Embed Size (px)
Citation preview

Review ArticleOsteogenic Induction of Wharton’s Jelly-Derived MesenchymalStem Cell for Bone Regeneration: A Systematic Review
Ayu Suraya Ansari,1 Muhammad Dain Yazid,2 Nur Qisya Afifah Veronica Sainik,1
Rabiatul Adawiyah Razali,1 Aminuddin Bin Saim,3 and Ruszymah Bt Hj Idrus 1
1Department of Physiology, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latif, 56000 Cheras,Kuala Lumpur, Malaysia2Tissue Engineering Centre, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latif, 56000 Cheras,Kuala Lumpur, Malaysia3Ear, Nose & Throat Consultant Clinic, Ampang Puteri Specialist Hospital, 68000 Ampang, Selangor, Malaysia
Correspondence should be addressed to Ruszymah Bt Hj Idrus; [email protected]
Received 19 May 2018; Revised 27 July 2018; Accepted 3 September 2018; Published 11 November 2018
Academic Editor: Jeong-Chae Lee
Copyright © 2018 Ayu Suraya Ansari et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Wharton’s jelly-derived mesenchymal stem cells (WJ-MSCs) are emerging as a promising source for bone regeneration in thetreatment of bone defects. Previous studies have reported the ability of WJ-MSCs to be induced into the osteogenic lineage. Thepurpose of this review was to systematically assess the potential of WJ-MSC differentiation into the osteogenic lineage. Acomprehensive search was conducted in Medline via Ebscohost and Scopus, where relevant studies published between 1961 and2018 were selected. The main inclusion criteria were that articles must be primary studies published in English evaluatingosteogenic induction of WJ-MSCs. The literature search identified 92 related articles, but only 18 articles met the inclusioncriteria. These include two animal studies, three articles containing both in vitro and in vivo assessments, and 13 articles onin vitro studies, all of which are discussed in this review. There were two types of osteogenic induction used in these studies,either chemical or physical. The studies demonstrate that WJ-MSCs are able to differentiate into osteogenic lineage and promoteosteogenesis. In light of these observations, it is suggested that WJ-MSCs can be a potential source of stem cells for osteogenicinduction, as an alternative to bone marrow-derived mesenchymal stem cells.
1. Introduction
1.1. Human Umbilical Cord. About 25 years ago, the umbili-cal cord was considered to be a type of medical waste,until it was found to be a rich source of stem cells [1].The abundance of stem cells and the ease of isolation havebecome deciding factors while choosing the source of adultstem cells. The human umbilical cord (HUC) is approxi-mately 65 cm in length and 1.5 cm in diameter [2, 3]; itconnects the fetus to the mother and supplies nourish-ment. The cord is covered by single or multiple layer ofsquamous cubic epithelial cells derived from the develop-ing amnion [4–6]. The HUC contains two arteries andone vein, which are surrounded by a mucoid connectivetissue known as Wharton’s jelly (WJ) [7]. This mucous
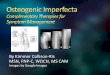
connective tissue is made up of mucopolysaccharides thatare hyaluronic acid and chondroitin sulphate [8]. Basi-cally, WJ can be divided into 4 layers with the outerlayer being the amniotic epithelium followed by cord lin-ing WJ and intermediate WJ. The inner layer of WJ isalso known as perivascular WJ which contains arteriesand vein [7] (Figure 1).
It has been reported that WJ also contains myofibroblast-like stromal cells, collagen fibers, proteoglycans, fibroblasts,and macrophages. WJ has garnered interest due to its avail-ability, the noninvasive method of collection, and high cellyields. It has been demonstrated that mesenchymal stem cells(MSCs) isolated from the umbilical cord express matrixreceptors (CD44 and CD105) and integrins (CD29 andCD51), but not hematopoietic lineage markers (CD34 and
HindawiStem Cells InternationalVolume 2018, Article ID 2406462, 17 pageshttps://doi.org/10.1155/2018/2406462

CD45) [9]. These cells exhibit a phenotype similar to that ofmesenchymal stem cells from other tissue sources [10].According to the International Society for Cellular Therapy(ISCT), stem cells should demonstrate plastic adherence,not expressing hematopoietic markers, and be able to com-mit to the adipogenic, osteogenic, and chondrogenic lineage[11]. WJ-MSCs have a huge advantage where the phenotypeand stemness are remained despite being in a long-term cul-ture. This enables a mass production of cells which is usuallyrequired for regenerative medicine [12].
1.2. WJ-MSCs and Their Potential in the Treatment ofDiseases. WJ, also known as substantia gelatinea funiculiumbilicalis, consists of fibroblast-like cells and mast cells thatare embedded in proteoglycans, mainly hyaluronic acid. Thecells are thought to be trapped in WJ during the early stage ofembryogenesis, when they migrate from the aortic gonado-tropin mesonephric region to the fetal liver through theumbilical cord [13]. WJ-MSCs have many advantages overother types of stem cells, including higher proliferation ratesand broader multipotency. WJ-MSCs are able to differentiateinto many cell types such as adipocytes [14, 15], osteoblasts[14, 16], hepatocytes [17], chondrocytes [18], and neural cells[19, 20]. Interestingly, it has also been demonstrated in athree-dimensional model that WJ-MSCs are able to differen-tiate in vitro into cornea epithelial-like cells, which may offera solution for patients with limbus stem cell deficiency [21].
Cui and colleagues have successfully improved cogni-tive function in a mouse model of Alzheimer’s diseaseusing intravenously delivered WJ-MSCs, which reducedoxidative stress and promoted hippocampal neurogenesis[20]. In a clinical trial conducted by Hu and colleagues,an intravenous infusion of WJ-MSCs in type 2 diabetesmellitus patients improved the function of islet β-cellsand reduced the incidence of diabetic complications [22].Additionally, WJ-MSC therapy is now used to treat cor-neal epithelial, stromal, and endothelial disorders apart
from the conventional intervention such as surgery, ioniz-ing radiation, or drug treatment [23, 24].
1.3. Immunomodulatory Aspect of WJ-MSCs and BM-MSCs.WJ harbours MSCs that possess a similar phenotype asharvested from the bone marrow and other sources. WJ-MSCs do not express HLA-DR and costimulatory moleculesCD40, CD80, and CD86 which are essential for the activationof T-cells [1, 2, 9, 25–27]. WJ-MSCs have been proven tohave lower immunogenicity than BM-MSCs as depicted byWeiss et al. [1] who conducted an experiment using mixedlymphocyte reaction (MCR) assay [26]. In a study conductedby Prasanna et al. and Deuse et al., both consistently showedlow HLA-DR expression compared to BM-MSCs after stim-ulation with IFN-γ and proinflammatory cytokines [28, 29].In normal culture conditions, HLA-DR is not expressed;hence, the activation of T-cell is inhibited, reducing the riskof allograft rejection which potentially makes it safe forhuman transplantation.
It is documented that BM-MSCs harbour viruses, whichis a major drawback in clinical application. There are reportsfrom patients who undergo BM-MSC transplant who areinfected with viral infection as a complication of the cell-based therapy [9]. Interestingly, the virus can escape fromdetection therefore increasing the morbidity and mortality[30]. Moreover, there are various diseases such as aplasticanemia, leukaemia, and bone marrow failure that impedesthe application of BM-MSCs in therapy [31].
1.4. WJ-MSC Homing and Migration for Bone Healing. Gen-erally, MSCs are known to migrate towards the injury siteand help the healing process. The migration process,known as homing, is defined as the arrest of MSCs withinthe vasculature of a tissue before it crosses over the endo-thelium [24, 32]. As for now, the mechanism of MSChoming is still vague and BM-MSCs are postulated to havea mechanism similar to leukocyte homing. The mechanism
INNER LAYER
OUTER LAYER
Amniotic epithelium
Cord lining Wharton’s jelly
Intermediate Wharton’s jelly
Perivascular Wharton’s jelly
Umbilical vein
Umbilical arteries
Umbilicalarteries
Umbilicalvein
Wharton’sjelly
Figure 1: Anatomical compartment of Wharton’s jelly mesenchymal stem cell.
2 Stem Cells International

is initiated when MSCs collide with the endothelium roll-ing, causing a slackening of cells in the blood flow. The G-protein-coupled receptors activated the cells and activatedintegrin mediation, causing activation-dependent arrest.The process is completed with the transmigration of thecells through the endothelium and the underlying base-ment membrane [33]. There are several factors thatcontribute to the homing mechanism which are growthfactor expression as well as chemokine and extracellularmatrix receptors on the MSCs’ surfaces [34].
