Embed Size (px)
Citation preview

Out-of-pocket health care expenditures due to excess of
body weight in Portugal
Paula Veiga *
Departments of Economics, and NIMA (Applied Microeconomics Research Unit), University of Minho, Portugal
Received 23 November 2006; received in revised form 2 August 2007; accepted 2 August 2007
Abstract
The prevalence for excessive weight has also been increasing dramatically in Portugal over the last
decades. The consequences for families as well as for the publicly funded Portuguese health care system are
a matter of policy interest. This paper uses an econometric model to compute the fraction of the national out-
of-pocket health care expenditures attributable to overweight and obesity among Portuguese adults. Given
that public health care system pays for a substantial share of the national health care expenditures, the
estimated the out-of-pocket expenditures is only a share of the total expenditures. Per-capita expenditures
and the burden that obesity and overweight impose on families are also estimated.
Two waves of the Portuguese National Health Survey (NHS), namely; 1995/1996 and 1998/1999 are
considered. The results suggest that out-of-pocket expenditures due to excess weight have increased sharply
during these 3 years. The two-part model estimates suggest that the obese and overweight are more likely to
incur out-of-pocket health care expenditures but, in the restricted sample of those that incur expenditures,
there is weak or no evidence that the obese or overweight spend, on average, more than those of normal
weight. Overall, it is estimated that in 1995/1996, more than 1.8% out-of-pocket health care expenditures
were attributable to obesity and 2% to overweight (although not statistically significant). The estimated
percentages are over 2.9% for obesity and 4% for overweight in 1998/1999. Combined, the estimated
attributable percentage of national out-of-pocket expenditures due to excess weight was 3.8% in 1995/1996
and 6.9% in 1998/1999. Per-capita expenditures due to obesity or overweight are small, on average, in
absolute terms, but they can be a significant cost for low income families. With respect to public policy
concerns, the results suggest that measures which only slightly increase the out-of-pocket health care
expenditures of being obese (overweight) are likely to be inefficient.
# 2007 Elsevier B.V. All rights reserved.
JEL classification: I19
Keywords: Obesity; Overweight; Out-of-pocket expenditures; Portugal
http://www.elsevier.com/locate/ehb
Economics and Human Biology 6 (2008) 127–142
* Present address: Escola de Economia e Gestao, Campus de Gualtar, 4710 – Braga, Portugal. Tel.: +351 2534549;
fax: +351 253676375.
E-mail address: [email protected].
1570-677X/$ – see front matter # 2007 Elsevier B.V. All rights reserved.
doi:10.1016/j.ehb.2007.08.001

1. Introduction
Excess body weight is becoming one of the most important public health problems also in
Portugal, as is the case in virtually every developed and some undeveloped countries (WHO,
2002). Recent evidence suggests that almost half of the adult population in Portugal is either
overweight or obese (Vidal and Dias, 2005) and the prevalence for excess weight has been
dramatically increasing over the last decades (Castro et al., 1998; Vidal and Dias, 2005). The
problem is even more worrying if one bears in mind that Portuguese children have become
fatter in the last decades and are now among the heaviest children in Europe (Padez et al.,
2004).
Obesity is a disease itself (WHO, 2000), and it is well established that overweight and obesity
are risk factors for several other disorders (Pi-Sunyer, 1991; Must et al., 1999). Excess weight is
also an economic phenomenon. The economic costs, mainly the excess of health care
expenditures, losses of productivity and shorter life expectancy, imposed by obesity and obesity-
related diseases are well documented (Colditz, 1992; Wolfe and Colditz, 1996; Pereira et al.,
1999, 2000). Using relative-risk approach, Colditz (1992) and Wolf and Colditz (1994, 1998)
provide evidence that the aggregate annual obesity-attributable direct medical costs in the U.S.
are between 5 and 7% of the annual health care expenditures. Two papers that use an econometric
approach (Finkelstein et al., 2003, 2004) found markedly similar results. They provide evidence
that the aggregate annual obesity-related medical costs in the United States are between 5.3 and
5.7% of annual adult health care expenditures. Because many obese individuals are covered by
Medicare and Medicaid the government finances roughly half of the total annual medical costs
attributable to obesity (Finkelstein et al., 2003, 2004). Obese (overweight) individuals and their
families bear some of the health care related costs. Sturm (2002) found that American obese
adults aged 18–65 years incur annual medical expenditures that are 36% higher than expenditures
of normal weight individuals. Similarly, Finkelstein et al. (2003) found that the average increase
in out-of-pocket medical expenditures associated with obesity for obese is 26.1%. Overall, the
authors estimate that the aggregate national out-of-pocket medical spending due to excess of
weight is 7.2%.
The aggregate costs of obesity have also been estimated for a number of European countries.
Seidell (1995) estimated that the cost of obesity-related diseases in the Netherlands amounted to
4% of the total Dutch health care costs. Levy et al. (1995) estimated that obesity-related costs
represented approximately 2% of the total health care costs in France.
Pereira et al. (1999) measured the impact of obesity on health care expenditures in Portugal.
Using the relative-risk method they estimated that the total direct health care costs attributable to
obesity were s231 million, 3.5% of the total health care expenditures in Portugal in 1996. Later
(2000) the authors show that direct costs are only part of the economic costs that can be
attributable to obesity since indirect costs are sizeable representing almost half of the total
obesity-attributable costs.
In this paper an econometric approach is taken in order to estimate the fraction of the costs
attributable to obesity and overweight in Portugal. Such method has been widely used in the
literature related to other unhealthy behaviours, such as smoking (Bartlett et al., 1994; Miller
et al., 1998; Zhang et al., 1999; Harrison et al., 2003; Finkelstein et al., 2003, 2004). The
econometric approach avoids important limitations of relative-risk studies. The latter are in the
tradition of the analysis of cost of illness and rely entirely on available clinical and
epidemiological data that causally link obesity and overweight to specific diseases. The
econometric method does not make a priori assumptions as to which medical care conditions lead
P. Veiga / Economics and Human Biology 6 (2008) 127–142128

