Embed Size (px)
Citation preview
Radiofrequency Ablation of Unresectable HepaticMalignancies: Lessons Learned
ANTON J. BILCHIK,a, b THOMAS F. WOOD,a DAVID P. ALLEGRAb
aDepartment of Surgical Oncology, John Wayne Cancer Institute, Santa Monica, California, USA; bthe CancerCenter at Century City Hospital, Los Angeles, California, USA
Key Words. Radiofrequency ablation · Hepatic malignancies
ABSTRACT
Radiofrequency ablation (RFA) is increasingly usedfor the local destruction of unresectable hepatic malig-nancies. Relative contraindications include tumors inproximity to vital structures that may be injured by RFAand lesions whose size exceeds the ablation capabilities ofthe probe system employed. Given current technology,we believe that RFA should be cautiously utilized forlesions greater than 5 cm in diameter. Open (celiotomy)and laparoscopic approaches to RFA allow intraopera-tive ultrasonography, which may demonstrate occult
hepatic disease. In addition, RFA performed viaceliotomy can be accompanied by resection or cryosur-gical ablation, and isolation of the liver from adjacentorgans. Percutaneous RFA should be reserved forpatients who cannot undergo general anesthesia, thosewith recurrent or progressive lesions, and those withsmaller lesions sufficiently isolated from adjacentorgans. Complications may be minimized when theseapproaches are selectively applied. The Oncologist2001;6:24-33
The Oncologist 2001;6:24-33 www.TheOncologist.com
Correspondence: Anton J. Bilchik, M.D., Ph.D., F.A.C.S., John Wayne Cancer Institute, 2200 Santa Monica Boulevard,Santa Monica, California 90404, USA. Telephone: 310-449-5206; Fax: 310-449-5261; e-mail: [email protected] August 15, 2000; accepted for publication October 18, 2000. ©AlphaMed Press 1083-7159/2001/$5.00/0
INTRODUCTION
The liver, a frequent site of primary and metastatic tumors,is second only to lymph nodes as the most common site ofmetastatic disease. Surgical resection of primary and metasta-tic hepatic tumors remains the gold standard of therapy.Unfortunately, because most hepatic malignancies are in unre-sectable locations or in patients with poor hepatic reserve,resection is possible in only 20% of these patients at the timeof their presentation [1]. The remaining patients may be can-didates for local ablative techniques (percutaneous ethanolinjection, microwave tumor coagulation, interstitial laser pho-tocoagulation, cryosurgical ablation, or radiofrequency abla-tion), hepatic-directed techniques (hepatic artery ligation,transcatheter arterial chemoembolization, hepatic artery infu-sional chemotherapy), or systemic chemotherapy. Cryosurgicalablation (CSA) of hepatic tumors is widely used for patients
with unresectable disease [2-5]. CSA can improve overall sur-vival [6], but it requires a celiotomy and is associated with arelatively high rate of serious complications, including coagu-lopathy, hemorrhage, pleural effusion, parenchymal cracking,bile duct injury, and acute renal failure [5, 7, 8]. Moreover, itsinstrumentation is cumbersome and expensive.
Radiofrequency ablation (RFA) destroys tumor by gen-erating heat within a lesion (Fig. 1). During RFA, high-fre-quency alternating current causes thermal coagulation andprotein denaturation; as the temperature is increased above45°C, cellular proteins denature and cell structure is lost.RFA technology is commonly used in the ablation of aber-rant conduction pathways in the heart and has become a pri-mary procedure in the treatment of cardiac dysrhythmias.RFA has increasingly been utilized for unresectable hepaticmalignancies.
TheOncologistDialogues in Oncology
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Bilchik, Wood, Allegra 25
Unlike CSA, RFA uses relatively inexpensive instru-mentation and can be performed in the operating room viaceliotomy or laparoscopy, or in the radiology suite via a per-cutaneous approach. Its reported complication and recur-rence rates are relatively low [9-11]. Previous reports havedemonstrated the utility of RFA for the destruction of smalllesions. However, relatively few studies have reported resultsof RFA in patients with primary and metastatic hepaticmalignancies, and its potential complications, optimalapproaches, and limitations have not been clearly defined. Atthe John Wayne Cancer Institute (JWCI), we have performedover 150 RFA procedures in a heterogeneous population ofpatients with primary and metastatic unresectable hepatictumors. This review summarizes the indications, limitations,and possible complications.
THE JWCI ALGORITHM FOR MANAGEMENT
OF UNRESECTABLE HEPATIC MALIGNANCIES
At JWCI, patients with a diagnosis of primary or metasta-tic hepatic tumors are treated with a multimodality approachthat includes surgical resection, CSA, RFA, and/or insertionof an hepatic artery infusion pump (HAIP) for delivery ofhepatic-directed chemotherapy [5]. Because our group [12]and other investigators [13] have reported a disease-free andoverall survival benefit associated with regional chemother-apy for metastatic colorectal cancer, we recommend place-ment of an HAIP in all patients who undergo resection and/orablation. The treatment plan is determined after a historyand physical, laboratory analysis including blood counts,chemistries, liver function tests, serum tumor markers, andradiologic evaluation. In addition, all patients undergo
spiral-computed tomography (CT) with intravenous contrast,and select patients also undergo magnetic resonance imaging(MRI) or positron emission tomography (PET) using 18FDG.
