Embed Size (px)
Citation preview
OtosclerosisOtosclerosis
Department of OtorhinolaryngoglogyDepartment of Otorhinolaryngoglogy
the 2nd Hospital affliatted to Medical college the 2nd Hospital affliatted to Medical college
Zhejiang UniversityZhejiang University
Xu YapingXu Yaping
Introduction
bull Otosclerosis
1 Primary metabolic bone disease of the otic capsule and ossicles
2 Results in fixation of the ossicles and conductive hearing loss
3 May have sensorineural component if the cochlea is involved
1048708Genetically mediated via autosomal dominant transmission with incomplete penetrance (40) and variable expressivity
History of Otosclerosis and Stapes surgery
1048708 1704 ndash Valsalva first described stapes fixation
1048708 1857 ndash Toynbee linked stapes fixation to hearing loss
1048708 1890 ndash Katz was first to find microscopic evidence of
otosclerosis
1048708 1893 ndash Politzer described the clinical entity of
ldquootosclerosisrdquo
1048708 1890 ndash Bacon describes medical therapy for the
condition and supports the common view that
ldquosurgery should not be considered for a momentldquo
Epidemiology
bull 10 overall prevalence of histologic otosclerosis
bull 1 overall prevalence of clinically significant otosclerosis
bull Clinical otosclerosis ndashndash21 (WM)
bull Possible progression during pregnancy (10-17)
bull Bilaterality more common (89 vs 65)
bull 15-45 most common age range of presentation increases with age
Pathophysiology
bull Osseous dyscrasia
1 Resorption and formation of new bone
2 Limited to the temporal bone and ossicles
3 Inciting event unknown
many theories
Hereditary endocrine metabolic infectious vascular autoimmunehormonal
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
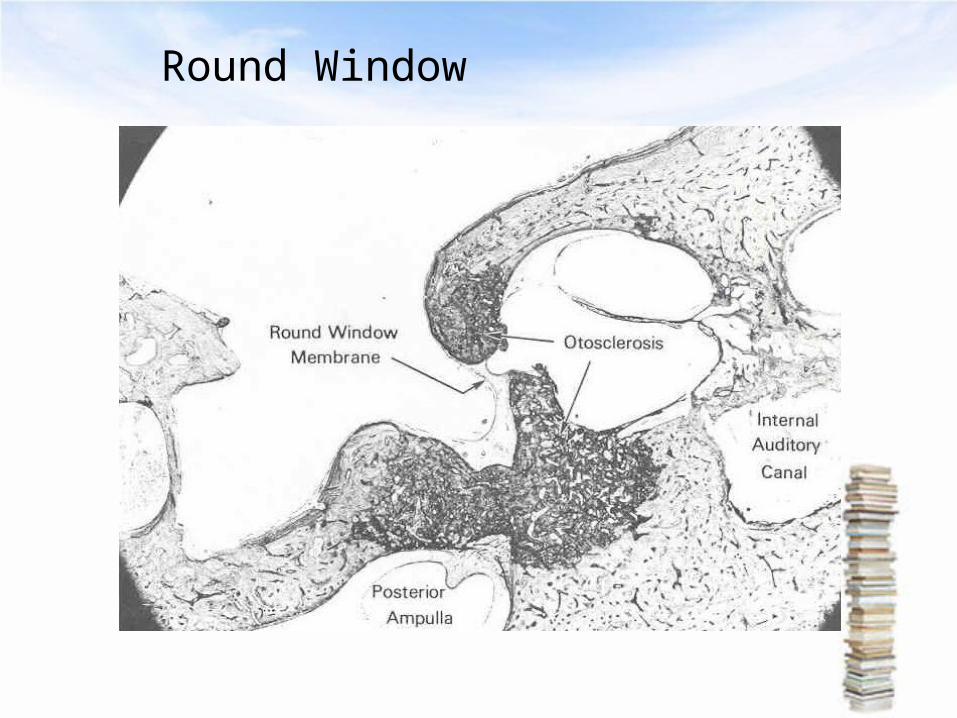
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
