Embed Size (px)
Citation preview

Home Care o f Your Chi ld a f t e r an Ostomy
Home Care of Your Child After an Ostomy
Guidelines for Parents

Home Care o f Your Chi ld a f t e r an Ostomy 1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Normal Digestion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Types of Ostomies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Ileostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Colostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Stomas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6What is a stoma? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Normal appearance of the stoma . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Types of Stomas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7End ostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Loop ostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Double-barrel ostomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Ostomy Pouches and Skin Care . . . . . . . . . . . . . . . . . . . . . . 8Types of pouches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Components of a pouching system . . . . . . . . . . . . . . . . . . . . . . . . . 8One-piece pouching process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Two-piece pouching process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Pouching Pointers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
The Importance of Pouch and Skin Care . . . . . . . . . . . . . . . . . . 9
Emptying and Cleaning the Ostomy Pouch . . . . . . . . . . . . . . . . . 10Step-by-step procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Helpful Tips . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Potential Complications . . . . . . . . . . . . . . . . . . . . . . . . . . 12Retraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Prolapse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Parastomal hernia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Stenosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Laceration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Irritant dermatitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Yeast infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Folliculitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Dehydration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Risk of dehydration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Signs and symptoms of dehydration . . . . . . . . . . . . . . . . . . . . . . . 15
Other Daily Care Tips . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Activities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Clothing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Nutrition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Food Lists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Foods that may have various effects on the stool . . . . . . . . . . . . . . . . . . 17
Helpful Tips by Age Group . . . . . . . . . . . . . . . . . . . . . . . . . 18Infants (1 – 12 months) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Toddlers (12 – 36 months) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Preschoolers (3 – 5 years) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18School-age children (6 – 11 years) . . . . . . . . . . . . . . . . . . . . . . . . . 18Adolescents (12 – 18 years) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Contents
Home Care o f Your Chi ld a f t e r an Ostomy 1

2
Your child’s condition has required an ostomy. An ostomy is an
opening in the abdominal wall created to divert body waste into a
pouch. The surgeon creates an ostomy by bringing part of the bowel
or urinary tract through the abdominal wall. The visible portion of the
ostomy is called a stoma.
There are many different conditions or reasons for creating an
ostomy. Some of the conditions that would require an ostomy are
Hirschsprung’s disease, imperforate anus, meconium ileus, necrotizing
enterocolitis, and pseudo-membranous enterocolitis. Your doctor will
discuss with you why an ostomy was necessary for your child. Ostomies
can be permanent, but in infants and children are often created as a
temporary solution to a medical problem. This allows time for your child’s
bowel to heal or grow before corrective surgery may be performed.
How will I learn to care for my child? You may feel frightened
and overwhelmed with your child’s need for an ostomy. After the
surgery, you may also feel anxious about taking care of the ostomy
at home. This is normal; most parents feel this way. To help assure
you before you leave the hospital, a specially trained nurse — an
enterostomal therapist (ET) — will teach you the step-by-step
procedures for changing and cleaning the ostomy pouch.
What is the purpose of this handbook? This handbook is provided
as a resource for you to use as you learn in the hospital, and for
your reference at home. Before going into detail about your
child’s type of ostomy and home care instructions, we start with an
overview of normal digestion. This is so that you can understand a
little bit more about how an ostomy works, and why some of the
care instructions we provide are important.
The instructions in this booklet are intended as guidelines only.
Your surgeon may change the recommendations given in this
booklet based on the particular needs of your child. Always follow
your physician’s instructions.
Pl ea s e a s k qu e s t i on s ! Asking questions along the way
is the best way to learn.
Introduction

Home Care o f Your Chi ld a f t e r an Ostomy 3
Normal Digestion
Pl ea s e a s k qu e s t i on s !
Before discussing how to care for your child after an ostomy, let us review the normal digestion process . Knowing how normal digestion occurs will help you understand why stool consistency, skin care, and other daily care instructions are so important for your child .
Digestion is the breakdown of food into very small pieces for the body to use as energy . Digestion starts in the mouth with the chewing action of the teeth . Food particles are then swallowed down the esophagus into the stomach .
In the stomach, food particles mix with enzymes (digestive juices) . Next, the food empties into the small intestine (also called the small bowel) where further breakdown of food occurs . It is in the small intestine that your body begins to absorb nutrients .
At the end of the small bowel, water and stool (waste material)
pass through the colon (large intestine) . Mucous is produced throughout the bowel to help the stool move through the
bowel . The colon is where water is absorbed and the stool is stored until it is eliminated through the rectum and anus (the opening to the outside of the body) .