RFA is approached either operatively, via laparoscopy orceliotomy, or percutaneously by ultrasound or CT scan guid-ance. Laparoscopic examination of the abdomen is undertakenin all operative cases to identify extrahepatic disease.Laparoscopy is extremely sensitive for the detection of peri-toneal lesions; laparoscopic ultrasonography can detect hepaticlesions <2 cm in diameter, and it can identify disease notdetected by preoperative imaging—including PET [14].Overall, use of laparoscopy will avoid laparotomy or changethe planned operation in 30% of the cases. Celiotomy is per-formed if laparoscopy is not possible. A formal assessment ofthe liver, parietal peritoneum, visceral surfaces of the stomach,small bowel, colon, lesser sac, and omentum is performed. Thegastrohepatic ligament is divided and the caudate lobe isdirectly examined. The porta hepatis, celiac axis, and venacava are examined and suspicious lymph nodes are biopsied.If enlarged periportal lymph nodes are not amenable to laparo-scopic examination, a laparotomy is performed and the nodesare examined. Patients who have extrahepatic disease (exceptthose with neuroendocrine tumors) are not eligible for RFA.Patients who have no evidence of extrahepatic disease undergointraoperative ultrasonography (IOUS) of all liver segments;the size and location of each lesion are recorded and comparedwith preoperative imaging results.
Curative resection is always the first choice of treatmentand is undertaken whenever possible. Patients who are notcandidates for curative resection based on the location or bilo-bar distribution of hepatic tumors are considered for RFA.Patients eligible for RFA have no evidence of extrahepaticdisease, a tumor volume less than 40% of total hepatic volumeas determined by IOUS, and sufficient hepatic reserve toundergo ablation (Child-Pugh class A or B). Figure 2 showsour algorithm for RFA in patients with unresectable hepaticmalignancies [9, 10]. A single 25-min ablation is used forlesions <3 cm in diameter. If the patient has severe hepaticdysfunction (Child B, C cirrhosis) or if laparotomy is con-traindicated because of cardiac or respiratory dysfunction,larger lesions may be managed by multiple overlapping abla-tions performed laparoscopically. However, we generally pre-fer to use CSA for lesions >3 cm because in our experience,the recurrence rate for RFA of larger lesions is 35% [6].Recurrence rates associated with newer-generation probesmay be lower.
EVOLVING TECHNOLOGY
Until mid-1999, we performed RFA using the Model 30(50W) probe (RITA Medical Systems; Mountain View, CA)(Fig. 3). This probe has a 15-gauge needle with a retractable
Figure 1. Schematic diagram shows that RFA causes ionic vibration, whichleads to protein denaturation, thermal coagulation, and ultimately cell death.
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from

26 Radiofrequency Ablation of Hepatic Tumors
curved-electrode configuration, and it can be used to ablate anarea of tissue that is 2.5-3 cm in diameter. Since mid-1999, wehave performed RFA using either the Model 70 probe (RITA),the 5-cm Starburst XL needle/150W electrode (RITA) (Fig. 3),or a 200W cluster probe (Cool-tip, Radionics; Burlington,MA). The latter two probes are capable of ablating an areaof 4-5 cm in diameter.
RFA TECHNIQUE
The technique of RFA is the same with any probe, exceptfor the power and duration of ablation. For lesions ≤2 cm indiameter, the needle is placed into the center of the lesionunder ultrasound guidance. This is most easily accomplishedby orienting the RFA needle parallel to the plane of the ultra-sound probe. Tynes with thermocouples are deployedthrough the primary channel, and 50-200 watts of alternatingcurrent are delivered. As soon as the temperature exceeds90°C, an 8-25 min ablation is performed (depending upon
Laparoscopy to rule out extrahepatic disease
Laparoscopic intraoperative ultrasonography of all hepatic segments
RFA of nonresectable hepatic lesions
Percutaneous RFA
Recurrent/New lesions
CT follow-up
Multiple overlappingablations for single
lesion >3 cm inhigh-risk patients
Combined modalityapproach for >3 lesions:• Celiotomy• RFA for lesions ≤3 cm• CSA for lesions >3 cm
Single ablationfor lesion(s) ≤3 cm
Figure 2. Algorithm for operative or percutaneous RFA at JWCI. Resectable lesions should be resected and an operative approachtaken whenever possible.
Figure 3. Technology of RFA probes and generators is improv-ing with the development of first-generation (top), second-gen-eration (middle), and latest-generation (bottom) probes (RITAMedical Systems), each capable of larger areas of ablation.Reprinted with permission from Wood et al. [18].
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Bilchik, Wood, Allegra 27
the probe used). The formation of the heat lesion is moni-tored with real-time ultrasonography. The tumor and a 1-cmmargin of normal hepatic parenchyma are ablated. The cur-rent is terminated and temperatures of the tynes are evalu-ated 30 sec later; a temperature of at least 60°C 30 secfollowing ablation insures adequate tissue necrosis [15-17].
Larger lesions are ablated with multiple overlapping fields.The probe is placed at the deep margin at one side of the tumor.Multiple overlapping ablations are then sequentially performed,progressing superficially and then laterally until the tumor anda 1-cm margin have been successfully ablated.
Following ablation, the probe tract is cauterized as theRFA needle is withdrawn. If target temperatures are notreached, as may be the case for lesions near major vascularstructures (heat-sink), the tynes are withdrawn slightly orrotated approximately 45°C to increase the temperature in theregion of ablation. Each tumor is ablated under imaging guid-ance with the goal of complete destruction of the tumor and a1-cm margin of parenchyma around the lesion in all directions.
RFA via celiotomy or laparoscopy is performed withIOUS guidance in the operating room while the patient isunder general anesthesia; percutaneous RFA is performed byan experienced interventional radiologist with ultrasonographyor CT guidance in the radiology suite, after local anesthesiaand conscious sedation.
