Embed Size (px)
Citation preview
Outcomes Following Inpatient Rehabilitation Following Brain Injury:
Who is Treated…and How Do They Do?
2
Presented by Liam Dessureault PT, MSc
3
“Once you set aside the acute phases or crises that mark injury or disease, much of modern health care is indeed rehabilitation in one form or another.”
David Naylor, MD, Former President, University of Toronto
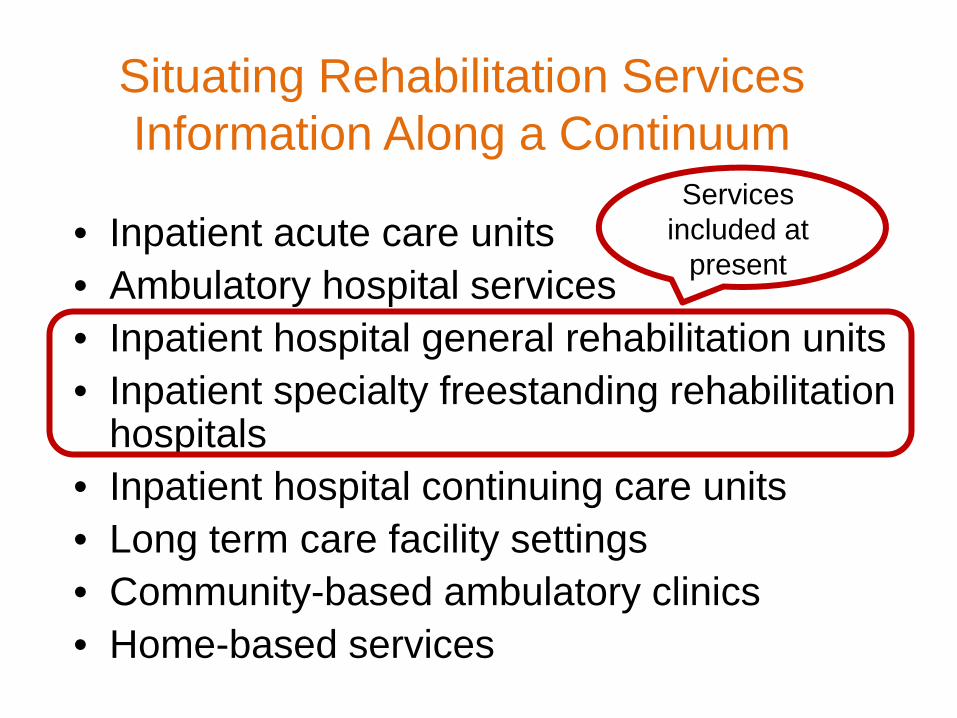
Situating Rehabilitation Services Information Along a Continuum
• Inpatient acute care units • Ambulatory hospital services • Inpatient hospital general rehabilitation units • Inpatient specialty freestanding rehabilitation
hospitals • Inpatient hospital continuing care units • Long term care facility settings • Community-based ambulatory clinics • Home-based services
Services included at
present
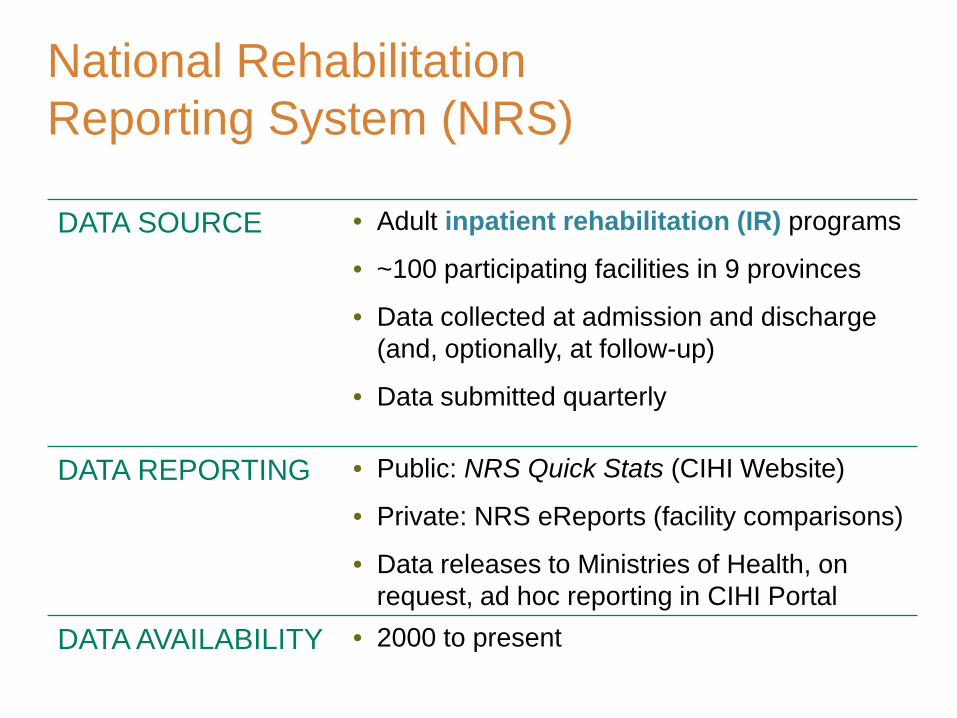
National Rehabilitation Reporting System (NRS)
DATA SOURCE • Adult inpatient rehabilitation (IR) programs
• ~100 participating facilities in 9 provinces
• Data collected at admission and discharge (and, optionally, at follow-up)
• Data submitted quarterly
DATA REPORTING • Public: NRS Quick Stats (CIHI Website)
