Embed Size (px)
Citation preview

OK
Redutwctotapamwoal
OCimT
D
A
0d
steomyelitis and Arthritisatrin D.M. Stumpe, MD, and Klaus Strobel, MD
Infections of bone and the joints can represent major diagnostic and therapeutic challenges toall clinicians. Together with osteomyelitis and septic arthritis, soft-tissue infections like cellu-lites/fasciitis and abscess formation can occur, which have to be treated appropriately. Bonescintigraphy is a sensitive method that can be used to search for bone and joint infections.Labeled leukocytes often are used as the gold standard to identify infectious foci in themusculoskeletal system, but major drawbacks of this method are the imaging of chronicinfections and imaging of the axial skeleton. Like 111In-labeled leukocyte imaging, 99mTc-labeledantigranulocyte antibody scintigraphy has a role in the imaging of osteomyelitis of the periph-eral skeleton. Magnetic resonance imaging is widely used to evaluate musculoskeletal infec-tions and is excellent in identifying abscess formation, but the extent and spread of infection issometimes difficult to delineate because hyperemia and infection are not congruent.Semin Nucl Med 39:27-35 © 2009 Elsevier Inc. All rights reserved.
as
atfauiidicattjdbal
pacblal
a
ecent studies indicate that 18F-fluorodeoxyglucose(FDG) positron emission tomography (PET) has consid-
rable value in the diagnosis of inflammatory and infectiousisease of the axial and peripheral skeleton. FDG-PET makesse of the fact that there is no physiological FDG accumula-ion in white cells that are not actively fighting an infection,hich permits excellent imaging of the axial skeleton, espe-
ially in patients with infection of the spine. PET/computedomograph (CT) appears to be more accurate for confirmingr excluding low-grade infection and chronic osteomyelitishan 99mTc bone scintigraphy, 99mTc-labeled antigranulocytentibody scintigraphy, and 111In-labeled leukocyte scintigra-hy. Although this usefulness extends to infections associ-ted with metallic implants used for trauma surgery, PETay not be as useful in the diagnosis of infections associatedith prosthetic joints. Compared with PET alone, PET/CTffers additional information because it provides precise an-tomical information and characterization of the infectiousesion, which is important for surgical planning.
steomyelitishoosing the appropriate combination of imaging methods
n the evaluation of infection may be challenging. A variety ofethods is available for imaging inflammation and infection.he role of imaging is to confirm the clinical suspicion, char-
ivision of Nuclear Medicine, Department of Medical Radiology, UniversityHospital, Zurich, Switzerland.
ddress reprint requests to Katrin D.M. Stumpe, MD, Division of NuclearMedicine, Department of Medical Radiology, University Hospital, 8091
eZurich, Switzerland. E-mail: [email protected]
001-2998/09/$-see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1053/j.semnuclmed.2008.08.003
cterize the lesion and its extent, and detect complicationsuch as abscess or fistula formation in infectious disease.
Standard radiography, magnetic resonance imaging (MRI),nd CT commonly are used to detect inflammatory and infec-ious lesions in the bone. Radiographs always should be per-ormed to provide an anatomic overview of the region of interestnd to select subsequent imaging modalities. MRI has beensed widely because of its excellent soft-tissue contrast and
ts sensitivity to tissue edema and hyperemia. MRI is valuablen the visualization of septic arthritis, spinal infection, andiabetic foot infections. However, these modalities are of lim-
ted value to detect early infection when morphologicalhanges are absent. In addition, diagnostic difficulties alwaysrise when chronic infection is suspected, particularly whenhere are preexisting alterations in the spine as the result ofrauma, surgery, or infection. Artifacts caused by prostheticoints or metallic implants in the spine or extremities canegrade images sufficiently to make diagnosis impossible inoth CT and MRI. Therefore, nuclear medicine proceduresre needed as a functional adjunct to complement morpho-ogic imaging techniques.
The choice of the best nuclear medicine procedure de-ends on the grade of inflammation, duration of infection,vailability, cost, and radiation exposure. Commonly usedonventional nuclear medicine procedures include 3-phaseone scintigraphy, 67Ga-citrate, 111In- and 99mTc-HMPAO-
abeled leukocytes, 99mTc-radiolabeled murine monoclonalntigranulocyte antibodies and 99mTc-radiolabeled nanocol-oids and human immunoglobulins.
Three-phase bone scintigraphy is readily available and hashigh negative predictive value in undamaged bone. How-
ver, it is nonspecific in patients with previously violated
27

bpgspja
tTabb
dsijccija
mpt
ibctit
iifpgcn
dciTsbrilc
idtg
Faogchs
28 K.D.M. Stumpe and K. Strobel
one, in patients with prosthetic joints, and in the neuro-athic joint. Under these circumstances, sequential bone/allium-67 (67Ga) scintigraphy is used; however, specificitiestill vary between less than 50% and 100%.1-4 The need toerform 2 imaging procedures and delayed imaging are ma-
or disadvantages. Gallium-67 imaging alone is useful as andjunct to MRI in the diagnosis of spinal infection.