In a study conducted by Granero-Moltó et al., MSCs aremigrated to the fracture site via the CXCR4 receptor causingimprovement of biomechanical properties and increasing thecartilage and bone of the callus [24]. Zwingenberger et al.demonstrated that the combination of the SDF-1 releasedand bone morphogenetic protein 2 contributes to the migra-tion of the stem cell [35]. This occurrence markedly boostsbone regeneration. Apart from that, MSCs are also recruitedtowards wear-particle-related osteolysis which is indicated bythe inflammatory macrophage that is also the chemokine CCreceptor (CCR) 1 of MSCs [30, 36]. The MSCs are demon-strated to increase bone mineral density and decrease theosteolytic process [37].
1.5. Cellular Mechanism of Bone Remodelling for BoneRegeneration. Bone repair or bone regeneration is character-ized by a series of tissue transformation mechanisms includ-ing resorption and formation of hard and soft tissue.Therefore, mineralized tissue remodelling is required forthe involvement of various cell types including osteoclastand osteoblast. Osteoblasts are bone-forming cells that canbe found at the surface of bone, while osteoclasts are multi-nucleated bone-resorbing cells derived from bone marrowstem cells [38]. Bone remodelling is a cyclical process inwhich bone undergoes consistent renewal to ensure thereplacement of primary bone, to maintain calcium homeo-stasis, and especially to heal ischemic and microfracturedbone [7, 20, 32–34, 39]. This process requires a correct bal-ance of bone resorption and bone formation and thusinvolves osteoclasts and osteoblasts, respectively.
Bone remodelling consists of five consecutive phases: (1)the resorption phase, where osteoclasts break down the bonetissue, resulting in mineral release; (2) the reversal phase,where mononuclear cells appear on the bone surface; (3)the formation phase, where osteoblasts trapped in the bonematrix become osteocytes; (4) the mineralization phase,where osteocytes produce type I collagen and other sub-stances that make up the bone extracellular matrix; and (5)the termination phase [38, 40]. Resorption is initiated byosteoclast progenitors that are recruited and disseminatedinto the bloodstream. These cells proliferate and differentiateinto mature osteoclasts, aided by osteoblast stromal cells viacell-to-cell interactions. These osteoblasts express two cyto-kines, i.e., receptor activator of NF-κB ligand (RANKL) andosteoprotegrin (OPG), involved in osteoclast progenitor celldifferentiation. Under parathyroid hormone (PTH) stimula-tion, RANKL will bind to RANK, a cytoplasmic membranereceptor on osteoclast progenitor cells, to stimulate theirfusion, differentiation, and activation. In contrast, OPG
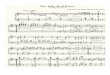
binds to RANKL to counterbalance the effect of RANKL-RANK, which thereby determines the extent of bone resorp-tion. These events are important in maintaining bonehomeostasis [41] (Figure 2). Bone resorption is terminatedwhen osteoclasts undergo apoptosis and the reversal phaseis initiated. Reversal cells may thus represent the missing linknecessary to understand the coupling between bone resorp-tion and formation. Researchers have found that reversalcells colonizing the resorbed bone surface are immature oste-oblastic cells that gradually mature into bone-forming osteo-blasts during the reversal phase and prepare the bone surfacefor bone formation [42].
1.6. Molecular Mechanism of Bone Remodelling for BoneRegeneration. The differentiation of MSCs depends on whichsignalling pathway is activated. Apart from osteoblasts, WJ-MSCs have also been demonstrated to differentiate into othermesenchymal cell lineages such as hepatocytes [43], chon-drocytes [18, 44], and adipocytes [14, 15]. The markers forosteogenic differentiation are alkaline phosphatase (ALP),an early marker of osteogenic differentiation and mineraliza-tion, and RUNX2, a runt domain-containing transcriptionfactor that is crucial for osteogenic differentiation and boneformation. The activation of RUNX2 triggers COL1 (collagentype 1), osteopontin (OPN), and osteocalcin (OC), which areosteoblast-specific markers. OPN is expressed later in the dif-ferentiation stage [45, 46]. Both OPN and COL1 are synthe-sized by osteoblasts. OC is also expressed later and isimportant for maintaining bone resorption. Osterix (Osx) isa downstream factor of Runx2 that binds to activated NFAT2in bone development [47]. A study by Zhou et al. exploredthe function of Osx where it regulates bone homeostasis afterbirth for bone and cartilage formation [26].
In osteoblasts, lineage-specific gene expression controlby specific transcription factors, i.e., Cbfa-1/RUNX2, actsto regulate osteoblastic specific gene expression [48]. Cbfa-1/RUNX2 is required for osteoblast differentiation, sinceCbfa-1 knockout mice display impaired or even absent boneformation [49, 50]. This transcription factor contains a runtDNA-binding domain, which can bind to DNA as a mono-mer or as a subunit of a monomeric complex. It binds to var-ious enhancers and promoters, including those for the genesencoding osteocalcin, osteopontin, bone sialoprotein, andGM-CSF. The expression of these proteins contributes tothe bone matrix, leading to the maturation of osteoblasts.These genes can also be used as markers for different stagesof osteoblast development [51–53].
The expression of transcription factors is controlled byseveral pathways that are activated by growth factors (GFs)that bind to a specific receptor. These growth factors includefibroblast growth factor (FGF), transforming growth factor-β(TGF-β), insulin-like growth factor (IGF), platelet-derivedgrowth factor (PDGF), and vascular endothelial growth fac-tor (VEGF) [54]. It has been reported that these GFs areresponsible for regulating the expression of Cbfa-1/RUNX2via the MAPK [55], ERK [52], and PI3K-Akt pathways [54,56]. GF binding to its receptor tyrosine kinase (RTK) acti-vates a downstream signaling cascade. The activated RTKactivates class I phosphatidylinositol 3-kinase (PI3K) or
3Stem Cells International

guanosine nucleotide-binding protein (Ras) and propagatesthe signal through direct binding or tyrosine phosphoryla-tion. This then activates Akt/PKB, IκK/IκB, or Raf/MEK,which then activates NF-κB or MAPK, accordingly. Acti-vated NF-κB and MAPK act through direct binding to phos-phorylate ERK/JNK-cJun, which then activate Cbfa1/RUNX2 gene expression. TGF-β plays important roles inosteoblast precursor recruitment, FGF enhances osteoblastrecruitment and proliferation, IGF is involved in the regula-tion of bone matrix synthesis and migration, VEGF regulatesosteoblast differentiation, and PDGF is involved in osteopro-genitor migration [51, 52]. Cumulatively, the osteogenic dif-ferentiation capability owned by WJ-MSCs supplementedwith specific GF is postulated to have a high potential forbone regeneration.
1.7. WJ-MSCs for Bone Regeneration. Albeit many have usedWJ-MSCs in the studies, the safety and efficacy of its applica-tion are indecisive particularly in bone regeneration. Thereare several aspects that need to be considered prior to usingWJ-MSCs that may influence the yield and its stemnesspotency. Different parts of the umbilical cord generateddiverse frequencies of MSCs and cell populations [6–8, 57–59]. It is known that Runx2 plays a pivotal role in osteoblastdifferentiation. In a previous study, it has shown that WJ-MSCs have lower capability to differentiate due to the highlevel of RUNX2 but lower ALP expression. ALP is importantfor matrix maturation [60, 61]. WJ-MSCs also exhibited
higher expression of pluripotent markers, OCT 4, SOX 2,and NANOG than in other parts of the umbilical cord [62].From those findings, it can be postulated that regulation ofRunx2 and pluripotent impedes ALP expression, thus need-ing a specific modulator that can serve as a molecular switchof WJ-MSCs’ fate. Current study by Bustos and colleagueshave demonstrated that JARID1B (Jumonji AT-rich interac-tive domain 1B) histone demethylase represses Runx2 inundifferentiatedWJ-MSCs. In JARID1B knockdown murine,it can be seen that Runx2 is highly expressed and ready forosteogenic commitment indicating that this molecularmechanism is relevant to modulating osteoblastic lineagecommitment [63].