• Private: NRS eReports (facility comparisons)
• Data releases to Ministries of Health, on request, ad hoc reporting in CIHI Portal
DATA AVAILABILITY • 2000 to present
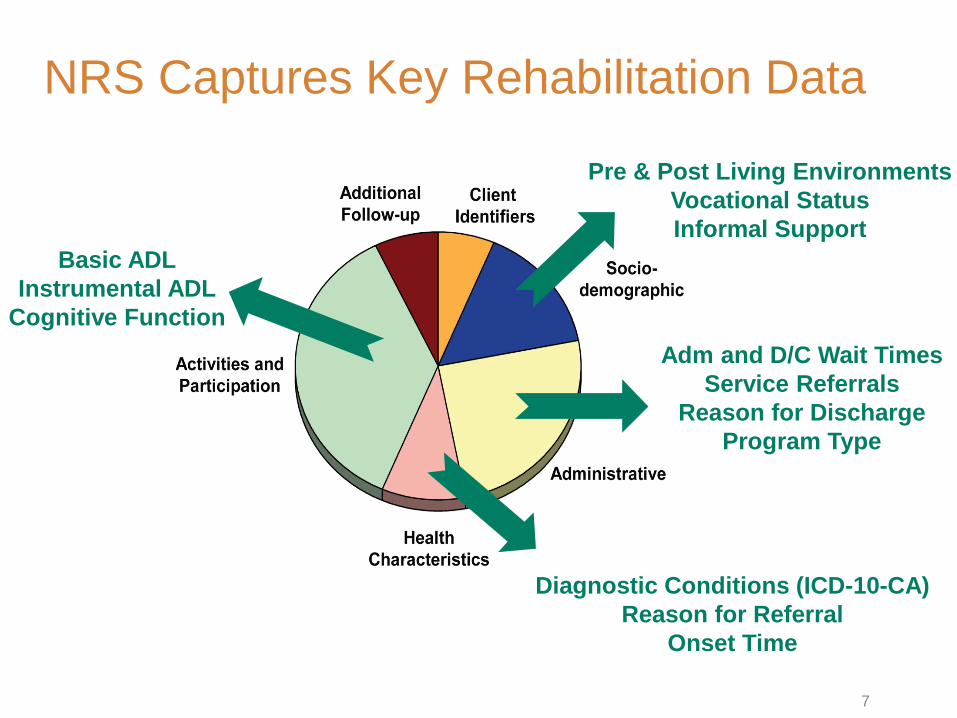
NRS Captures Key Rehabilitation Data
Basic ADL Instrumental ADL
Cognitive Function
7
Pre & Post Living Environments Vocational Status Informal Support
Adm and D/C Wait Times Service Referrals
Reason for Discharge Program Type
Diagnostic Conditions (ICD-10-CA) Reason for Referral
Onset Time
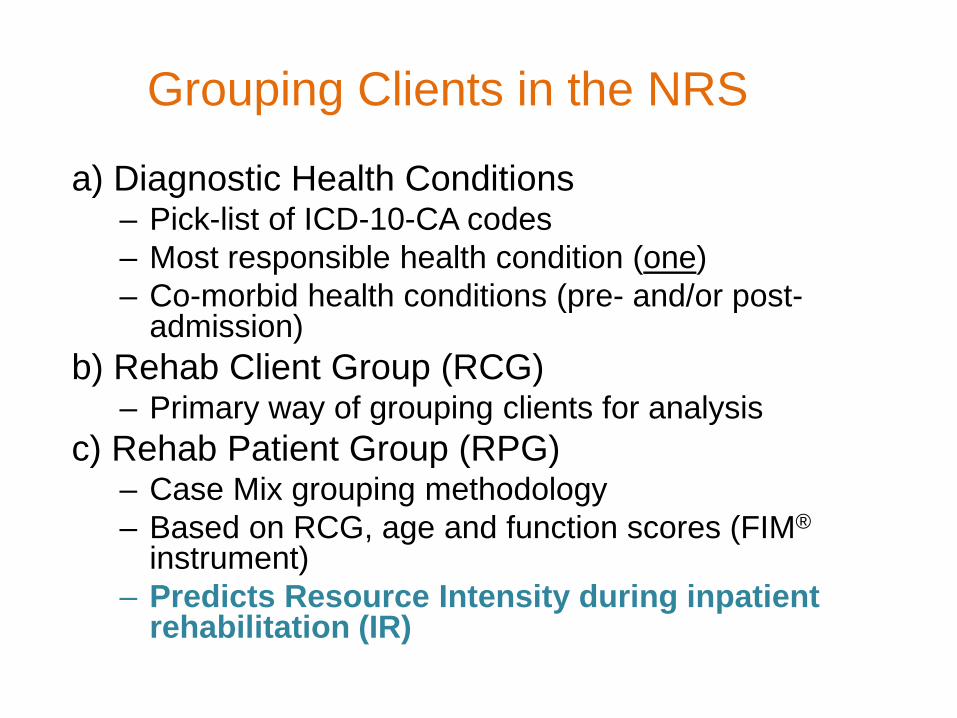
Grouping Clients in the NRS
a) Diagnostic Health Conditions – Pick-list of ICD-10-CA codes – Most responsible health condition (one) – Co-morbid health conditions (pre- and/or post-
admission) b) Rehab Client Group (RCG)
– Primary way of grouping clients for analysis c) Rehab Patient Group (RPG)
– Case Mix grouping methodology – Based on RCG, age and function scores (FIM®
instrument) – Predicts Resource Intensity during inpatient
rehabilitation (IR)

9
10
You are right here
12
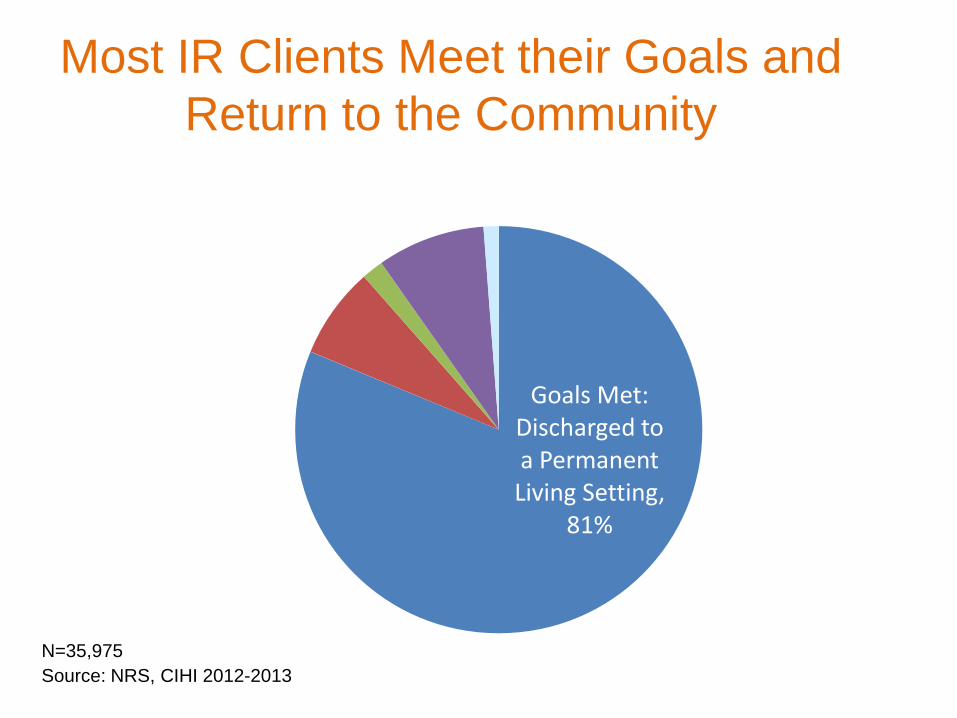
Goals Met: Discharged to a Permanent
Living Setting, 81%
Most IR Clients Meet their Goals and Return to the Community