Labeled leukocytes and antigranulocyte antibodies are nei-her sensitive nor specific for infection in the axial skeleton.5-7
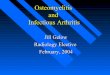
he latter imaging techniques have appropriate diagnosticccuracy in the peripheral skeleton; however, differentiationetween soft tissue and bone infection is often impossibleecause of limited spatial resolution (Fig. 1).Among the various conventional nuclear medicine proce-
ures, the use of 111In-labeled leukocytes is one of the mostpecific imaging techniques and is useful in acute infections,n osteomyelitis of the diabetic foot, and in the neuropathicoint. In addition, the use of labeled leukocytes, together withomplementary bone marrow scintigraphy, is the radionu-lide procedure of choice in the assessment of prosthetic jointnfection. However, presentation of patients with prostheticoints and the diabetic foot is complex and discussed in sep-rate articles in this seminar on infectious disease.
The development of single-photon emission computed to-ography (SPECT)/computed tomography (CT) camerasartly has overcome the lack of spatial resolution in conven-ional nuclear medicine by the use image coregistration.8
FDG-PET has shown some advantages in contrast to othermaging methods as a result of the so-called “respiratoryurst,” which mononuclear cells and neutrophilic granulo-ytes undergo when activated and while fighting an infec-ion.9,10 Infection can be acute or chronic, the former show-ng predominantly neutrophilic granulocytes infiltrates. Inhe latter, macrophages join the neutrophils.
In contrast to acute osteomyelitis, low-grade and chronicnfections are more difficult to diagnose with the currentmaging modalities. In this setting, PET is successfully per-ormed because FDG is avidly taken up by activated macro-hages in the chronic phases of infection. FDG-PET has thereatest diagnostic accuracy for confirming or excludinghronic osteomyelitis.11 According to the literature,12,13 aegative FDG-PET scan can virtually rule out osteomyelitis.FDG-PET is superior to labeled leukocyte imaging for the
etection of chronic osteomyelitis in the axial skeleton be-ause physiologic FDG uptake in the hematopoietic marrows relatively low.11 According to a recent meta-analysis byermaat and coworkers11 FDG-PET is not only the most sen-itive examination for the detection of chronic osteomyelitisut also more specific than labeled leukocytes, bone scintig-aphy, or MRI in this setting. Because of the high physiolog-cal uptake in the hematopoietic bone marrow in labeledeukocyte imaging, sensitivities are as low as 21% to detecthronic osteomyelitis in the axial skeleton.11
Increased FDG accumulation in PET is also associated withnflammatory arthritis, fractures, normally healing bone, andegenerative changes.14-16 However, in contrast to bone scin-igraphy, FDG-PET rapidly normalizes after traumatic or sur-
ical fractures14,16 as fibroblasts predominate in normally tigure 1 A 72-year old man with peripheral arterial occlusive diseasefter amputation of the first toe of the foot and with suspicion forsteomyelitis of the second toe of the right foot. 99mTc-labeled anti-ranulocyte antibody scintigraphy shows focally increased radionu-lide uptake of the distal tip of the second toe after 5 hours (A) and 24ours (B, ventral view; C, right lateral view). Differentiation betweenoft tissue and bone infection was not possible. After partial amputation of
he second toe of the right foot, histopathology confirmed osteomyelitis.
hatca
prfiatia1c
aelcttaioia2Ftwa
tro1iitcs
ctgPfvcti
DTlw
FltcwPluhscIlicjt
Osteomyelitis and arthritis 29
ealing bone, and FDG uptake quickly subsides 4 monthsfter surgery.17 The healing process shows most of the cellshat are present in inflammation.18 Therefore, specificity in-reases if recently (less than 4 months) traumatized or oper-ted bone is excluded.
Our group reported on FDG-PET in 18 patients with sus-ected acute and subacute osteomyelitis in the axial and pe-ipheral skeleton and found sensitivities of 100% and speci-cities in the range of 83% to 99%, respectively.19 de Winternd coworkers13 prospectively studied FDG-PET in 60 pa-ients with chronic osteomyelitis and found sensitivity, spec-ficity, and accuracy of 100%, 86%, and 93%, respectively. Inretrospective study, Kälicke and coworkers20 reported on5 true positive findings in 15 patients with histologicallyonfirmed acute (n � 7) and chronic osteomyelitis (n � 8).
