Embed Size (px)
Citation preview

1
Acute otitis media is different than otitis media with effusion (fluid in the middle ear, secretory otitis
media, serous otitis, “glue ear”) and chronic otitis media (chronic suppurative otitis media). People usually get acute otitis media with, or after, a cold.1 Chronic otitis
media is rare in developed countries, because in about 1930 we started treating ear infections with antibiotics. Before this, chronic otitis media was common, and often led to deafness and other complications.2
Diagnosis of acute otitis media
Acute otitis media is fluid in the middle ear combined with signs or symptoms of acute local or
systemic illness. The ear may hurt, or may drain fluid; or the patient may have fever.3 But the specifics for diagnosis are not so clear. In 26 clinical trials, there were 18 different sets of diagnostic criteria. One survey of 165 pediatricians resulted in 147 different sets of criteria!4 The 2013 AAP-AAFP guideline The Diagnosis and Man-agement of Acute Otitis Media5 provides the following advice on diagnosing otitis media, trying to standardize the diagnosis:
• Clinicians should [emphasis added] diagnose acute otitis media (AOM) in children who present with moderate to severe bulging of the tympanic mem-brane (TM) or new onset of otorrhea not due to acute otitis externa.
• Clinicians may [emphasis added] diagnose AOM in children who present with mild bulging of the TM and recent (less than 48 hours) onset of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM.
• Clinicians should not [emphasis added] diagnose AOM in children who do not have middle ear effu-sion (MEE) (based on pneumatic otoscopy and/or tympanometry).
Diagnosing a middle ear effusion is fairly easy. Do pneu-matic otoscopy. That’s where you use a soft ear speculum (to get a seal with the ear canal), with an insufflation bulb attached to the otoscope, and puff air into the ear. You look at the tympanic membrane (eardrum, TM) for position, color, translucency, and mobility.3 In one study, as confirmed by myringotomy (needle aspiration of the middle ear to get fluid), pneumatic otoscopy was 93% sensitive and 58% specific for effusion, which compares favorably with tympanometry (see below) which was 90% sensitive and 86% specific.6
A 2004 clinical guideline on otitis media with effusion (OME) says: Distinct redness of the TM should not be a criterion for antibiotic prescribing because it has poor pre-dictive value for acute otitis media and is present in about 5% of ears with OME.7 Screaming babies always have a red TM, and removing wax often makes the TM red.8 A retracted TM, which hurts, is from eustachian tube
dysfunction, and not a bacterial infection.1
A recent study recommended you diagnose acute otitis media with two or more of
• decreased or absent TM mobility,
• yellow or white discolor-ation of the TM,
• opacification of the TM not due to scarring, and
• visible bubbles or air-fluid levels.9
Another study correlated color, position and mobility with acute otitis media (diagnosed with myringotomy).10 A cloudy TM, and a bulging TM, and a TM with decreased mobil-ity (all three) correlated 99% with acute otitis media (see Table 1). You might want to get your own insufflation bulb (Welch-Allyn #23804), as it adds a lot to the accuracy of your diagnosis; I did. You need soft speculum sheaths to make a good seal with the external ear canal. The ED or clinic should supply these, though most don’t. I bought a
box of 80 of each size of the Welch Allyn SofSeal sheaths, 24330 (med) and 24320 (small), that fit the speculums of the Welch Allyn Macroview otoscopes in every ED and clinic in which I have worked for the past 10 years. It cost
Emergency Medicine Grand RoundsUpdated March 2013
Keith Conover, M.D., FACEP Otitis Media
Predictive Value (%)
Color Position Mobility
99 Cloudy Bulging Distinctly impaired
99 Cloudy Bulging Slightly impaired
97 Cloudy Normal Distinctly impaired
94 Distinctly red Bulging Distinctly impaired
94 Cloudy Normal Distinctly impaired
93 Slightly red Bulging Slightly impaired
89 Distinctly red Normal Distinctly impaired
85 Slightly red Bulging Distinctly impaired
83 Distinctly red Bulging Slightly impaired
47 Distinctly red Normal Slightly impaired
41 Slightly red Normal Slightly impaired
37 Cloudy Normal Normal
29 Normal Retracted Distinctly impaired
15 Distinctly red Normal Normal
7 Slightly red Normal Normal
3 Normal Retracted Slightly impaired
0.1 Normal Normal Normal
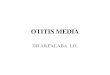
A, Normal TM. B, TM with mild bulging. C, TM with moderate bulging. D, TM with severe bulging. Courtesy of Alejandro Hoberman, MD.

2
$44.50/box from schoolhealth.com.
A machine that tells you if the patient has a middle ear effusion without digging the wax out of the ear of a squirming, screaming infant sounds good. Tympanom-etry uses such a device to assess for middle ear effusion. Since the early 1970s, tympanometers have been found in many ENT offices and pediatric offices and a few Emergency Departments. They’re easy to use, but results are a bit hard to figure out. Basic tympanometers mea-sure how much of a 226 Hz musical tone reflects back from the TM, as the air pressure in the external canal is varied, both above and below ambient air pressure. More modern tympanometers use a pair of musical tones. The tympanometer plots a pressure-versus-compliance curve on a graph known as a tympanogram. The interpretation of tympanograms is described in the medical literature and online but is beyond the scope of this handout.11,12 Tympanometry is no better than pneumatic otoscopy
for diagnosing a middle ear effusion.