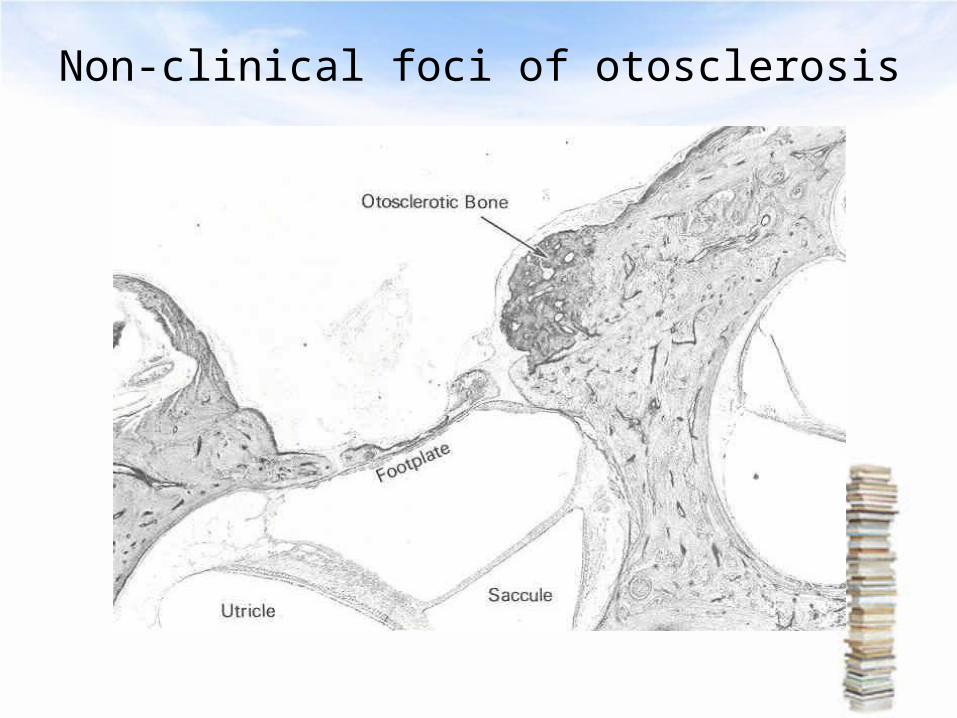
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
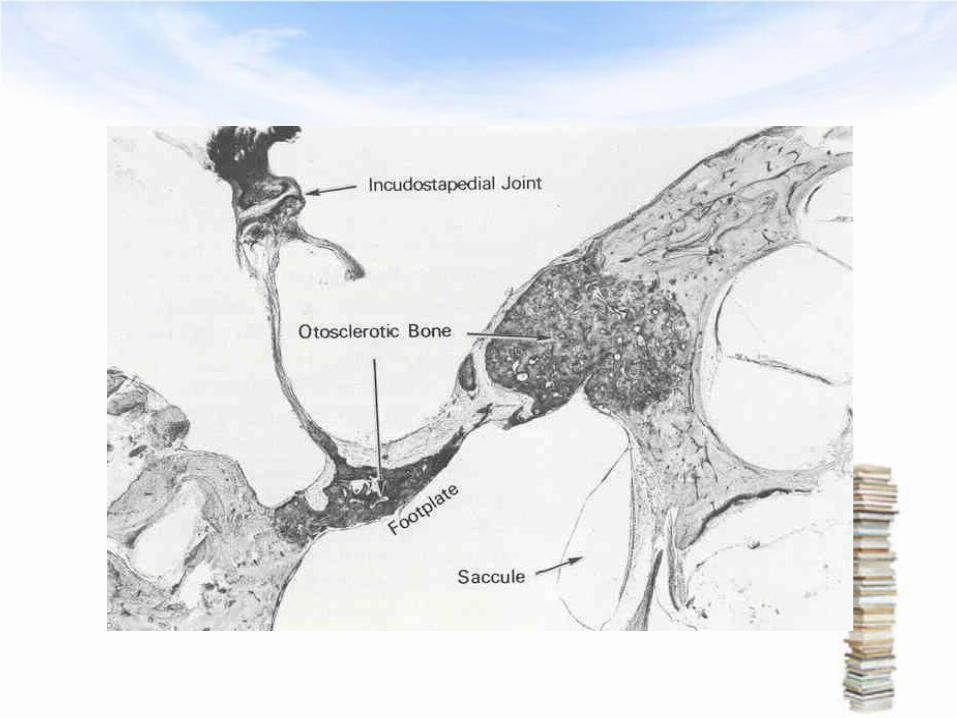
Non-clinical foci of otosclerosis
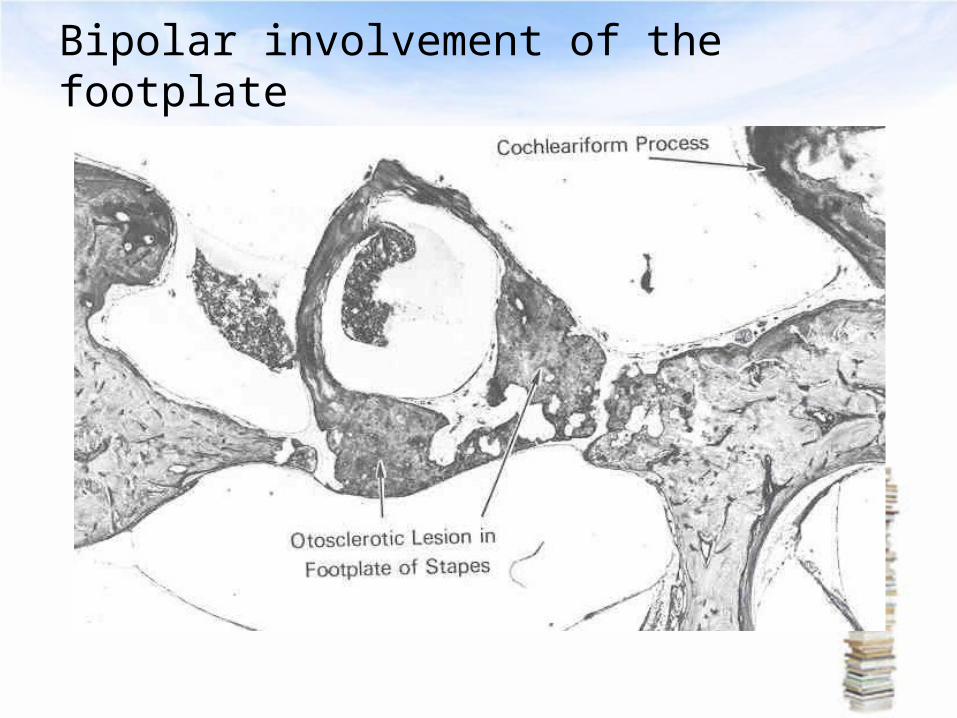
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
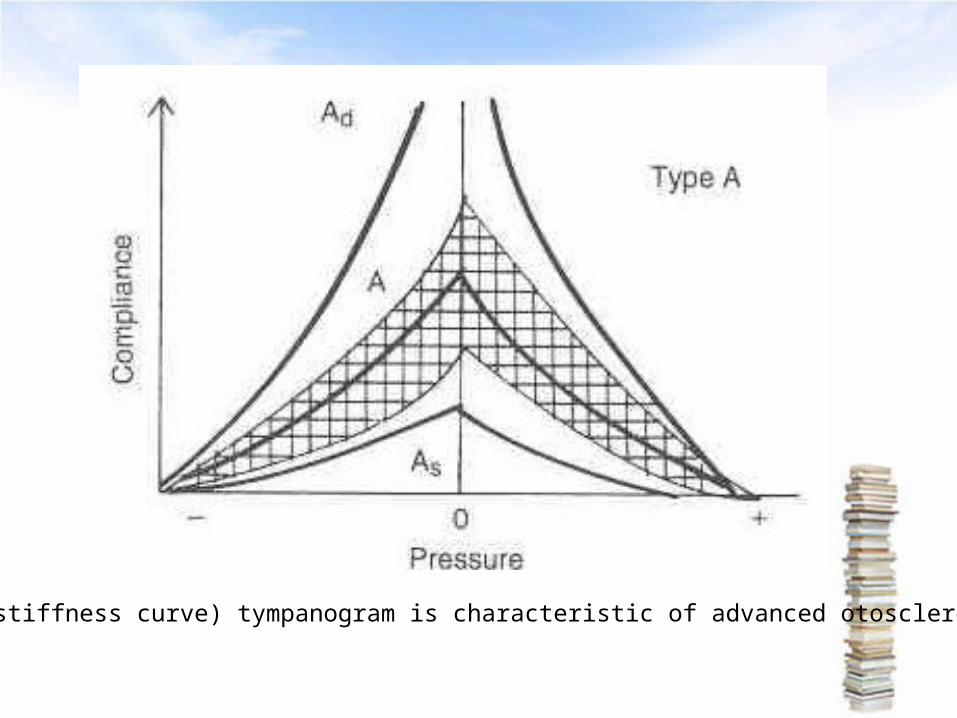
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Introduction
bull Otosclerosis
1 Primary metabolic bone disease of the otic capsule and ossicles
2 Results in fixation of the ossicles and conductive hearing loss
3 May have sensorineural component if the cochlea is involved
1048708Genetically mediated via autosomal dominant transmission with incomplete penetrance (40) and variable expressivity
History of Otosclerosis and Stapes surgery
1048708 1704 ndash Valsalva first described stapes fixation
1048708 1857 ndash Toynbee linked stapes fixation to hearing loss
1048708 1890 ndash Katz was first to find microscopic evidence of
otosclerosis
1048708 1893 ndash Politzer described the clinical entity of
ldquootosclerosisrdquo
1048708 1890 ndash Bacon describes medical therapy for the
condition and supports the common view that
ldquosurgery should not be considered for a momentldquo
Epidemiology
bull 10 overall prevalence of histologic otosclerosis
bull 1 overall prevalence of clinically significant otosclerosis
bull Clinical otosclerosis ndashndash21 (WM)
bull Possible progression during pregnancy (10-17)
bull Bilaterality more common (89 vs 65)
bull 15-45 most common age range of presentation increases with age
Pathophysiology
bull Osseous dyscrasia
1 Resorption and formation of new bone
2 Limited to the temporal bone and ossicles
3 Inciting event unknown
many theories
Hereditary endocrine metabolic infectious vascular autoimmunehormonal
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
History of Otosclerosis and Stapes surgery