FDG-PET was superior to 99mTc-labeled antigranulocytentibody scintigraphy in the evaluation of chronic osteomy-litis involving in the axial skeleton (n � 15 of 51).12 99mTc-abeled antigranulocyte antibody scintigraphy frequentlyannot differentiate between active and inactive processes ashe result of nonspecific areas of decreased radionuclide up-ake. FDG-PET provides sufficient anatomical informationnd spatial resolution to distinguish soft tissue from bonenfection, despite the presence of metallic implants. In an-ther study by Guhlmann and coworkers,21 overall sensitiv-ty and specificity were 100% and 92%, respectively, in thessessment of chronic osteomyelitis in the peripheral (n �1) and axial skeleton (n � 10). In the latter study, the use ofDG-PET showed particularly promising results in the detec-ion of chronic osteomyelitis in the axial skeleton, an area inhich labeled white cell scanning is of limited value, with an
ccuracy in the range between 53% and 76%.22
In a study performed by Zhuang and coworkers,23 sensi-ivity, specificity, and accuracy were 100%, 87.5%, and 90.9%,espectively, for FDG-PET in 22 patients with suspected chronicsteomyelitis. Chacko and coworkers24 reviewed the results of67 FDG-PET scans in patients with the suspicion of various
nfections. Fifty-six of these 167 patients were suspected of hav-ng chronic osteomyelitis, with an accuracy of 91%. In addition,he available data show that the use of FDG-PET is superior toonventional nuclear medicine methods to distinguish betweenoft tissue and bone infection (Fig. 2).
FDG-PET and FDG-PET/CT have many advantages overonventional nuclear medicine imaging techniques: comple-ion within 1 hour, high sensitivity, high target-to-back-round contrast, and high-resolution tomographic images.ET/CT with the combination of PET and a low-dose orull-dose diagnostic CT helps in this setting because it pro-ides exact anatomic localization of FDG uptake and in-reases the specificity compared with PET alone. The logis-ics of the PET technique make its use easier in chronic thann acute inflammation.
isc Space Infectionhe diagnosis of disc space infection has always been a chal-
enge for the clinician. Conventional radiography is normal
ithin the first 8 weeks before structural changes occur. Thei
igure 2 A 75-year-old man with adenocarcinoma of the left upperobe. In addition, the patient presented with an abscess in the righthoracic wall. (A) Maximum intensity projection (MIP) demonstratesircular increased FDG uptake in the left upper lung (short arrow) asell as diffuse FDG uptake in the right upper hemithorax (long arrow).hysiological FDG uptake is seen in the scaleni muscles as well as in the
arynx. (B) Axial CT scan demonstrates the lung tumor in the rightpper lobe (short arrow) and a tumorous lesion subpectoral (arrow-eads) in the right thoracic wall with air and involvement of the rightterno-clavicular joint (long arrow). (C) Axial PET/CT scan shows in-reased FDG uptake in the bronchial carcinoma in the left upper lobe.n addition, circular increased FDG uptake is found in the tumorousesion in the right hemithorax representing the abscess as well as focallyncreased FDG uptake of the right sterno-clavicular joint and the adja-ent bones with osseous destruction. In addition, the right sternocostaloint was involved. In contrast to PET or CT imaging alone, coregis-rated PET/CT helps to diagnose soft tissue infection and additional
nfectious involvement of the adjacent bones.
dMebliMcb
dnccartntrs9
msi
dktstleasusppsvc
ucpbiepdF
30 K.D.M. Stumpe and K. Strobel
iagnostic imaging technique of choice is contrast-enhancedRI with an accuracy of approximately 90%, which provides
arly diagnosis of disc space infection.25,26 In addition toone marrow abnormalities, epidural, subdural, intramedul-
ary, and paraspinal soft-tissue changes are signs for spinalnfection that can be clearly delineated in contrast-enhanced
RI. However, differentiation between degenerative (so-alled Modic abnormalities) and infectious disc disease cane difficult because of potentially similar abnormalities.Three-phase bone scintigraphy is of limited value in the
ifferentiation of degenerative from infectious end plate ab-ormalities. It showed an overall accuracy of only 67% andannot be recommended in the clinical routine.27 Modic andoworkers25 described a sensitivity and specificity of 90%nd 78% for bone scintigraphy and 96% and 92% for MRI,espectively. Bone scintigraphy, together with 67Ga SPECT, ishe radionuclide imaging method of choice so far for diag-osing spinal osteomyelitis. Love and coworkers4 reportedhat 67Ga scintigraphy was more sensitive than bone scintig-aphy and, when performed as SPECT, was comparable withequential bone-gallium scintigraphy with sensitivities of1% and specificities of 77%, respectively.In contrast to bone scintigraphy, 67Ga scintigraphy canore easily identify local extension of spinal infection (eg,
oft-tissue infection). In addition, 67Ga is more useful in mon-toring treatment response as it reflects more accurately the
Figure 3 A 72-year-old man with fever of unknown originlower lumbar spine (black arrowheads). (B) Sagittal PETbodies L1-L2 and L4-L5 (white arrowheads). (C) On axi
soft tissues ventrally to L1-L2 is seen. Disc space infection at L1egree of activity of infective processes.28 111In-labeled leu-ocytes have a limited value in the diagnosis of spinal infec-ion because of photopenic defects, which are nonspecific aseveral noninfectious conditions (eg, tumors and infarction)end to show photopenia.29,30 Although most of the pub-ished series are small, FDG-PET appears to be superior in thevaluation of spinal osteomyelitis with higher sensitivitiesnd specificities compared with 67Ga-citrate imaging.31-33 In atudy performed by Gratz and coworkers33 in which theysed a coincidence camera, they found that FDG-PET wasuperior to MRI and gallium imaging in patients with sus-ected disc space infection. Schmitz and coworkers32 re-orted that FDG-PET is sensitive in the detection of discpace infection and additional paravertebral soft-tissue in-olvement. Twelve of 16 patients had a histopathologicallyonfirmed disc space infection.