Like using an insufflation bulb, tympanometry requires an airtight seal; however, spectral gradient acoustic reflec-tometry (SGAR), also known as acoustic reflectometry, does not. SGAR machines emit tones from 1.8 to 4.4 kHz, and measure how much is reflected. As with tym-panometry, accuracy depends on how experienced you are,13 though SGAR is easier than tympanometry.9
Neither tympanometry or SGAR is better than history, physical exam, and pneumatic otoscopy to diagnose acute otitis media.14 As Combs writes: “No technology can replace the careful history and otoscopic examina-tion by an experienced physician.”15
Physicians can’t diagnose acute otitis media by symp-toms alone. But parents can. Their sensitivity is 71% and their specificity is 80%.16
Antibiotics for acute otitis media?
Back in the 1980s, when I was a resident, I was taught that “any child with an earache has an acute
amoxicillin deficiency until proven otherwise.” In the USA, parents bringing an infant or child to you with an earache usually expect antibiotics. In Europe, though, they seldom get antibiotics.17,18 In the USA 95% of kids with acute otitis media get antibiotics; in the Nether-lands, it’s only 31-56%.19-21
Having acute otitis media before you’re 6 months old means you’re more likely to get recurrent acute otitis media later in life. But family history of allergy, breast-feeding, day care, gender, and home environment make no difference in how likely you are to get acute otitis media.22 Recurrent acute otitis media tends to resolve as children grow older.23 There is some evidence that, for children with recurrent episodes of acute otitis media, that prophylactic antibiotics, either throughout the cold season, or with onset of a viral upper respiratory infection, may help prevent acute otitis media.24 But the 2013 AAP-AAFP guidelines5 state: Clinicians should not prescribe prophylactic antibiotics to reduce the frequency
of episodes of AOM in children with recurrent AOM.
I was taught to prescribe anti-biotics for acute otitis media to decrease the incidence of deafness. However, permanent deafness comes primarily from chronic otitis media (2 or more weeks of otitis media with discharge) which is quite rare in North America; 25 acute otitis media does not cause permanent deafness, but it’s common to have a bit of tem-porary deafness from left-over fluid in the middle ear.26 Worse complications, such as perma-nent deafness or death from
brain infection, are rare outside the developing world.27
If we prescribe lots of antibiotics for red tympanic mem-branes, do we create resistant bacteria? Yes. Do we help or hurt the patient? We may be hurting the patient.28 An
immediate antibiotic decreases crying during the day and provides better sleep the first day. It decreases pain, but only slightly, and only on the second day of antibiot-ics, when symptoms are already improving. This small benefit may not outweigh complications such as diarrhea and creating resistant bacteria.29
It’s now OK to give a “safety-net antibiotic prescrip-tion,”30 and tell parents not to fill it unless the ear pain goes on for a couple of days. A lot of the time, parents don’t fill the prescription. Parents are happy and you’re creating fewer resistant bugs.30,31 Telling the parents to call back for a prescription in a couple of days has the same satisfaction rate, but seems to me as though it would work better for offices than EDs.32,33 Nobody has (yet) studied delayed antibiotics for adults.
The American Academy of Pediatrics and American Academy of Family Physicians 2013 joint clinical practice guideline5 says:
• The clinician should prescribe antibiotic therapy for AOM (bilateral or unilateral) in children 6 months and older with severe signs or symptoms (i.e., mod-erate or severe otalgia or otalgia for at least 48 hours or temperature 39°C [102.2°F] or higher).
• The clinician should prescribe antibiotic therapy for bilateral AOM in children 6 months through 23 months of age without severe signs or symptoms (i.e., mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]).
• The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision making with the parent(s)/caregiver for unilateral AOM in children 6 months to 23 months of age without severe signs or symptoms (i.e., mild otalgia for less than 48 hours and tem-perature less than 39°C [102.2°F]). When observa-tion is used, a mechanism must be in place to ensure follow-up and begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms.
• The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision-making with the parent(s)/

3
caregiver for AOM (bilateral or unilateral) in children 24 months or older without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]). When observation is used, a mechanism must be in place to ensure follow-up and begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms.
This may be summarized as: Treat with antibiotics if severe acute otitis media, or if nonsevere bilateral acute otitis media in young children. Treat with antibiotics or “observe” (no antibiotics and have patient call back if not improving, or provide a “safety net prescription”) if non-severe unilateral acute otitis media in young children, or if nonsevere acute otitis media in older children.
But there is a review of antibiotics for acute otitis media in children from the Cochrane Collaboration.34 Un-like the US-only AAP-AAFP guideline, it represents worldwide experts. It notes that antibiotics decrease pain only slightly and only for a couple of days, and, they don’t decrease temporary deafness, rupture of the TM, or mastoiditis. And, 37% of those who get antibiotics get vomiting, diarrhea or rash. So, the Cochrane Review says that you should prescribe antibiotics only if:
• there is bilateral acute otitis media, or• there is acute otitis media with otorrhea (dis-
charge from the ear).
So what do you do? I treat acute otitis media only if I’m absolutely sure it’s there and it looks bad, otherwise I just treat for eustachian tube dysfunction, with oxy-metazoline (AFRIN) nasal spray, as described below.