Source: NRS, CIHI 2012-2013 N=35,975
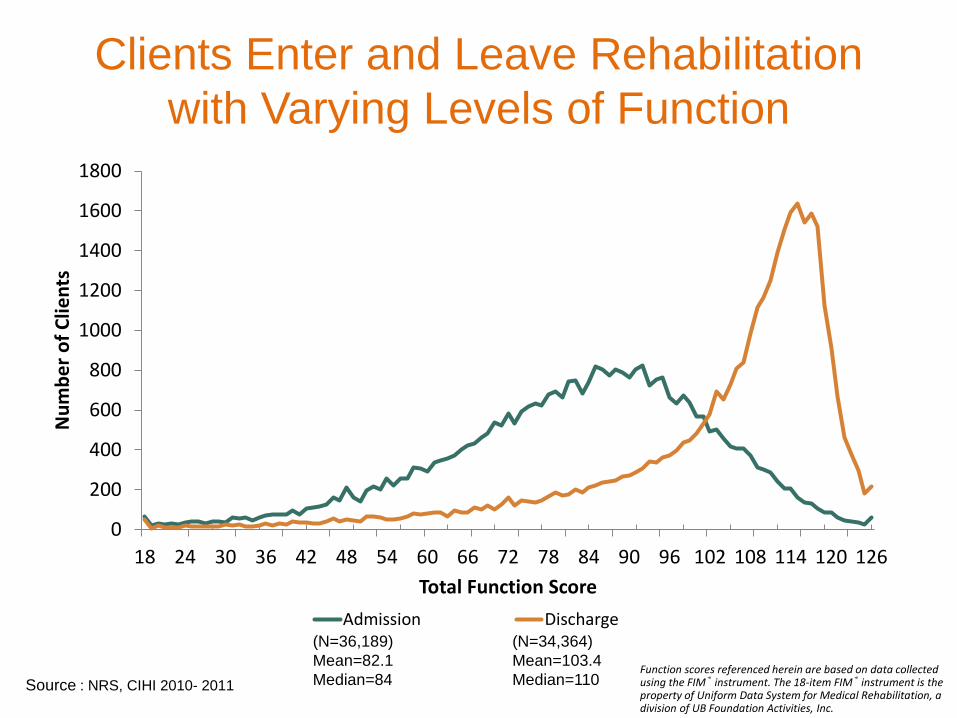
Clients Enter and Leave Rehabilitation with Varying Levels of Function
0
200
400
600
800
1000
1200
1400
1600
1800
18 24 30 36 42 48 54 60 66 72 78 84 90 96 102 108 114 120 126
Num
ber o
f Clie
nts
Total Function Score Admission Discharge
Source : NRS, CIHI 2010- 2011
(N=36,189) Mean=82.1 Median=84
(N=34,364) Mean=103.4 Median=110
Function scores referenced herein are based on data collected using the FIM® instrument. The 18-item FIM® instrument is the property of Uniform Data System for Medical Rehabilitation, a division of UB Foundation Activities, Inc.
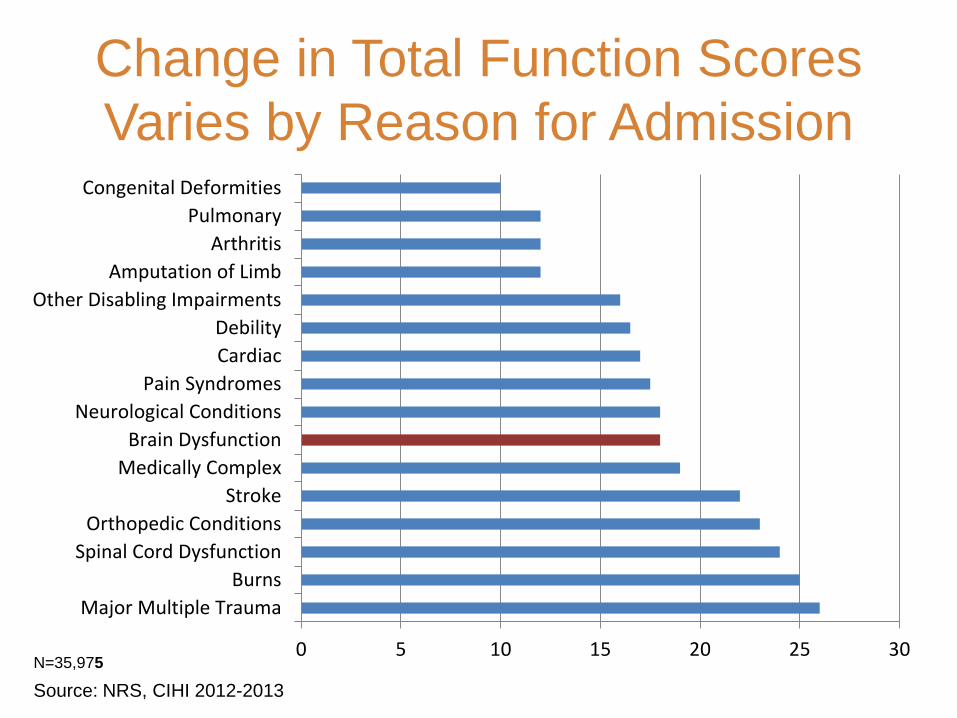
Change in Total Function Scores Varies by Reason for Admission
0 5 10 15 20 25 30
Major Multiple TraumaBurns
Spinal Cord DysfunctionOrthopedic Conditions
StrokeMedically Complex
Brain DysfunctionNeurological Conditions
Pain SyndromesCardiacDebility
Other Disabling ImpairmentsAmputation of Limb
ArthritisPulmonary
Congenital Deformities
Source: NRS, CIHI 2012-2013 N=35,975
Outcomes Following Inpatient Rehabilitation Following Brain Injury:
Who is Treated…and How Do They Do?
