Embed Size (px)
Citation preview
OSTEONECROSISAND
THE ANKLE JOINT
Julie Norin FoxMay 2006
Costa Mesa, CA
1
ABSTRACT
Osteonecrosis (ON) is the destruction (necrosis) of bone tissue (literally dead bone). It is
a not uncommon, often progressive disease, caused by a decrease in the blood flow to a
bone as a result of which the bone is unable to replace the cells that are dying off in the
usual course of events. Because the bone cells cannot be replaced (at least at a fast
enough rate), the bone weakens, degenerates and may crack or collapse. Joint pain is the
primary symptom. It is a chronic pain, usually occurring when standing, walking or
lifting. The pain becomes worse as weight is put on the bones or joints. Other symptoms
include joint stiffness and limitation of motion. ON affects approximately 20,000 new
patients per year in the United States. Typically the patients are between 20 and 50 years
old with the average age in the 30’s.
2
CONTENTS
Title page……………………………………………………….page one
Abstract…………………………………………………………page two
Contents………………………………………………………...page three
Anatomical description…………………………………………page four-seven
Case study………………………………………………………page eight
Conditioning program…………………………………………..page nine, ten
Conclusion………………………………………………………page eleven
Bibliography…………………………………………………….page twelve
3
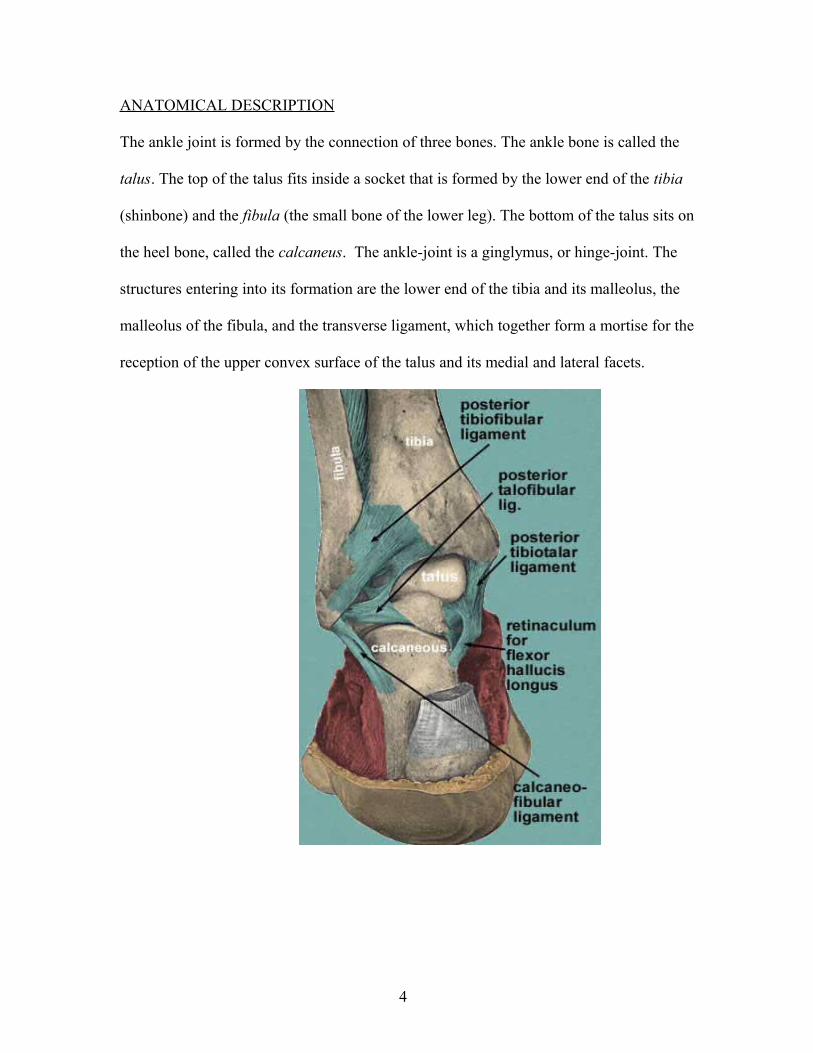
ANATOMICAL DESCRIPTION
The ankle joint is formed by the connection of three bones. The ankle bone is called the
talus. The top of the talus fits inside a socket that is formed by the lower end of the tibia
(shinbone) and the fibula (the small bone of the lower leg). The bottom of the talus sits on
the heel bone, called the calcaneus. The ankle-joint is a ginglymus, or hinge-joint. The
structures entering into its formation are the lower end of the tibia and its malleolus, the
malleolus of the fibula, and the transverse ligament, which together form a mortise for the
reception of the upper convex surface of the talus and its medial and lateral facets.