Bacteria that cause acute otitis media are often resistant to amoxicillin (particularly pneumococcus: Streptococ-cus pneumoniae). But amoxicillin is still the first-line antibiotic; it’s as good as other antibiotics, because the amoxicillin concentrates in middle ear fluid, enough to overcome the resistance.38,39 That is, if, instead of standard-dose amoxicillin (25-50 mg/kg/day divided
BID or TID; maximum 30 mg/kg/day if child is < 3 months old) you prescribe high-dose (80-90 mg/kg/day divided BID, though a conservative Cochran Review says to give TID35), for a full 7-10 days.36 A single shot of IM ceftriaxone, or 5 days of oral azithromycin, are good alternatives.37
The 2013 AAP-AAFP guidelines succinctly but confus-ingly states: Clinicians should prescribe amoxicillin for acute otitis media when a decision to treat with antibiotics has been made and the child has not received amoxicillin in the past 30 days or the child does not have concurrent purulent conjunctivitis or the child is not allergic to penicillin. When I’m not playing doctor I play computer nerd and think in Boolean logic, so I would reword it thusly: prescribe amoxicil-lin unless ((the child has had amoxicillin in the past 30 days) OR (the child has otitis-conjunctivitis syndrome) OR (the child is allergic to penicillins)).
If, after three days of an antibiotic, the patient still has, fever, ear pain, a red, bulging TM, or discharge from the ear, what do you do? High-dose amoxicillin–clavulanate (AUGMENTIN), or cefuroxime axetil (CEFTIN), or intramuscular ceftriaxone (ROCEPHIN) for three days.38 And if you see a patient with this in the ED, emphasize the need for primary-care follow-up!
Repeat episodes of acute otitis media (more than a month after the first time) is almost always (>90%) from a new virus or bacterium.39 Amoxicillin-clavulanate (AUGMENTIN) is probably appropriate at this point.
BTW, when a mother (it always seems to be the mother, not the father) says “amoxicillin never works for his/her ear infections!” I believe the mother. Some kids are probably colonized with highly amoxicillin-resistant bacteria. Our scientific studies are not good enough yet to tease out these outliers. So I prescribe something else, and call it the art of medicine.
Other Treatments for acute otitis media
Oral decongestants and antihistamines might help just slightly, but cause so many problems that
the cure is worse than the disease.40,41 And taking them during a cold doesn’t prevent acute otitis media.42
A decongestant nasal spray such as oxymetazoline (AF-RIN) helps a bit: ~19% residual effusion at one month as opposed to 27% residual effusion for oral decongestants, antihistamines, or untreated controls.41 I recommend a few days of oxymetazoline (AFRIN) nasal spray – less than 10 days – to avoid rhinitis medicamentosa, which
I describe as “being addicted to nasal spray so you have to use it to breathe through your nose.”43,44 I tell them to spray into both nostrils, then lie flat on their backs for a few minutes, so that they can taste the spray getting back to where the Eustachian tubes drain out in the back of the nose/throat.
Antipyrine and benzocaine ear drops (commonly known as AURALGAN, though no longer available under that brand name) may help the pain a bit.45,46
Otitis-Conjunctivitis Syndrome
Conjunctivitis and otitis media are sometimes occur together, and the combination is highly likely
to be caused by H influenzae;47 H. flu tends to be resistant to amoxicillin and azithromycin (ZITHROMAX). So, when treating otitis media, look for conjunctivitis; if you see it, consider amoxicillin-clavulanate (AUGMENTIN), cefuroxime (CEFTIN) or cefdinir (OMNICEF).48-52
For the same reason, if you see a child with purulent con-
junctivitis, take a look at the ears; roughly 2/3 will also have otitis media.53 Treat with an oral antibiotic, but you don’t need to prescribe eye drops. The tears have enough of the oral antibiotic to work as antibiotic eye drops.54
Normal Tympanic Membrane (Wikimedia Commons)

4
Otitis Media with Effusion (OME; “Glue Ear”; Serous Otitis; Middle Ear Effusion)
Sometimes people come to the ED with decreased hearing, sometimes sudden-onset. The most com-
mon cause is earwax impaction. But if you look in the ear, and rather than a cerumen impaction, you might see a clear effusion – fluid behind the tympanic membrane. Or, you might find the same on a routine ear exam.
Middle ear effusions are common after acute otitis media. Two weeks after they have otitis media, about ¾ of kids will have a persistent effusion; a month after, half will; and three months later, maybe ¼ will. Antibiotics don’t help.3,55,56
Serous otitis may also come from eustachian tube dysfunction (ETD) from other causes: chronic eusta-chian tube deformity, allergies,57 tobacco smoking and esophageal reflux.58 Less common causes include chronic sinus disease (particularly of the ethmoids), adenoidal hyperplasia, and rarely head and neck tumors.59 People with serous otitis may complain of a feeling of “water in the ear,” mild pain or decreased hearing. Serous otitis is defined as fluid in the middle ear without signs or symp-toms of ear infection. Like otitis media, it’s more com-mon in kids.7 Serous otitis is not a big deal in the ED, but it’s a big deal for pediatricians and family doctors, as decreased hearing causes problems in class.60
If you see a cloudy tympanic membrane, or a visible effusion with an air-fluid level, or bubbles behind the tympanic membrane, without symptoms of acute infec-tion, you’ve diagnosed serous otitis. Refer the patient to a primary care doctor for follow-up. It’s optional in the ED, but decreased mobility with insufflation confirms your diagnosis.61
Unfortunately, there is almost nothing we can do. Antibiotics, antihistamines, oral decongestants, oral ste-roids, mucolytics like guaifenesin (e.g., ROBITUSSIN, MUCINEX) and autoinflation with a Politzer device (don’t ask) are all useless.7,62-66 Some think that many cases of adult serous otitis are from allergies.67 Espe-cially in adults with obvious nasal allergies, a nonsedat-ing antihistamine and a steroid nasal spray might help. Since it may help acute otitis media,41 a short course of oxymetazoline (AFRIN) nasal spray – less than 10 days to avoid rhinitis medicamentosa – might help, too.43,44 As with acute otitis media, I recommend a few minute lying supine after spraying the nose. Refer to an appropri-ate primary care physician. However, warn the patient that “treatment” for kids with serous otitis is a three (3) month period of “watchful waiting,” checking hearing tests, and considering tympanostomy tubes.7
Acute otitis media With Tubes or Ruptured TM
Tympanostomy tubes (myringotomy tubes, venti-lation tubes, “grommets”) are sometimes surgically
inserted in the tympanic membranes of children with recurrent acute otitis media or, particularly in children > 3 years old, chronic otitis media with effusion (serous otitis). The tubes are expected to drain fluid for days or weeks after insertion. About 5% of children with tubes develop chronic otorrhea (drainage from the ear), usu-ally due to skin flora such as Pseudomonas aeruginosa and Staphylococcus aureus.68
You may be unsure if a patient has a hole in the tympanic membrane or not. A patient may have had tympanos-tomy tubes in the past, and you can’t tell if they are still there. And, sometimes, the pressure from acute otitis media will cause the tympanic membrane to rupture; this may fill the ear canal enough that it’s hard to tell if you’re dealing with otitis media with perforation or otitis externa.
