS

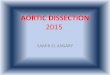
Mean Interval 56 ± 77 monthsInterval range 3d - 370 months
Interval
2 pts: 2 previous sternotomies2 pts: 2 previous sternotomies

Previous Cardiac Surgery

Procedures (Re-Op)Procedures (Re-Op)
Aortic Root
8%
Ascending
100%
Prox Arch
94%
CABG 16%
Total Arch
10%
ET1 4%

Variable
Previous Cardiac Surgery
Number (%)n=49
No Previous Cardiac Surgery
Number (%)n=281 P-Value
MI 4 (8) 15 (5) .50
CVA/Coma 5 (10) 7 (2.5) <.03
TND 12 (24) 28 (10) <.007
Bleed 2 (4) 24 (8.5) .39
Renal Failure (Dialysis) 6 (12) 28 (9.9) .55
Repiratory Failure (Vent >3 days) 16 (33) 85 (30) .58
Hospital Death 15 (31) 39 (13.8) <.007
Results

Cause N (%) N=15
CardiacPreoperative tamponade (4)Right ventricular failure (1)AMI (occlude RCA SVG) (1)EF=10% (1)
7 (47)
Multiorgan failure(Necrotic bowel, ARF, PA fistula, paraplegia)
7 (47)
Neurological (Preoperative coma)
1 (6)
Causes of Early Death

Location N (%) n=49 Note
De Novo 25 (51)
Aortic Cannulation Site 2 (4)
Aortotomy 6 (12) 40% (Valves*)
Saphenous Vein Graft Site 16 (33) 46% (CABG)
Location of Aortic Dissection Tear
* 12/15 (80%) of previous valves had a Bicuspid Aortic Valve

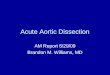
Survival: Kaplan-Meier
P<0.03
1-year 5 10 15
Primary
80% 76% 58% 53%
PCS 62% 57% 50% 36%

Patients with ATAAD following PCS exhibited risks for malperfusion, hypotension, and cardiac tamponade that were similar to primary ATAAD cases.
This suggests that adhesions formed after PCS do not eliminate the risk of cardiac tamponade from aortic rupture.
Although results from surgical repair are acceptable, and thus justifying timely repair, mortality still remains higher than without a prior history of cardiac surgery.
Patients need to be individualized.
Conclusions