Following laparoscopic RFA, patients are usually admit-ted for 23 h; percutaneous RFA is performed either on an out-patient or a 23-h-stay basis. Patients undergoing RFA viaceliotomy require hospital admission. Complete blood countsand liver function tests are obtained following RFA and thenext morning for patients staying in the hospital. Thosepatients undergoing additional procedures are treated accord-ing to the extent necessary. Patients are followed postopera-tively with repeat spiral CT scanning or other anatomicimaging and tumor markers as appropriate. Scans are obtainedat one week as a baseline and then every three months.
JWCI EXPERIENCE
We recently reported the results of RFA for the treat-ment of 231 unresectable hepatic tumors in 84 patients whohad no evidence of extrahepatic disease [18]. The patientgroup was heterogeneous in terms of tumor type and previ-ous therapy. The 84 patients underwent a total of 91 RFAprocedures, most of which used an operative approach. In51 cases, RFA was performed as the sole hepatic procedure.In the remaining 40 procedures, RFA was combined withresection, CSA, or HAIP. CSA was combined with RFA ina total of 16 patients with multiple hepatic metastases. CSAwas selectively used for larger diameter lesions (>3 cm)approached via celiotomy. We previously demonstratedthat RFA and CSA may be combined safely and that CSA
allows more rapid ablation of larger lesions [5]. In thissmall group of patients, there were no significant intraoper-ative or postoperative complications. The median diameterof lesions treated by RFA was 3.0 cm (range, 0.3-9.0 cm).The median length of hospital stay was five days after RFAvia celiotomy, one day after laparoscopic RFA, and 0 daysafter percutaneous RFA.
IOUS identified additional intrahepatic lesions not notedon preoperative spiral CT scans in 25 of 66 patients (38%)undergoing RFA via celiotomy or laparoscopy (Fig. 4). In allof these cases, the newly identified lesions were ablatedunder ultrasound guidance.
Ten patients required a second RFA procedure (sequentialablation), and one of the 10 required a third RFA procedure.Seven repeat procedures were performed for progressive liverlesions outside the initial RFA site, three were for recurrentlesions, and one was necessary to complete the ablation of a 5-cm hepatic lesion. Of the 11 repeat procedures, two wereperformed in the same patient, who developed progressiveintrahepatic disease outside the initial RFA site at 6 and 11
Figure 4. Intraoperative ultrasonogram shows a 0.8-cm colorec-tal carcinoma metastasis that was not visible on a preoperativespiral-CT scan. The RFA probe is placed into the center of thelesion and ablation performed. Reprinted with permission fromWood et al. [18].
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from
28 Radiofrequency Ablation of Hepatic Tumors
months after the initial RFA procedure. This patient is cur-rently well 18 months after the initial RFA for an hepaticcolorectal metastasis.
COMPLICATIONS
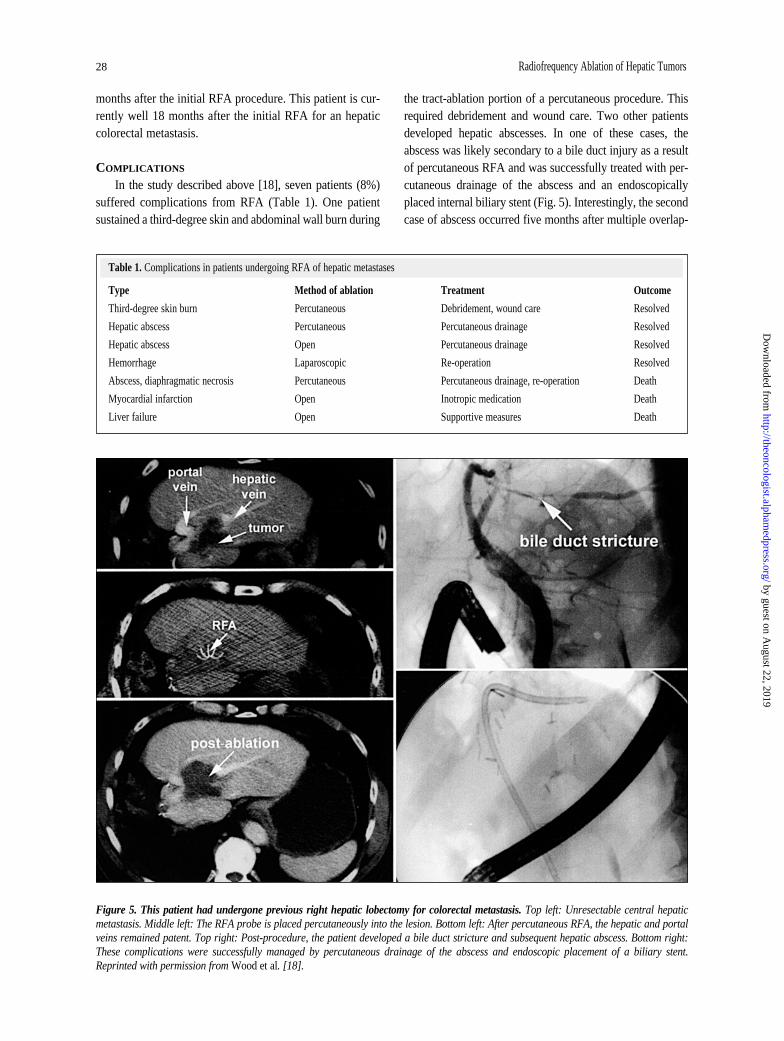
In the study described above [18], seven patients (8%)suffered complications from RFA (Table 1). One patientsustained a third-degree skin and abdominal wall burn during
the tract-ablation portion of a percutaneous procedure. Thisrequired debridement and wound care. Two other patientsdeveloped hepatic abscesses. In one of these cases, theabscess was likely secondary to a bile duct injury as a resultof percutaneous RFA and was successfully treated with per-cutaneous drainage of the abscess and an endoscopicallyplaced internal biliary stent (Fig. 5). Interestingly, the secondcase of abscess occurred five months after multiple overlap-
Table 1. Complications in patients undergoing RFA of hepatic metastases
Type Method of ablation Treatment Outcome
Third-degree skin burn Percutaneous Debridement, wound care Resolved
Hepatic abscess Percutaneous Percutaneous drainage Resolved
Hepatic abscess Open Percutaneous drainage Resolved
Hemorrhage Laparoscopic Re-operation Resolved
Abscess, diaphragmatic necrosis Percutaneous Percutaneous drainage, re-operation Death
Myocardial infarction Open Inotropic medication Death
Liver failure Open Supportive measures Death
Figure 5. This patient had undergone previous right hepatic lobectomy for colorectal metastasis. Top left: Unresectable central hepaticmetastasis. Middle left: The RFA probe is placed percutaneously into the lesion. Bottom left: After percutaneous RFA, the hepatic and portalveins remained patent. Top right: Post-procedure, the patient developed a bile duct stricture and subsequent hepatic abscess. Bottom right:These complications were successfully managed by percutaneous drainage of the abscess and endoscopic placement of a biliary stent.Reprinted with permission from Wood et al. [18].