4
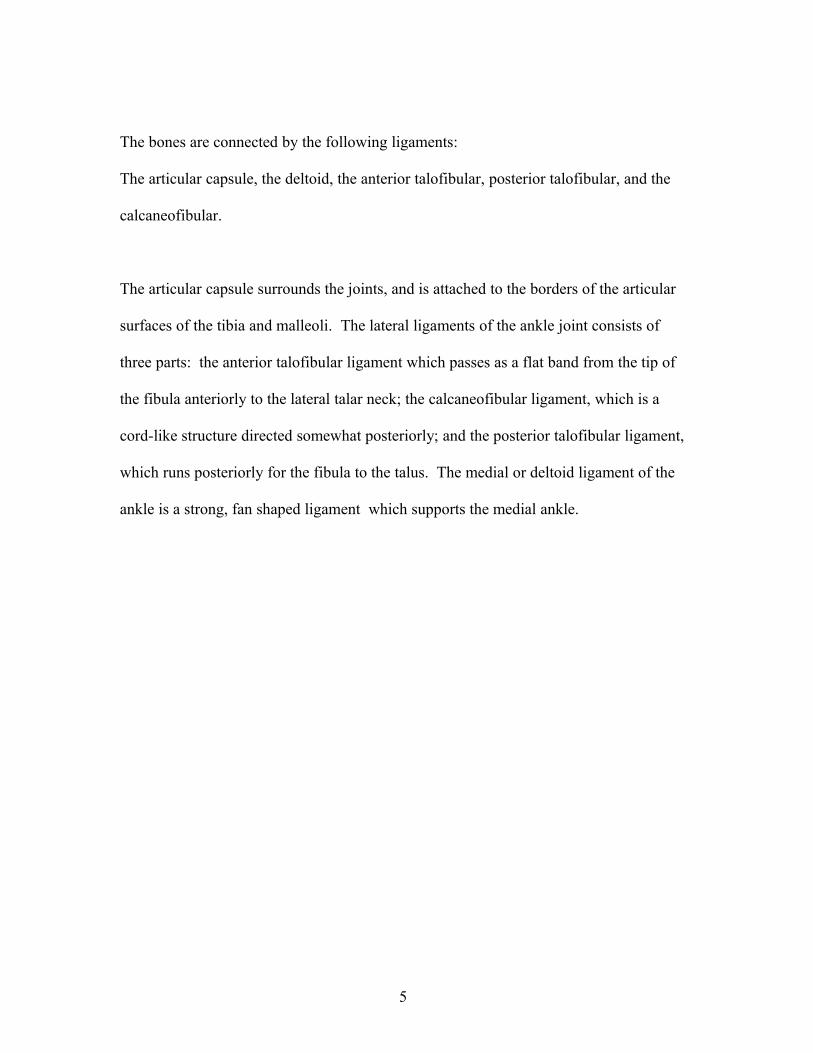
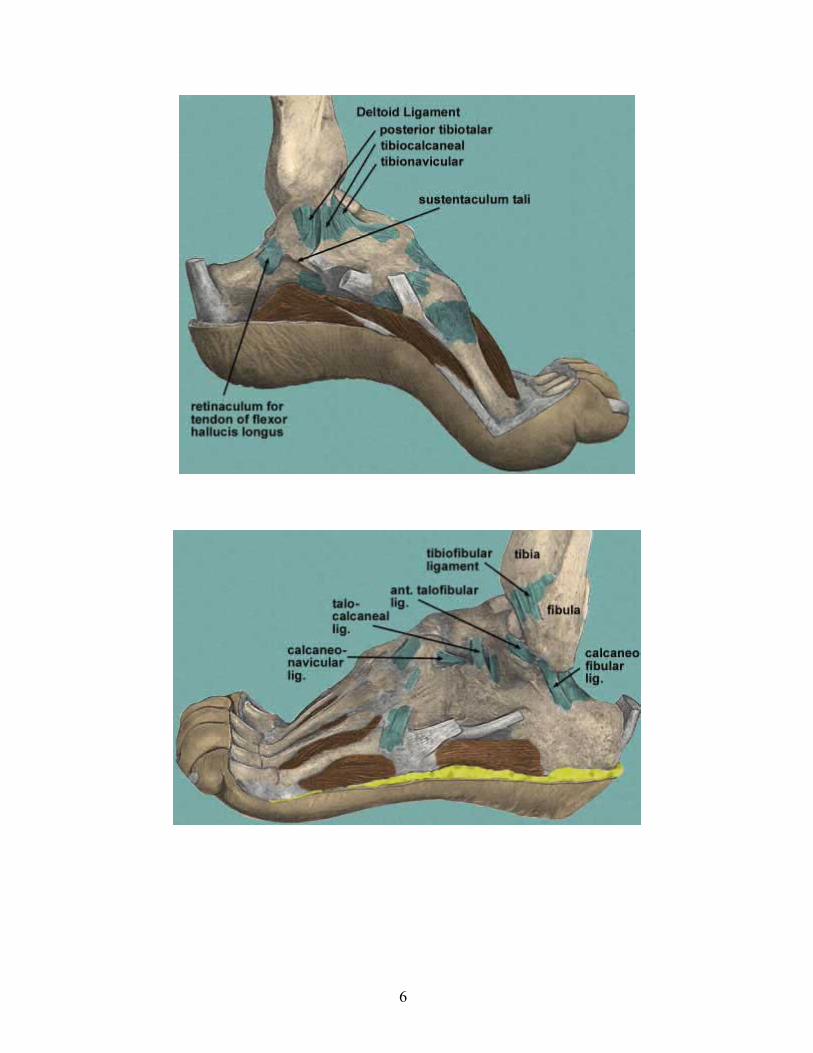
The bones are connected by the following ligaments:
The articular capsule, the deltoid, the anterior talofibular, posterior talofibular, and the
calcaneofibular.
The articular capsule surrounds the joints, and is attached to the borders of the articular
surfaces of the tibia and malleoli. The lateral ligaments of the ankle joint consists of
three parts: the anterior talofibular ligament which passes as a flat band from the tip of
the fibula anteriorly to the lateral talar neck; the calcaneofibular ligament, which is a
cord-like structure directed somewhat posteriorly; and the posterior talofibular ligament,
which runs posteriorly for the fibula to the talus. The medial or deltoid ligament of the
ankle is a strong, fan shaped ligament which supports the medial ankle.