Ileostomy
Ascending Colostomy
Transverse Colostomy
Sigmoid Colostomy
Colostomy
Ileostomy
4
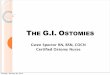
Types of OstomiesThere are two basic types
of ostomies:
• Ileostomy
• Colostomy
Ileostomy
An ileostomy is an ostomy located in the small intestine (small bowel) area . Stool here will be loose and watery . There is minimal odor and gas may or may not be present .
Colostomy
A colostomy is an ostomy located in the large intestine or colon . A colostomy is called ascending, transverse, or sigmoid, depending on the area of the large intestine in which it is located .
Ascending Colostomy
An ascending colostomy is located in the ascending section of the large intestine or colon area . Stool here will be loose to watery . Gas and odor are present .
Transverse Colostomy
A transverse colostomy is located in the transverse section of the large intestine or colon area . Stool here will be loose . Gas and odor will be present .
Sigmoid Colostomy
A sigmoid colostomy is located in the sigmoid section of the large intes-tine or colon area . Stool here will be formed and soft . Gas and odor will be present .

Ascending Colostomy
Transverse Colostomy
Sigmoid Colostomy
Home Care o f Your Chi ld a f t e r an Ostomy 5
Ostomy with a pouch
The location of the ostomy and
the type of pouching system used
vary from child to child.

Normal stoma Stoma slightly swollen
6
What is a stoma?
The stoma is the visible opening of the ostomy . It is the portion of the intestine that was surgically brought out to the skin through the opening in the abdominal wall that was made during your child’s ostomy surgery . It is important to learn and recognize what the normal appearance of the stoma is, especially for the type of stoma your child has .
Normal appearance of the stoma
The stoma should be a pink/red color and should be moist . Touching the stoma will not be painful for your child . You might notice that the stoma has some motion . This is the normal motion of the bowel, called “peristalsis,” that moves the stool through the bowel .
The stoma will be swollen for six to eight weeks after the operation . Over time, its size will decrease . The stoma may bleed easily if it is handled roughly . If the stoma has a large amount of bleeding, gently apply pressure to the area with your clean finger . If it does not stop within five minutes, call your doctor or surgeon .
Shortly after surgery, you may notice dark black tissue around the stoma . This is necrotic (dead) tissue . (The Loop Ostomy picture on the follow-ing page shows some necrotic tissue .)
Once the necrotic tissue has sloughed off (shed), the stoma will be shaped differently . Generally, the sloughing is completed before your child goes home . Once you are home, if the stoma becomes dark in color, call your surgeon .
Stomas

Home Care o f Your Chi ld a f t e r an Ostomy 7
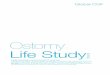
End ostomy
An end ostomy has one stoma . This picture shows a normal, healthy, pink end stoma .
Loop ostomy
The loop ostomy has two openings in one stoma . In this picture, the dark area around the base of the stoma is necrotic (dead) tissue . A supportive device called a rod or a bridge is placed to hold the bowel above skin level until the abdominal wall has healed . The rod will be in place for five days to two weeks .
Double-barrel ostomy
In a double-barrel ostomy, there are two stomas . When the bowel is divided, both ends are brought to the skin surface . One end permits passage of stool; the other is an outlet for mucous . A mucous fistula (non-functioning stoma) may be created to allow mucous to drain from a non-functioning bowel part .
Types of Stomas
Diagrams above show cross sections
of bowel and stoma
End ostomy
Loop ostomy
Double-barrel ostomy