1.8. Clinical Application of WJ-MSCs in Bone Regeneration.The current standard commonly used for bone tissuereplacement is bone grafting obtained from patientsthemselves (autograft) or from other individuals (allograft).However, this has raised various effects including immunore-activity and infection as well as procedure. WJ-MSCs haveproved its capability to help in bone regeneration for clinicalapplication. Qu et al. treated 36 patients with nonunion bonefracture with WJ-MSCs cultured with platelet-rich plasma(PRP) resulting in a faster recovery with no infectionrecorded compared to the other 36 patients with autoiliactreatment [64]. In another study, the intravenous injectionof 3–5 million WJ-MSCs alleviated the condition of Beckermuscular dystrophy patients with increased muscle strength,
Cbfa-1
OCNOPNBSPGM-CSF
Cbfa-1c-Jun
Cbfa-1NF-𝜅B
Akt
Ras/MEF
MAPK
ERK/JNK-c-Jun
Osteoblast
Area of bone regeneration
FGF TGF-𝛽IGF PDGF
PI3K
I𝜅K/I𝜅B
NF-𝜅B
Osteoclastprogenitor Osteoclast
RANKRANKLOPG
FusionNo fusion
Figure 2: Mechanism of bone regeneration and activation of signaling pathways.
4 Stem Cells International

improved appetite, and also improved patient’s gait [65].Recently, a patient in Indonesia with infected nonunion boneis able to walk with no pain and no postoperative compli-cations recorded after local implantation of 5 million cellssupplemented with BMP-2 and hydroxyapatite [66]. Atransplantation of autologous BM-MSCs and allogeneicWJ-MSCs in treating osteonecrosis of femoral headshowed improvement where it relieved the pain andimproved the joint function [67].
To this date, there are many various positive outcomesupon WJ-MSC treatment in clinical trials for different dis-orders including neurology [67], hematology [68], liverdiseases [69], and particularly musculoskeletal diseases[65, 70]. WJ-MSCs have a huge potential to be used asan alternative treatment for bone disorders as it does notrequire ethical issues to obtain and it is alleviatingpatients’ morbidities [71]. Since WJ-MSCs can retain thestemness and phenotypic stability compared to BM-MSCs,it has potency to be commercialised [72].
2. Methods
2.1. Search Strategy. A systematic review was conducted tosystematically assess articles on the potential of WJ-MSCsfor bone regeneration. Two databases were comprehensivelyused to search for relevant studies, i.e., Medline via Ebscohostand Scopus. For search term keywords, the combination ofwords used was “Wharton’s jelly” AND “osteo∗” OR “bone”.
2.2. Selection Criteria. The year limit for searches was from1961 to 2018, and only studies published in English wereconsidered. The search outcomes identified all articlescontaining the words Wharton’s jelly, umbilical cord, osteo-genesis, osteogenic, and bone. Databases were searched indi-vidually to ensure all relevant studies were considered. Thetitles and abstracts were carefully screened for eligibilityrelated to the topic of interest. Primary studies related tobone formation or bone regeneration were included. Reviewarticles, news articles, letters, editorials, and case studies wereexcluded from the search.
2.3. Data Extraction and Management. Data were extractedfrom each eligible article by two reviewers. The selectedpapers were screened in several phases prior to inclusion.First, the titles that were not relevant to the topic wereexcluded. Next, the abstracts of the papers were screened,and unrelated studies were excluded. All duplicates wereremoved. The following data were summarized from theselected studies: (1) authors, (2) type of study, (3) subject/sample, (4) induction factor, (5) methodology, (6) results,and (7) conclusions.
3. Results
3.1. Search Results. The primary searches identified 386 arti-cles: 41 articles came from Medline and 345 articles werefound in Scopus. To minimize bias and improve the strengthof the related articles, two reviewers independently assessedthe articles according to the inclusion and exclusion criteria.There were 244 articles removed as they were unrelated to
either Wharton’s jelly or osteogenesis/bone. A joint discus-sion was conducted to achieve consensus where differencesemerged during the assessment. From the 142 remainingarticles, 50 duplicates were removed before full articles wereretrieved. From 92 articles, 74 articles were rejected basedon the inclusion criteria as the articles were not primary stud-ies, were not related to Wharton’s jelly or osteogenesis, orwere not available as full articles. Finally, a total of 18 studieswere selected for data extraction in this review. The flowchart of the selection process is shown in Figure 3.
3.2. Study Characteristics. All studies were published between1961 and 2018. An article reported on animal studies(in vivo), two articles on both in vitro and in vivo assess-ments, and 14 articles on in vitro studies. There were six arti-cles which included scaffold fabrication in the study. Threeout of six scaffold studies involved the optimization of thescaffold component for better bone regeneration. Elevenstudies proposed a different type of tissue as the MSC source.From the generated data, we classified the articles into twosubgroups: (1) chemical methods to promote osteogenesisand (2) physical methods (scaffolds) to promote osteogene-sis. A summary of the studies is provided in Table 1.
4. Discussion
The database search provided 18 articles related to Whar-ton’s jelly, umbilical cord, osteogenesis, osteogenic lineage,and bone. From these articles, various tissue sources wereassessed for potential MSCs. Each of these sources was exam-ined regarding MSC differentiation capacities into the adipo-genic, chondrogenic, and osteogenic lineages. This reviewassessed the osteogenic potential of WJ-MSCs, which mayhave remarkable potential for bone regeneration in the clinic.
4.1. Mesenchymal Stem Cells: Potential Sources. Mesenchy-mal stem cells (MSCs) have attracted attention because oftheir unique plasticity and ability to differentiate into multi-ple cell lineages, i.e., osteoblasts, chondrocytes, and adipo-cytes, with potential for clinical usage. The bone marrow isa primary source of MSCs. However, it has been reportedthat the frequency as well as the differentiation potential ofBM-derived MSCs (BM-MSCs) decline with increasing age[73]. Therefore, alternative sources of MSCs are needed,especially those that can be obtained noninvasively. Cur-rently, various tissues are under consideration for MSC isola-tion, including adipose tissue, muscle, amniotic fluid,menstrual blood [74, 75], fetal blood [76], and periodontalligaments (PDL) [61]. The human umbilical cord is a prom-ising source of MSCs, as MSCs can be isolated either from thewhole umbilical cord [16, 77], the umbilical vein subendothe-lium [78], or WJ [14, 19, 74]. One group of researchersdivided the umbilical cord into three anatomical segments,i.e., the maternal, middle, and fetal segments [79]. They dem-onstrated that MSCs from the maternal and fetal segmentsdisplayed greater viability, possessed significantly higher pro-liferation rates, and underwent more complete osteogenicdifferentiation, showing that these segments are a goodsource of MSCs for bone tissue engineering [79].
5Stem Cells International

It is important to characterize cells derived from tissuesto determine the type of cell population that exists in thepreparation. A heterogeneous population could influencethe differentiation properties, specifically the osteogenicpotential of MSCs for bone regeneration. There are a few sur-face markers that are commonly reported for MSCs such asCD13, CD29, CD44, CD73, CD90, CD105, and CD166.MSCs do not express CD31, CD144, and CD309 (endothelialcell markers) or CD14, CD34, CD45, CD117, and CD133(hematopoietic cell markers) [61, 79].
4.2. Wharton’s Jelly Mesenchymal Stem Cells UndergoOsteogenic Differentiation. WJ-MSCs have been shown tohave good potential for osteogenic differentiation. These cellsdisplay all features of functional osteocytes/osteoblasts basedon osteogenic gene expression, extracellular matrix (ECM)mineralization, and the ability to adhere to a fabricatedscaffold [80, 81]. Although WJ-MSCs have been broadlyinvestigated, there are still problems when it comes to trans-plantation, as an immune response and rejection could occur[82]. In the database search, we only found one article thatused autoserum for WJ-MSCs in vitro as a substitute forFBS to reduce the rejection rate. Autoserum is serumobtained from the umbilical cord blood. Baba et al. reported
that the cell culture medium using autologous serum is supe-rior in quality to medium using FBS. WJ-MSCs cultured inautologous serum exhibited successful osteoblastic andadipogenic differentiation. The WJ-MSCs were then trans-planted subcutaneously into nude mice, and their potentialto form bone was proven [16].