5
6
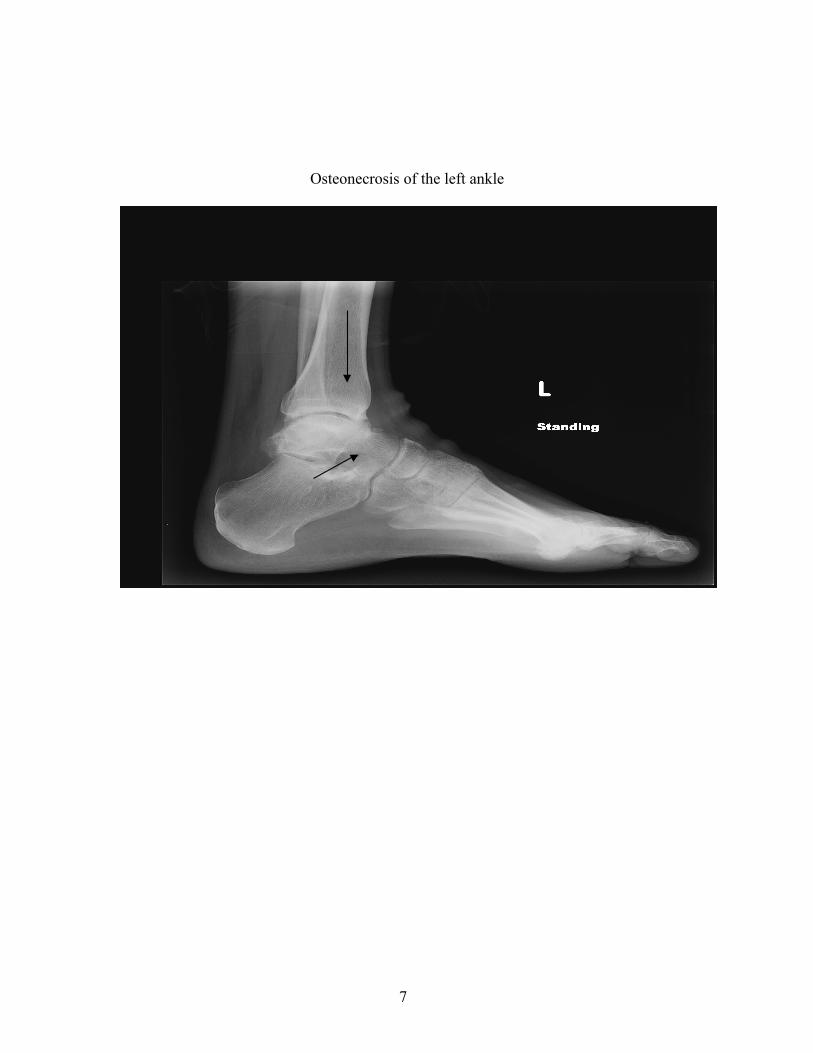
Osteonecrosis of the left ankle
7
CASE STUDY
A 56 year old male with limited range of motion in the ankle joints of both feet. Due to
Osteonecrosis of the Ankle bones he has chronic pain in the joints, tendons, and
surrounding tissues which limits his ability to participate in extended activities required
while standing or walking. The subject recently had arthoscopic surgery on the left ankle
to remove scar tissue. The result was a re-distribution of the angle of the foot and a
tightening of the tendons and ligaments particularly on the medial side of the left ankle.
The tissue surrounding the joints swells after a short time of consistent walking or
standing. The pain can be debilitating and as a result the subject limps favoring his left
foot while externally rotating and inverting it. This is a response to pain and painful
stimuli as the musculature developed a response to adapt or prevent it. An emphasis will
be placed on the left ankle with the exercises in order to gain an equal amount of
flexibility and strength as the right ankle (which is limited in itself). Past physical
therapy included, electro-stimulation, ice therapy, massage, stretching the feet alternating
in a plantarflex/dorsiflex position.
General overall health is good, except for a rare blood disorder called Hereditary
Hemochromotosis in which the subject’s most recent orthopedic surgeon attributes to
causing the Osteonecrosis. Hereditary Hemochromatosis is an inherited, autosomal
recessive disorder of iron metabolism that causes the body to absorb and store an excess
amount of iron resulting in "iron overload" disease. If left untreated, Hereditary
Hemochromatosis can result in the progressive accumulation of iron in the joints, liver,
8
pancreas, and heart. For the purpose of this paper I will not address this condition in
depth, as the Osteonecrosis is a presumed manifestation of the Hemochromatosis.
The subject has been extremely limited in his physical activity. His past exercise
program consisted of occasionally playing golf. In order for him to complete 9 or 18
holes he would consume 600 mgs. of ibuprofen which reduces the swelling around the
joints and gives him some relief of pain.