Two clues to a perforated tympanic membrane are (1) people who can taste the drops after putting ear drops in their ear, and (2) people who can blow air out their ear when blowing their noses.69
You may see an infant or child with known tympanos-tomy tubes complaining of acute (sudden onset, severe) otorrhea. This occurs in roughly half of children with tubes.70 From the drainage, the external ear canal may look eczematous.69 The patient may have a low-grade temperature or fatigue, but due to the tubes, not much pain.
About a third of kids with acute otitis media have a spon-taneous rupture of the tympanic membrane during one of their episodes of otitis media, more likely if they’ve had prior otitis media. Usually the pain gets a lot better
when the tympanic membrane ruptures. Ninety-four percent of the perforations were spontaneously healed within a month. Children who have had a perforation are twice as likely to have recurrent acute otitis media.71
The bacteria in ear drainage in those under age 3 is the same as that in acute otitis media: a mixture of viruses and airway-derived bacteria.72,73 In older children, it will usually be skin flora including Pseudomonas aeruginosa and Staphylococcus aureus.74
There are many treatments for such ear drainage, from doing nothing (“observation”), through ear drops, to oral antibiotics. In children younger than 3 years old with acute tube-associated drainage, ear drops are as good as oral antibiotics; ofloxacin ear drops (FLOXIN) are as good as oral amoxicillin-clavulanate (AUGMEN-TIN).75 Given that ear drops are effective for tube-associ-ated and perforation-associated ear drainage in all ages, it seems prudent to use ear drops as the initial treatment, unless there is severe ear pain or high fever, in which case you should probably prescribe both ear drops (to cover skin bacteria) and one of the usual otitis media oral antibiotics.72,76
Prescribe only non-ototoxic eardrops when there might be a tube or perforation, as some of the ear drops may get into the middle ear.77 Neomycin and polymyxin B and hydrocortisone otic suspension (CORTISPORIN) contains both an ototoxic aminoglycoside (neomycin) as well as ototoxic propylene glycol; acetic acid ear drops (VOSOL, ACETASOL; VOSOL-HC, ACETASOL-HC) also contain ototoxic propylene glycol, as well as being acidic enough to make the middle ear hurt, so don’t prescribe them if there might be a tube or perforation, unless the benefits outweigh the risks. 77,78 Oflaxacin (FLOXIN) and ciprofloxacin/dexamethasone (CIPRO-

5
DEX) drops are non-ototoxic.78 Including a steroid with an antibiotic may make ear drops slightly more effective, but generic ofloxacin (FLOXIN) drops are both cheap and effective.79,80
If you see a child with tubes with discharge not improv-
ing with appropriate antibiotics, culture the drainage, but don’t change treatment. Refer for primary care physician follow-up and the physician may use culture results to guide treatment. If there is new ear pain or fever, and the patient is on just ear drops, start oral antibiotics.72
Mastoiditis and Petrositis
In the early 1900s, a fifth of those with acute otitis media got mastoiditis or petrositis. But since
antibiotics became available in the 1930s, they became rare (<1%), especially in the US and other developed nations.81
Mastoiditis is a symptomatic infection of the air cells in the bony mastoid process behind the ear, most com-monly in infants.82 Classic mastoiditis shows swelling and perhaps warmth or redness over the mastoid, with the pinna (auricle) pushed down and forwards. But soon after the first use of antibiotics for otitis media, in 1941, there were reports of “masked mastoiditis”: patients with further complications of mastoiditis, such as brain abscess, without classic signs and symptoms.83,84 Now, the most common findings are only seen with an otoscope: an abnormal appearing tympanic membrane, and sagging of the posterior wall of the external ear canal.2 Although the ear may not be visible displace, but sometimes the postauricular fold – the crease behind the pinna (auricle) of the ear – is gone; compare with the unaffected side.85
Trying to confirm a clinical suspicion of mastoiditis is hard, as there are no accepted diagnostic criteria.86 And, as with fluid in the sinuses on CT that occurs with most any cold,87-89 fluid in the mastoid air cells on CT scan doesn’t diagnose mastoiditis, as it’s found in many cases of otitis media.90 If you do a high-resolution CT or MRI and find bony resorption in the mastoid (the bony septae between the mastoid air cells are being destroyed) then you can diagnose “coalescent” mastoiditis, but CT or MRI won’t help you diagnose earlier stages of mastoid-itis.86,91,92
Patients with mastoiditis are generally admitted for
further workup and treatment. Myringotomy is usu-ally performed and tympanostomy tubes are generally placed. If there is neither subperiosteal abscess nor CNS involvement, a period of 48 hours of observation and broad-spectrum IV antibiotics is recommended prior to considering mastoidectomy.93 Subperiosteal abscesses are surgically drained.