16
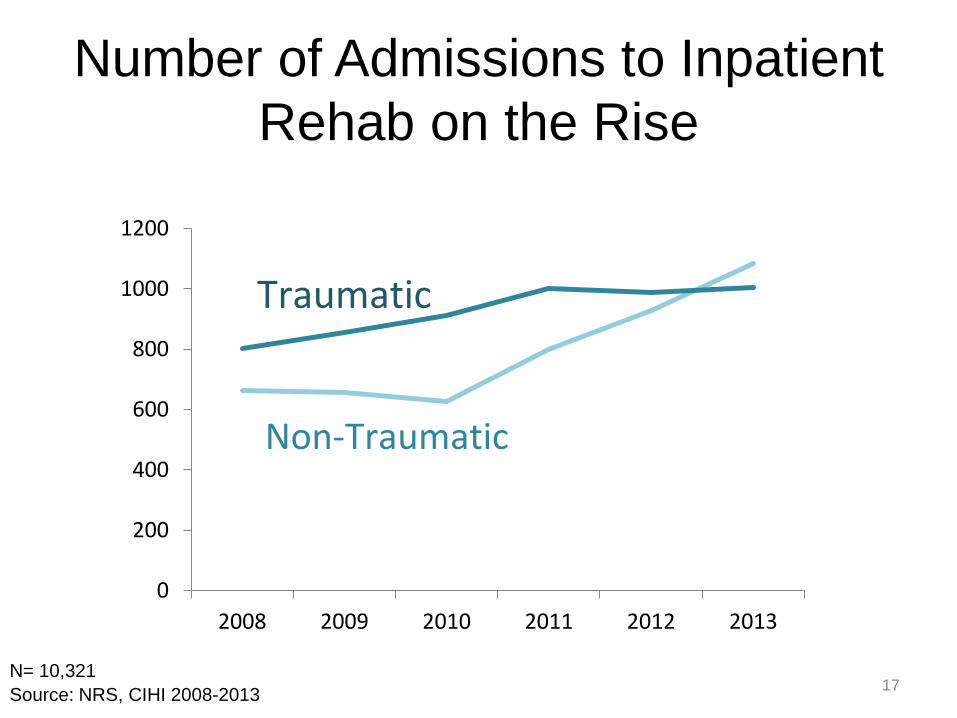
Number of Admissions to Inpatient Rehab on the Rise
0
200
400
600
800
1000
1200
2008 2009 2010 2011 2012 2013
Non-Traumatic
Traumatic
N= 10,321 17 Source: NRS, CIHI 2008-2013
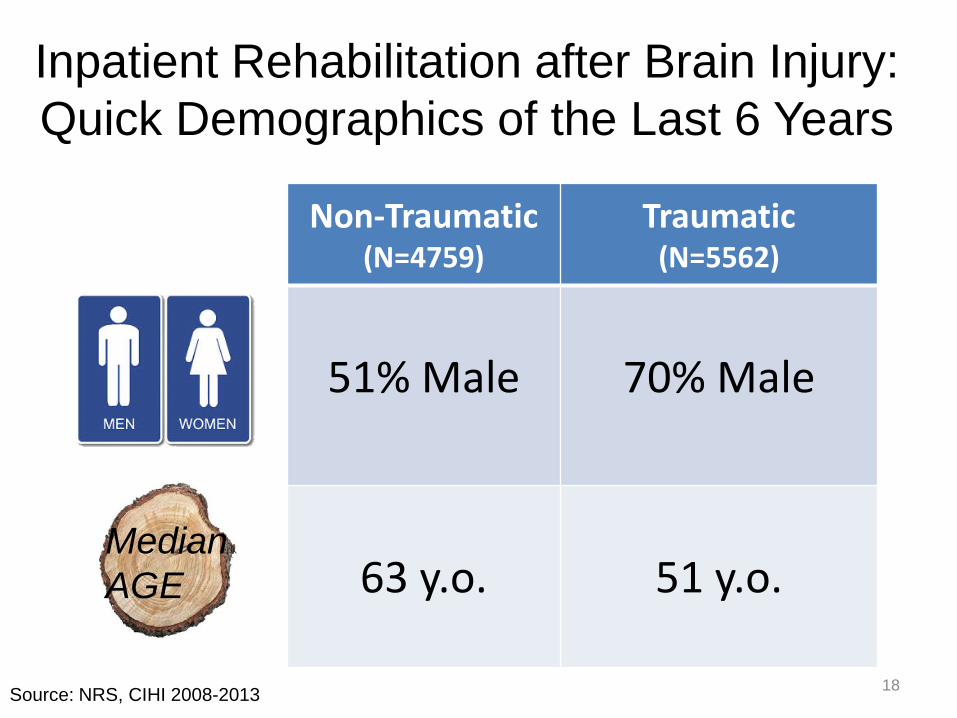
Inpatient Rehabilitation after Brain Injury: Quick Demographics of the Last 6 Years
Median AGE
Non-Traumatic (N=4759)
Traumatic (N=5562)
51% Male
70% Male
63 y.o.
51 y.o.
18 Source: NRS, CIHI 2008-2013
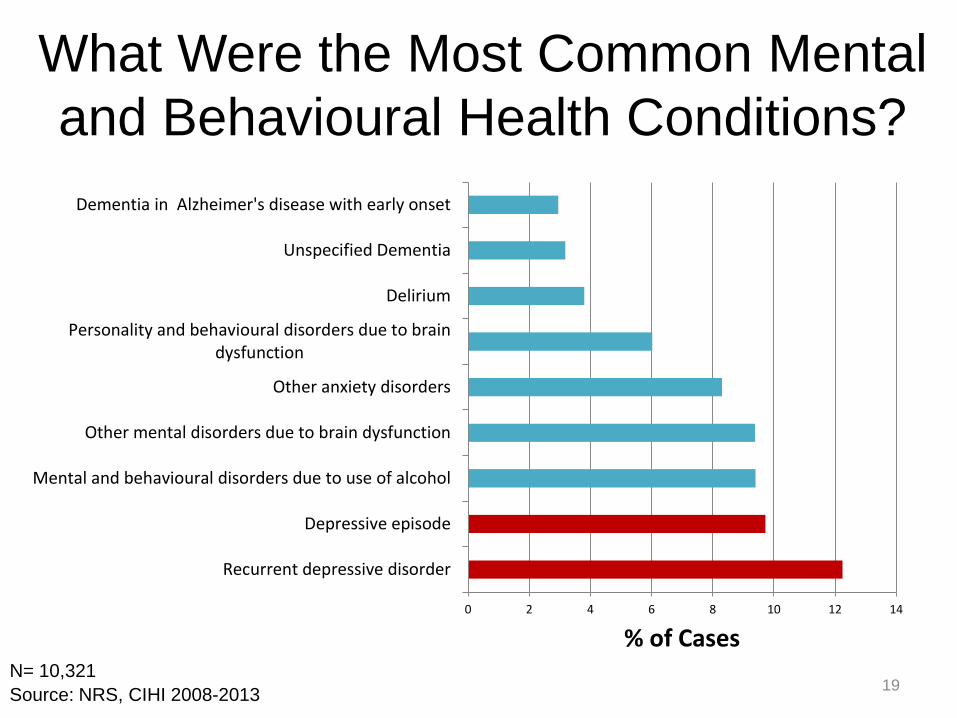
What Were the Most Common Mental and Behavioural Health Conditions?
0 2 4 6 8 10 12 14
Recurrent depressive disorder
Depressive episode
Mental and behavioural disorders due to use of alcohol
Other mental disorders due to brain dysfunction
Other anxiety disorders
Personality and behavioural disorders due to braindysfunction
Delirium
Unspecified Dementia
Dementia in Alzheimer's disease with early onset
% of Cases
19 Source: NRS, CIHI 2008-2013 N= 10,321
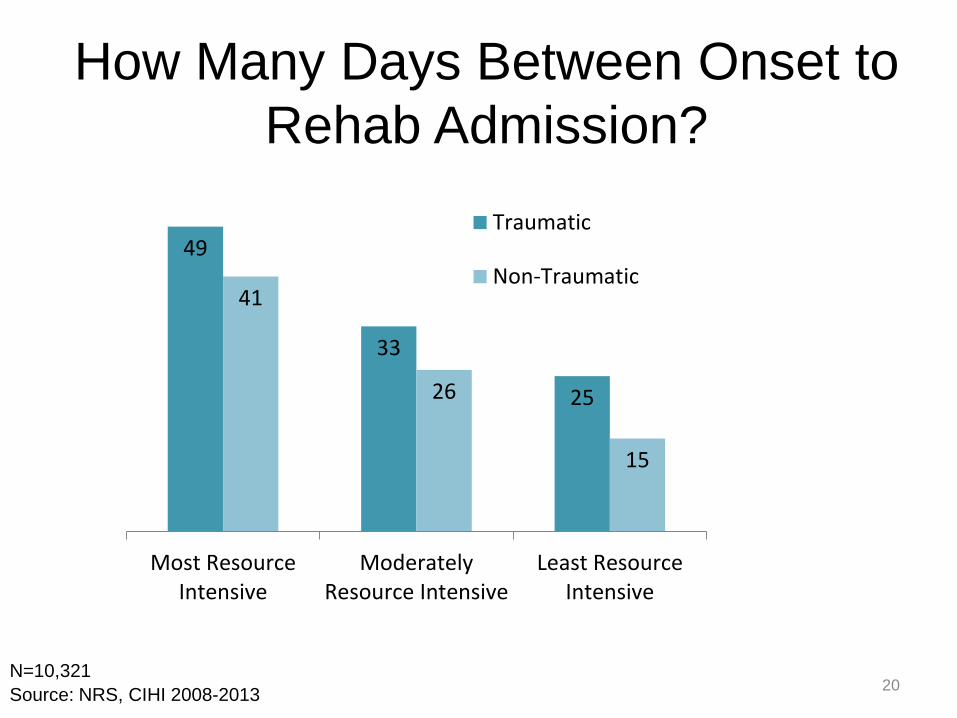
How Many Days Between Onset to Rehab Admission?