4.2.1. Chemical Induction. Seven studies out of 18 selectedarticles used chemical factors to promote osteogenesis inWJ-MSCs. Batsali et al. [83] demonstrated that WJ-MSCsare able to differentiate into the osteogenic lineage,although this was inferior compared to BM-MSCs. Theydemonstrated that WISP1, a canonical Wnt pathway targetprotein, was able to promote better osteogenic differentia-tion in WJ-MSCs [83]. A study by Szepesi et al. [61]showed that adipose tissue-derived mesenchymal stemcells (AT-MSCs) and periodontal ligament-derived mesen-chymal stem cells (PDL-MSCs) have excellent potential forbone replacement applications and better endothelial dif-ferentiation ability as compared to WJ-MSCs [61]. Thehigh degree of calcification in AT-MSCs and PDL-MSCsdemonstrates that calcium deposition was better as com-pared to WJ-MSCs for generating vascularized bone grafts[61]. Similar findings were reported by [84] where AD-
Search of electronic databasesMedline = 41, Scopus = 345
Total = 386
Identification of abstractsMedline = 94, Scopus = 48
Total = 142
Removal of abstracts due to duplicates = 50
Primary screening of abstracts = 92
Rejection of abstracts based on selection criteria(74 articles)
(i) Not primary studies = 53(ii) Not related with Wharton’s jelly and/or
osteogenesis = 14(iii) Not a full article = 7
Selected abstractsScopus = 6
Medline =12
Full articles obtainedScopus = 6
Medline = 12Total = 18
Exclusion of unrelated papers = 244
Figure 3: Flow chart of the article selection process using the Scopus and MEDLINE databases.
6 Stem Cells International

Table1:Summaryandclassification
ofthe18
articles
selected
from
thedatabase
search.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
1.Fu
etal.
2018
[91]
Invitro
and
invivo
(i)Hum
anum
bilical
cord-derived
mesenchym
alstem
cells
(UC-M
SCs)
(ii)Sprague-Daw
ley’s
osteoblast
(iii)
Sprague-Daw
ley’s
osteoclast
Differentiationmedium
Osteogenicmedium:
(1)High-glucoseDMEM
(2)10%
serum
(3)10
−8M
dexamethasone
(4)50
ng/m
LL-ascorbicacid
(5)10
mM
β-glyceroph
osph
ate
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)MicroCTresultshow
edthat
transplantationof
UC-M
SCsincreased
bone
massin
thedistalcond
yleof
norm
alratfemur
comparedto
other
grou
ps(2)Goldn
er’sstaining
indicatedthatcompactarrangem
entof
collagenwith
lesstrabecular
thickn
essin
thegrou
pun
dergoesim
plantation
withUC-
MSC
s.Atrabeculae-likestructurecontaining
lamellaewas
detected,but
thereareno
cellarrangem
entsfoun
din
thearea
(3)Osteocalcin
(OC)staining
show
edincreasedosteocalcinlevelinOVX-
receivingUC-M
SCs
(4)Antihum
an-specificnu
cleiantigenshow
edengraftedUC-M
SCshad
differentiated
into
osteoblasts
(5)RTPCR:
(i)Hum
anosteocalcinandabun
dant
osterix(O
SX)was
detected
inovx-
receivingUC-M
SCs
(6)In
vitrococultu
resystem
show
edmoreexpression
ofalkalin
eph
osph
atase(A
LP)iftheosteoblastiscocultured
withUC-M
SCs
UC-M
SCsableto
bedifferentiated
into
osteoblast
andaresafefor
transplantationin
bone
diseasetreatm
ent.
Osteoclastdifferentiation
(1)10
or100ng
RANKL
2.AlJofi
etal.
2018
[92]
Invitro
(i)Wharton
’sjelly
mesenchym
alstem
cells
(WJ-MSC
s)
(i)10
μmol/L
metform
in(antidiabetic
drug)
(i)Com
mercialUC-
MSC
s(ii)Partof
UC:n
otmention
ed
Metform
in-treated
UC-M
SCsincreasedin
mineralizationstainedthrough
Alizarin
Red
Staining.B
utin
OCT-1-(organiccation
transporter-)siRNA-
transfectedcells,a
significant
decrease
incalcium-richno
duleform
ation
was
observed.
OCT-expressingWJ-MSC
shave
theability
tobe
differentiated
into
osteoblastswhenindu
ced
withmetform
in.
3.Bhartietal.
(2018)
[44]
Invitro
(i)Wharton
’sjelly
mesenchym
alstem
cells
(WJ-MSC
s)
(i)Osteogenicmedium
(1)ADMEM
(2)0.1mM
dexamethasone
(3)50
mM
ascorbicacid
(4)10
mM
glycerol-2-pho
sphate
(ii)Adipo
genicmedium:
(1)ADMEM
(2)500mM
isobutyl
methylxanthine
(3)1mM
dexamethasone
(4)Insulin
(5)100mM
indo
methacin
(6)10
mM
insulin
(iii)
Cho
ndrogenicmedium
using
comer
(1)Stem
Pro1O
steocyte/
Cho
ndrocyte
DifferentiationBasal
Medium;StemPro1
Cho
ndrogenesissupp
lement;
Gibco).
(2)Hepatocyte
(3)ADMEM
(4)2%
FBS
(5)10
ng/m
lofon
costatin
M(6)10
nmol/L
dexamethasone
(7)1%
insulin
transferrin-selenium
(i)Explant
metho
d(ii)Partof
UC:
maternal,middle
andfetal
segm
ents
(1)Bon
eno
dules:form
edby
cells
from
allsegments
(2)Cho
ndrogenicpo
tential:occurred
incells
from
allsegments
WJ-MSC
sareagood
cell
source
forautologous/
allogeneicstem
cellsource.
4.Batsalietal.
2017
[83]
Invitro
(i)Bon
emarrow
mesenchym
alstem
cell(BM-M
SCs)
(ii)Wharton
’sjelly
Differentiationmedium:
Osteogenicmedium:
(1)High-glucoseDMEM
(2)10%
serum
(3)10
−7M
dexamethasone
(i)Explant
metho
d(ii)Partof
UC:
maternal,middle,
andfetal
segm
ents
(1)Osteogenicdifferentiation(A
lizarin
Red
andvonKossa
staining):WJ-
MSC
sshow
edsimilarstaining
potentialasBM-M
SC(2)Real-time-
(RT-)PCR:
(i)Osteocyte-related
gene
expression
:higherexpression
ofRun
t-related
transcriptionfactor
2(RUNX2),distal-lessho
meoboxprotein5(D
LX5),
The
osteogenic
differentiationpo
tentialo
fWJ-MSC
sisregulatedby
WISP1andsFRP4,
respectively.
7Stem Cells International

Table1:Con
tinu
ed.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
mesenchym
alstem
cells
(WJ-MSC
s)(4)25
μg/mLL-ascorbicacid
(5)3mM
NaH
2PO4
osteocalcin(O
CN),andalkalin
eph
osph
atase(A
LP)by
BM-M
SCs
(3)Differentialexpression
ofWNTligands;sFR
P4(secretedfrizzled-related
protein4)
andWISP1(W
NT1-indu
ciblesignallin
gpathway
protein1)
weresignificantlyredu
cedin
WJ-MSC
s(4)WISP1im
plicated
inosteogenicdifferentiation;
RUNX2,ALP
,and
OSC
weresignificantlyup
regulated
5.Zajdeletal.
2017
[84]
Invitro
(i)Adipo
setissue
(AT-
MSC
s)(ii)WJ-MSC
s
Osteogenicmedium
(Lon
za):
(1)Dexam
ethasone
(2)Ascorbicacid
(3)β-G
lyceroph
osph
ate
(i)Com
mercialAT-
MSC
sandUC-
MSC
s(ii)Partof
UC:n
otmention
ed
(1)Calcium
depo
sition
byAlizarin
Red
staining
(i)Calcium
depo
sition
was
greaterin
AT-M
SCswhencomparedto
WJ-
MSC
s(2)ALP
activity
(i)ALP
activity
was
higher
inAT-M
SCswhencomparedto
WJ-MSC
s(3)Osteoprotogerin
(OPG)secretion
(i)Bothosteo-indu
cedcelltypesshow
edhigh
OPGsecretionwhen
comparedto
control
(4)Osteocalcin
(OC)secretion
(i)OCsecretionwas
higher
inWJ-MSC
swhencomparedto
AT-M
SCs
WJ-MSC
shave
theability
todifferentiateinto
the
osteogeniclin
eage.
6.Mechiche
Alamietal.