to more health care costs due to obesity. Moreover, the method better controls for the effects of
determinants other than body weight on health care expenditures. A main virtue of the approach
is that one can use the only representative micro dataset available in Portugal, the National Health
Survey (NHS), to evaluate out-of-pocket expenditures health care and related health variables
with several demographic and socio-economic determinants.
Due to limitations in the available data it is not possible to accurately estimate the national
health care expenditures attributable to obesity in Portugal using our method. Therefore, only
the fraction of out-of-pocket health care expenditures due to obesity and overweight in
Portugal was estimated. Out-of-pocket health care expenditures, although not studied
frequently (Sturm, 2002; Finkelstein et al., 2003) have broad implications for individual
behaviour. The argument is that the individual (family) share of the burden for his/her
unhealthy behaviours and the response to variations on that burden are important variables for
designing incentives and public actions. More than other health conditions, obesity and
overweight are avoidable states and are a consequence of personal choices. Economic theory
claims that individuals may rationally decide to become (or stay) obese (overweight) if the
utility they get from behaviours leading to obesity (overweight) is higher than the costs they
have to bear, conditional to the information available to them. Decisions about body weight
can only be optimal (in a clinical sense), in the absence of government policies, if the
individuals know and face the full costs of their decisions (Bhattacharya and Sood, 2007) and
are able to discount the future disutility properly (Kolmos et al., 2004). There is no doubt that
this is not the case in Portugal, where the majority of the health care costs are passed on to the
society through a generous public insurance. The Portuguese health care system is based on a
universal health system, general in health care provision and (ideally) almost free at point of
usage. Although the system has not accomplished some of its goals, health care is still highly
publicly subsidised. The Portuguese public health system is particularly generous with
chronic diseases such as those related to obesity. Therefore, the excess of national health care
costs due to excess weight is likely to be more than proportional to the excess of out-of-
pocket costs.
Roux and Donaldson (2004) argue that studies on obesity should go far beyond measuring
costs and should perform cost-benefit analysis of different strategies in preventing and treating
obesity. Some of the arguments raised by Roux and Donaldson (2004) are valid and there is a
consensus in the literature, on the importance of the cost-benefit analysis (as well as on their
limitations) for policy decisions. Nonetheless, cost studies are still important. They are a crucial
step in cost-benefit analysis, a helpful tool to promote the awareness of the dimension of the
epidemic, as well as an important instrument to forecast costs and therefore to design prevention
policies. In addition, cost studies may be useful to clarify the debate on the personal and societal
share of health care costs, and is one of the purposes of this study.
2. Methods
2.1. Econometric method
In order to estimate the obesity (overweight)-attributable fraction a counter-factual
simulation of a statistical model was undertaken. Assume that one has estimated an equation
for expected health care expenditures that controls for the Body Mass Index (BMI) classes
and for other different characteristics that are thought to affect individual health care
expenditures. To estimate the obesity (overweight)-attributable fraction, the first step is to
P. Veiga / Economics and Human Biology 6 (2008) 127–142 129

predict the out-of-pocket expenditures, given the observed BMI class of the individual
(EXPA). The second step is to assume that the individual is not-obese (not-overweight), and
then re-evaluate the equation (EXPNA). Therefore, EXPNA represents the expected
expenditure of the individual if he were not-obese (not-overweight), holding all other
factors constant. Individual obesity (overweight)-attributable fraction is then calculated as the
excess of expenditure due to obesity (overweight) divided by the actual expenses, that is
attributable fraction = (EXPA � EXPNA)/EXPA. Obesity (overweight)-attributable fraction
for a not-obese (not-overweight) person is zero by construction. Estimation of the
aggregate obesity (overweight)-attributable fraction is as follows: each individual obesity
(overweight)-attributable fraction is multiplied by actual out-of-pocket health care
expenditures and then summed. Aggregate obesity (overweight)-attributable fraction is
then given by the ratio of this sum and the total of all individual’s health out-of-pocket health
care expenses.
2.2. Statistical model
EXPA and EXPNA are estimated by a two-part model, which has been widely applied
elsewhere (Coller et al., 2002; Harrison et al., 2003). The model can be represented as follows:
� Observed expenditure: y = dy**
� Participation equation: w ¼ a0Z þ v, d = 1 if w> 0;¼ 0 otherwise
� Expenditure equation: y** = max [0, y*], y* = b0X + u.
The participation equation determines the probability that a person would incur an out-of-
pocket expense and it is estimated using a probit model. The expenditure equation determines the
level of out-of-pocket costs and is estimated by ordinary least squares (OLS) on a logarithmic
transformation of the variable, on the conditional sample of people who report an out-of-pocket
expenditure. The inclusion, in both equations, of dichotomous variables indicating an
individual’s BMI category allows us to predict the impact of obesity (overweight) on out-of-
pocket health care expenditures.
Once the equations are estimated they are used to predict the probability that the individual
has expenses (PA), the probability that the individual would have expenses if he is not-obese (not-
overweight), everything else constant (PNA), and the level of expenses in the two cases (UA,
UNA). Then the prediction EXPA = PA �UA and EXPNA = PNA �UNA is estimated. Next, steps
described in Section 2.1 are followed to estimate the individual and the aggregate fraction. The
final step is to multiply the estimated obesity (overweight)-attributable fraction by the national
out-of-pocket health care expenditures in order to obtain the total out-of-pocket expenditures
caused by obesity.
The method is used to determine obesity (overweight)-attributable fraction considering the
predicted total expenditures of the full sample and considering the predicted expenditures for the
obese (overweight) samples. The second type of estimates gives the fraction of out-of-pocket
health care expenditures of obese (overweight) that are attributable to the obesity (overweight)
condition. In addition, the individual obesity (overweight)-attributable fraction is used to
calculate the additional costs for the obese (overweight) people in the sample. This result is then
divided by the per-capita family net income to get the relative cost of obesity (overweight).
Estimations were carried out using STATA 8. All regressions include controls for sex, age,
region, per-capita family income, years of schooling, marital status, and employment status, type
P. Veiga / Economics and Human Biology 6 (2008) 127–142130