49
33
25
41
26
15
Most ResourceIntensive
ModeratelyResource Intensive
Least ResourceIntensive
Traumatic
Non-Traumatic
20 Source: NRS, CIHI 2008-2013 N=10,321
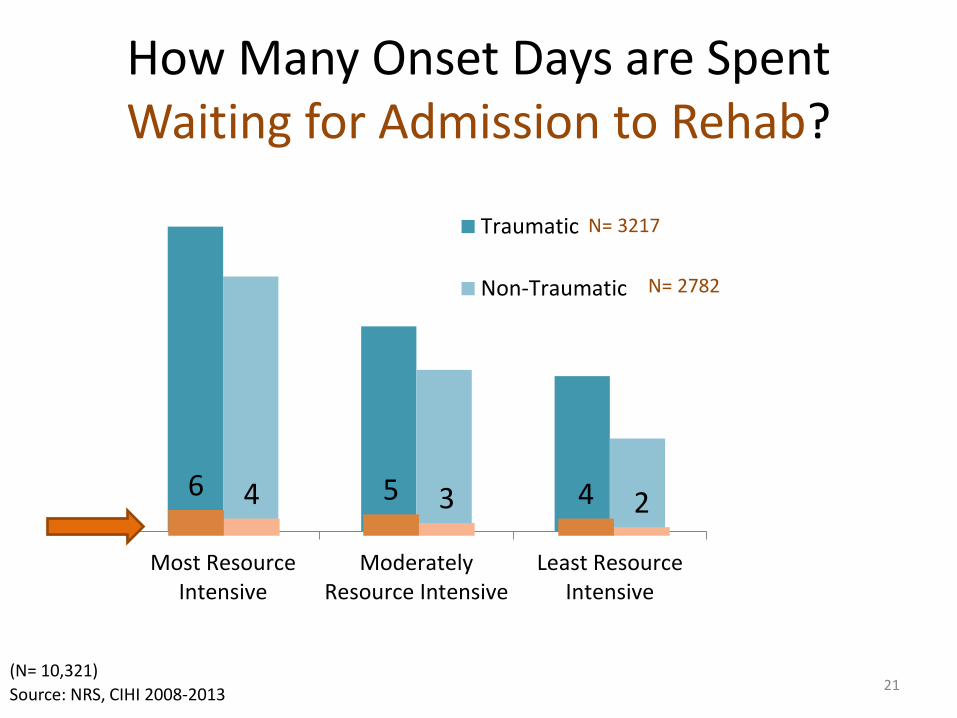
How Many Onset Days are Spent Waiting for Admission to Rehab?
Most ResourceIntensive
ModeratelyResource Intensive
Least ResourceIntensive
Traumatic
Non-Traumatic
6 5 4 4 3 2
N= 3217
N= 2782
21 Source: NRS, CIHI 2008-2013 (N= 10,321)
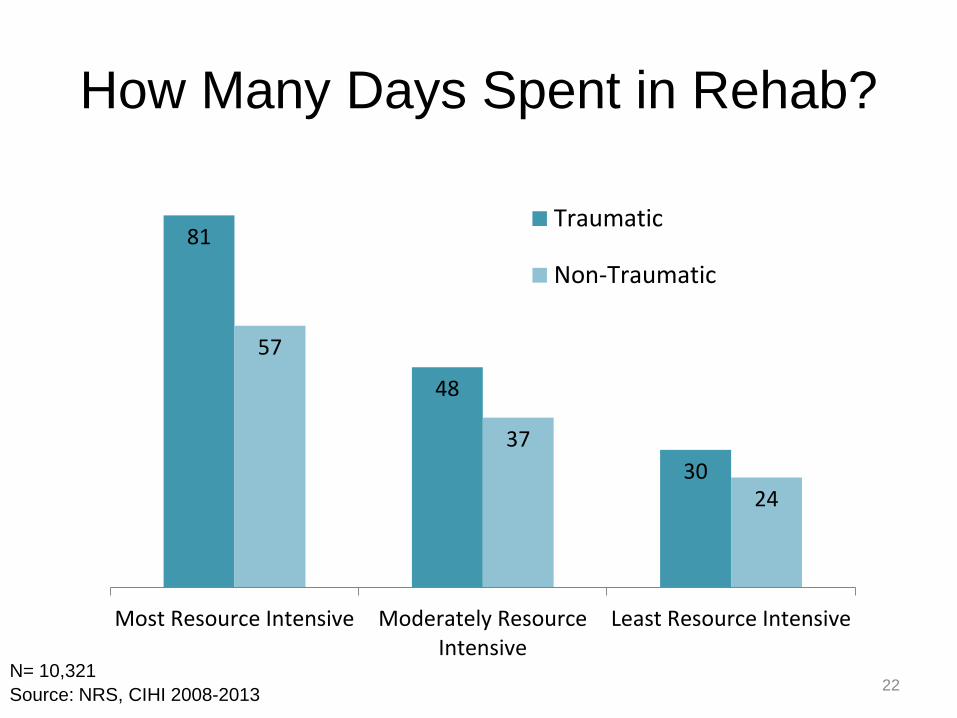
How Many Days Spent in Rehab?