1048708 1704 ndash Valsalva first described stapes fixation
1048708 1857 ndash Toynbee linked stapes fixation to hearing loss
1048708 1890 ndash Katz was first to find microscopic evidence of
otosclerosis
1048708 1893 ndash Politzer described the clinical entity of
ldquootosclerosisrdquo
1048708 1890 ndash Bacon describes medical therapy for the
condition and supports the common view that
ldquosurgery should not be considered for a momentldquo
Epidemiology
bull 10 overall prevalence of histologic otosclerosis
bull 1 overall prevalence of clinically significant otosclerosis
bull Clinical otosclerosis ndashndash21 (WM)
bull Possible progression during pregnancy (10-17)
bull Bilaterality more common (89 vs 65)
bull 15-45 most common age range of presentation increases with age
Pathophysiology
bull Osseous dyscrasia
1 Resorption and formation of new bone
2 Limited to the temporal bone and ossicles
3 Inciting event unknown
many theories
Hereditary endocrine metabolic infectious vascular autoimmunehormonal
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Epidemiology
bull 10 overall prevalence of histologic otosclerosis
bull 1 overall prevalence of clinically significant otosclerosis
bull Clinical otosclerosis ndashndash21 (WM)
bull Possible progression during pregnancy (10-17)
bull Bilaterality more common (89 vs 65)
bull 15-45 most common age range of presentation increases with age
Pathophysiology
bull Osseous dyscrasia
1 Resorption and formation of new bone
2 Limited to the temporal bone and ossicles
3 Inciting event unknown
many theories
Hereditary endocrine metabolic infectious vascular autoimmunehormonal
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Pathophysiology
bull Osseous dyscrasia
1 Resorption and formation of new bone
2 Limited to the temporal bone and ossicles
3 Inciting event unknown
many theories