of health insurance, tobacco consumption and alcohol consumption. Standard errors for the
aggregate estimates are computed via bootstrap method.
2.3. Data
The individual data used in this paper are from the two waves of NHS collected in 1995/1996
and 1998/1999. NHS is a representative survey of household residents in mainland Portugal.
NHS asked adult households (members older than 18) about the out-of-pocket health care
expenditures that had been incurred in the 2 weeks before the interview. The individuals also
reported their weight and height. It has been suggested that excess weight people tend to
underreport their weight (Flegal et al., 2002). There is a similar concern for the self-report on
height. As a result obesity/overweight prevalence and the estimate out-of-pocket health care
expenditures fraction attributable to obesity/overweight fraction may be underestimated.
Therefore, reporting errors have been corrected following Cawley and Burkhauser (in press).
The authors use data from the American National Health and Nutrition Examination Survey III
which contains both self-reported and measured data and provide prediction equations to correct
for self-reporting bias. Table 1 shows the difference this correction makes to average BMI
estimates.
In addition, the NHS questionnaire included other questions on demographic and socio-
economic conditions, health status, health risks and health care use. Observations with missing
information on weight or/and height variables were excluded. The missing values for ‘‘family net
monthly income level’’ and for ‘‘years of schooling’’ in the data are high, and affect
disproportionately the obese sample. To reduce the potential bias, ‘‘family net monthly income’’
and ‘‘years of schooling’’ variables were imputed, using the impute command in STATA 8 (2003)
which uses regression equations to fill in missing values. The final sample includes 38332 in
1995/1996 and 22831 observations in 1998/1999.
Data for the national health care costs came from the OECD. In 1995, the total health care
expenditure, in Portugal, amounted to s6707 million, approximately 8.3% of the GDP (OECD,
2002). Out-of-pocket expenditures were approximately 32% of the total health care expenditures
(OECD, 2002; WHO, 2006), i.e., s2141 million. In 1999, the total health care expenditure
amounted to s9042 million, approximately 8.4% of the GDP (OECD, 2002). Out-of-pocket
expenditures were approximately 27.8% (OECD, 2002; WHO, 2006) of the total and thus
reached s2508 million.
2.4. Definitions
BMI is calculated as weight in kilograms divided by the squared height in meters. We use the
World Health Organization’s definitions of overweight and obesity. Underweight was defined as
BMI < 18.5, normal weight as BMI � 18.5 and<25.0, overweight as BMI � 25.0 and<30, and
obesity as BMI � 30. A dichotomous variable was created for each weight group variable equal
P. Veiga / Economics and Human Biology 6 (2008) 127–142 131
Table 1
Average self-reported BMI and corrected BMI (standard deviation)
Self-reported Corrected
1995/1996 25.217 (4.022) 25.388 (4.166)
1998/1999 25.824 (4.247) 26.097 (4.444)

to 1 if the individual BMI is within the respective interval and 0 otherwise. Additionally, we
created dummy variables for different levels of obesity, as they tend to be associated with
different and increasingly grave clinical conditions: obesity type I (30 � BMI < 35), obesity
type II (35 � BMI < 40) and obesity type III (BMI � 40).
3. Results
3.1. Descriptive variables
After correcting for reporting errors, the NHS data indicate that more than half of the
Portuguese adults have excess weight. Moreover, the rates of obesity and overweight have
increased dramatically, from 1995/1996 to 1998/1999 (Table 2). An alarming trend was
identified in the increase of incidence of obesity type III which almost doubled during the period.
The gender gap has decreased between waves.
Definitions and descriptive statistics for variables are presented in Table 3. In comparison to
normal weight people, the obese and overweight tend to be older, have higher incidence of
chronic diseases, be less educated, and more likely to belong to lower income families (Table 3).
There is a similar age pattern for the obese and overweight. Data limitations do not allow us to
separate cohort effects from the life cycle pattern effects. The observable incidence of obesity for
age groups is a mix of both effects. In 1998/1999 almost 21% of adults younger than 30 years old
were overweight. The percentage of overweight increases with age and reaches 45% among
people in their 60’s. The percentage of obese people is 5.6% among younger adults, and more
than 21% among people in their 50’s.
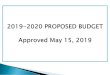
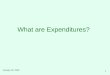
Fig. 1 illustrates the income related inequality in obesity prevalence, favouring the richest
group. In 1995/1996 overweight affects disproportionately the lower income groups. On the other
hand, in 1998/1999 sample overweight does not appear to have a clear income pattern (Fig. 2).
P. Veiga / Economics and Human Biology 6 (2008) 127–142132
Table 2
Percentage of obese and overweight, persons 18 years of age and older
All 1995/1996 1998/1999 Increase (%)
Obesity 12.7 17.3 36.2
Obesity I 10.3 13.8 34.0
Obesity II 2.0 2.8 40.0
Obesity III 0.4 0.7 75.0
Overweight 36.5 38.9 6.6
Males
Obesity 9.6 13.2 37.5
Obesity I 8.3 11.5 38.6
Obesity II 1.0 1.4 40
Obesity III 0.1 0.3 200
Overweight 39.7 44.1 11.1
Females
Obesity 15.5 19.7 27.1
Obesity I 12.1 15.2 25.6
Obesity II 2.8 3.6 28.6
Obesity III 0.7 1.0 42.9
Overweight 33.8 35.8 5.9