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from

Bilchik, Wood, Allegra 29
ping RFAs of a 9-cm hepatoma in a patient with advancedcirrhosis. This patient did well for 20 months but recentlydemonstrated evidence of recurrence at the RFA site, as wellas progression at other hepatic sites. These complicationsresulted in no permanent sequelae.
However, the remaining three complications weresevere and eventually fatal (4%). The first of these patients,who had metastatic colorectal carcinoma, underwent a sec-ond percutaneous RFA procedure to complete the ablationof a 5-cm hepatic lesion that extended to the dome of theliver. This patient sustained a heat-necrosis injury to hisdiaphragm and associated hepatic abscess. Despite aggres-sive care, he succumbed to sepsis and multiorgan failure. Inretrospect, the percutaneous approach should not have beenused in this patient, in whom an operative approach wouldhave been safer. Of the three mortalities reported in thisseries, this is the only death that was directly related to theRFA (Table 1).
UNUSUAL COMPLICATIONS
Since that study, we have noted two unusual complica-tions as a result of percutaneous RFA. The first case was a78-year-old man with a significant cardiac history, whodeveloped a solitary colorectal metastasis in the left lobe ofthe liver. Percutaneous RFA resulted in a left hepatic arterypseudoaneurysm, which was subsequently successfullyembolized (Fig. 6). The second case was an 80-year-oldman who sustained an injury to the right hepatic artery dur-ing RFA of a hepatoma in segment 5, very close to the por-tal vein. Again, embolization was successful, but the patientlater developed an hepatic abscess that required percutaneousdrainage.
RECURRENCE
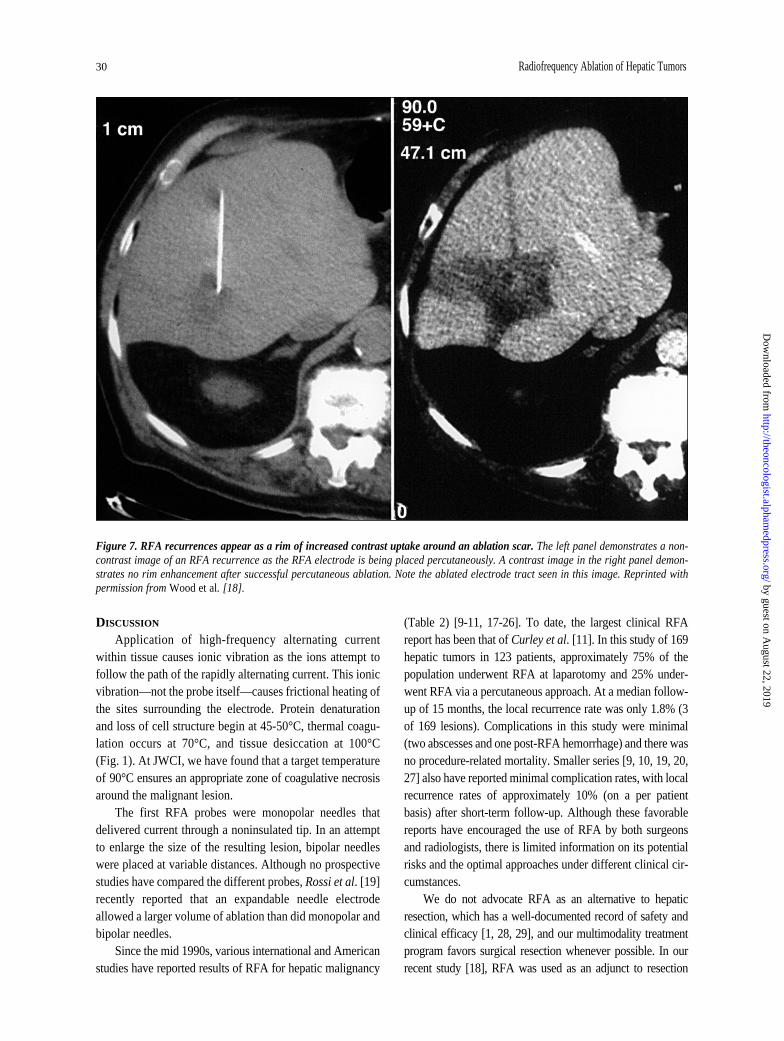
At a median follow-up of 13 months (range, 1-31months), 16 patients had developed a recurrence at the RFAsite (Fig. 7). Of those patients who recurred, three are with-out clinical evidence of disease after repeat RFA, 10 are alivewith disease, and three have died of their disease after amedian follow-up of 15 months. Of those patients who havenot recurred at RFA sites, 34 have no clinical evidence of dis-ease, 14 are alive with disease, and 21 have died of their dis-ease. New liver tumors or extrahepatic metastases thereforedeveloped in 38 patients (45%). Approximately one-third oflesions ≥3 cm in diameter recurred. All of the 16 recurrencesrequired multiple overlapping ablations to include the lesionand 1-cm margins. Recurrence after RFA was significantlyrelated to the size of the ablated lesion: recurrence was morelikely to follow ablation of larger lesions (average diameter,4.1 cm; median, 3.5 cm; range, 3-9 cm) than smaller lesions(average diameter, 2.8 cm; median, 2.5 cm; range, 1.5-7 cm)
(p < 0.001 by two-tailed t-test). The likelihood of recurrencewas not statistically related to the number of lesions ablated,the ablation of colorectal versus noncolorectal hepatic metas-tases, or the RFA approach (celiotomy versus laparoscopyversus percutaneous). Thirty-seven patients experienced pro-gressive intrahepatic disease outside the site of ablation. Therate of new intrahepatic metastases was independent of theRFA approach.