81
48
30
57
37
24
Most Resource Intensive Moderately ResourceIntensive
Least Resource Intensive
Traumatic
Non-Traumatic
22 Source: NRS, CIHI 2008-2013 N= 10,321
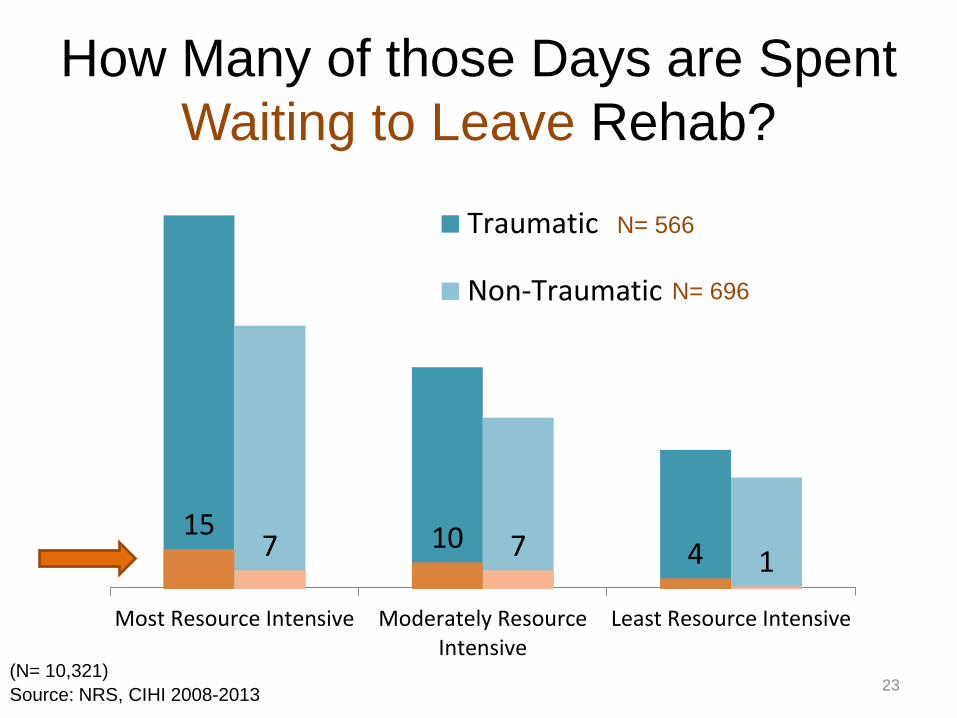
How Many of those Days are Spent Waiting to Leave Rehab?
(N= 10,321)
Most Resource Intensive Moderately ResourceIntensive
Least Resource Intensive
Traumatic
Non-Traumatic
15 10 4 7 7 1
N= 566
N= 696
23 Source: NRS, CIHI 2008-2013
24
25
26
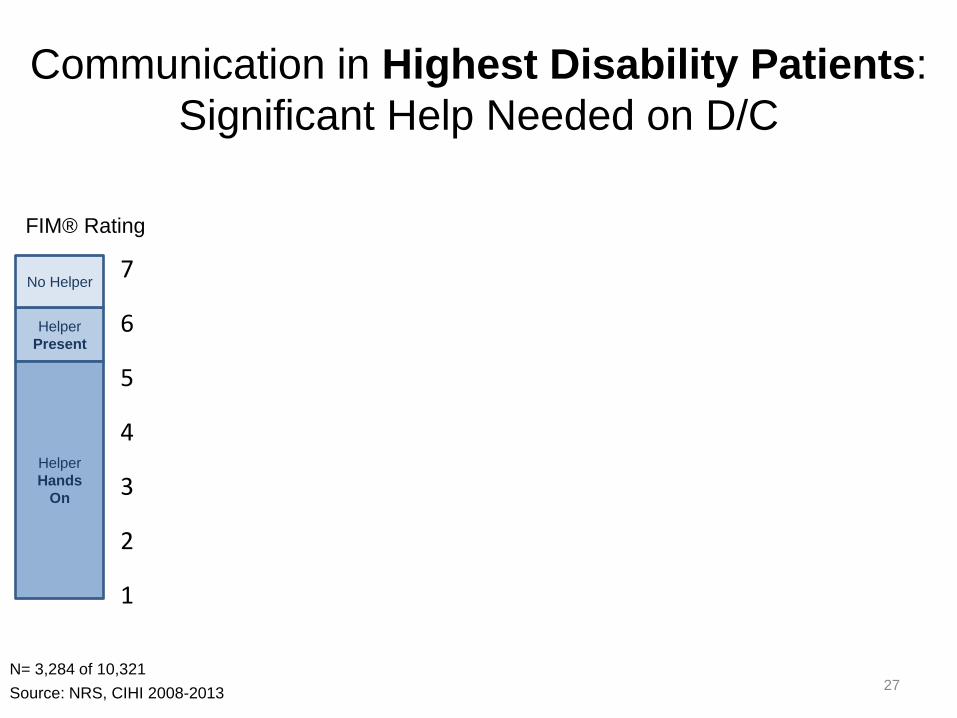
Communication in Highest Disability Patients: Significant Help Needed on D/C
Helper Present
No Helper
Helper Hands
On
FIM® Rating
N= 3,284 of 10,321
Non-Traumatic Traumatic
27 Source: NRS, CIHI 2008-2013
1
2
3
4
5
6
7
Comprehension Expression Comprehension Expression
FunctionChangeAdmissionFunction
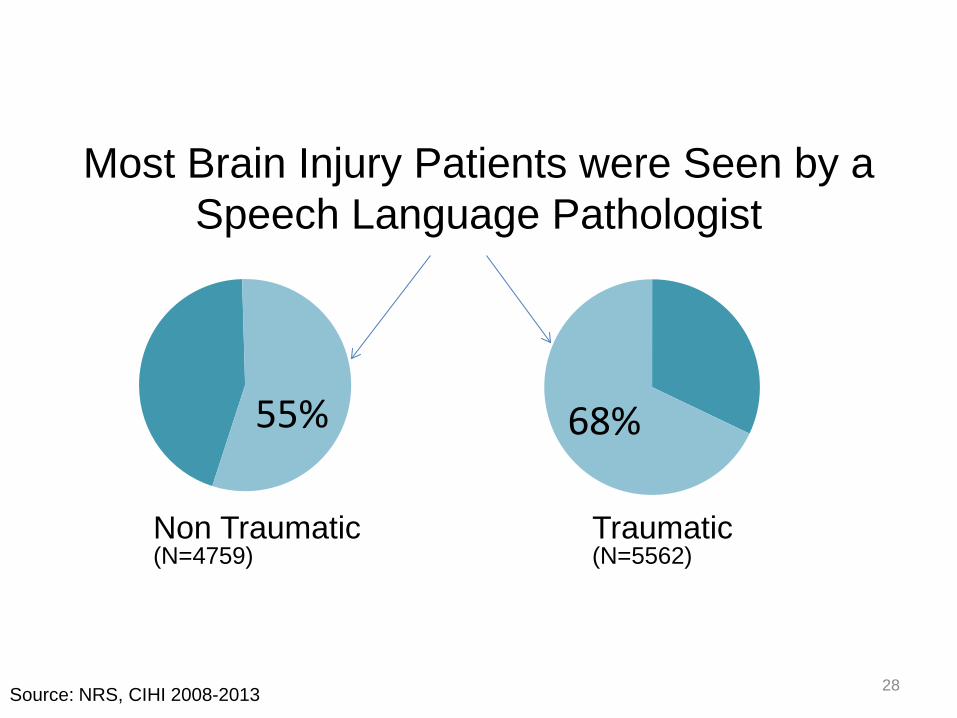
Most Brain Injury Patients were Seen by a Speech Language Pathologist
55% 68%
Non Traumatic Traumatic (N=5562) (N=4759)
28 Source: NRS, CIHI 2008-2013
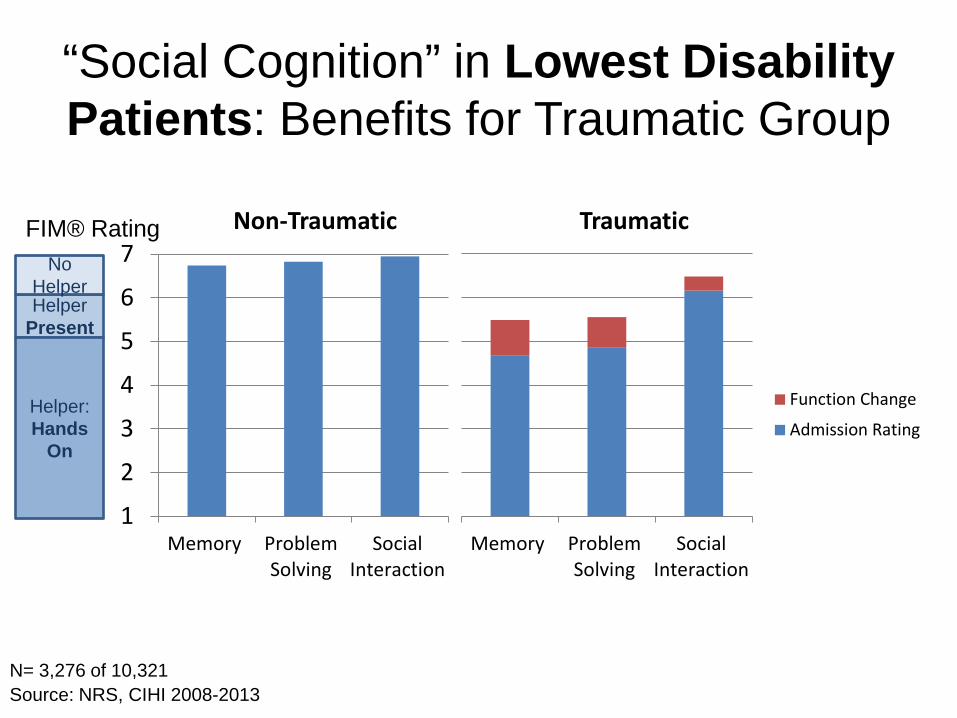
“Social Cognition” in Lowest Disability Patients: Benefits for Traumatic Group
Helper Present
No Helper
Helper: Hands
On
Non-Traumatic Traumatic
1
2
3
4
5
6
7
Memory ProblemSolving
SocialInteraction
Memory ProblemSolving
SocialInteraction
Function Change
Admission Rating
FIM® Rating
N= 3,276 of 10,321 Source: NRS, CIHI 2008-2013