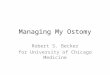
Two- Piece Ostomy bag One- Piece Ostomy bag
8
One-piece pouching system
Types of pouches
There are many types and sizes of pouches available. They fall into two basic categories:
• One-piece pouch (skin barrier and pouch are attached)
• Two-piece pouch (skin barrier and pouch are separate)
Many of these systems require cut-ting the skin barrier to fit the stoma
Components of a
pouching system
• Skin barrier (also called a wafer): attaches to the pouch and protects the skin
• Pouch: collects output and captures odor
Optional items:
• Tape: secures the pouch to the skin
• Stoma paste: caulking for gaps and creases on the skin
4Cut the shape being careful not to
puncture the pouch
5Apply the pouch by peeling the backing
from the skin barrier
6 Gently press to ensure good contact with
the skin
08 cut one-piece
09 Peel one-piece
10 Press down one-piece
Two- Piece Ostomy bag One- Piece Ostomy bag
Two-piece pouching system
One-piece pouching process
1Make sure the skin around the stoma is
clean and dry (Do not use lotion, soap, or
oils that will interfere with adhesion)
Prepare the pouch by doing the following:
2Use guide to measure the stoma
3 Trace measured shape on to the
skin barrier
01. Clean the stoma
02 Measure stoma
03 Trace two-piece
Ostomy Pouches and Skin Care

Home Care o f Your Chi ld a f t e r an Ostomy 9
Two-piece pouching process
1Make sure the skin around the stoma is
clean and dry (Do not use lotion, soap, or
oils that will interfere with adhesion)
Prepare the skin barrier (also called a wafer) by doing the following:
2Use guide to measure the stoma
3 Trace measured shape on to the
skin barrier
01. Clean the stoma
02 Measure stoma
03 Trace two-piece
4Cut out the shape
5Apply the skin barrier by peeling the back-
ing from the skin barrier and gently press-
ing to ensure good contact with the skin.
6 Apply pouch to the skin barrier by placing
the lower edge of the pouch flange against
the lower portion of the skin barrier.
7Press both pieces together while moving upward and then back down. Gently tug downward on the pouch to assure it is
properly attached.
04 Cut two-piece
05 Peel two-piece
06 stick on two-piece
POuching POinTerS
Clean the surrounding skin with
warm water and a washcloth.
It is not necessary to use soap but if
soap is used it should be very mild.
Avoid cleansers or moisturizers that
contain oils deodorants or perfumes.
This may cause skin problems and
prevent the barrier from sticking.
Warm the skin barrier before and af-
ter application for better adhesion.
Do not use stoma paste as an ad-
hesive. It will not adhere and may
cause skin irritation. Use only as a
“caulking” next to the stoma to fill
the creases in the skin.
The iMPOrTance Of POuch
and Skin care Proper pouch and skin care help you
meet the goals of caring for a child
with an ostomy, which are to:
• maintainnormalbowelfunction
• protecttheskinfromwastematerial
• controlodorandmaintaincleanli-
ness by collecting waste material.
Good skin care around the stoma
includes keeping the skin
around the stoma clean and dry.
Ill-fitting pouches that allow
stool to leak onto the skin can
cause skin problems. It is
important to keep a good seal on
the pouch so stool will not leak
onto the skin.

10
Step-by-step procedure
empty the pouch when it is ⅓ full of air or stool, or earlier if the pouch begins pulling away from the skin. if stool or air is allowed to build up, the pouch will balloon and break the seal or pull away from the skin.
Odor should not be a problem if the end of the pouch and the clamp are kept clean.
Odor should be noticeable only when changing and emptying the pouch, or if the pouch is leaking. if odor is a problem, odor reducers are available to put in the pouch.
To empty and clean the pouch, use a
container, diaper, or catheter-tipped
syringe. You will also need a bottle of
mild soap or water.
1.Pour the stool into the container or dia-
per, or withdraw stool into the syringe.
2.Use room temperature tap
water (1-2 ounces) and a small
amount of mild soap (1-2 sprays) to
clean the pouch. Pour water into the
pouch, swish the water around, and
then remove water by using a contain-
er, diaper, or syringe.
Step 2 is optional
Emptying and Cleaning the Ostomy Pouch