Figure 6. Left hepatic artery pseudoaneurysm following percuta-neous RFA of a solitary colorectal metastasis in a 78-year-old mandemonstrated on CT scan (A) and angiogram (B). Successfulembolization of the pseudoaneurysm (C).
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from
30 Radiofrequency Ablation of Hepatic Tumors
DISCUSSION
Application of high-frequency alternating currentwithin tissue causes ionic vibration as the ions attempt tofollow the path of the rapidly alternating current. This ionicvibration—not the probe itself—causes frictional heating ofthe sites surrounding the electrode. Protein denaturationand loss of cell structure begin at 45-50°C, thermal coagu-lation occurs at 70°C, and tissue desiccation at 100°C(Fig. 1). At JWCI, we have found that a target temperatureof 90°C ensures an appropriate zone of coagulative necrosisaround the malignant lesion.
The first RFA probes were monopolar needles thatdelivered current through a noninsulated tip. In an attemptto enlarge the size of the resulting lesion, bipolar needleswere placed at variable distances. Although no prospectivestudies have compared the different probes, Rossi et al. [19]recently reported that an expandable needle electrodeallowed a larger volume of ablation than did monopolar andbipolar needles.
Since the mid 1990s, various international and Americanstudies have reported results of RFA for hepatic malignancy
(Table 2) [9-11, 17-26]. To date, the largest clinical RFAreport has been that of Curley et al. [11]. In this study of 169hepatic tumors in 123 patients, approximately 75% of thepopulation underwent RFA at laparotomy and 25% under-went RFA via a percutaneous approach. At a median follow-up of 15 months, the local recurrence rate was only 1.8% (3of 169 lesions). Complications in this study were minimal(two abscesses and one post-RFA hemorrhage) and there wasno procedure-related mortality. Smaller series [9, 10, 19, 20,27] also have reported minimal complication rates, with localrecurrence rates of approximately 10% (on a per patientbasis) after short-term follow-up. Although these favorablereports have encouraged the use of RFA by both surgeonsand radiologists, there is limited information on its potentialrisks and the optimal approaches under different clinical cir-cumstances.
We do not advocate RFA as an alternative to hepaticresection, which has a well-documented record of safety andclinical efficacy [1, 28, 29], and our multimodality treatmentprogram favors surgical resection whenever possible. In ourrecent study [18], RFA was used as an adjunct to resection
Figure 7. RFA recurrences appear as a rim of increased contrast uptake around an ablation scar. The left panel demonstrates a non-contrast image of an RFA recurrence as the RFA electrode is being placed percutaneously. A contrast image in the right panel demon-strates no rim enhancement after successful percutaneous ablation. Note the ablated electrode tract seen in this image. Reprinted withpermission from Wood et al. [18].