According to our results, the use of FDG-PET appears to beseful for excluding disc space infection in equivocal MRases. In the latter PET study, we included 30 symptomaticatients with substantial end-plate abnormalities of the lum-ar spine in MRI.31 FDG-PET did not show uptake in the
ntervertebral spaces of any patient with degenerative dis-ase, whereas infectious end plate abnormalities were alwaysositive (Fig. 3). The sensitivity and specificity for MRI inetecting disc space infection were 50% and 96%, and forDG-PET 100% and 100%, respectively.
IP shows linear increased FDG uptake in the upper andage shows FDG uptake in the endplates of the vertebralCT scan, additional increased FDG accumulation in the
. (A) M/CT imal PET/
-L2 and L4-L5 intervertebral disc level was confirmed.

MTSnt
fddn
FcascbFtIcw
Osteomyelitis and arthritis 31
etallic Implant-Associated Infections inrauma Patients (Except Prosthetic Joints)tandard radiography in trauma patients may demonstrateonunion, sequestered bone, intraosseous abscess forma-
igure 4 A 19-year-old woman with pain and in-reased inflammatory blood parameters 18 monthsfter lumbar spine stabilization surgery because ofevere scoliosis. (A) MIP shows increased FDG ac-umulation in the lower thoracic and upper lum-ar spine (black arrow). Axial (B) and sagittal (C)DG-PET/CT show increased FDG uptake aroundhe screws and the adjacent muscles of the spine.nfection of the soft tissues and metallic device wasonfirmed intraoperatively and the metallic deviceas removed.
ion, and bone resorption at implant–bone interfaces in in- e
ection. Standard radiography is not useful, however, for theiagnosis of early or low-grade infection. The use of MRIemonstrates abnormalities of bone marrow and soft tissue ifot hampered by artifacts caused by metallic implants. How-
ver, healing and infected tissue may be impossible to differ-
eacdb3fsoc
btsmr
rotaahriwaUa
cT(tda
smoWdwfIsip
wacpistl
32 K.D.M. Stumpe and K. Strobel
ntiate. This is also true for ultrasound, the use of which islso limited to bone surfaces and soft tissue. CT more pre-isely demonstrates fragments and sequestration than stan-ard radiography but is inferior to MRI in soft tissue andone marrow assessment. In conventional nuclear medicine,-phase bone scintigraphy is used for the initial evaluationor osteomyelitis, but the findings are affected by previousurgery and trauma and often are not specific. The limitationsf spatial resolution are a relevant problem. Specificity in-reases if combined bone and gallium scanning is used.
In the last decade, the use of 111In-labeled leukocytes com-ined with 99mTc bone marrow scintigraphy has been showno be highly accurate for the diagnosis of various musculo-keletal infections, which could alter distribution of bonearrow with sensitivities and specificities of 100% and 94%,
espectively.34
Labeled leukocyte scintigraphy combined with bone mar-ow scintigraphy is the conventional radionuclide proceduref choice for diagnosing complicating osteomyelitis like inrauma patients with metallic implants. FDG-PET representspromising imaging technique in the diagnosis of implant-
ssociated infections the imaging of in trauma patients andas shown to be both sensitive and specific.13,35 Conventionaladionuclide methods are often first-line imaging proceduresn the diagnosis of implant-associated infections in patientsith trauma. However, nonspecific tissue uptake of imaging
gents and imaging over several days restrict their usefulness.nlike MRI and CT, FDG-PET images are not substantially
ffected by metallic implants inserted for fixing fractures, in aontradistinction to PET imaging in prosthetic joint devices.his is most likely attributable to the more slender materialseg, titanium) and methods (eg, external fixation) used inrauma patients (Figs. 4 and 5). Patients with prosthetic jointevices show artifacts because of the relatively high photonbsorption of the prosthesis.35,36
FDG-PET demonstrates a sensitivity of nearly 100% and apecificity in the range of 88-93% in the diagnosis of chronicusculoskeletal infections, including patients with and with-
ut metallic implants or prosthetic replacements.13,21,35 deinter and coworkers13 evaluated the use of FDG-PET in the
iagnosis of chronic musculoskeletal infections in 34 patientsith metallic implants. Seventeen patients demonstrated in-
ections around metallic implants used in trauma surgery.nfectious lesions in the peripheral, as well as in the axialkeleton, were correctly identified with the use of FDG-PET,n contrast to the results of 17 patients with suspectederiprosthetic infections.Similar results were found by Guhlmann and coworkers,21
ho examined 6 patients with suspected metallic implant-ssociated infection in a group of 31 patients with suspectedhronic osteomyelitis. The only false-positive finding was aatient with a soft-tissue infection, which in PET was local-
zed to bone because of missing anatomic landmarks. In atudy performed by Kälicke and coworkers,20 FDG-PET wasrue positive in all cases. FDG-PET was not affected by metal-ike implants used for fixation of fractures. Moreover, Kälicke
Figure 5 A 72-year-old manwith suspicion for metallic im-plant associated infection ofthe right femur is shown. Thepatient had a history of chronicosteomyelitis in the past as theresult of undergoing surgeryfor liposarcoma of the rightthigh. (A) MIP shows increasedFDG uptake around the metal-lic implant in the right lateralfemur (black arrow). AxialPET/CT demonstrates focallyincreased FDG along the me-tallic material and the adjacentfemur (B and C, white arrows).Diagnosis of an infected metal-lic implant with osteomyelitiswas established.