2017
[88]
Invitro
(i)WJ-MSC
sCalcium
phosph
ate(CaP)substratebu
ild-
up(w
itho
utosteogenicindu
ction
(i)Com
mercialUC-
MSC
s(ii)Partof
UC:n
otmention
ed
(1)Geneexpression
analysis
(i)Day
7:Run
t-relatedtranscriptionfactor
2(RUNX2)
andsecreted
phosph
oprotein
1(SPP-1)wereup
regulated
(ii)Day
14:collagentype
1Alpha
1(COL1
A1)
andALP
wereup
regulated
(iii)
Day
21:bon
egamma-carboxyglutamicacid-con
tainingprotein(BGLP
)andALP
wereup
regulated
(2)Nod
ulecharacterization
(i)Hem
atoxylin-eosin-saff
ron(H
ES)
staining
revealed
continuo
uslayersof
cells
atthesurfaceof
theno
dulewithrand
omlydistribu
tedcells
embedd
edwithinfibrou
stissues
(ii)Masson’strichrom
estaining
show
edthepresence
ofgreen-stained
fibrou
stissue
compo
sedof
newlyform
edcollagen
Excellent
osteogenic
potentialofsprayed
CaP
and
WJ-MSC
sin
bone
tissue
engineering
7.Szepesietal.
2016
[61]
Invitro
(i)WJ-MSC
s(ii)AT-M
SCs
(iii)
Periodo
ntal
ligam
entMSC
s(PDL-MSC
s)
Differentiationmedium:
(i)Stem
Pro
OsteogenesisDifferentiation
kit
(ii)Stem
Pro
Cho
ndrogenesis
Differentiationkit
(iii)
Stem
Pro
Adipo
genesisDifferentiation
kit
(iv)
End
othelialC
ellG
rowth
Medium
(i)Enzym
atic
digestionUC-
MSC
s(ii)Partof
UC:n
otmention
ed
(1)Osteogenicdifferentiation:
AT-M
SCsandPDL-MSC
sshow
edgreater
calcium
depo
sition
(2)Osteogenicdifferentiationassessed
viaRT-PCR:
(i)Run
t-relatedtranscriptionfactor
2(RUNX2):allcelltypesshow
edhigh
expression
afterindu
ction
(ii)Alkalineph
osph
atase(A
LP):AT-M
SCsandPDL-MSC
sshow
edincreasedexpression
,but
ALP
was
significantlylower
inWJ-MSC
s(iii)
Calcium
depo
sition
:AT-M
SCsandPDL-MSC
sshow
edgreatercalcium
depo
sition
ascomparedto
WJ-MSC
s(3)There
was
asignificant
correlationbetweenCD90
expression
and
thelevelsof
calcium
depo
sition
indifferentMSC
isolates
WJ-MSC
shave
osteogenic
potentialand
aregood
cell
sourcesforbone
regeneration
.
8.Lim
etal.
2016
[79]
Invitro
Hum
anWJ-MSC
s(i)Fetalsegment
(ii)Maternalsegment
(iii)
Middlesegm
ent
(i)Osteogenicmedium
(1)Alpha-M
EM
(2)Dexam
ethasone
(3)Ascorbicacid
(4)β-G
lycerolp
hosphate
(ii)Adipo
genicmedium:
(1)DMEM/F12
(2)3-Isobutyl-3-m
ethylxanthine
(3)Dexam
ethasone
(4)Insulin
(iii)
Cho
ndrogenicmedium
(1)Alpha-M
EM
(i)Enzym
atic
digestion
(ii)Maternal,middle,
andfetal
segm
ents
Bon
eno
dules:form
edby
cells
from
allsegments
WJ-MSC
sareagood
cell
source
forbone
regeneration
.
8 Stem Cells International

Table1:Con
tinu
ed.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
(2)Transform
inggrow
thfactor
3(TGF-β3)
9.Kargozar
etal.2018
[80]
Invitro
and
invivo
(i)BM-M
SCs
(ii)AT-M
SCs
(iii)
UC-M
SCs
(i)Nanocom
posite
scaffolds
(3D
bioactive
glass/gelatinscaffolds
(BaG
/Gel)
consisting
ofSiO2-P2O
5-CaO
(64%
SiO2,5%
P2O
5,and31%
CaO
).
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
Invitrostud
y(1)Cellviability:
(i)Scaffoldhadno
significant
inhibitory
effecton
MSC
proliferation
over
time
(ii)MSC
proliferation
gradually
increasedwithincubation
time
BM-M
SCs,grow
non
BaG
/Gelnano
compo
site
scaffolds,are
possible
sourcesforbone
regeneration
.
Invivo
stud
y(1)Histologicalo
bservation
s:(i)H&Estaining:allMSC
-seededscaffolds
successfullygeneratednew
bone
anddemon
stratedan
ongoinghealingprocessat
4and12
weeks
aftertransplantation.
The
UC-M
SC-seededscaffoldshow
edsignificantlyincreasedneovascularization
comparedto
theothers
(ii)IH
Cstaining:increased
expression
ofOCN
andALP
intheBM-M
SC-
seeded
scaffold.
Vascularendo
thelialgrowth
factor
(VEGF)
expressed
inallthe
grou
psof
treatedcell/scaffold.
Increasedneovascularization
withtheUC-M
SC-seededscaffold
(iii)
Histomorph
ometry:B
M-M
SC-seededscaffolds
show
edmorebone
regeneration
at4and12
weeks
10.
Tod
eschi
etal.2015
[81]
Invivo
(i)UC-M
SCs
(ii)BM-M
SCs
(i)Ceram
icscaffolds
(Skelite;
4×4×4mm
cubesof
33%
hydroxyapatiteand67%
silicon
-stabilizedtricalcium
phosph
ate,Si-
TCP)
(ii)Platelet-rich
plasma(PRP)
(iii)
Con
dition
edmedium
(CM)
(i)Explant
metho
d(ii)Partof
UC:n
otmention
ed
(1)Histologicalassessm
entrevealed
theform
ationan
immaturebone-like
structures
andcompactfibrou
stissue
inUC-M
SC-seededconstructs
(2)Polarized
light
exam
inationrevealed
lessorganizedcollagenfibersin
the
UC-M
SC-seededscaffolds.T
heim
maturebone-likematrixin
UC-M
SC-
seeded
scaffolds
was
mostly
filledwithalooseconn
ective
tissue
(3)Histologicalevaluationin
anorthotop
icmou
semod
elshow
edthatno
neof
thebone
defectshadcompletelyclosed.H
owever,goldMTCstaining
indicatedthepresence
ofredbloodcells
inbloodvessel-likestructures
which
issignificant
intheUC-M
SC-transplantedgrou
p(4)Osteocyteswereclearlydetectablein
theBMMSC
-seededscaffolds
(5)How
ever,hum
anALU
sequ
enceswereno
tdetectedin
osteocytes
within
thenewlyform
edbone
intheUC-M
SCim
plantsandno
nseeded
implants
UC-M
SCsprom
otebone
regeneration
.
11.
Karadas
etal.2014
[74]
Invitro
(i)WJ-MSC
s(ii)BM-M
SCs
(iii)
Menstrualblood
mesenchym
alstem
cells
(MBMSC
s)
(i)Collagenscaffolds
within
situ
calcium
phosph
ate(CaP)
(ii)Differentiationmedium:
(1)High-glucoseDMEM
(2)10
nMdexamethasone
(3)50
μg/mLascorbicacid
(4)10
mM
β-glyceroph
osph
ate
(5)10%
FBS
(6)100un
its/mLpenicillin
(7)100μg/mLstreptom
ycin
(i)Explant
metho
d(ii)Partof
UC:n
otmention
ed
(1)Cellp
roliferationassays:
(i)WJ-MSC
son
tissue
cultu
repo
lystyrene(TCPS)
andcollagenwitho
utCaP
treatm
entincreasedproliferation
(2)Cellattachm
ent(fluo
rescence
staining):
(i)Goodattachmentof
both
celltypesto
thescaffold
(ii)Con
focalm
icrographs
show
edthatthecells
wereableto
penetrateinto
thepo
res
(3)Osteogenicdifferentiation:
(i)ALP
assay:
(a)WJ-MSC
sshow
edbetter
differentiationon
untreatedandCaP-
containing
foam
sthan
ingrow
thmedium
(b)ALP
levelswerehigherin
WJ-MSC
sgrow
non
CaP-freefoam
sthan
onTCPS
(c)ALP
activity
was
significantlyhigher
incells
grow
non
collagenwith
CaP
crystalsform
edin
situ
forboth
WJ-MSC
sandMBMSC
s(days14
and21)
Collagenfoam
withtheuse
ofCaP
crystalsform
edin
situ
enhances
theosteogenic
indu
ctionof
WJ-MSC
s.
vonKossa
staining:
(1)WJ-MSC
shadhigher
ALP
activity
anddenser
mineraldepo
sition
comparedto
MBMSC
s
9Stem Cells International

Table1:Con
tinu
ed.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
12.