Hereditary endocrine metabolic infectious vascular autoimmunehormonal
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
bull Most common sites of involvement
1 1048708Fissula ante fenestrum
2 1048708Round window niche (30-50 of cases)
3 1048708Anterior wall of the IAC
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Histology
otosclerosis has two main forms
1 an early of spongiotic phase (otospongiosis)
multiple active cell groups including
osteocytes osteoblasts and histiocytes
2 a late or sclerotic phase dense sclerotic bone forms
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Non-clinical foci of otosclerosis
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Bipolar involvement of the footplate
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Round Window
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Diagnosis of Otosclerosis
10487081 Most common presentation
1048708Women age 20 - 30
10487082 Conductive or Mixed hearing loss
slowly progressivebilateral (80)asymmetric
1048708Tinnitus (75)
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
a complete history
1 Age of onset of hearing loss
2 Progression
3 Laterality
4 Associated symptomsbull Dizzinessbull Otalgiabull Otorrheabull Tinnitus
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
bull Family history 104870823 have a significant family history 1048708Particularly helpful in patients with severe or profound mixed hearing loss
bull Prior otologic surgerybull History of ear infectionsbull Vestibular symptoms 104870825 1048708Most commonly dysequilibrium 1048708Occasionally attacks of vertigo with rotatory nystagmu
s
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Physical Exam
bull Otomicroscopy
Most helpful in ruling out other disorders
1048708Middle ear effusions
1048708Tympanosclerosis
1048708Tympanic membrane perforations