nd coworkers20 demonstrated that FDG uptake at the sites

ot
1Fawfiwooett
dFsim1iw6Acl
awrptwatfnscbtc
SBtijoticstai
am
robuohc
Faaclasi
Osteomyelitis and arthritis 33
f fractures and nonunions is significantly lower than it is athe sites of infections, thereby facilitating differentiation.
The results of our own data showed a sensitivity of00%, a specificity of 93%, and an accuracy of 97% whenDG-PET is used in the diagnosis of metallic implant-ssociated chronic infections in 22 patients (29 scans)ith a previous history of trauma.35 One false-positivending was detected in the soft tissue of a patient sixeeks after surgery and no false-negative findings werebserved. In addition, the surgeons assessed the influencef FDG-PET on their treatment decisions. FDG-PET influ-nced the clinical decision-making process in almost two-hirds of the patients. FDG-PET could accurately differen-iate between bone and soft-tissue infection.
One of the largest studies was prospectively performed bye Winter and coworkers.37 The latter group investigatedDG-PET in 57 patients (n � 27 with metallic implants) withuspected infection after previous spinal surgery. The mediannterval between surgery and FDG-PET examination was 10
onths (range 1.25-288 months). Infection was detected in0 of 27 patients with and in 5 of 30 patients without metallic
mplants in the spine. Sensitivity, specificity, and accuracyere 100%, 81%, and 86%, respectively. In approximately0% of patients, infection could be ruled out with FDG-PET.lthough specificity of FDG-PET was not greater than 81%,omparable results are not obtained with bone scintigraphy,abeled leukocytes, or MRI in the postoperative spine.38
In a recent study performed by our own group, we evalu-ted the diagnostic value of FDG-PET/CT in trauma patientsith suspected chronic osteomyelitis and found promising
esults (Fig. 6).39 Among 33 PET/CT scans, 17 were trueositive, 13 true negative, 2 false positive, and 1 false nega-ive. Sensitivity, specificity, and accuracy for FDG-PET/CTas 94%, 87%, and 91% for the whole group; 88%, 100%,
nd 90% for the axial skeleton; and 100%, 85%, and 91% forhe peripheral skeleton, respectively. Our data showed 2alse-positive (both in the peripheral skeleton) and one false-egative finding (in the axial skeleton). Summarizing the re-ults of these studies, FDG-PET is superior for detectinghronic osteomyelitis in the axial skeleton in contrast to la-eled leukocyte imaging.11 PET/CT allowed precise localiza-ion of the infectious focus and demonstrated the extent ofhronic osteomyelitis with a high degree of accuracy.
eptic Arthritisacterial arthritis may be caused by penetrating trauma orhrough ulcers such as those occurring in diabetes. Directmplantation of infectious agents also may occur after in-ections or surgery. Hematogenous routes of infectionccur, especially in immunocompromised patients. Al-hough bone scintigraphy is used widely in imaging non-nfectious arthritis in rheumatologic patients, radionu-lide imaging has a limited role in the management ofeptic arthritis because ultrasound and joint fluid aspira-ion with microbiologic workup are easy to perform andvailable everywhere. Radionuclide imaging can be useful
n the differentiation of septic arthritis from osteomyelitis 7nd soft tissue infection as well as in the detection ofultifocal joint infections.The appearance of septic arthritis in 3-phase bone scintig-
aphy with 99mTc-diphosphonates is characteristic: becausef hyperemia in synovial vessels, all 3 phases (the perfusion,lood pool, and osseous phase) show increased radionuclideptake.40-42 Normal or even decreased radiotracer uptake canccur in cases of arthritis if the blood flow is compromised byigh intracapsular pressure. Majd and Frankel43 found in-reased uptake in 6 of 7 children and decreased uptake in 1 of
igure 6 A 57-year-old man a year after implantation of a prostheticnkle joint on the right side is shown. Perfusion (A), blood pool (B),nd osseous phase (C) of bone scintigraphy show markedly in-reased activity around the right ankle joint. Additionally 99mTc-abeled antigranulocyte antibody scintigraphy (D) was performed,gain showing increased uptake in the right ankle joint. Diagnosis ofeptic arthritis of the right prosthetic ankle joint was confirmedntraoperatively.