Ram
esh
etal.2014
[93]
Invitro
(i)WJ-MSC
s
(i)Hydrogelalginatemicrospheres
(ii)Osteogenicdifferentiationmedia:
(1)Basalmedium
(2)10
mM
β-glyceroph
osph
ate
(3)1mM
dexamethasone
(4)5mg/mLascorbicacid
(i)Explant
metho
d(ii)Partof
UC:n
otmention
ed
(1)Characterizationof
osteod
ifferentiated
WJ-MSC
svia:
(i)Bradfordassay:calcium
depo
sition
increasedin
2%alginate
(ii)Alizarin
Red
staining:excellent
matrixmineralizationin
WJ-MSC
sim
mobilizedon
2%alginate
(iii)
Immun
ocytochemicalanalysis(osteocalcin):significant
expression
ofosteocalcinin
WJ-MSC
aggregates
in1.5%
and2%
alginateat
day21
(2)Genotypicanalysisof
encapsulated
WJ-MSC
sshow
edthat
OCN
andRun
x2wereup
regulatedin
1.5%
and2%
alginate
WJ-MSC
sencapsulated
inhydrogelalginate
microsphereshave
osteogenicpo
tentialfor
stem
cell-basedtissue
engineering.
13.
Babaetal.
2012
[16]
Invivo
&in
vitro
Hum
anum
bilicalcord
mesenchym
alstem
cells
(hUC-M
SCs)
Differentiationmedium:
(i)NH
OsteoDiff
Medium
(ii)NH
Adipo
Diff
Medium
(iii)
rhBMP2
(iv)
Scaffold
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(3)Osteogenicdifferentiation:
strong
calcium
depo
sition
Adipo
genicdifferentiation:
lipid
drop
letprod
uction
(4)H&Estaining:p
ositiveforbone
tissue
prod
ucingosteocalcin(O
CN)
(5)RT-PCR:h
ighexpression
ofRUNX2,ALP
,and
OCN
ascomparedto
undifferentiated
cells
UC-M
SCssupp
lemented
withgrow
thfactorsand
serum
have
osteogenic
differentiationpo
tentialfor
bone
regeneration
.
14.
Penolazzi
etal.2012
[89]
Invitro
(i)WJ-MSC
s(i)Porcine
urinarybladdermatrix(pUBM)
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)Proliferationassays
show
ed(i)pU
BM
didno
thave
aneffecton
cells
insuspension
cond
itions
but
affectedcells
cultu
redin
adherent
cond
itions
(ii)Viablecells
wereho
mogenou
slydistribu
tedover
theentire
scaffold
(2)TUNELassays
show
ed(i)Noapop
tosisin
hWJ-MSC
scultu
redin
agarose-coated
wellswith
increasing
amou
ntsof
pUBM
(ii)The
scaffoldup
regulatedcyclin
D1
(iii)
Matrixmetanop
roteinase(M
MPI3)w
aslowerbu
tthisdidno
taffect
β-catenin
(3)Morph
ologicalcharacterization
:(i)Scanning
electron
microscop
e(SEM)analysisshow
ed(a)There
was
asignificant
interactionbetweenthecells
andthe
biom
aterial
(b)WJ-MSC
scompletelywereenvelopedin
pUBM
particlesto
form
smooth
spheroids,displaying
anECM
networkcovering
thesurface
(c)The
cells
andthebiom
aterialformed
adensestructure
(ii)X-ray
energy-dispersivespectroscopy
(EDX)show
edthatspheroids
inosteogenicmedium
containedhigh
amou
ntsof
calcium
and
phosph
orou
s(highdegree
ofmineralization)
(iii)
Transmission
electron
microscop
y(TEM)show
edthepresence
offocalcon
tactsbetweencells
andthepU
BM
scaffold
(4)RT-PCR:
(i)RUNX2expression
was
notaffectedby
pUBM,but
increasedup
onosteoind
uction
(ii)WJ-MSC
sseeded
onpU
BM
wereableto
prod
uceCol
IAIandOPN
after21
days
inosteogenicmedium
(iii)
WJ-MSC
sshow
edincreasedALP
activity
andability
todepo
sit
mineralized
matrix
(iv)
OPN
expression
was
higher
incells
grow
non
pUBM
scaffolds
inosteogenicmedium
than
inosteogenicmedium
alon
e
The
combination
ofWJ-
MSC
sandpU
BM
show
sthe
prom
iseof
scaffolds
forbone
regeneration
.
15.
Wangetal.
2011
[94]
Invitro
(i)UC-M
SCs
(i)Poly-L-lacticacid
(PLL
A)scaffold
(ii)Osteogenicindu
ctionmedium:
(1)Lo
w-glucose
DMEM
(2)10%
FBS
(3)1%
penicillin/streptom
ycin
(4)100nM
dexamethasone,
(5)10
mM
sodium
β-
glycerop
hosphate,
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)Biochem
icalassays
wereperformed
toassess
(i)DNAcontent:osteogenicpartsof
theC-cell-Ocompo
siteshadhigher
DNAcontentsthan
theO-O
compo
sitesandtheosteogenicpartsof
theC-O
compo
sites
(ii)Glycosaminoglycan(G
AG)content:allosteogenicgrou
pshadsimilar
GAGcontents
(iii)
Hydroxyproline(H
YP)content:osteogenicgrou
pshadasignificantly
higher
HYPcontent
WJ-MSC
sareasuitablecell
source
forasand
wich
approach
strategy
inosteocho
ndraltissue
engineering.
10 Stem Cells International

Table1:Con
tinu
ed.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
(6)50
μg/mLascorbicacid
2-ph
osph
ate(A
A2P
)(7)10
nM1α
,25-dihydroxyvitam
inD3
(i)Cho
ndrogenicindu
ction
medium:
(1)High-glucoseDMEM
(DMEM-
HG)
(2)1%
nonessentialam
inoacids
(NEAA)
(3)1x
sodium
pyruvate
(4)1x
insulin
-transferrin-selenium
prem
ix(ITS)
(5)50
μg/mL(A
A2P
)(6)40
μg/mLL-proline
(7)100nM
dexamethasone
(8)10
ng/m
LTGF-β1
(iv)
Calcium
content:osteogenicgrou
psshow
edsignificantlyincreased
calcium
levelsover
time
(2)Histologicalanalyses:po
sitive
Alizarin
Red
staining
inthe
osteogenicgrou
p(3)RT-PCR:
(i)Collagentype
II(ColII):no
texpressedin
theosteogenicgrou
p(ii)Collagentype
I(ColI):u
pregulated
inallgroup
s(iii)
RUNX2:increasedin
theosteogenicgrou
p(iv)
Aggrecan:
increasedsignificantlyin
chon
drogenicgrou
p
16.
Schn
eider
etal.2010
[85]
Invitro
Hum
anmesenchym
alstem
cells
(hMSC
):(i)UC-M
SCs
(ii)BM-M
SCs
(i)Scaffold:
3Dcollagengel
(ii)Osteogenicindu
ctionmedium:
(1)Lo
w-glucose
DMEM
(2)10%
FCS
(3)100nM
dexamethasone
(4)10
mM
sodium
β-
glycerop
hosphate
(5)0.05
mM/L-ascorbicacid
2-ph
osph
ate
(iii)
Adipo
genicindu
ctionmedium:
(1)DMEM
high
glucose
(2)1μM
dexamethasone
(3)0.2mM
indo
methacin
(4)0.01
mg/mLinsulin
(5)0.5mM
3-isobutyl-1-
methylxanthine
(6)10%
FCS
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)Scaffold:
(i)3D
collagengelu
nderwentprogressivecontraction
(ii)After
osteogenicdifferentiation,
collagengelswerestronger
and
harder
withBM-M
SCsandUC-M
SCs
(2)Characterizationof
BM-M
SCsandUC-M
SCsby
(i)Osteogenicdifferentiation:
UC-M
SCsshow
edincreasedextracellular
matrix(ECM)depo
sition
byAlizarin
Red
(AR)staining
(ii)Adipo
genicdifferentiation:
UC-M
SCsshow
edalim
ited
numberof
smalllipid
vacuoles
stainedby
OilRed
O(O
RO)
(iii)
Immun
ofluo
rescence:positiveexpression
ofcollagenIV
andlaminin
inUC-M
SCsafter21
days
ofosteogenicdifferentiationon
collagen
gels
(iv)
Immun
ohistochem
istryanalyses:p
ositiveexpression
ofosteop
ontin
(OPN)andbispho
spho
nate
[2-(2-pyridinyl)ethylid
ene-BP](PEBP)
inthecollagengel
(3)TEM
analysis:
(i)Osteogenicdifferentiation:
contractionof
thecollageno
usmatrixon
the
UC-M
SC-seededcollagensurface
(ii)Adipo
genicdifferentiation:
UC-M
SC-derived
lipid
vacuoles
weresm
all
andstainedwithtoluidineblue
(4)RT-PCR:U
C-M
SCsexpressedcollagenI,collagenIII,collagenIV
,andlaminin
(5)Cellm
igration
:migrating
UC-M
SCsappeared
asspindle-shaped
cells
withelon
gatedcytoplasmicprocesses
UC-M
SCshave
asignificant
therapeuticim
pactin
bone
tissue
engineeringin
the
future.