CONDITIONING PROGRAM
The following conditioning program utilizing the Block System from the Body Arts and
Science International approach has been chosen with the goal of increasing and
improving the range of motion in the ankle/foot area and strengthening surrounding
musculature without causing further inflammation or joint damage. We will work the
whole body to gain “core strength” which will develop the musculature to support proper
alignment and as a result will relieve pressure on the joints and bones.
With the left ankle we will focus on stretching the muscles and ligaments on the medial
side of the ankle/foot, such as the deltoid ligament, the tibialis anterior and the tibialis
posterior, while focusing on strengthening the lateral ankle/foot muscles including the
peroneus brevis, peroneus longus, and peroneal retinacula. In both ankles we will stretch
the primary plantar flexors (the gastrocnemius and the soleus) and the primary
dorsiflexors (the tibialis anterior and extensor digitorum longus). The exercises
highlighted to achieve this include: 1.) leg extension with the theraband as the foot
alternates between plantarflex, dorsiflex, lateral, medial, and circular movements. The
9
focus with the theraband on the left ankle with the lateral (or eversion) movement will
stretch the medial muscles and tendons while strengthening the lateral muscles;
2.) the full footwork series starting on the reformer and at a later date move on to
footwork on the wunda chair or cadillac; 3.) the jump board on the reformer will be used
in which the subject will not “jump” but alternate between dorsiflex and plantarflex in a
“walking” manner. This will provide stretching and ROM without the added stress of
weight on the ankle joints.
The following exercises will be in the overall program to balance the body and establish
“core strength.” We begin the session with a warm up and do the pelvic curl, spine twist
supine, chest lift, and chest lift with rotation on the mat; next will be the footwork as
mentioned above; abdominal work, such as the hundred prep, hundred, and coordination
on the reformer; hip work, such as leg up circles, down circles, and frog on the reformer;
spinal articulation, such as bottom lift on the reformer; stretches, including standing lunge
and kneeling lunge on the reformer; arm work, such as arm work supine on the reformer;
additional leg work on the mat including forward with drops, hip extension bent knee,
and hip abduction bent knee; lateral flexion, such as mermaid on the reformer and/or side
lift on the step barrel; finally, the breast stroke prep on the reformer and/or prone 1 on the
cadillac to strengthen the back extensors. The program will begin with an introduction to
the subject of the above-mentioned process and will advance to the next level when
appropriate.
10
CONCLUSION
Although there is no cure for Osteonecrosis, the program outlined can help alleviate the
subject’s pain in his ankles. Non-surgical treatments in addition to the conditioning
program are orthodics and ankle braces. Surgical alternatives include, 1.) core
decompression bone grafts designed to remove the inner layer of the bone and thus
increase blood flow to the bone and blood vessels in the bone; 2.) ankle fusion with
extensive bone grafting; 3.) total replacement with artificial parts (which historically has
not been very successful). Finally, as Joseph Pilates emphasized, the “whole” must be
exercised to achieve good health. The client must commit to the program and engage his
“mind” in the effort for success. A key issue in coaching this client is to keep him
motivated and inspire him to believe in the end result which will be less pain and more
range of motion in the ankles. Additionally, with the overall workout of the program he
will be able to have a more active, full life and, ultimately, what we all yearn for, total
well being.
11

BIBLIOGRAPHY
National Organization of Rare Disorders, Osteonecrosis, Jay R. Lieberman, MD, Dept. of Orthopedic Surgery, David Geffen School of Medicine of UCLACopyright 1990, 1992, 1995, 2003
Body Arts and Science International Study Guide, Comprehensive Course 2000-2004, Rael Isacowitz, MA, Founder and Director
National Osteonecrosis Foundation and The Center for Osteonecrosis Research and Education
Dr. Glenn B. Pfeffer, MD, Director, Foot and Ankle Center, Cedars Sinai Medical Center
Anatomy of Movement, Blandine Calais-Germain, 1993 by Eastland Press, Inc.
Web MD Health Guide
Google images
12