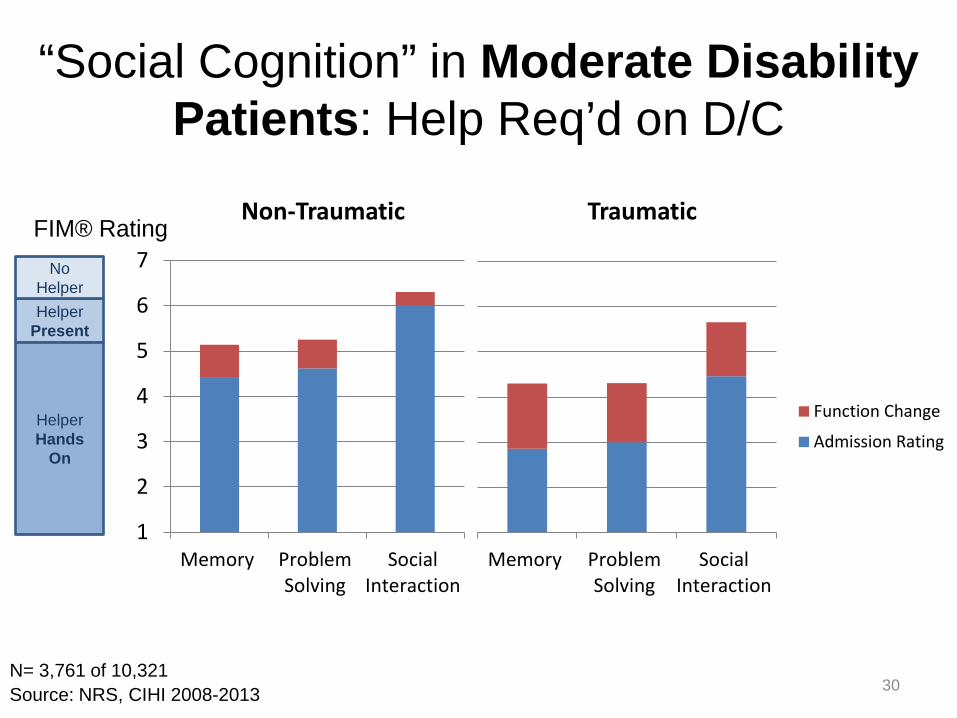
“Social Cognition” in Moderate Disability Patients: Help Req’d on D/C
Helper Present
No Helper
Helper Hands
On
FIM® Rating
N= 3,761 of 10,321
1
2
3
4
5
6
7
Memory ProblemSolving
SocialInteraction
Memory ProblemSolving
SocialInteraction
Function Change
Admission Rating
Non-Traumatic Traumatic
30 Source: NRS, CIHI 2008-2013
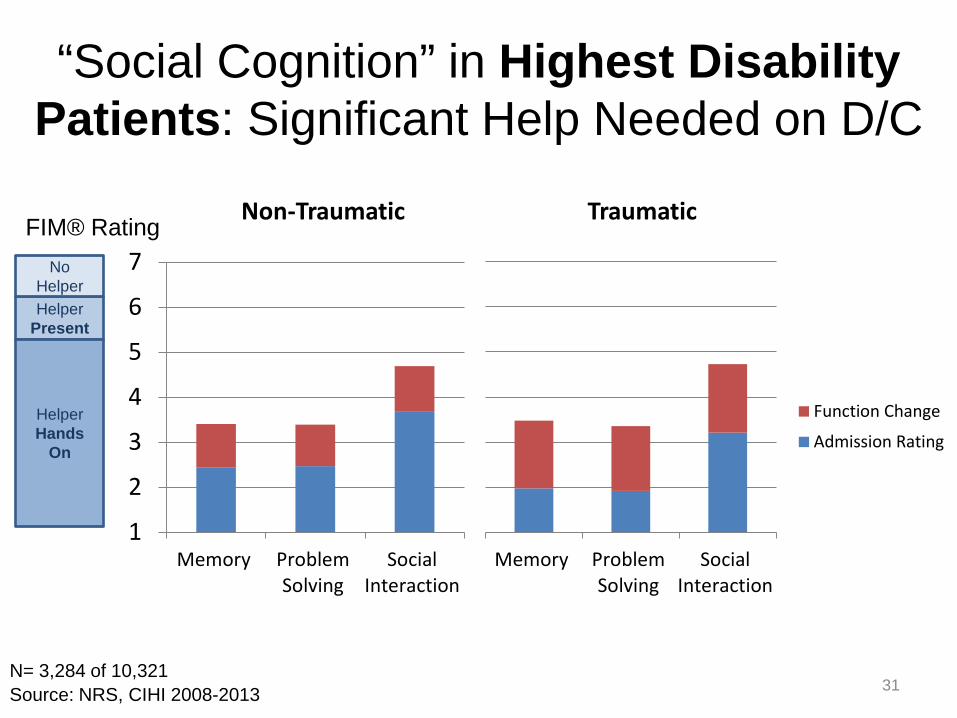
“Social Cognition” in Highest Disability Patients: Significant Help Needed on D/C
Helper Present
No Helper
Helper Hands
On
FIM® Rating
N= 3,284 of 10,321
1
2
3
4
5
6
7
Memory ProblemSolving
SocialInteraction
Memory ProblemSolving
SocialInteraction
Function Change
Admission Rating
Non-Traumatic Traumatic
31 Source: NRS, CIHI 2008-2013
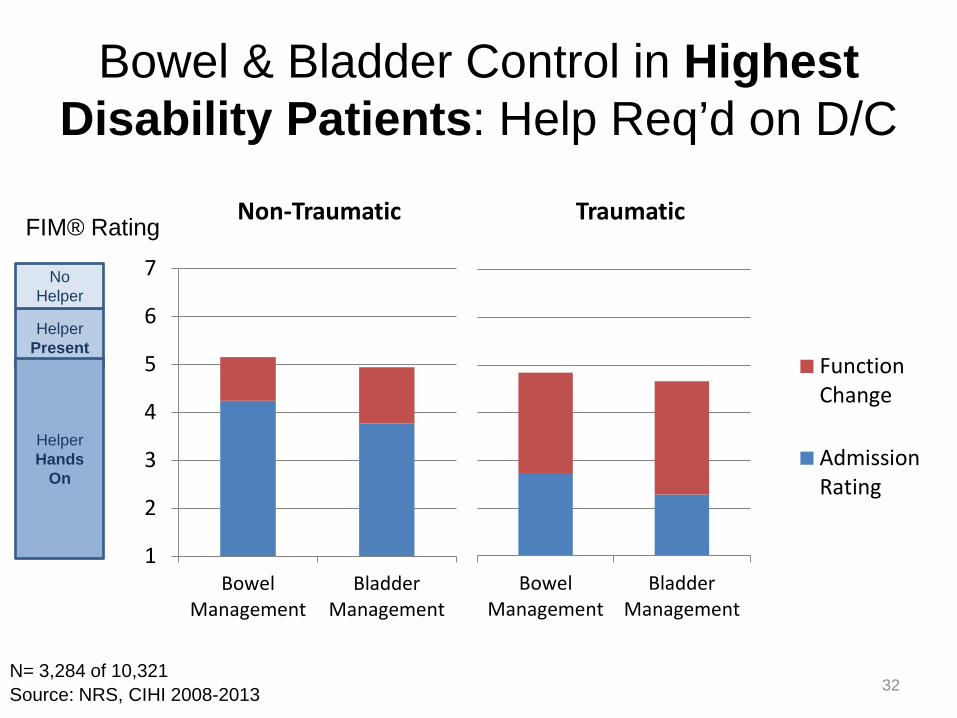
Bowel & Bladder Control in Highest Disability Patients: Help Req’d on D/C
Helper Present
No Helper
Helper Hands
On
FIM® Rating Non-Traumatic Traumatic
1
2
3
4
5
6
7
BowelManagement
BladderManagement
BowelManagement
BladderManagement
FunctionChange
AdmissionRating
32 Source: NRS, CIHI 2008-2013 N= 3,284 of 10,321
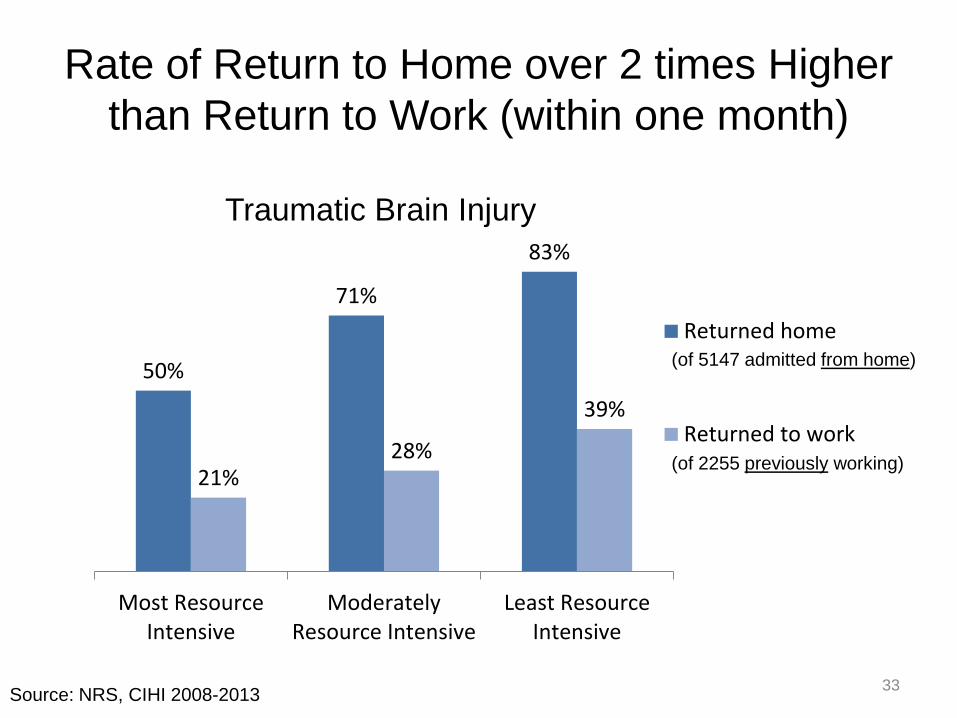
Rate of Return to Home over 2 times Higher than Return to Work (within one month)
50%
71%
83%
21% 28%
39%
Most ResourceIntensive
ModeratelyResource Intensive
Least ResourceIntensive
Returned home