P.
Veig
a/E
con
om
icsa
nd
Hu
ma
nB
iolo
gy
6(2
00
8)
12
7–
14
21
33
Table 3
Descriptive statistics (mean (standard deviation))
Variables Description 1995/1996 1998/1999
Normal Overweight Obese Normal Overweight Obese
Probability Probability of an expenditure 0.254 (0.435) 0.293 (0.455) 0.369 (0.482) 0.359 (0.480) 0.406 (0.491) 0.457 (0.498)
Expenditure Expenditure 966.453
(3066.581)
953.912
(2767.170)
859.56
(1907.070)
1288.476
(4124.555)
1192.362
(2582.440)
1129.678
(2008.036)
Marrieda Married = 1 0.598 0.759 0.767 0.663 0.774 0.743
Yrs school Years of schooling 6.492 (4.182) 5.159 (3.351) 4.397 (2.767) 7.280 (4.400) 5.327 (3.510) 4.622 (3.013)
Joba Worked in last 2 weeks = 1 0.537 0.520 0.491 0.494 0.459 0.38
Malea Male = 1 0.479 0.509 0.477 0.373 0.740 0.284
Chronica Has a chronic disease = 1 0.474 0.607 0.743 0.612 0.734 0.818
18–29a Age 18–29 = 1 0.291 0.110 0.048 0.193 0.066 0.046
30–39a Age 30–39 = 1 0.173 0.151 0.108 0.182 0.130 0.097
40–49a Age 40–49 = 1 0.146 0.191 0.190 0.161 0.180 0.168
50–59a Age 50–59 = 1 0.123 0.196 0.233 0.135 0.190 0.231
60–69a Age 60–69 = 1 0.125 0.187 0.238 0.150 0.230 0.242
70–79a Age 70–79 = 1 0.094 0.123 0.136 0.127 0.160 0.174
�80a Age �80 = 1 0.045 0.040 0.048 0.050 0.040 0.040
Northa Lives in North = 1 0.305 0.283 0.248 0.277 0.278 0.255
Centera Lives in Center = 1 0.198 0.201 0.195 0.207 0.220 0.201
LVTa Lives in Lisbon
and Tejo Valley = 1
0.263 0.282 0.316 0.265 0.273 0.295
Alentejoa Lives in Alentejo = 1 0.118 0.125 0.151 0.132 0.128 0.153
Algarvea Lives Algarve = 1 0.111 0.109 0.091 0.118 0.105 0.094
Cigsnow Number of cigarette smokes daily 1.848 (7.387) 2.995 (8.588) 1.774 (7.274) 3.652 (8.685) 2.330 (7.360) 1.323 (5.772)
Cigspast Number of cigarette smoked in past. 4.170 (9.400) 3.149 (10.184) 2.994 (10.320) 2.447 (8.728) 3.710 (11.061) 3.376 (11.387)
Private Insurancea Has private insurance = 1 0.046 0.042 0.156 0.061 0.040 0.032
SNSa Uses NHS = 1 0.844 0. 864 0.881 0.828 0.840 0.867
ADSEa Uses ADSE = 1 0.086 0.071 0.060 0.115 0.090 0.078
Incapacitya Has a temporary incapacity = 1 0.085 0.096 0.129 0.136 0.160 0.177
Alcohol Average amount of alcohol drunk per week 0.148 (0.296) 0.181 (0.317) 0.144 (0.282) 0.202 (0.317) 0.220 (0.297) 0.177 (0.283)
aDummy variable equal to zero, otherwise, bdata for underweight group is not reported because it is irrelevant for this study.

Nonetheless, it is still having a higher incidence among the middle income class. No gender
differences were found.
3.2. Two-steps model estimates
Table 4 presents the two-step estimated obesity and overweight coefficients and reports the
results of an F-test on the hypothesis that coefficients are jointly zero. The model has a low
P. Veiga / Economics and Human Biology 6 (2008) 127–142134
Fig. 1.
Fig. 2.