17.
Hsieh
etal.
2010
[14]
(i)In
vitro
(i)WJ-MSC
s(ii)BM-M
SCs
Osteogenicdifferentiationmedium:
(1)DMEM
(2)10%
FBS
(3)0.1mM
dexamethasone
(4)10
mM
β-glyceroph
osph
ate
(5)50
mM
ascorbicacid
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)Array
data
show
edthat
both
BM-M
SCsandWJ-MSC
sexpressed
multilin
eage
differentiationprop
erties.
(2)Real-time-PCR:
BM-M
SCs>WJ-MSC
sin
term
sof
(i)Adipo
cyticmarkerexpression
:lipoprotein
lipase(LPL),leptin,
peroxisomeproliferator-activatedreceptor
gamma(PPARγ),and
fattyacid-binding
protein4(FABP4)
(ii)Lipidaccumulation
(3)Osteogenicdifferentiationpo
tential
(i)BM-M
SCs>WJ-MSC
swhencultu
redin
definedMesenCult
(ii)Expressed
higher
levelsof
ALP
,SPP-1,and
RUNX2
WJ-MSC
sarecapableof
differentiatinginto
the
osteogeniclin
eage,but
BM-
MSC
saresuperior.
11Stem Cells International

Table1:Con
tinu
ed.
No.
Autho
rand
year
Typeof
stud
ySubject/sample
Indu
ctionfactor
WJ-MSC
isolation
metho
dResults
Con
clusion
(iii)
BM-M
SCs>WJ-MSC
swhencultu
redin
definedcultured
in10%
FBS:
(a)Expressed
higher
levelsof
ALP
,osteopo
ntin,and
RUNX2
(4)ALP
staining
(betterosteogenicability)
18.
Hou
etal.
2009
[15]
(i)In
vitro
(i)hU
C-M
SCs
(ii)BM-M
SCs
(i)BMP-2
treatm
ent:
(a)Bon
emorph
ogeneticprotein2-
blocking
antibodies
(BMP2Ab)
(b)Recom
binant
human
BMP2
(rhB
MP2)
(c)Noggin
(ii)Osteogenicdifferentiationmedium:
(1)DMEM/F12
(2)10%
FBS
(3)Dexam
ethasone
(4)Ascorbicacid
(AsA
)2-
phosph
ate
(5)β-G
lyceroph
osph
ate
(iii)
Adipo
genicdifferentiation
medium:
(1)DMEM/F12
(2)1%
FBS
(3)100nM
dexamethasone
(4)1nM
insulin
(iv)
Cho
ndrogenicdifferentiation
medium:
(1)DMEM/F12
(2)Dexam
ethasone
(3)AsA
(4)TGF-β1
(5)ITS+
Premix
(i)Enzym
atic
digestion
(ii)Partof
UC:n
otmention
ed
(1)Trilin
eage
differentiation
(i)Osteogenesis:osteon
ectin,
ALP
,and
RUNX2wereexpressed
(ii)Cho
ndrogenesis:COLII,collagentype
X(COLX),andaggrecan
were
expressed
(iii)
Adipo
genesis:adipsin,
PPARγ,andlip
oprotein
lipase
(2)ALP
activity
was
significantlyincreasedin
BMP2-indu
cedUC-
MSC
s(i)Western
blot
revealed
activation
oftheBMP2signalingpathway
inboth
celltypesviaSM
ADs,p38,andextracellularregulatedkinase
activation
BMP2-indu
cedUC-M
SCs
have
good
osteogenic
differentiation(ind
icated
bytheactivation
ofBMP2
signaling)
andmay
beused
intissue-engineeredbone.
12 Stem Cells International

MSCs were found to be superior to WJ-MSCs in terms ofdifferentiating into the osteogenic lineage after 21 dayscompared. In a different study by Lim and colleagues,MSCs derived from different parts of the umbilical cord,i.e., the fetal, middle, and maternal segments, have theability to differentiate into osteogenic lineage cells usingthe osteogenic medium consisting of dexamethasone,ascorbic acid, and β-glycerophosphate. The fetal part wasshown to have the best differentiation potential [79]. Astudy by Hsieh et al. [14] showed that BM-MSCs expressmore osteogenic genes compared to WJ-MSCs; conversely,WJ-MSCs are more responsible for angiogenesis [66].Bone morphogenetic protein 2 (BMP-2) was used in astudy by Hou et al. to promote osteogenic differentiationin WJ-MSCs [15].
4.2.2. Physical Induction. It is noteworthy that the microenvi-ronment influences cell behaviour and leads to the pro-duction of a specific chemical composition that buildsthe ECM. Therefore, fabricated scaffolds have been activelyinvestigated to find better materials and to produce thebest structure of ECM-like components. From the databasesearch, eight out of 18 articles investigated the fabricationof various scaffolds to test the potential of WJ-MSCs topromote complex bone regeneration. Various biomaterialswere used to construct these scaffolds, ranging from colla-gen hydrogels [85] to bioactive glass [80]. 3D scaffoldshave been documented as one of the best carriers for celldelivery in bone regeneration. The ideal scaffold shouldbe osteoconductive, biocompatible, and bioresorbable; pos-sess interconnected porosity; and promote cell binding/attachment [82, 86].
The first phase in scaffold development used collagen asthe main organic component in bone tissue for bone grafting[85]. Collagen type I can be isolated from Sprague-Dawley rattails after processing and pelleting. Genipin has been selec-tively used for crosslinking collagen scaffolds to improvethe stability and mechanical strength of the scaffolds in theculture medium [74]. Other crosslinkers have also been used,such as glutaraldehyde and formaldehyde. However, thosehave been reported to have some cytotoxic effects [87]. Cal-cium phosphate is another major constituent in bone thathas been widely studied as a scaffold material for bone tissueengineering [88]. A study by Karadas et al. [74] produced anin situ mineralized collagen scaffold whereby, after crosslink-ing with genipin, the scaffold was immersed in a calcium andphosphate solution. As a result, highly integrated calciumphosphate minerals were successfully formed [74]. The com-bination of collagen I and III has also been reported to resem-ble the native ECM, where umbilical cord MSCs (UC-MSCs)were found to have better osteogenic potential compared toBM-MSCs [85]. In addition, porcine ECM, derived fromthe urinary bladder, has also been used as a biomaterial forscaffold preparation as it contains collagen, glycoproteins,glycosaminoglycans, and GFs [89].
Scaffold design then moved to the second phase, inwhich bioactive glass has been used as a scaffold in bonetissue engineering [80]. Kargozar and colleagues used acombination of bioactive glass/gelatin (BaG/Gel) scaffolds,
aiming for a highly porous structure, which is consideredideal for bone substitution. A comprehensive physiochem-ical analysis showed that the structure had an intact, 3Dporous microstructure with interconnected pores. It wasalso shown that the properties were very close to thoseof natural spongy bone [80]. They demonstrated that neo-vascularization was significantly better in the UC-MSC-seeded scaffold when compared to the BM-MSC-seededscaffold, indicating that the BaG/Gel scaffold is MSCtype-dependent. A study by Todeschi and colleagues usedhydroxyapatite (HA), beta-tricalcium phosphate (β-TCP),or a mixture of the two [81] as the scaffold. They showedthat a significantly higher number of blood vessels werepresent in the UC-MSC-seeded implants [81].