Returned to work
(of 5147 admitted from home)
(of 2255 previously working)
33 Source: NRS, CIHI 2008-2013
Traumatic Brain Injury
Summary of Findings • Inpatient Rehabilitation (IR) admissions for Brain
Dysfunction on the rise • Higher disability, longer time to IR admission and
longer wait once ready for IR discharge • “Depression” is most commonly coded mental
health comorbidity in IR
• On discharge from IR – 2/3 require help with cognitive tasks – 2/3 require significant help/equipment to manage
bladder and/or bowel – Rate of returning home is 2 to 3 times the rate of
returning to work 34
What Lies Around the Bend for Brain Injury Health Information Services
• Enhanced guidelines for ICD-10-CA diagnoses and classification in NRS
• Refinement of case mix grouping methodology in NRS
• Additional outpatient/ambulatory rehab reporting for brain injury
35
You are right here
36
-Pierre Louis Lapointe (2004) Les Editions GID

Let’s spark some interest in rehabilitation data
37
Questions?
38





















![FY 2020 Inpatient Rehabilitation Facility PPS Final Rule ... · Medicare Inpatient Rehabilitation Facility Prospective Payment System for FY 2020 [CMS-1710-F] Summary of Final Rule](https://img.pdfslide.us/doc/110x75/5e152d886e3b54465b2e79a7/fy-2020-inpatient-rehabilitation-facility-pps-final-rule-medicare-inpatient.jpg)