explanatory power (low R2), which suggests that out-of-pocket health care expenditures are
determined by complex relations and often non-observable variables.
The results offer convincing evidence that excess weight has an impact on out-of-pocket
expenditures mainly because the obese and overweight are more likely to incur out-of-pocket
health care expenditures than people of normal weight. According to the marginal probability
estimates, in 1995/1996, obesity increases the probability of having an out-of-pocket health care
expense by 4.9 percentage points and overweight by 1.5 percentage points when compared with
normal weight. The hypothesis that both coefficients are equal to zero is rejected, at the
conventional levels of confidence. On the other hand, there is no evidence that excess weight in
1995/1996 was associated with the amount of out-of-pocket expenditures, given that individuals
have made an expenditure, because the coefficients are close to zero and insignificant. In other
words, the out-of-pocket expenditures of those with excess of weight were the same of those with
normal weight, but the former incurred those expenses more frequently. The odds of having out-
of-pocket expenditures are remarkably stable for the obese from 1995/1996 to 1998/1999, but
almost double in the case of the overweight. In the latter period, the obese were 5.1 percentage
points more likely to have an out-of-pocket health care expenditure when compared with persons
of normal weight. The overweight was 2.8 percentage points more likely. In contrast to the earlier
period the estimated coefficients of the expenditure equation suggest that obese and overweight
persons did spend more on health care, when compared with those of normal weight who also
incurred out-of-pocket expenditures.1
To characterise the relationship between excess weight and out-of-pocket expenditures more
fully, the model was re-estimated including the dummy variables for different types of obesity,
rather than only one dummy for obesity. In both, 1995/1996 and 1998/1999, the evidence
suggests that obese type I and obese type II are more likely to have incurred out-of-pocket
expenditures than people of normal weight. For the obese type III the estimate coefficient is
positive but not statistically significant in 1995/1996, and is barely significant in 1998/1999
(Table 5). There are at least two possible explanations for this result. First, medical literature
suggests that obese type III are more likely to suffer from chronic diseases, and therefore likely to
P. Veiga / Economics and Human Biology 6 (2008) 127–142 135
Table 4
Two-part model—probit and OLS estimates (standard error)
1995/1996 1998/1999
Probability of
an expenditurea
Log of
expenditure
Probability of
an expenditurea
Log of
expenditure
Obesity 0.049*** (0.008) 0.000 (0.032) 0.051*** (0.010) 0.070** (0.032)
Overweight 0.015*** (0.005) 0.006 (0.025) 0.028*** (0.007) 0.047* (0.028)
F-test Ch2 = 41.75 P = 0.00 Ch2 = 0.04 P = 0.96 Ch2 = 29.43 P = 0.00 Ch2 = 2.70 P = 0.06
R-squared (Pseudo) (0.101) 0.039 (0.096) 0.051
Regressions controlled for the following variables: married, yrs school, job, male, age group (18–29 omitted), income
group, regions (North omitted), Cigsnow, Cigspast, Private Insurance, SNS, ADSE, Incapacity and Alcohol. *Statistically
significant at 10%; **statistically significant at 5%; *** statistically significant at 1%.a Results reported are marginal effects from probit using dprobit command in Stata.
1 When the model includes variables thought to be related to overweight, such as the presence of chronic diseases or
permanent incapacity, the estimated relation between overweight and positive health care expenditures, is still positive
but no longer significant (results not reported).

benefit from a more generous health care public insurance. Second, they may indeed tend to be
less likely to have out-of-pocket health care expenditure because they may tend to be less health
conscious and therefore less likely to demand health care.
The results confirm that obesity in 1995/1996, no matter how severe, does not appear to be
linked to the amount of out-of-pocket health care expenditures, given that individuals did have
expenditures. The results are mixed for 1998/1999: only obese type I and III individuals tend, on
average, to spend more than normal weight people who also incurred expenditures.
3.3. Aggregate obesity and overweight-attributable fraction of expenditures
Once the regression equations are estimated one can infer the value of obesity and overweight-
attributable fraction of out-of-pocket expenditures. These are presented, in percentage, in
Table 6. Table 6 also reports the estimated contribution of each type of obesity for the total
obesity-attributable fraction. Differences in obesity-attributable fraction, by obesity type, reflect
mainly the differences in prevalence.
Estimates for 1995/1996 suggest that 1.84% of the national out-of-pocket expenditures are
attributable to obesity and 1.98% to overweight. Nonetheless, the bootstrap exercise indicates
that the estimated coefficient on overweight is not statistically significant at the conventional
levels. In the 1998/1999 wave almost 2.9% of the total out-of-pocket national expenditures can
be attributable to obesity. In addition, overweight is responsible for 4% of the total out-of-pocket
health costs. Therefore, the costs of excess weight represent approximately 6.9% of total out-of-
pocket expenditures, compared to 3.8% in 1995.
3.4. Individual obesity and overweight-attributable fraction
Table 7 shows the obesity (overweight)-attributable fraction for those who were obese
(overweight).2
P. Veiga / Economics and Human Biology 6 (2008) 127–142136
Table 5
Two-part model: probit and OLS estimates (standard error)
1995/1996 1998/1999
Probability of
an expenditurea
Log of
expenditure
Probability of
an expenditurea
Log of
expenditure
Obesity I 0.045*** (0.008) �0.024 (0.035) 0.046*** (0.011) 0.067* (0.034)
Obesity II 0.073*** (0.018) 0.094 (0.060) 0.076*** (0.022) 0.044 (0.060)
Obesity III 0.036 (0.037) 0.100 (0.112) 0.075* (0.041) 0.217** (0.096)
F-test Ch2 = 41.75 P = 0.000 Ch2 = 0.04 P = 0.96 Ch2 = 28.76 P = 0.000 Ch2 = 2.60 P = 0.050
Obesity type I (30 � BMI < 35), obesity type II (35 � BMI < 40) and obesity type III (BMI � 40). Regressions
controlled for the following variables: married, yrs school job, male, age group (18–29 omitted), Income group, regions
(North omitted), Cigsnow, Cigspast, Private Insurance, SNS, ADSE, Incapacity and Alcohol. *Statistically significant at
10%; **statistically significant at 5%; ***statistically significant at 1%.a Results reported are marginal effects from probit using dprobit command in Stata.
2 The estimates should be interpreted as the fraction attributable to obesity (overweight) and obesity (overweight)
related health problems on the out-of-pocket expenditures of obese (overweight) individuals themselves.