children with proven septic arthritis. Bone scintigraphy is

maccttcmmmaraacg
dtptimtwjm
hPwiiaipftaontM
CBccpoaIjlaon
iibmm(ttbstpt
FtPsw
34 K.D.M. Stumpe and K. Strobel
ore sensitive than standard radiography in the diagnosis ofrthritis because radionuclide uptake precedes morphologi-al bone changes.41,44 If the bone scan is negative but thelinical impression is still suspicious for septic arthritis,he specificity of bone scans can be improved by the addi-ional performance of 67Ga, labeled leukocytes, or mono-lonal antibody studies (Fig. 6). However, the need to useultiple radionuclide tracers and to perform imaging atultiple times adds complexity, delays the start of treat-ent, and causes inconvenience to the patients. SPECT
nd SPECT/CT are useful supplements to planar scintig-aphy, especially in equivocal cases and in the differenti-tion of soft tissue and bone infection as demonstrated inpatient with osteomyelitis.8,45 SPECT/CT also should be
onsidered in patients with arthritis in complex body re-ions like the spine.46,47
MRI with intravenous contrast administration reliablyemonstrates the abnormalities associated with septic ar-hritis, including joint effusion, synovial hyperemia, androliferation. In addition, reactive bone marrow and soft-issue edema, secondary osteomyelitis, tendon abnormal-ties, and soft-tissue abscesses are found.48 Although MRI
ight be superior in monoarticular infections, the advan-age of bone scintigraphy over MRI is that a bone scan is ahole-body imaging technique and covers all involved
oints in one investigation. Thus, in infections involvingultiple joints, radionuclide studies should be performed.The role of FDG-PET/CT in the workup of septic arthritis
as not been defined yet. According to our experience, FDG-ET/CT is particularly useful in clinically difficult cases inhich the advantage of PET as a relatively fast, whole-body
maging modality plays an important role, as demonstratedn Fig. 7. Compared with bone scintigraphy, FDG-PET/CTlso can be used to discover infectious foci outside the bonen the lung or other organs. Dumarey and coworkers showedromising initial results using 18F-FDG-labeled leukocytesor infection imaging and reported 1 case of septic knee ar-hritis among the 23 patients included.49 Cost effectiveness ofdvanced and expensive imaging modalities like SPECT/CTr PET/CT have not been investigated, and further studies areeeded to define the role of nuclear medicine in septic arthri-is compared with morphologic imaging like ultrasound and
RI.
onclusionone scintigraphy, 67Ga, and labeled leukocytes are theonventional nuclear medicine imaging techniques ofhoice for imaging musculoskeletal infection. At theresent time, FDG-PET has an incremental value overther imaging modalities and appears to be more sensitivend specific in the detection of various infectious diseases.n the diagnosis of osseous infection, FDG-PET has a ma-or impact in patients with chronic osteomyelitis. Particu-arly in the axial skeleton, FDG-PET is an important im-ging technique in the diagnosis and exclusion of chronicsteomyelitis, showing superior accuracy to other radio-
uclide imaging modalities. Moreover, FDG-PET plays an omportant role in the differentiation between disc spacenfection and erosive degenerative disc disease, whereoth MRI and bone scan may be falsely positive. FDG-PETay replace other imaging modalities in the assessment ofetallic implant-associated infection in trauma patients
excluding prosthetic joints). Differentiation between os-eomyelitis and soft-tissue infection may be better ob-ained with the use of FDG-PET than with CT or MRI,ecause of better lesion-to-background contrast and thecarcity of artifacts arising from metallic implants used inrauma surgery compared with CT and MRI. FDG-PET/CTermits more precise delineation and characterization ofhe infectious focus and helps to improve the management
igure 7 A 48-year-old woman with bacteriemia and septic polyar-hritis. Staphylococcus aureus was found in the left ankle joint. FDG-ET/CT was performed for screening of the involved joints. MIPhows multiple joints (left shoulder, right sternoclavicular joint, leftrist, both knees and ankles, arrows) with increased FDG uptake.
f patients with various infectious diseases.