The triad of deep facial pain, otitis media, and ipsilat-eral abducens nerve paralysis (inability to look to the affected side) are the classic signs of petrositis (infection of the petrous portion of the temporal bone; Gradenigo’s Syndrome)94 However, as with mastoiditis, such classic presentations are now rare. If you see someone who presents with deep facial pain and signs or symptoms of infection, and a history of chronic otitis media or surgery for mastoiditis, you should suspect petrositis.95 Get a CT or MRI scan, and consider admitting the patient for further workup and treatment. A CT scan showing bony changes in the petrous part of the temporal bone clinches the diagnosis.95 Mastoidectomy is a common inpatient treatment, but conserva-tive management with just antibiotics is reasonable as well.96-98
Bullous Myringitis
I was taught that bullous myringitis – tiny blisters on the tympanic membrane – clinches the diagnosis
mycoplasma-induced otitis media.99 But the bacteria in ears with bullous myringitis are basically the same as in any case of acute otitis media,100 though bullous
myringitis hurts worse than other types of acute otitis media.100 As one review put it, bullous myringitis is just acute otitis media with blisters on the eardrum.99
References1. Hendley JO. Clinical practice. Otitis media. N Engl J Med 2002;347:1169-74.2. Fliss DM, Leiberman A, Dagan R. Medical sequelae and complications of acute otitis media. Pediatr Infect Dis J 1994;13:S34-40; discussion S50-4.3. Dowell SF, Marcy SM, Phillips WR, Gerber MA, Schwartz B. Otitis Media—Principles of Judicious Use of Antimicro-bial Agents. Pediatrics 1998;101:165-71.4. Hayden GF. Acute suppurative otitis media in children. Diversity of clinical diagnostic criteria. Clin Pediatr (Phila) 1981;20:99-104.5. Lieberthal AS, Carroll AE, Chon-
maitree T, et al. The diagnosis and man-agement of acute otitis media. Pediatrics 2013;131:e964-99.6. Finitzo T, Friel-Patti S, Chinn K, Brown O. Tympanometry and otoscopy prior to myringotomy: issues in diagnosis of otitis media. International journal of pediatric otorhinolaryngology 1992;24:101-10.7. Rosenfeld RM, Culpepper L, Doyle KJ, et al. Clinical practice guideline: Otitis media with effusion. Otolaryngol Head Neck Surg 2004;130:S95-118.8. Weiss JC, Yates GR, Quinn LD. Acute otitis media: making an ac-
curate diagnosis. Am Fam Physician 1996;53:1200-6.9. Chianese J, Hoberman A, Paradise JL, et al. Spectral gradient acoustic reflec-tometry compared with tympanometry in diagnosing middle ear effusion in children aged 6 to 24 months. Arch Pediatr Adolesc Med 2007;161:884-8.10. Pelton SI. Otoscopy for the diagnosis of otitis media. Pediatr Infect Dis J 1998;17:540-3; discussion 80.11. Popelka GR. Acoustic immittance measures: terminology and instrumenta-tion. Ear and hearing 1984;5:262-7.12. Tympanometry. ASHA Working
Group on Aural Acoustic-Immittance Measurements Committee on Audiologic Evaluation. The Journal of speech and hearing disorders 1988;53:354-77.13. Kimball S. Acoustic reflectometry: spectral gradient analysis for improved detection of middle ear effusion in chil-dren. Pediatr Infect Dis J 1998;17:552-5; discussion 80.14. Stewart MH, Siff JE, Cydulka RK. Evaluation of the patient with sore throat, earache, and sinusitis: an evidence based approach. Emergency medicine clinics of North America 1999;17:153-87, ix.15. Combs JT. The diagnosis of otitis
Key Points• Chronic suppurative otitis
media, which causes serious long-term problems, occurs almost entirely in the devel-oping world.
• You should diagnose acute otitis media by:
· signs and symptoms of acute otitis media (fever, earache); and
· evidence of a middle ear effusion.
• You should diagnose a middle ear effusion when you see:
· fluid behind the tympanic membrane, or
· decreased mobility with insufflation , or
· opacity or discoloration of tympanic membrane (not counting scarring), or
· evidence from tympanom-etry or spectral gradient acoustic reflectometry.
• Do not diagnose acute otitis media when you just see redness of the tympanic membrane.
• Should you treat acute otitis media with antibiotics? Maybe. There are dueling recommendations.
• You can, for certain kids with acute otitis media, give a prescription for an antibiotic but tell the parents not to fill it unless the ear is still hurting in
a couple of days.
• High-dose amoxicillin, due to high concentrations in the middle ear that will kill even resistant organisms, is still the drug of choice for acute otitis media.
• Although nasal-spray decon-gestants may help acute otitis media, oral decongestant and antihistamines are not recom-mended (don’t help much or at all, lots of side effects).
• Otitis-Conjunctivitis Syn-drome is usually from H influ-enzae; prescribe Augmentin rather than amoxicillin.
• For otitis media with effusion (serous otitis), no acute treat-ments work, except maybe decongestant nasal spray, or if allergic, steroid nasal spray. It is simply observed for months for resolution.
• For acute otitis media with tympanostomy tubes or a rup-tured tympanic membrane, treat not with oral antibiotics, but with non-ototoxic ear drops such as ofloxacin or ciprofloxacin.