Obesity-related expenditures represent about 12.3% of out-of-pocket health care expenditures
in 1995/1996, for obese individuals. Obese type II persons face a higher burden. The estimated
share of the overweight on the individual’s out-of-pocket expenditures is smaller and is not
statistically significant. In 1998/1999 excess of weight related health care expenditures
represented 15.5% of the out-of-pocket health expenses for the obese and 10.3% for the
overweight. The estimated attributable fraction increased with increasing gravity according to
obesity type. For obese type III excess weight accounts for almost 30% of their total out-of-
pocket expenditures.
3.5. Individual excess of out-of-pocket costs due to obesity and overweight
Individual obesity (overweight)-attributable fraction was applied to out-of-pocket costs
reported in NHS to obtain the individual additional expenditure due to obesity (overweight) in the
sample. Then, the relative burden that the additional costs impose on individuals and their
families was estimated. Estimates are restricted to 1998/1999 NHS because income variable is
not fully comparable among waves. In 1995/1996 survey the individuals’ self-reported family
gross income, while in 1998/1999 self-reported the net income.
In the 1998/1999 NHS wave, the monthly net income earned by the families includes all
sources of income and is measured as a categorical variable. A midpoint of each income group
was attributed to all families in the category and divided by the number of family members.
Annual per-capita income was obtained by multiplying monthly per-capita income by 14.3 Then
we create a new variable that indicates which per-capita income decile a family belongs to.
In 1998/1999, an adult obese spend annually, on average, s80 more than not-obese. This
additional expenditure corresponds roughly to 3.1% of their annual per-capita family net income.
Overweight individuals on average spend approximately s50 on related health care costs, which
P. Veiga / Economics and Human Biology 6 (2008) 127–142 137
Table 6
Estimated obesity (overweight)-attributable fraction
Attributable
fraction
Bootstrap estimate of
the standard error (1000 iterations)
95% Confidence interval
(bias corrected)
1995/1996
Obesity 1.84 0.54 0.82–2.94
Obesity I 1.09 0.46 0.15–1.95
Obesity II 0.68 0.22 0.30–1.19
Obesity III 0.08 0.06 �0.03–0.20
Overweight 1.98 1.14 �0.13–4.21
1998/1999
Obesity 2.89 0.67 1.66–4.38
Obesity I 2.11 0.57 1.02–3.32
Obesity II 0.51 0.22 0.11–0.98
Obesity III 0.26 0.10 0.08–0.49
Overweight 4.04 1.19 1.66–6.34
Whole sample.
3 It is assumed that to estimate the annual income, the reported monthly income should be multiplied by 14 months
because in Portugal, workers and retirees receive an additional salary and pension payment in both June and December.

roughly corresponds to 1.8% of their annual family per-capita net income. The estimated excess
of out-of-pocket health care expenditures, due to obesity, as percentage of the family per-capita
income, ranges from 1.4% in the highest income decile group to 7.5% in the lowest income decile
group. Obese Type III spend on average s173 more than normal weight individuals, which
corresponds to 6.7% of their family per-capita net income. The estimated excess of expenditures
ranges from 3.4% of per-capita income for the highest income decile group to 13.2% in the lowest
income decile group. For overweight group, the excess of health care expenditures represents
around 4.3% of the total per-capita family income in the lowest income group and 0.8% in the
highest group.
The results suggest that for individuals from low income families, in particular for obese type
III individuals, the additional out-of-pocket health care expenditures due to excess of weight may
represent an important share of their net income. Nonetheless, for individuals from high income
families the impact of additional costs tends to be relatively small. Still, the higher prevalence of
obese (overweight) among low income individuals suggests that the actual relative health care
costs do not influence this group. Upper income group are even less affected. Thus, the results
suggest that small variations in private co-payments for health care will not be effective in
decreasing obesity prevalence.
3.6. Obesity and overweight-attributable national out-of-pocket costs
Once the aggregate obesity and overweight-attributable fractions are estimated, the implied
expenditures are calculated Table 8 shows the estimated total out-of-pocket costs attributable to
obesity and overweight. The estimated costs are the maximum amounts that could be saved by
individuals if excess weight were eradicated. Weight loss cannot instantly reverse all the
consequences of the excess weight, and therefore will not imply that all health care costs would
vanish. Nonetheless, the evidence provided here suggests that Portuguese families would save a
sizeable amount in avoidable out-of-pocket health care costs, if they do not become obese
(overweight). The combined annual obesity and overweight-attributable out-of-pocket
expenditures are estimated to be s72 million in 1995/1996 and s174 million in 1998/1999.
P. Veiga / Economics and Human Biology 6 (2008) 127–142138
Table 7
Estimated obesity (overweight)-attributable fraction
Attributable
fraction
Bootstrap estimate of
the standard error (1000 iterations)
95% Confidence interval
(bias corrected)
1995/1996
Obesity 12.27 3.23 5.84–18.32
Obesity I 9.34 3.65 1.21–15.58
Obesity II 23.80 5.47 11.39–33.61
Obesity III 17.46 11.74 �9.38–35.51
Overweight 5.19 2.92 �0.40–10.68
1998/1999
Obesity 15.55 3.18 9.57–21.61
Obesity I 14.48 3.50 7.48–21.27
Obesity II 16.17 5.91 3.53–26.76
Obesity III 29.89 8.90 11.19–45.18
Overweight 10.28 2.82 4.30–15.40
Restricted sample of obese (overweight).