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from
Bilchik, Wood, Allegra 31
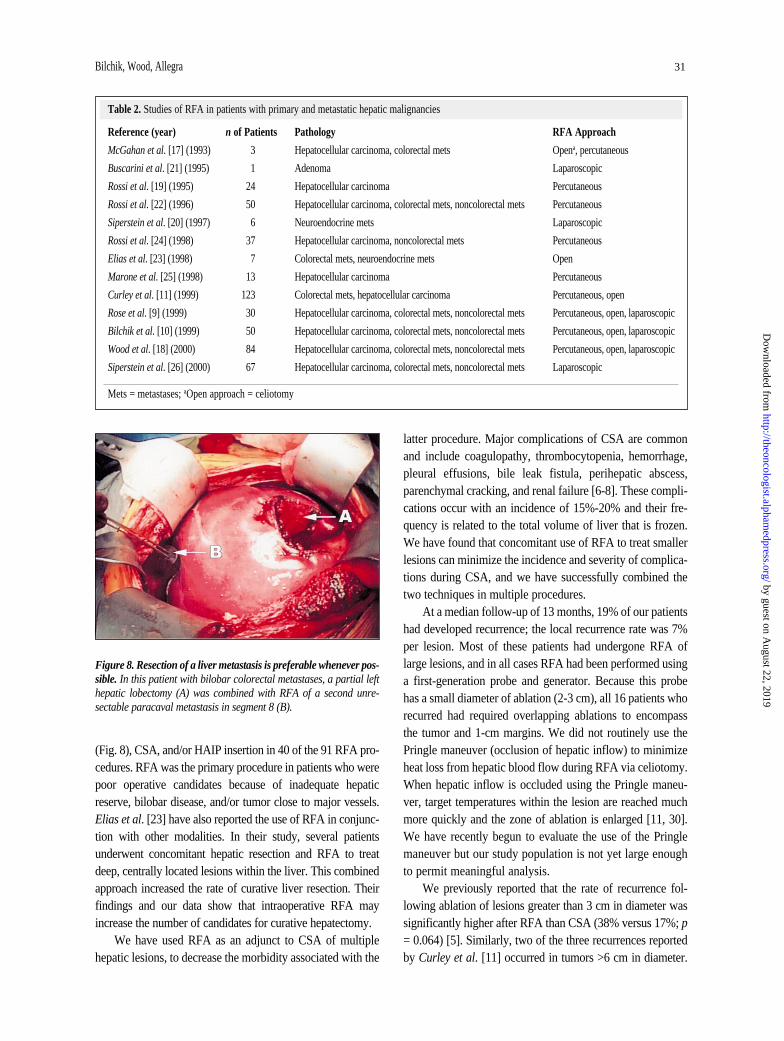
(Fig. 8), CSA, and/or HAIP insertion in 40 of the 91 RFA pro-cedures. RFA was the primary procedure in patients who werepoor operative candidates because of inadequate hepaticreserve, bilobar disease, and/or tumor close to major vessels.Elias et al. [23] have also reported the use of RFA in conjunc-tion with other modalities. In their study, several patientsunderwent concomitant hepatic resection and RFA to treatdeep, centrally located lesions within the liver. This combinedapproach increased the rate of curative liver resection. Theirfindings and our data show that intraoperative RFA mayincrease the number of candidates for curative hepatectomy.
We have used RFA as an adjunct to CSA of multiplehepatic lesions, to decrease the morbidity associated with the
latter procedure. Major complications of CSA are commonand include coagulopathy, thrombocytopenia, hemorrhage,pleural effusions, bile leak fistula, perihepatic abscess,parenchymal cracking, and renal failure [6-8]. These compli-cations occur with an incidence of 15%-20% and their fre-quency is related to the total volume of liver that is frozen.We have found that concomitant use of RFA to treat smallerlesions can minimize the incidence and severity of complica-tions during CSA, and we have successfully combined thetwo techniques in multiple procedures.
At a median follow-up of 13 months, 19% of our patientshad developed recurrence; the local recurrence rate was 7%per lesion. Most of these patients had undergone RFA oflarge lesions, and in all cases RFA had been performed usinga first-generation probe and generator. Because this probehas a small diameter of ablation (2-3 cm), all 16 patients whorecurred had required overlapping ablations to encompassthe tumor and 1-cm margins. We did not routinely use thePringle maneuver (occlusion of hepatic inflow) to minimizeheat loss from hepatic blood flow during RFA via celiotomy.When hepatic inflow is occluded using the Pringle maneu-ver, target temperatures within the lesion are reached muchmore quickly and the zone of ablation is enlarged [11, 30].We have recently begun to evaluate the use of the Pringlemaneuver but our study population is not yet large enoughto permit meaningful analysis.
We previously reported that the rate of recurrence fol-lowing ablation of lesions greater than 3 cm in diameter wassignificantly higher after RFA than CSA (38% versus 17%; p= 0.064) [5]. Similarly, two of the three recurrences reportedby Curley et al. [11] occurred in tumors >6 cm in diameter.
Table 2. Studies of RFA in patients with primary and metastatic hepatic malignancies
Reference (year) n of Patients Pathology RFA Approach
McGahan et al. [17] (1993) 3 Hepatocellular carcinoma, colorectal mets Opena, percutaneous
Buscarini et al. [21] (1995) 1 Adenoma Laparoscopic
Rossi et al. [19] (1995) 24 Hepatocellular carcinoma Percutaneous
Rossi et al. [22] (1996) 50 Hepatocellular carcinoma, colorectal mets, noncolorectal mets Percutaneous
Siperstein et al. [20] (1997) 6 Neuroendocrine mets Laparoscopic
Rossi et al. [24] (1998) 37 Hepatocellular carcinoma, noncolorectal mets Percutaneous
Elias et al. [23] (1998) 7 Colorectal mets, neuroendocrine mets Open
Marone et al. [25] (1998) 13 Hepatocellular carcinoma Percutaneous
Curley et al. [11] (1999) 123 Colorectal mets, hepatocellular carcinoma Percutaneous, open
Rose et al. [9] (1999) 30 Hepatocellular carcinoma, colorectal mets, noncolorectal mets Percutaneous, open, laparoscopic
Bilchik et al. [10] (1999) 50 Hepatocellular carcinoma, colorectal mets, noncolorectal mets Percutaneous, open, laparoscopic
Wood et al. [18] (2000) 84 Hepatocellular carcinoma, colorectal mets, noncolorectal mets Percutaneous, open, laparoscopic
Siperstein et al. [26] (2000) 67 Hepatocellular carcinoma, colorectal mets, noncolorectal mets Laparoscopic
Mets = metastases; aOpen approach = celiotomy
Figure 8. Resection of a liver metastasis is preferable whenever pos-sible. In this patient with bilobar colorectal metastases, a partial lefthepatic lobectomy (A) was combined with RFA of a second unre-sectable paracaval metastasis in segment 8 (B).