1048708Cholesteatoma or retraction pockets
1048708Superior semicircular canal dehiscence
Schwartzersquorsquos signs ( by Schwartze in 1873)
1048708Red hue behind the tympanic membrane (in oval window niche area)
104870810 of casesbull Pneumatic otoscopy
1048708Distinguish from malleus fixation
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
bull Tuning forks10487081 Hearing loss progresses form low frequencies to high
frequencies1048708 2 256 512 and 1024 Hz TF should be used 3 Rinne1048708256 Hz ndashndashnegative test indicates at least a 20 dB ABG 1048708512 Hz ndashndashnegative test indicates at least a 25 dB ABG (air-bone gaps)
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Differential Diagnosis
1Ossicular discontinuityAconductive loss of 60 db
B type Ad tympanogram
2Congenital stapes fixationA25 incidence of other
congenital anomalies
B non-progressive CHL
3Malleus head fixation when congenital associated with other stigmata (aural atresia)
4Pagetrsquorsquos disease diffuse involvement of the bony skeleton
5Osteogenesis imperfecta presence of blue sclera
6Superior semicircular canal dehiscence vertigo or eye movements with loud noise
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Audiometry
1048708Tympanometry
1048708Impedance testing
Acoustic reflexes
1048708Pure tones
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
As (s-stiffness curve) tympanogram is characteristic of advanced otosclerosis
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Acoustic Reflexes
bull Otosclerosis has a predictable pattern of abnormal reflexes over time
1 Reduced reflex amplitude
2 Elevation of ipsilateral thresholds
3 Elevation of contralateral thresholds
4 Absence of reflexes
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Pure Tone Audiometry