The increase these care expenditures attributable to obesity (60% in real terms) and
overweight (108% in real terms) from 1995/1996 to 1998/1999 result from the increase of
prevalence, as well as the increased impact of excess weight on expenditures.4 The results stress
the importance of taking overweight into account in economic policy. Although, at the individual
level, the obesity costs are substantially higher than the overweight costs the aggregate pattern
due to higher prevalence of overweight, suggests that overweight is a somewhat larger economic
problem for Portuguese families. Moreover, the burden due to overweight increased more over
the period considered.
3.7. Obesity and overweight-attributable health national expenditures
Let us assume that the share of obesity and overweight-attributable fractions of total
expenditures is comparable to the fractions estimated above for the out-of-pocket costs. The
values in Table 9 were calculated by multiplying the estimated obesity (overweight)-
attributable fraction for out-of-pocket costs by the actual total national health care costs. The
results confirm that excess weight is indeed a serious economic problem that is dramatically
increasing.
P. Veiga / Economics and Human Biology 6 (2008) 127–142 139
Table 8
Out-of-pocket health care expenditures attributable to obesity and overweight prevalence in Portugal
Total
(million euros)
Bootstrap estimate of
the standard error (1000 iterations)
95% Confidence interval
(bias corrected)
1995/1996
Obesity 39.49 11.46 17.50–62.91
Overweight 42.36 24.44 �2.87–90.19
1998/1999
Obesity 72.46 17.02 41.68–109.86
Overweight 101.44 29.79 41.64–159.22
Table 9
Portuguese health care expenditures attributable to obesity and overweight prevalence in Portugal using the estimated out-
of-pocket attributable fractions
Total
(million euros)
Bootstrap estimate of the
standard error (1000 iterations)
95% Confidence interval
(bias corrected)
1995/1996
Obesity 123.72 35.90 54.81–197.09
Overweight 132.69 76.58 �8.98–282.52
1998/1999
Obesity 261.23 61.36 150.28–396.06
Overweight 365.70 107.41 150.11–574.02
4 GDP deflator. Source: International Monetary Fund, World Bank database, September 1995.

4. Conclusions
Excess weight prevalence has risen substantially in Portugal from 1995 to 1999, and already
affects more than half of the adult population. The above analysis suggests that excess weight
affects out-of-pocket health care expenditures. This is the result of both an increase in the
prevalence and an increase in the excess of health care costs by obese (overweight) individuals
among all socio-economic groups. The direct health care costs of excess weight represent
approximately 3.8% of national out-pocket expenditures in 1995 and 6.9% in 1999 (Table 5).
Unless prevalence can be reduced the direct out-of-pocket costs of overweight and obesity will
continue to increase. Moreover, the results indicate that at the aggregate level, due to the higher
prevalence, overweight is an even a more important health care cost problem than obesity for the
Portuguese families.
There is an argument that there is an externality associated with excess weight. Although the
present study does not estimate an exact amount, it provides evidence that public health care costs
due to obesity (overweight) are substantial, and a decrease in excess weight would result in
sizeable health care costs savings. Therefore, there are clear economic motivations for the
governments to consider strategies aimed to reduce the prevalence of these conditions.
The evidence provided here suggests that the individual relative health care costs of obesity
are not a main determinant of obesity (overweight) prevalence. Hence, small variations on private
co-payment for health care services are likely to be ineffective in reducing the costs, borne by
society of treating obese (overweight) related diseases. Perhaps a significant increase in the
individual’s share of the health care costs of obesity (overweight) would contribute to changing
behaviours. It would be a policy difficult to implement. In addition to being difficult to
appropriately measure the role of obesity or overweight on diseases, a significant increase in out-
of-pocket expenditures to the obese/overweight could raise ethical concerns and have
distributional effects that may be undesirable from a societal point of view.
The design of alternative public policies is also a difficult task. It has been claimed that
technological changes are the main determinant for the recent increase of obesity (overweight)
prevalence, because it has both lowered the price of calories and raised the cost of expending
calories (Philipson et al., 2003). Nonetheless, the evidence suggests that taxes are likely to be
ineffective in changing patterns of consumption and have little impact on diet quality or heath
outcomes (Kuchler et al., 2005). It should be noted that this type of policies has only a limited
effect on changing other unhealthy behaviours such as smoking (Chaloupka and Warner, 2000).
Another often recommended policy is to promote education about the benefits of diets and
exercise. A main argument is that people do not accurately account for the economic and
intangible costs that excess of weight impose on themselves. Nonetheless, the marginal value of
more information casts doubts: there is evidence that public knowledge has been increasing
whilst obesity is also rising.
Programs to lower the time preference of individuals may contribute since time preference and
obesity appear to be positively related (Kolmos et al., 2004). Incentives to physical activity such
as promotion of school sports, subsidising health club memberships and the purchase of exercise
equipment, as well as more adequate transportation and urban policies may also be helpful.
Our analysis has several limitations. Cawley and Burkhauser (in press) method of correction
for self-reported bias assumes that the relation between measured and self-reported height and
weight is the same in NHANESII and NHS. National health care values include the health care
costs from Azores and Madeira in addition to the continental health care costs. Madeira and
Azores are not included in the NHS. However, there are no reasons to believe that the estimated
P. Veiga / Economics and Human Biology 6 (2008) 127–142140