• Mastoiditis and petrositis (Gradenigo’s Syndrome) are quite rare in the developed world, and while CT or MRI may help a bit, you have to make the initial diagnosis clinically.

6
media: new techniques. Pediatr Infect Dis J 1994;13:1039-46.16. Kontiokari T, Koivunen P, Niemela M, Pokka T, Uhari M. Symptoms of acute otitis media. Pediatr Infect Dis J 1998;17:676-9.17. Del Mar C, Glasziou P, Hayem M. Are antibiotics indicated as initial treat-ment for children with acute otitis media? A meta-analysis. BMJ 1997;314:1526-9.18. Van Zuijlen DA, Schilder AG, Van Balen FA, Hoes AW. National differences in incidence of acute mastoiditis: relation-ship to prescribing patterns of antibiotics for acute otitis media? Pediatr Infect Dis J 2001;20:140-4.19. Akkerman AE, Kuyvenhoven MM, van der Wouden JC, Verheij TJ. Analysis of under- and overprescribing of antibiotics in acute otitis media in general practice. J Antimicrob Chemother 2005;56:569-74.20. Froom J, Culpepper L, Grob P, et al. Diagnosis and antibiotic treatment of acute otitis media: report from Inter-national Primary Care Network. BMJ 1990;300:582-6.21. Froom J, Culpepper L, Green LA, et al. A cross-national study of acute otitis media: risk factors, severity, and treatment at initial visit. Report from the Interna-tional Primary Care Network (IPCN) and the Ambulatory Sentinel Practice Network (ASPN). J Am Board Fam Pract 2001;14:406-17.22. Harsten G, Prellner K, Heldrup J, Kalm O, Kornfalt R. Recurrent acute oti-tis media. A prospective study of children during the first three years of life. Acta Otolaryngol 1989;107:111-9.23. Alho OP, Laara E, Oja H. What is the natural history of recurrent acute otitis media in infancy? The Journal of family practice 1996;43:258-64.24. Berman S. Otitis media in children. N Engl J Med 1995;332:1560-5.25. Davidson J, Hyde ML, Alberti PW. Epidemiologic patterns in childhood hearing loss: a review. International journal of pediatric otorhinolaryngology 1989;17:239-66.26. Berman S. Otitis media in developing countries. Pediatrics 1995;96:126-31.27. Acuin J. Chronic suppurative otitis media: Burden of Illness and Manage-ment Options. Geneva, Switzerland: World Health Organization; 2004.28. Bluestone CD. Otitis media in children: to treat or not to treat? N Engl J Med 1982;306:1399-404.29. Little P, Gould C, Williamson I, Moore M, Warner G, Dunleavey J. Prag-matic randomised controlled trial of two prescribing strategies for childhood acute otitis media. BMJ 2001;322:336-42.30. Cates C. An evidence based approach to reducing antibiotic use in children with acute otitis media: controlled before and after study. BMJ 1999;318:715-6.31. Siegel RM, Kiely M, Bien JP, et al. Treatment of otitis media with observa-tion and a safety-net antibiotic prescrip-tion. Pediatrics 2003;112:527-31.32. Chao JH, Kunkov S, Reyes LB, Lichten S, Crain EF. Comparison of two approaches to observation therapy for acute otitis media in the emergency department. Pediatrics 2008;121:e1352-6.33. McCormick DP, Chonmaitree T, Pittman C, et al. Nonsevere acute otitis media: a clinical trial comparing outcomes of watchful waiting versus immediate antibiotic treatment. Pediatrics 2005;115:1455-65.34. Sanders SL, Glasziou PP, Del Mar CB, Rovers MM. Antibiotics for acute otitis media in children. Cochrane database of systematic reviews (Online) 2010:CD000219.35. Thanaviratananich S, Laopaiboon M, Vatanasapt P. Once or twice daily versus three times daily amoxicillin with or without clavulanate for the treatment of acute otitis media. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2008.36. Kozyrskyj A, Klassen TP, Moffatt M, Harvey K. Short-course antibiot-ics for acute otitis media. Cochrane database of systematic reviews (Online) 2010:CD001095.