Home Care o f Your Chi ld a f t e r an Ostomy 11
3. Use toilet paper or paper towel to dry the
last 2-3 inches of the inside and
outside of the pouch.
4. Press air out of the pouch and replace
the clamp.
5.If stool is on the clamp, wash it before
reusing it.
helPful TiPS To help the pouch-emptying process, place the bag on your child so it drapes off to the side of your child’s body. Once your child is toilet trained, put the bag on so it hangs down your child’s leg. The pouch can then drain into the toilet.
Cut at least one extra pouch for the middle-of-the-night pouch change. Always keep supplies for one pouch change with the child. There will be more stool output after your child has eaten. If possible, do not
change the pouch at that time.Occupy your infant’s attention (and hands) with toys during a pouch change. Try hanging a mobile over the changing area.
Be aware that products containing alcohol will sting when applied to irritated skin. Read the label of any unfamiliar product.

Prolapse
Retraction
12
Retraction
With retraction, the stoma retracts (is drawn back) into the body. It does not protrude from the abdomen. This makes it very difficult to keep a pouch in place. Good skin care is a must. Please contact your ET nurse for possible treatment options.
Prolapse
With prolapse, the stoma becomes elongated (longer) and swollen. If the stoma color changes to dark red or blue, notify your surgeon. Your surgeon may teach you to reduce the size of the stoma by putting it back inside the skin. It is fairly com-mon for stomas to prolapse in children. This is because children have poorly developed abdominal muscles, and crying causes an in-crease in pressure inside the abdo-men. A prolapsed stoma may need to be corrected with surgery. A one-piece pouch is recommended to prevent pinching the stoma in the flange.
Diagrams above show cross sections
of bowel and stoma
Potential Complications

Home Care o f Your Chi ld a f t e r an Ostomy 13
Peristomal hernia
With peristomal hernia, there is bulging at the base of the stoma. This may be completely around the stoma, or just on part of the stoma base. This bulging may come and go, depending on the pressure inside the abdomen. The pouch might need to be changed more often.
Stenosis
Stenosis occurs when the stoma opening narrows either at skin level or deeper in the abdomen’s muscular wall. If this happens, notify your sur-geon. Stool will be pencil-thin when it comes out of the stoma. If no stool is produced, call your surgeon.
Laceration
A laceration is a cut on the stoma. This occurs mostly when the pouch hole is too small or when the pouch is centered too close to the stoma. Your child should feel no pain, but there may be some bleeding from the stoma.
Diagrams above show cross sections
of bowel and stoma
Stenosis
Peristomal hernia

14
There are three common
infections that may be seen
around the stoma:
• Irritant dermatitis
• Yeast infections
• Folliculitis
To cArE For A YEAST InFEcTIon
1. Clean the skin, rinse it, and
pat dry.
2. Apply a very small amount
of the prescribed anti-fungal
powder on the red areas.
3. Lightly rub in the anti-fungal
powder, and then brush off
excess powder.
4. Place pouch as usual.
5. Change the pouch every day
until there is no more rash.
Yeast infections
Yeast infections are generally caused by candida albicans. It looks like a red, raised, bumpy rash which can appear anywhere from the base of the stoma to under the skin barrier or pouch.
If your child has a yeast infection, your doctor will prescribe an antifungal powder.
Note: Be sure to ask your
physician for a prescription
for anti-fungal powder,
not cream. Pouches will not
stick to the cream.
Potential Complications continued
Irritant dermatitis
Irritant dermatitis is an irritation of the skin caused by stool that has leaked out of the pouch onto the skin. The leaking is often due to a pouch hole that is too large or a pouch that has not been changed often enough. The stool then leaks under the wafer and causes skin breakdown. Irritant dermatitis will make the skin look red and broken.
stoma paste
1. Clean the skin, rinse it, and pat dry.
2. Apply a very small amount of Stomahesive®
powder on the irritated, red areas.
3. Lightly rub in the powder and brush off excess.
4. Place pouch as usual. This procedure will
need to be done with each pouch change
until the skin is healed. If the skin still
looks irritated after five days, call the
enterostomal therapy nurse.
To cArE For IrrITAnT dErmATITIS