continental obesity (overweight)-attributable fraction is not valid for the Portuguese islands. A
stronger assumption is that children would have a similar obesity (overweight)-attributable
fraction as adults. Given the chronic nature of obesity-related diseases the value of obesity
(overweight)-attributable fraction for children is likely to be smaller.
Acknowledgements
I would like to thanks Anabela Botelho for sharing a STATA code with me. I am grateful to the
editor of this journal for the many helpful comments. I would like to acknowledge Ministerio da
Saude–Instituto Nacional Dr8 Ricardo Jorge for providing the data for this research project.
References
Bartlett, J., Miller, L., Rice, D., Max, W., 1994. Medical care expenditures attributable to cigarette smoking-United States,
1993. Morb. Mortal. Wkly. Rep. 43(26), 469–472. http://www.cdc.gov/mmwr/PDF/wk/mm4326.pdf.
Bhattacharya, J., Sood, N., 2007. Health insurance and the obesity externality. In: Bolin, K., Cawley, J. (Eds.), Advances
in Health Economics and Health Services Research (17). Elsevier, New York.
Castro, J., Dias, J., Baptista, F., Costa, J., Galvao-Teles, A., Camilo-Alves, A., 1998. Secular trends of weight, height and
obesity in cohorts of young Portuguese males in the district of Lisbon: 1960 to 1990. Eur. J. Epidemiol. 14 (3), 299–
303.
Cawley, J., Burkhauser, R. Beyond BMI: the value of more accurate measures of fatness and obesity in social science
research. J. Health Econ., in press.
Chaloupka, F., Warner, K., 2000. The economics of smoking. In: Newhouse, J., Cuyler, A. (Eds.), The Handbook of
Health Economics. Elsevier Science B.V, New York, North-Holland, pp. 1539–1627.
Colditz, G., 1992. Economic costs of obesity. Am. J. Clin. Nutr. 55, 503S–507S.
Coller, L., Harrison, G., McInnes, M., 2002. Evaluating the tobacco settlement: are the damages awards too much or not
enough? Am. J. Public Health 92(6), 984–989. http://www.ajph.org/cgi/reprint/92/6/984.pdf.
Finkelstein, E., Flebelkorn, I., Wang, G., 2003. National medical spending attributable to overweight and obesity: how
much, and who’s paying? Health Affairs Web Exclusive w3, 219–226. http://content.healthaffairs.org/cgi/reprint/
hlthaff.w3.219v1.
Finkelstein, E., Fiebelkorn, I, Wang, G., 2004. State-level estimates of annual medical expenditures attributable to obesity.
Obes. Res. 12, 18–24. http://www.obesityresearch.org/cgi/content/abstract/12/1/18.
Flegal, K., Carrol, M., Ogden, C., Johnson, C., 2002. Prevalence and trends in obesity among US adults 1998/1999–2000.
J. Am. Med. Assoc. 288 (14), 1723–1727.
Harrison, G., James, F., Edwards, A., Segovia, J., 2003. Cigarette smoking and costs of hospital and physician care. Can.
Public Policy – Anal. Polit. XXIX (1), 1–20.
Kolmos, J., Smith, P., Bogin, B., 2004. Obesity and the rate of preference is there a connection? J. Biosoc. Sci. 36 (2),
209–219.
Kuchler, F., Tegene, A., Harris, J., 2005. Taxing snacking foods: manipulating diet quality or financing information
programs? Rev. Agric. Econ. 27, 4–20.
Miller, L., Zhang, X., Novotny, T., Rice, D., Max W., 1998. State estimates of total expenditures attributable to
cigarette smoking, 2003. Public Health Rep. 113(2), 140–151. http://www.pubmedcentral.nih.gov/articlerender.
fcgi?artid=1308653.
Ministerio da Saude, Instituto Nacional Dr8 Ricardo Jorge, Observatorio Nacional de Saude: Inquerito Nacional de Saude.
Must, A., Spanado, J., Coackey, E., Field, A., Colditz, G., Dietz, W., 1999. The disease burden associated with overweight
and obesity. J. Am. Med. Assoc. 282 (16), 1523–1529.
Padez, C., Fernandes, T., Mourao, I., Moreira, P., Rosado, V., 2004. Prevalence of overweight and obesity in 7–9 year-old
Portuguese children: trends in body mass index from 1970–2002. Am. J. Hum. Biol. 16, 670–678.
Pereira, J., Mateus, C., Amaral, M., 1999. Custos da obesidade em Portugal. Documento de Trabalho 4/99, Associacao
Portuguesa de Economia da Saude, http://www.apes.pt/files/dts/dt_041999.pdf.
Pereira, J., Mateus, C., Amaral, M., 2000. Custos indirectos da obesidade. Comunicacao ao 7 ( Encontro Nacional de
Economia da Saude APES, Torre do Tombo, Lisboa, 16–17 de Novembro de 2000. http://www.adexo.pt/pdfs/
APES-JoaoPereira.pdf.
P. Veiga / Economics and Human Biology 6 (2008) 127–142 141

Philipson, T., Posner, J., Richard, A., 2003. The long-run growth in obesity as a function of technological change.
Perspect. Biol. Med. 46 (3), S87–S107.
Pi-Sunyer, F., 1991. Health implications of obesity. Am. J. Clin. Nutr. 53, 1595S–1603S.
Seidell, J., 1995. The impact of obesity on health status: some implications for health care costs. Int. J. Obes. Relat. Metab.
Disord. 19 (Suppl. 6), S13–S16.
StataCorp, 2003. Statistical Software: Release 8.0. Stata Corporation, College Station, TX.
Sturm, R., 2002. The effects of obesity, smoking, and drinking on medical problems and costs. Obesity outranks both
smoking and drinking in its deleterious effects on health and health costs. Health Affair 21, 245–253. http://
content.healthaffairs.org/cgi/reprint/21/2/245.pdf.
Vidal, P., Dias, M., 2005. Trends in overweight and obesity in Portugal: the national health survey 1995/1996–6 and 1998–
9. Obes. Res. 13, 1141–1145.
Wolfe, A., Colditz, G., 1996. Social and economic effects of body weight in the United States. Am. J. Clin. Nutr. 63, 466S–
469S.
World Health Organization, 2000. Obesity: preventing and managing the global epidemic. WHO Tech. Rep. Ser. 894.
http://whqlibdoc.who.int/trs/WHO_TRS_894_(part2).pdf.
Zhang, X., Miller, L., Max W., Rice, D., 1999. The cost of smoking to the Medicare program, 1993. Health Care Financing
Rev. 20(4), 179–196. http://www.tcsg.org/tobacco/99SummerHCFR.pdf.
P. Veiga / Economics and Human Biology 6 (2008) 127–142142