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from

32 Radiofrequency Ablation of Hepatic Tumors
We believe that the maximum diameter of tumors treatedwith RFA depends in part on the specific probe. It alsodepends on the accurate delineation of the margins of abla-tion using ultrasonography or CT; this is especially importantwhen multiple overlapping ablations are attempted. DuringCSA, the characteristic iceball is easily followed via real-time ultrasonography; by contrast, the increased echogenic-ity during RFA is more difficult to follow. Perhaps as RFAand intraoperative imaging technologies improve and proce-dures are performed under temporary occlusion of hepaticinflow (Pringle maneuver), larger lesions will be more suc-cessfully approached by RFA. However, in our limited expe-rience with the larger probes, more time is required to ablatelarger lesions. The current generators have increased outputbut they can power only one probe.
Our experience indicates that the rates of recurrence andcomplications following RFA are not negligible but can beminimized. Patients with hepatic malignancies, except thosewith neuroendocrine tumors, should be approached withcurative intent and the goal of extending survival. IOUS dur-ing celiotomy or laparoscopy can upstage cancers bydemonstrating intrahepatic disease not evident on spiral CTscans [31, 32]. Approximately 12% of patients undergoinglaparoscopy prior to RFA will have extrahepatic disease andtherefore will not be candidates for potentially curative pro-cedures [5]. We prefer operative ablative proceduresbecause either an open or laparoscopic approach allowsdetection of extrahepatic disease missed by preprocedureimaging. The laparoscopic approach is minimally invasiveand useful for ablating a small number of small lesions. Theceliotomy approach is more invasive but also more versatile;large and multiple tumors may be safely treated and RFAcan be combined with other hepatic therapies (resection,CSA, or HAIP). We recommend RFA via celiotomy orlaparoscopy in patients who are operative candidates; wereserve percutaneous RFA for patients who would not toler-ate surgery or have recurrent or progressive disease. Toavoid injury to adjacent structures, lesions approached per-cutaneously must not be located peripherally in the liver.Furthermore, lesion size and location must be within thecapacity of the percutaneous approach.
In our experience, the risk of recurrence increases afterablation of lesions adjacent to major blood vessels.Because of the heat-sink effect of large vessels, the zone ofablation extends to near the vessel wall, but the tissue clos-est to the vessel is not ablated and therefore at high risk ofpersistent or recurrent disease. Also, a portal vein throm-bosis has been reported after ablation of a periportal tumorduring a Pringle maneuver [33], so due care should be exer-cised during ablations close to major vessels. Becausemajor bile ducts are at increased danger for heat injury dur-ing ablation of central lesions, we place prophylactic bil-iary stents in patients undergoing ablation of tumoradjacent to major bile ducts. Thus far, we have been able toablate these lesions with stents in place, without untowardbiliary complications.
SUMMARY
In summary, RFA can be safely applied via operativeapproaches (laparoscopy or celiotomy) or percutaneously forunresectable hepatic malignancies. Operative approachesallow more accurate assessment for the presence of extrahep-atic disease, better evaluation of intrahepatic disease (IOUS),and isolation of the liver from adjacent organs that may beinjured during ablation of superficial lesions. Operativeapproaches also are preferable in patients with multiple andlarge lesions, since optimal management usually requires acombination of treatment modalities. Percutaneous RFAshould be reserved for patients who are not operative candi-dates and patients with recurrent or progressive disease.Extra care should be taken when using RFA in lesions largerthan 3 cm in diameter, to reduce the rate of recurrence.Because of the relatively high rate of disease progression atintrahepatic and extrahepatic sites, consideration of hepatic-directed and systemic chemotherapy is reasonable in thesepatients [11, 13]. Severe complications and even death afterRFA are rare but warrant careful selection of patients and RFAapproaches.
ACKNOWLEDGMENT
Supported in part by funding from the Rogovin-Davidow Foundation, Los Angeles, CA.
REFERENCES
1 Cady B, Jenkins RL, Steele GD Jr. et al. Surgical margin inhepatic resection for colorectal metastasis: a critical and improv-able determinant of outcome. Ann Surg 1998;227:566-571.
2 Bilchik AJ, Sarantou T, Wardlaw JC et al. Cryosurgery causesa profound reduction in tumor markers in hepatoma and non-colorectal hepatic metastases. Am Surg 1997;63:796-800.
3 Bilchik AJ, Sarantou T, Foshag LJ et al. Cryosurgical palliationof metastatic neuroendocrine tumors resistant to conventionaltherapy. Surgery 1997;122:1040-1047.
4 Pearson AS, Izzo F, Fleming RY et al. Intraoperative radiofre-quency ablation or cryoablation for hepatic malignancies. AmJ Surg 1999;178:592-599.
5 Bilchik AJ, Wood TF, Allegra D et al. Cryosurgical ablation andradiofrequency ablation of unresectable hepatic malignant neo-plasms: a proposed algorithm. Arch Surg 2000;135:657-664.
6 Ravikumar TS, Kane R, Cady B et al. A 5-year study of cryosurgery in the treatment of liver tumors. Arch Surg1991;126:1520-1523.
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from
Bilchik, Wood, Allegra 33
7 Seifert JK, Morris DL. World survey on the complications ofhepatic and prostate cryotherapy. World J Surg 1999;23:109-113.