Home Care o f Your Chi ld a f t e r an Ostomy 15
Sign of dehydration is an increase in your child’s temperature
DehydrationRisk of dehydration
children who have had an ostomy can become dehydrated more quickly than other children. children and adults perspire (sweat) even when not physically active. It is difficult to know how much fluid is lost to perspiration, chiefly in dry areas such as the Intermountain West and during the summer. This is especially a concern for children with ileosto-mies. If you suspect dehydration, call your physician.
careful attention to stool output is necessary. You will become familiar with the amount of stool your child normally puts out each day. When this output increases, you need to be alert for dehydration. dehydration might also occur when your child has diarrhea or vomits.
Folliculitis
Folliculitis is an infection at the base of the hair shaft (the follicle) and may cause itching or pain. It occurs when hair has been removed traumatically, such as being pulled out or attached to tape. The infection is generally caused by Staphylococcus aureus. It looks like a pustule or a pimple.
To prevent folliculitis, remove the hair around the stoma and under the skin barrier. This can be done by clip-ping the hair with scissors or by using an electric razor. Be sure to keep the razor away from the stoma.
Signs and symptoms of
dehydration
• decrease in number of wet diapers.
• Tired, listless, lethargic; child seems more sleepy, less active, and unable to hold head up.
• Urine is darker in color and has a stronger smell.
• Increased temperature or fever.
• dry mucous membranes; no tears, dry mouth.
• Foul-smelling stools.
• Vomiting along with diarrhea.
• Sunken fontanel (soft spot on top of baby’s head).
P lease ask qu e s t i o n s !

16
Activities
Don’t be afraid to bathe your child with or without the pouch. Your child should have a pouch on when swimming in a pool. Your child’s activity should not be limited because of the ostomy. Always consult your doctor before your child engages in contact sports or activities.
Clothing
Children with ostomies should be clothed so that they cannot scratch their stomas or pull off their pouches. One-piece outfits or undershirts pinned to diapers may help. For older children, overalls may help. The belt or waistband should not ride or rub on the stoma. This could injure the stoma.
Nutrition
Your child’s doctor will discuss your child’s diet with you. For the most part, your child’s diet should not be different from that of a child without an ostomy.
Certain foods may produce specific changes in your child’s stool. This does not mean you need to remove the food from your child’s diet, but rather to be aware of the poten-tial effect.
Children with an ileostomy
should be taught to chew their
food well. This is especially
true for high fiber foods such
as nuts and popcorn, which can
cause blockage of the stoma.
Other Daily Care Tips

Home Care o f Your Chi ld a f t e r an Ostomy 17
Foods that may have various
effects on the stool.
Foods that may loosen stool
Dried or string beans•
Chocolate•
Raw fruits•
Raw vegetables•
Highly spiced foods•
Fried foods•
Greasy foods•
Prune or grape juice•
Leafy green vegetables (lettuce, •
broccoli, spinach)
Foods that may thicken stool
Bananas•
Rice•
Bread•
Potatoes•
Creamy peanut butter•
Applesauce•
Cheese•
Tapioca•
Yogurt•
Pasta•
Pretzels•
Marshmallows•
Food that may cause stool odor
Fish•
Eggs•
Asparagus•
Garlic•
Some spices•
Beans•
Turnips•
Cabbage-family vegetables •
(onions, cabbage, Brussel sprouts,
broccoli, cauliflower)
Food that may cause gas
Dried and string beans•
Carbonated beverages•
Cucumbers •
Cabbage-family vegetables •
(onions, cabbage, Brussel sprouts,
broccoli, cauliflower)
Dairy products•
Spinach•
Corn•
Radishes•
Foods that may color stool
Beets•
Red Jell-O• ®
Some medications•
Foods that may cause urine odor
Seafood•
Asparagus•
Food that have high fiber*
Corn•
Raw celery•
Coconut•
Legumes (chick peas, kidney beans, •
chili beans)
Chinese vegetables•
Apples with peels•
Grapes•
Raw cabbage (coleslaw)•
Dried fruits (raisins, figs, apricots)•
Nuts•
Popcorn•
Meat with casings (bologna, •
sausage, hot dogs)
Mushrooms•
*Remember, high-fiber foods need to be well-chewed.
Food Lists