R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
Osteomyelitis and arthritis 35
eferences1. Rosenthall L, Lisbona R, Hernandez M, et al: 99mTc-PP and 67Ga imaging
following insertion of orthopedic devices. Radiology 133:717-721, 19792. Schauwecker DS, Park HM, Mock BH, et al: Evaluation of complicating
osteomyelitis with Tc-99m MDP, In-111 granulocytes, and Ga-67 ci-trate. J Nucl Med 25:849-853, 1984
3. Schauwecker DS: The scintigraphic diagnosis of osteomyelitis. AJRAm J Roentgenol 158:9-18, 1992
4. Palestro CJ, Torres MA: Radionuclide imaging in orthopedic infections.Semin Nucl Med 27:334-345, 1997
5. Chung JK, Yeo J, Lee DS, et al: Bone marrow scintigraphy using tech-netium-99m-antigranulocyte antibody in hematologic disorders.J Nucl Med 37:978-982, 1996
6. Jacobson AF, Gilles CP, Cerqueira MD: Photopenic defects in marrow-containing skeleton on indium-111 leucocyte scintigraphy: Prevalenceat sites suspected of osteomyelitis and as an incidental finding. EurJ Nucl Med 19:858-864, 1992
7. Gratz S, Braun HG, Behr TM, et al: Photopenia in chronic vertebralosteomyelitis with technetium-99m-antigranulocyte antibody (BW250/183). J Nucl Med 38:211-216, 1997
8. Horger M, Eschmann SM, Pfannenberg C, et al: The value of SPET/CT inchronic osteomyelitis. Eur J Nucl Med Mol Imaging 30:1665-1673, 2003
9. Babior BM: The respiratory burst of phagocytes. J Clin Invest 73:599-601, 1984
0. Kaim AH, Weber B, Kurrer MO, et al: Autoradiographic quantificationof 18F-FDG uptake in experimental soft-tissue abscesses in rats. Radi-ology 223:446-451, 2002
1. Termaat MF, Raijmakers PG, Scholten HJ, et al: The accuracy of diag-nostic imaging for the assessment of chronic osteomyelitis: a systematicreview and meta-analysis. J Bone Joint Surg Am 87:2464-2471, 2005
2. Guhlmann A, Brecht-Krauss D, Suger G, et al: Fluorine-18-FDG PETand technetium-99m antigranulocyte antibody scintigraphy in chronicosteomyelitis. J Nucl Med 39:2145-2152, 1998
3. de Winter F, van de Wiele C, Vogelaers D, et al: Fluorine-18 fluorode-oxyglucose-position emission tomography: A highly accurate imagingmodality for the diagnosis of chronic musculoskeletal infections. J BoneJoint Surg Am 83-A:651-660, 2001
4. Meyer M, Gast T, Raja S, et al: Increased F-18 FDG accumulation in anacute fracture. Clin Nucl Med 19:13-14, 1994
5. von Schulthess GK, Meier N, Stumpe KD: Joint accumulations of FDGin whole body PET scans. Nuklearmedizin 40:193-197, 2001
6. Zhuang H, Sam JW, Chacko TK, et al: Rapid normalization of osseousFDG uptake following traumatic or surgical fractures. Eur J Nucl MedMol Imaging 30:1096-1103, 2003
7. Kaim AH, Gross T, von Schulthess GK: Imaging of chronic posttrau-matic osteomyelitis. Eur Radiol 12:1193-1202, 2002
8. Henry G, Garner WL: Inflammatory mediators in wound healing. SurgClin North Am 83:483-507, 2003
9. Stumpe KD, Dazzi H, Schaffner A, et al: Infection imaging using whole-body FDG-PET. Eur J Nucl Med 27:822-832, 2000
0. Kälicke T, Schmitz A, Risse JH, et al: Fluorine-18 fluorodeoxyglucosePET in infectious bone diseases: Results of histologically confirmedcases. Eur J Nucl Med 27:524-528, 2000
1. Guhlmann A, Brecht-Krauss D, Suger G, et al: Chronic osteomyelitis:Detection with FDG PET and correlation with histopathologic findings.Radiology 206:749-754, 1998
2. Palestro CJ, Kim CK, Swyer AJ, et al: Radionuclide diagnosis of vertebralosteomyelitis: Indium-111-leukocyte and technetium-99m-methylenediphosphonate bone scintigraphy. J Nucl Med 32:1861-1865, 1991
3. Zhuang H, Duarte PS, Pourdehand M, et al: Exclusion of chronic os-teomyelitis with F-18 fluorodeoxyglucose positron emission tomo-graphic imaging. Clin Nucl Med 25:281-284, 2000
4. Chacko TK, Zhuang H, Nakhoda KZ, et al: Applications of fluorode-oxyglucose positron emission tomography in the diagnosis of infection.Nucl Med Commun 24:615-624, 2003
5. Modic MT, Feiglin DH, Piraino DW, et al: Vertebral osteomyelitis:
Assessment usinMsg MR. Radiology 157:157-166, 19856. Meyers SP, Wiener SN: Diagnosis of hematogenous pyogenic vertebralosteomyelitis by magnetic resonance imaging. Arch Intern Med 151:683-687, 1991
7. Love C, Patel M, Lonner BS, et al: Diagnosing spinal osteomyelitis: acomparison of bone and Ga-67 scintigraphy and magnetic resonanceimaging. Clin Nucl Med 25:963-977, 2000
8. Tyrrell PN, Cassar-Pullicino VN, McCall IW: Spinal infection. Eur Ra-diol 9:1066-1077, 1999
9. Gemmel F, Dumarey N, Palestro CJ: Radionuclide imaging of spinalinfections. Eur J Nucl Med Mol Imaging 33:1226-1237, 2006
0. Whalen JL, Brown ML, McLeod R, et al: Limitations of indium leuko-cyte imaging for the diagnosis of spine infections. Spine 16:193-197,1991
1. Stumpe KD, Zanetti M, Weishaupt D, et al: FDG positron emissiontomography for differentiation of degenerative and infectious endplateabnormalities in the lumbar spine detected on MR imaging. AJR Am JRoentgenol 179:1151-1157, 2002
2. Schmitz A, Risse JH, Grunwald F, et al: Fluorine-18 fluorodeoxyglu-cose positron emission tomography findings in spondylodiscitis: pre-liminary results. Eur Spine J 10:534-539, 2001
3. Gratz S, Dorner J, Fischer U, et al: 18F-FDG hybrid PET in patients withsuspected spondylitis. Eur J Nucl Med Mol Imaging 29:516-524, 2002
4. Palestro CJ, Roumanas P, Swyer AJ, et al: Diagnosis of musculoskeletalinfection using combined In-111 labeled leukocyte and Tc-99m SCmarrow imaging. Clin Nucl Med 17:269-273, 1992
5. Schiesser M, Stumpe KD, Trentz O, et al: Detection of metallic implant-associated infections with FDG PET in patients with trauma: correla-tion with microbiologic results. Radiology 226:391-398, 2003
6. Stumpe KD, Notzli HP, Zanetti M, et al: FDG PET for differentiation ofinfection and aseptic loosening in total hip replacements: Comparisonwith conventional radiography and three-phase bone scintigraphy. Ra-diology 231:333-341, 2004
7. De Winter F, Gemmel F, Van De Wiele C, et al: 18-Fluorine fluorode-oxyglucose positron emission tomography for the diagnosis of infectionin the postoperative spine. Spine 28:1314-1319, 2003
8. Rothman SL: The diagnosis of infections of the spine by modern imag-ing techniques. Orthop Clin North Am 27:15-31, 1996
9. Hartmann A, Eid K, Dora C, et al: Diagnostic value of (18)F-FDGPET/CT in trauma patients with suspected chronic osteomyelitis. EurJ Nucl Med Mol Imaging 2006.
0. Rosenthall L, Kloiber R, Damtew B, et al: Sequential use of radiophos-phate and radiogallium imaging in the differential diagnosis of bone,joint and soft tissue infection: quantitative analysis. Diagn Imaging51:249-258, 1982
1. Gilday DL, Paul DJ, Paterson J: Diagnosis of osteomyelitis in children bycombined blood pool and bone imaging. Radiology 117:331-335, 1975
2. Maurer AH, Chen DC, Camargo EE, et al: Utility of three-phase skeletalscintigraphy in suspected osteomyelitis: Concise communication.J Nucl Med 22:941-949, 1981
3. Majd M, Frankel RS: Radionuclide imaging in skeletal inflammatory andischemic disease in children. AJR Am J Roentgenol 126:832-841, 1976
4. Gilday DL: Problems in the scintigraphic detection of osteomyelitis.Radiology 135:791, 1980
5. Filippi L, Schillaci O: Usefulness of hybrid SPECT/CT in 99mTc-HMPAO-labeled leukocyte scintigraphy for bone and joint infections.J Nucl Med 47:1908-1913, 2006
6. Michel-Batot C, Dintinger H, Blum A, et al: A particular form of septicarthritis: Septic arthritis of facet joint. Joint Bone Spine 75:78-83, 2008
7. Swayne LC, Dorsky S, Caruana V, et al: Septic arthritis of a lumbar facetjoint: Detection with bone SPECT imaging. J Nucl Med 30:1408-1411,1989
8. Learch TJ, Farooki S: Magnetic resonance imaging of septic arthritis.Clin Imaging 24:236-242, 2000
9. Dumarey N, Egrise D, Blocklet D, et al: Imaging infection with 18F-FDG-labeled leukocyte PET/CT: Initial experience in 21 patients.
J Nucl Med 47:625-632, 2006