37. Takata GS, Chan LS, Shekelle P, Morton SC, Mason W, Marcy SM. Evi-dence assessment of management of acute otitis media: I. The role of antibiotics in treatment of uncomplicated acute otitis media. Pediatrics 2001;108:239-47.38. Dowell SF, Butler JC, Giebink GS, et al. Acute otitis media: management and surveillance in an era of pneumococcal resistance--a report from the Drug-resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J 1999;18:1-9.39. Leibovitz E, Greenberg D, Piglansky L, et al. Recurrent acute otitis media oc-curring within one month from comple-tion of antibiotic therapy: relationship to the original pathogen. Pediatr Infect Dis J 2003;22:209-16.40. Coleman C, Moore M. Decon-gestants and antihistamines for acute otitis media in children. Cochrane database of systematic reviews (Online) 2007:CD001727.41. Eyibilen A, Aladag I, Guven M, Koc S, Gurbuzler L. The effectiveness of nasal decongestants, oral decongestants and oral decongestant-antihistamines in the treatment of acute otitis media in chil-dren. Kulak burun bogaz ihtisas dergisi : KBB = Journal of ear, nose, and throat 2009;19:289-93.42. Randall JE, Hendley JO. A decongestant-antihistamine mixture in the prevention of otitis media in children with colds. Pediatrics 1979;63:483-5.43. Taverner D, Latte GJ. Nasal decon-gestants for the common cold. Cochrane Database of Systematic Reviews. Chich-ester, UK: John Wiley & Sons, Ltd; 2009.44. Eccles R, Martensson K, Chen SC. Effects of intranasal xylometazoline, alone or in combination with ipratropium, in patients with common cold. Curr Med Res Opin 2010.45. Hoberman A, Paradise JL, Reynolds EA, Urkin J. Efficacy of Auralgan for treating ear pain in children with acute otitis media. Arch Pediatr Adolesc Med 1997;151:675-8.46. Foxlee R, Johansson A, Wejfalk J, Dawkins J, Dooley L, Del Mar C. Topical analgesia for acute otitis media. Cochrane database of systematic reviews (Online) 2006:CD005657.47. Bodor FF, Marchant CD, Shurin PA, Barenkamp SJ. Bacterial etiology of conjunctivitis-otitis media syndrome. Pediatrics 1985;76:26-8.48. Bingen E, Cohen R, Jourenkova N, Gehanno P. Epidemiologic study of conjunctivitis-otitis syndrome. Pediatr Infect Dis J 2005;24:731-2.49. Bodor FF. Systemic antibiotics for treatment of the conjunctivitis-otitis media syndrome. Pediatr Infect Dis J 1989;8:287-90.50. Harrison CJ, Hedrick JA, Block SL, Gilchrist MJ. Relation of the outcome of conjunctivitis and the conjunctivitis-otitis syndrome to identifiable risk factors and oral antimicrobial therapy. Pediatr Infect Dis J 1987;6:536-40.51. Gigliotti F, Williams WT, Hayden FG, et al. Etiology of acute conjunctivitis in children. J Pediatr 1981;98:531-6.52. Gilbert DN. The Sanford guide to antimicrobial therapy 2011. Sperryville, VA: Antimicrobial Therapy, Inc.; 2011.53. Bodor FF. Conjunctivitis-otitis syndrome. Pediatrics 1982;69:695-8.54. Nelson JD, Ginsburg CM, McLeland O, Clahsen J, Culbertson MC, Jr., Carder H. Concentrations of antimicrobial agents in middle ear fluid, saliva and tears. International journal of pediatric otorhinolaryngology 1981;3:327-34.55. Teele DW, Klein JO, Rosner B. Epi-demiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study. J Infect Dis 1989;160:83-94.56. Teele DW, Klein JO, Rosner BA. Epidemiology of otitis media in children. Ann Otol Rhinol Laryngol Suppl 1980;89:5-6.57. Bluestone CD. Eustachian tube func-tion and allergy in otitis media. Pediatrics 1978;61:753-60.58. Bluestone CD, Hebda PA, Alper CM, et al. Recent advances in otitis me-
dia. 2. Eustachian tube, middle ear, and mastoid anatomy; physiology, pathophysi-ology, and pathogenesis. Ann Otol Rhinol Laryngol Suppl 2005;194:16-30.59. Finkelstein Y, Ophir D, Talmi YP, Shabtai A, Strauss M, Zohar Y. Adult-onset otitis media with effusion. Arch Otolaryngol Head Neck Surg 1994;120:517-27.60. Klein JO. Otitis media. Clin Infect Dis 1994;19:823-33.61. American Academy of Pediatrics Subcommittee on Management of Acute Otitis M. Diagnosis and manage-ment of acute otitis media. Pediatrics 2004;113:1451-65.62. Perera R, Haynes J, Glasziou P, Heneghan CJ. Autoinflation for hearing loss associated with otitis media with effusion. Cochrane database of systematic reviews (Online) 2006:CD006285.63. Simpson SA, Lewis R, van der Voort J, Butler CC. Oral or topical nasal steroids for hearing loss associated with otitis media with effusion in children. Cochrane database of systematic reviews (Online) 2011:CD001935.64. van Zon A, van der Heijden GJ, van Dongen TM, Burton MJ, Schilder AG. Antibiotics for otitis media with effusion in children. Cochrane database of system-atic reviews (Online) 2012;9:CD009163.65. Griffin G, Flynn CA. Antihistamines and/or decongestants for otitis media with effusion (OME) in children. Cochrane database of systematic reviews (Online) 2011:CD003423.66. van der Merwe J, Wagenfeld DJ. The negative effects of mucolytics in otitis media with effusion. S Afr Med J 1987;72:625-6.67. Bernstein JM. Role of allergy in eustachian tube blockage and otitis media with effusion: a review. Otolaryngol Head Neck Surg 1996;114:562-8.68. McLelland CA. Incidence of compli-cations from use of tympanostomy tubes. Archives of otolaryngology 1980;106:97-9.69. Rosenfeld RM, Brown L, Cannon CR, et al. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg 2006;134:S4-23.70. Gates GA, Avery C, Prihoda TJ, Holt GR. Delayed onset post-tympanot-omy otorrhea. Otolaryngol Head Neck Surg 1988;98:111-5.71. Berger G. Nature of spontaneous tympanic membrane perforation in acute otitis media in children. The Journal of laryngology and otology 1989;103:1150-3.72. Granath A, Rynnel-Dagoo B, Back-heden M, Lindberg K. Tube associated otorrhea in children with recurrent acute otitis media; results of a prospective ran-domized study on bacteriology and topical treatment with or without systemic anti-biotics. International journal of pediatric otorhinolaryngology 2008;72:1225-33.73. Ruohola A, Meurman O, Nikkari S, et al. Microbiology of acute otitis media in children with tympanostomy tubes: prevalences of bacteria and viruses. Clin Infect Dis 2006;43:1417-22.74. Mandel EM, Casselbrant ML, Kurs-Lasky M. Acute otorrhea: bacteriology of a common complication of tympanos-tomy tubes. Ann Otol Rhinol Laryngol 1994;103:713-8.75. Goldblatt EL. Efficacy of ofloxacin and other otic preparations for acute otitis media in patients with tympanostomy tubes. Pediatr Infect Dis J 2001;20:116-9; discussion 20-2.76. Roland PS, Parry DA, Stroman DW. Microbiology of acute otitis media with tympanostomy tubes. Otolaryngol Head Neck Surg 2005;133:585-95.77. Saunders MW, Robinson PJ. How easily do topical antibiotics pass through tympanostomy tubes?--an in vitro study. International journal of pediatric otorhi-nolaryngology 1999;50:45-50.78. Daniel SJ, Munguia R. Ototoxicity of topical ciprofloxacin/dexamethasone otic suspension in a chinchilla animal model. Otolaryngol Head Neck Surg 2008;139:840-5.79. Emgard P, Hellstrom S, Holm S. External otitis caused by infection with
Pseudomonas aeruginosa or Candida albicans cured by use of a topical group III steroid, without any antibiotics. Acta Otolaryngol 2005;125:346-52.80. Emgard P, Hellstrom S. A topical steroid without an antibiotic cures exter-nal otitis efficiently: a study in an animal model. Eur Arch Otorhinolaryngol 2001;258:287-91.81. Smeraldi R. Clinica e diagnosi di alcune mastoiditi atipichi Gazz Sanitar 1947;18:58-61.82. Groth A, Enoksson F, Hultcrantz M, Stalfors J, Stenfeldt K, Hermansson A. Acute mastoiditis in children aged 0-16 years-A national study of 678 cases in Sweden comparing different age groups. International journal of pediatric otorhi-nolaryngology 2012.83. Holt GR, Gates GA. Masked mas-toiditis. Laryngoscope 1983;93:1034-7.84. Hutchinson CA. Chemotherapy in Acute Middle-ear Disease: “Masked Mastoiditis”. Br Med J 1941;2:159-60.85. Beers SL, Abramo TJ. Otitis externa review. Pediatr Emerg Care 2004;20:250-6.86. van den Aardweg MT, Rovers MM, de Ru JA, Albers FW, Schilder AG. A systematic review of diagnostic criteria for acute mastoiditis in children. Otol Neurotol 2008;29:751-7.87. Schwartz RH, Pitkaranta A, Winther B. Computed tomography imaging of the maxillary and ethmoid sinuses in children with short-duration purulent rhinorrhea. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery 2001;124:160-3.88. Gwaltney JM, Jr., Phillips CD, Miller RD, Riker DK. Computed tomographic study of the common cold. The New Eng-land journal of medicine 1994;330:25-30.89. Kaiser L, Lew D, Hirschel B, et al. Effects of antibiotic treatment in the subset of common-cold patients who have bacteria in nasopharyngeal secretions. Lancet 1996;347:1507-10.90. Dhooge IJ, Vandenbussche T, Lemmerling M. Value of computed tomography of the temporal bone in acute otomastoiditis. Revue de laryngologie - otologie - rhinologie 1998;119:91-4.91. Antonelli PJ, Garside JA, Mancuso AA, Strickler ST, Kubilis PS. Computed tomography and the diagnosis of coales-cent mastoiditis. Otolaryngol Head Neck Surg 1999;120:350-4.92. Vazquez E, Castellote A, Piqueras J, et al. Imaging of complications of acute mastoiditis in children. Radiographics : a review publication of the Radiological So-ciety of North America, Inc 2003;23:359-72.93. Nadal D, Herrmann P, Baumann A, Fanconi A. Acute mastoiditis: clinical, microbiological, and therapeutic aspects. Eur J Pediatr 1990;149:560-4.94. Gradenigo G. Über die paralyse des nervus abducens bei otitis. Arch Ohren-heilunde 1907;774:149–87.95. Chole RA, Donald PJ. Petrous apicitis. Clinical considerations. Ann Otol Rhinol Laryngol 1983;92:544-51.96. Marianowski R, Rocton S, Ait-Amer JL, Morisseau-Durand MP, Manach Y. Conservative management of Grad-enigo syndrome in a child. International journal of pediatric otorhinolaryngology 2001;57:79-83.97. Rossor TE, Anderson YC, Steventon NB, Voss LM. Conservative management of Gradenigo’s syndrome in a child. BMJ case reports 2011;2011.98. Ulkumen B, Kaplan Y. Conservative treatment of Gradenigo’s syndrome trig-gered by acute otitismedia. Pak J Med Sci Q 2012;28:735-7.99. Roberts DB. The etiology of bullous myringitis and the role of mycoplas-mas in ear disease: a review. Pediatrics 1980;65:761-6.100. McCormick DP, Saeed KA, Pittman C, et al. Bullous myringitis: a case-control study. Pediatrics 2003;112:982-6.
g
This work is licensed under the Creative Commons Attribution-Share Alike 3.0 United States License. To view a copy of this license, visit http://creativecom-mons.org/licenses/by-sa/3.0/us/ or send a letter to Creative Com-mons, 171 Second Street, Suite 300, San Francisco, California, 94105, USA.
This license lets others remix, tweak, and build upon your work even for commercial purposes, as long as they credit you and license their new creations under the identical terms. This license is often compared to “copyleft” free and open source software licenses. All new works based on yours will carry the same license, so any derivatives will also allow commercial use. This is the license used by Wikipedia, and is recom-mended for materials that would benefit from incorporating con-tent from Wikipedia and similarly licensed projects.
Set in Adobe Myriad and Text in InDesign
This document may be downloaded from www.conovers.org/ftp