18
Infants (1–12 months)
In the first year, most infants triple their birth weight. Therefore, it may be necessary to measure the stoma’s size frequently. You may also need to try different pouches as your child grows.
Infants are active—rolling, explor-ing their bodies, and discovering the world. To protect the pouch, keep it concealed in the diaper. Dress your baby in one-piece outfits or overalls.
Toddlers (12–36 months)
Toddlers are even more active—crawling, walking, running. Before you change the pouch, it is helpful to have all supplies ready. You can begin teaching older toddlers how to help empty the pouch and what steps are necessary. To help protect the pouch, dress your toddler in overalls or pants with no tight waistbands that ride over the stoma.
Preschoolers (3–5 years)
Preschoolers are intensely curious and want to be independent. They can assist with certain parts of ostomy care, such as removing the pouch, emptying the pouch, and cleaning the skin. Keep lessons short because your child’s attention span is probably short. Help your preschooler choose clothes without tight-fitting waistbands.
School-age children (6–11 years)
Children at this age can learn more about changing and emptying the pouch. By age 7 or 8, they should be able to take care of changing the pouch and emptying it on their own. However, parents still need to occa-sionally look at the skin to make sure there are no problems.
When your child starts school, he will need to take an extra pouch and changing supplies with him. Teachers will need written step-by-step in-structions. Review these instructions with the teacher and school nurse. This will give your child a support person at school.
At some point in this age group, it may be necessary to change to an adult-size pouch.
Helpful Tips by Age Group
Adolescents (12–18 years)
By age 12 or so, your child is gener-ally able to assume self-care, make appointments, and order equipment. Your role as parent is to offer support.
Teenagers do not need to tell every-one about their ostomy. They should tell only the people they want to. To participate in active sports such as wrestling or football, your child should have approval from the surgeon.
Ostomy equipment for adolescents is the same as for adults. Selection should be based on what is most ef-fective for your child.

Notes
Home Care o f Your Chi ld a f t e r an Ostomy 19

20
Colostomy: A surgically created opening of the large bowel, which forms a stoma and diverts body wastes.
Enterostomy: Surgical formation of an opening into the digetive tract.
Hirschsprung’s disease: A disease associated with lack of nerve (gan-glion) cells in a part of the intestine. The lack of ganglion cells affects the intestine’s ability to move stool through the intestine.
Ileostomy: A surgically created opening of the small bowel, which forms a stoma and diverts body wastes.
Imperforate anus: An anus that is closed by a membrane or tissue such that there is no opening for stool to pass.
Meconium ileus: A blockage in the newborn bowel with thick meconium stool. Meconium is the first feces produced by a newborn baby.
Necrotizing enterocolitis (NEC): Condition when the blood supply to the intestine slows or is cut off. The intestine becomes infected and dies.
Ostomy: A surgically created opening which is made through the abdominal wall to divert body wastes.
Peristalsis: The normal motion of the bowel that propels bowel con-tents forward through the bowel.
Peristomal: The area surrounding the stoma.
Prolapsed stoma: Stoma that is elongated (lengthened) and some-times swollen. All layers of the bowel come through the stoma opening. This is common.
Pseudo-membranous enteroco-litis: Inflammation of the lining of the intestine, which can involve both the small intestine and the colon.
Retracted stoma: Stoma that does not protrude (stick out) from the abdomen. Instead, the stoma looks like a hole or pucker in the abdo-men. The mucosal surface (moist tissue lining of the intestine) may or may not be visible.
Stoma: The visible opening of the portion of the intestine that is surgically brought out to the skin through the opening in the abdominal wall during your child’s ostomy surgery.
Glossary
Primary Children’s Medical Center 100 North Mario Capecchi Drive Salt Lake City, Utah 84113

xxii
©2008 INTERMOUNTAIN HEALTHCARE, Primary Children’s Medical Center, Pediatric Education Services.
All rights reserved.
The content presented here is for your information only. It is not a substitute for professional medical
advice, and it should not be used to diagnose or treat a health problem or disease. Please consult
your healthcare provider if you have any questions or concerns. More health information is available at
intermountainhealthcare.org.
Patient and Provider Publications 801.442.2963 IHCEDPES001 – 07/08 1KAP