bull Most useful audiometric test for otosclerosis 1048708Characterizes the severity of disease 1048708Frequency specific
bull Carhartrsquorsquos notch 1048708Hallmark audiologic sign of otosclerosis 1048708Decrease in bone conduction thresholds 10487085 dB at 500 Hz 104870810 dB at 1000 Hz 104870815 dB at 2000 Hz 10487085 dB at 4000 Hz
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
early stage
middle stage
bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you

bull late stage
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
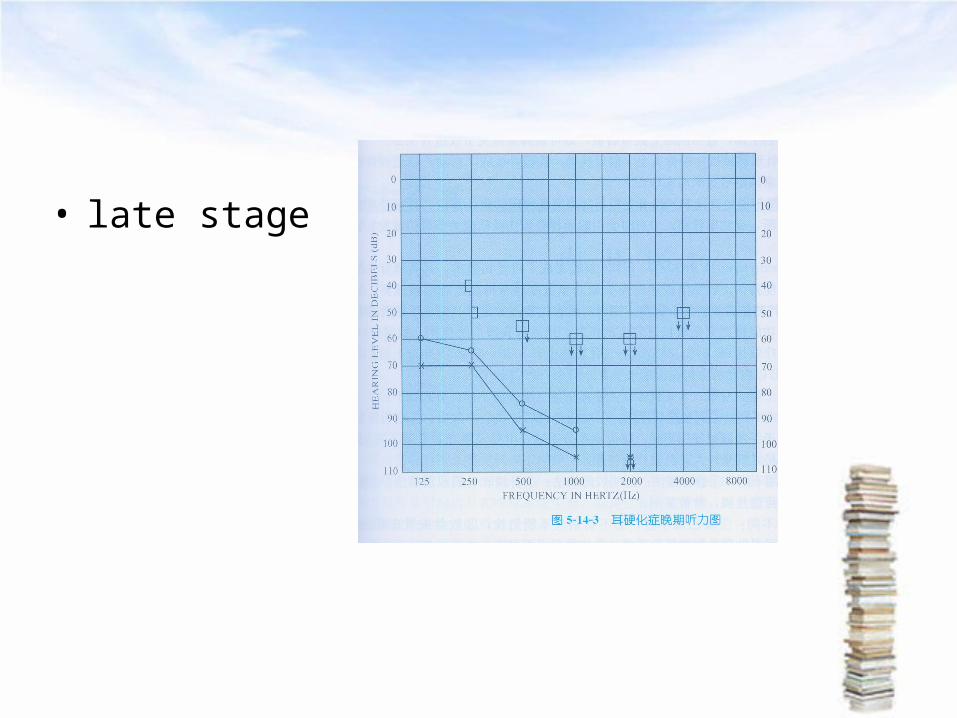
Imaging
bull Computed tomography (CT) of the temporal bone
1048708Proponents of CT for evaluation of otosclerosis
Pre-op
1 Characterize the extent of otosclerosis
2 Severe or profound mixed hearing loss
3 Evaluate for enlarge cochlear aqueduct
Post-op
1 Recurrent CHL
2 Re-obliteration vs prosthesis dislocation
3 Vertigo
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Management options
bull Medical Sodium FluorideBisphosphonatesVitamin D and Calcium
bull AmplificationNon-surgical candidates-wearing hearing aids
bull Surgery Stapedectomy vs Stapedotomy
bull Combinations
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
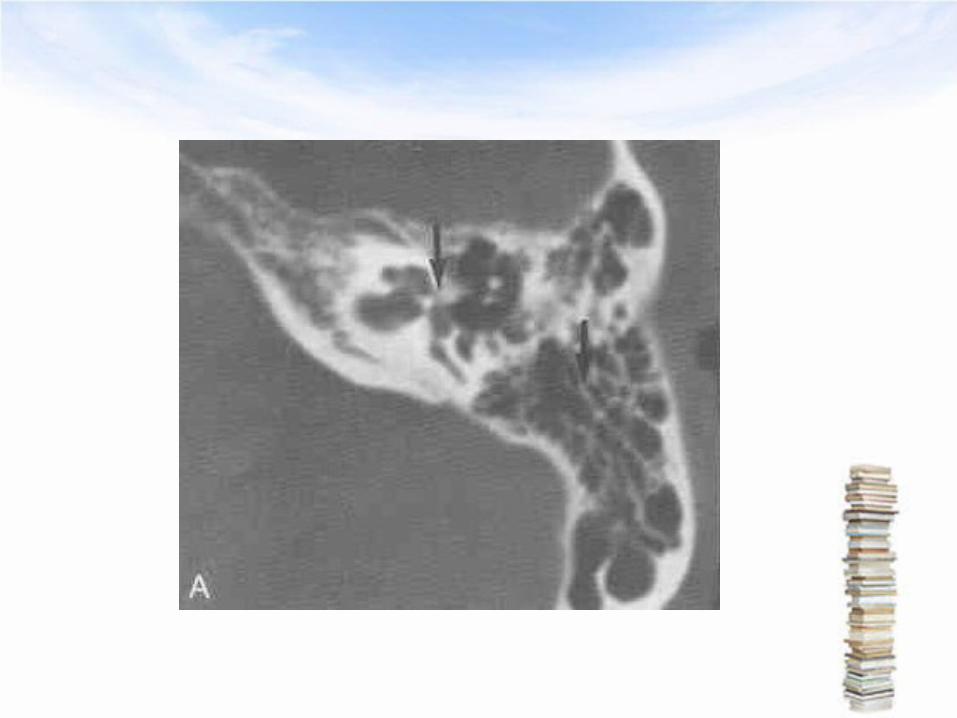
Surgery
bull Best surgical candidate
1Previously un-operated ear
2Good health
3Unacceptable ABG
425 to 40 dB
5Negative Rinne test
6Excellent discrimination
7Desire for surgery
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
Tympanosclerosis
bull Definition a whitish plaque of the TMbull Pathology submucosal hyaline degeneration in t
he TM and middle ear mucosabull extensive involvement of the TM and ossicle am
y result in conductive hearing loss(air-bone gap gt40dB)
bull medical therapy and pressure equalization tubes (PETs) do not prevent progression of disease
The end thank youThe end thank you
The end thank youThe end thank you