8 Sarantou T, Bilchik A, Ramming KP. Complications of hepaticcryosurgery. Semin Surg Oncol 1998;14:156-162.
9 Rose DM, Allegra DP, Bostick PJ et al. Radiofrequency abla-tion: a novel primary and adjunctive ablative technique forhepatic malignancies. Am Surg 1999;65:1009-1014.
10 Bilchik AJ, Rose DM, Allegra DP et al. Radiofrequency abla-tion: a minimally invasive technique with multiple applications.Cancer J Sci Am 1999;5:356-361.
11 Curley SA, Izzo F, Delrio P et al. Radiofrequency ablation ofunresectable primary and metastatic hepatic malignancies:results in 123 patients. Ann Surg 1999;230:1-8.
12 Bilchik AJ, Chawla S, Rose DM et al. Systemic irinotecan(CPT-11) and regional chemotherapy prolong survival afterhepatic cryosurgery in patients with metastatic colon cancerrefractory to 5-fluorouracil (5-FU). Proc Am Soc Clin Oncol1999;18:254a.
13 Kemeny N, Huang Y, Cohen AM et al. Hepatic arterial infu-sion of chemotherapy after resection of hepatic metastasesfrom colorectal cancer. N Engl J Med 1999;341:2039-2048.
14 Tsioulias GJ, Wood TF, Chung M et al. Diagnostic laparo-scopy and laparoscopic ultrasonography optimize staging andresectability of intraabdominal neoplasms. Surg Endosc (in press).
15 Lounsberry W, Goldschmidt V, Linke C. The early histologicchanges following electrocoagulation. Gastrointest Endosc1995;41:68-70.
16 McGahan JP, Brock JM, Tesluk H. Hepatic ablation with useof radio-frequency electrocautery in the animal model. J VascInterv Radiol 1992;3:291-297.
17 McGahan J, Schneider P, Brock J. Treatment of liver tumors bypercutaneous radio frequency electrocautery. Semin InterventRadiol 1993:10:143-149.
18 Wood TF, Rose DM, Chung M et al. Radiofrequency ablationof 231 unresectable hepatic tumors: indications, limitations,and complications. Ann Surg Oncol 2000;7:593-600.
19 Rossi S, Di Stasi M, Buscarini E et al. Percutaneous radiofre-quency interstitial thermal ablation in the treatment of smallhepatocellular carcinoma. Cancer J Sci Am 1995;1:73.
20 Siperstein AE, Rogers SJ, Hansen PD et al. Laparoscopicthermal ablation of hepatic neuroendocrine tumor metastases.Surgery 1997;122:1147-1154.
21 Buscarini L, Rossi S, Fornari F et al. Laparoscopic ablation ofliver adenoma by radiofrequency electrocautery. GastrointestEndosc 1995;41:68-70.
22 Rossi S, Di Stasi M, Buscarini E et al. Percutaneous RF inter-stitial thermal ablation in the treatment of hepatic cancer. AJRAm J Roentgenol 1996;167:759-768.
23 Elias D, Debaere T, Muttillo I et al. Intraoperative use ofradiofrequency treatment allows an increase in the rate ofcurative liver resection. J Surg Oncol 1998;67:190-191.
24 Rossi S, Buscarini E, Garbagnati F et al. Percutaneous treat-ment of small hepatic tumors by an expandable RF needleelectrode. Am J Roentgenol 1998;170:1015-1022.
25 Marone G, Francica G, D’Angelo V et al. Echo-guidedradiofrequency percutaneous ablation of hepatocellular carci-noma in cirrhosis using a cooled needle. Radiol Med (Torino)1998;95:624-629.
26 Siperstein A, Garland A, Engle K et al. Laparoscopic radiofre-quency ablation of primary and metastatic liver tumors.Technical considerations. Surg Endosc 2000;14:400-405.
27 Solbiati L, Ierace T, Goldberg SN et al. Percutaneous US-guided radio-frequency tissue ablation of liver metastases:treatment and follow-up in 16 patients. Radiology1997;202:195-203.
28 Fong Y, Sun RL, Jarnagin W et al. An analysis of 412 casesof hepatocellular carcinoma at a Western center. Ann Surg1999;229:790-799.
29 Fong Y, Fortner J, Sun RL et al. Clinical score for predictingrecurrence after hepatic resection for metastatic colorectalcancer: analysis of 1001 consecutive cases. Ann Surg1999;230:309-318.
30 Patterson EJ, Scudamore CH, Owen DA et al. Radiofrequencyablation of porcine liver in vivo: effects of blood flow and treat-ment time on lesion size. Ann Surg 1998;227:559-565.
31 Clarke MP, Kane RA, Steele G Jr et al. Prospective com-parison of preoperative imaging and intraoperative ultra-sonography in the detection of liver tumors. Surgery1989;106:849-855.
32 Rahusen FD, Cuesta MA, Borgstein PJ et al. Selection ofpatients for resection of colorectal metastases to the liverusing diagnostic laparoscopy and laparoscopic ultrasonogra-phy. Ann Surg 1999;230:31-37.
33 Scudamore CH, Lee SI, Patterson EJ et al. Radiofrequencyablation followed by resection of malignant liver tumors. AmJ Surg 1999;177:411-417.
Related articles in The Oncologist:
Emerging New Opportunities for Patients with Hepatic Metastases from Colorectal Cancer orPrimary Hepatocellular Cancer. Pinedo HM, van Groeningen CJ. The Oncologist2001;6:12-13.
Radiofrequency Ablation of Malignant Liver Tumors. Curley S. The Oncologist 2001;6:14-23.
by guest on August 22, 2019
http://theoncologist.alphamedpress.org/
Dow
nloaded from