5. Conclusion
WJ-MSCs were first isolated by Mitchell et al. in 2003.During embryogenesis, totipotent cells such as primordialgerm cells and hematopoietic stem cells migrate from theyolk sac through this region to populate target tissues inthe embryo and fetus [90]. Characterization indicated thatthese cells are stem cells, as they express c-kit and can dif-ferentiate into neural cells. WJ-MSCs have similar prolifer-ation and differentiation capacity and have multilineagedifferentiation potential [77], including osteogenesis. Thisreview demonstrates that WJ-MSCs are capable of differ-entiation into osteoblasts, which may be useful for moreeffective bone fracture healing as these cells have beenshown to migrate into and colonize a collagenous matrix.With the aid of 3D scaffolds, cell proliferation and survivalare improved as these scaffolds provide structural stabilitysimilar to that of bone. However, MSCs have to be com-patible with the scaffold prior to integration and incorpo-ration into engineered bone.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Acknowledgments
The research was carried out with the financial support ofUniversiti Kebangsaan Malaysia and AMRUS Medik Sdn.Bhd. through research grant numbers FF-2017-482 andFF-2017-020, respectively.
References
[1] M. L. Weiss and D. L. Troyer, “Stem cells in the umbilicalcord,” Stem Cell Reviews, vol. 2, no. 2, pp. 155–162, 2006.
[2] L. Raio, F. Ghezzi, E. di Naro et al., “Prenatal diagnosis of alean umbilical cord: a simple marker for the fetus at risk ofbeing small for gestational age at birth,” Ultrasound in Obstet-rics & Gynecology, vol. 13, no. 3, pp. 176–180, 1999.
[3] E. Di Naro, F. Ghezzi, L. Raio, M. Franchi, and V. D’Addario,“Umbilical cord morphology and pregnancy outcome,” Euro-pean Journal of Obstetrics & Gynecology and ReproductiveBiology, vol. 96, no. 2, pp. 150–157, 2001.
13Stem Cells International

[4] F. A. Meyer, Z. Laver-Rudich, and R. Tanenbaum, “Evidencefor a mechanical coupling of glycoprotein microfibrils withcollagen fibrils in Wharton’s jelly,” Biochimica et BiophysicaActa (BBA) - General Subjects, vol. 755, no. 3, pp. 376–387,1983.
[5] I. B. Copland, S. L. Adamson, M. Post, S. J. Lye, andI. Caniggia, “TGF-β3 expression during umbilical cord devel-opment and its alteration in pre-eclampsia,” Placenta,vol. 23, no. 4, pp. 311–321, 2002.
[6] M. Mizoguchi, Y. Suga, B. Sanmano, S. Ikeda, and H. Ogawa,“Organotypic culture and surface plantation using umbilicalcord epithelial cells: morphogenesis and expression of differ-entiation markers mimicking cutaneous epidermis,” Journalof Dermatological Science, vol. 35, no. 3, pp. 199–206, 2004.
[7] J. E. Davies, J. T. Walker, and A. Keating, “Concise review:Wharton’s jelly: the rich, but enigmatic, source of mesenchy-mal stromal cells,” Stem Cells Translational Medicine, vol. 6,no. 7, pp. 1620–1630, 2017.
[8] K. Sobolewski, E. Bańkowski, L. Chyczewski, and S. Jaworski,“Collagen and glycosaminoglycans ofWharton’s jelly,”Neona-tology, vol. 71, no. 1, pp. 11–21, 1997.
[9] H.-S. Wang, et al.S.-C. Hung, S.-T. Peng et al., “Mesenchymalstem cells in the Wharton’s jelly of the human umbilical cord,”Stem Cells, vol. 22, no. 7, pp. 1330–1337, 2004.
[10] I. Kalaszczynska and K. Ferdyn, “Wharton’s jelly derived mes-enchymal stem cells: future of regenerative medicine? Recentfindings and clinical significance,” BioMed Research Interna-tional, vol. 2015, Article ID 430847, 11 pages, 2015.
[11] M. Dominici, K. le Blanc, I. Mueller et al., “Minimal criteria fordefining multipotent mesenchymal stromal cells. The Interna-tional Society for Cellular Therapy position statement,”Cytotherapy, vol. 8, no. 4, pp. 315–317, 2006.
[12] S. Tipnis, C. Viswanathan, and A. S. Majumdar, “Immunosup-pressive properties of human umbilical cord-derived mesen-chymal stem cells: role of B7-H1 and IDO,” Immunology &Cell Biology, vol. 88, no. 8, pp. 795–806, 2010.
[13] X. Y. Wang, Y. Lan, W. Y. He et al., “Identification of mesen-chymal stem cells in aorta-gonad-mesonephros and yolk sac ofhuman embryos,” Blood, vol. 111, no. 4, pp. 2436–2443, 2008.
[14] J.-Y. Hsieh, Y.-S. Fu, S.-J. Chang, Y.-H. Tsuang, and H.-W. Wang, “Functional module analysis reveals differentialosteogenic and stemness potentials in human mesenchymalstem cells from bone marrow and Wharton’s jelly of umbilicalcord,” Stem Cells and Development, vol. 19, no. 12, pp. 1895–1910, 2010.
[15] T. Hou, J. Xu, X. Wu et al., “Umbilical cord Wharton’s jelly: anew potential cell source of mesenchymal stromal cells forbone tissue engineering,” Tissue Engineering Part A, vol. 15,no. 9, pp. 2325–2334, 2009.
[16] K. Baba, Y. Yamazaki, S. Ikemoto, K. Aoyagi, A. Takeda, andE. Uchinuma, “Osteogenic potential of human umbilicalcord-derived mesenchymal stromal cells cultured with umbil-ical cord blood-derived autoserum,” Journal of Cranio-Maxillofacial Surgery, vol. 40, no. 8, pp. 768–772, 2012.
[17] G. la Rocca, M. Lo Iacono, T. Corsello, S. Corrao, F. Farina,and R. Anzalone, “Human Wharton’s jelly mesenchymal stemcells maintain the expression of key immunomodulatory mol-ecules when subjected to osteogenic, adipogenic and chondro-genic differentiation in vitro: new perspectives for cellulartherapy,” Current Stem Cell Research & Therapy, vol. 8,no. 1, pp. 100–113, 2013.
[18] M. Esposito, A. Lucariello, C. Costanzo et al., “Differentiation ofhuman umbilical cord-derived mesenchymal stem cells, WJ-MSCs, into chondrogenic cells in the presence of pulsed elec-tromagnetic fields,” In Vivo, vol. 27, no. 4, pp. 495–500, 2013.
[19] M.Messerli, A.Wagner, R. Sager et al., “Stem cells from umbil-ical cord Wharton’s jelly from preterm birth have neuroglialdifferentiation potential,” Reproductive Sciences, vol. 20,no. 12, pp. 1455–1464, 2013.
[20] Y. B. Cui, S. S. Ma, C. Y. Zhang et al., “Human umbilical cordmesenchymal stem cells transplantation improves cognitivefunction in Alzheimer’s disease mice by decreasing oxidativestress and promoting hippocampal neurogenesis,” BehaviouralBrain Research, vol. 320, pp. 291–301, 2017.
[21] I. Garzón, M. A. Martín-Piedra, C. Alfonso-Rodríguez et al.,“Generation of a biomimetic human artificial cornea modelusing wharton’s jelly mesenchymal stem cells,” InvestigativeOpthalmology & Visual Science, vol. 55, no. 7, pp. 4073–4083, 2014.
[22] J. Hu, Y. Wang, H. Gong et al., “Long term effect and safety ofWharton’s jelly-derived mesenchymal stem cells on type 2 dia-betes,” Experimental and Therapeutic Medicine, vol. 12, no. 3,pp. 1857–1866, 2016.
[23] M. L. Weiss, et al.C. Anderson, S. Medicetty et al., “Immuneproperties of human umbilical cord Wharton’s jelly-derivedcells,” Stem Cells, vol. 26, no. 11, pp. 2865–2874, 2008.
[24] F. Granero-Moltó, J. A. Weis, M. I. Miga et al., “Regenerativeeffects of transplanted mesenchymal stem cells in fracturehealing,” Stem Cells, vol. 27, no. 8, pp. 1887–1898, 2009.
[25] H. Kaneki, R. Guo, D. Chen et al., “Tumor necrosis factor pro-motes Runx2 degradation through up-regulation of Smurf1and Smurf2 in osteoblasts,” Journal of Biological Chemistry,vol. 281, no. 7, pp. 4326–4333, 2006.
[26] X. Zhou, et al.Z. Zhang, J. Q. Feng et al., “Multiple functions ofOsterix are required for bone growth and homeostasis in post-natal mice,” Proceedings of the National Academy of Sciences ofthe United States of America, vol. 107, no. 29, pp. 12919–12924, 2010.
[27] Y.-i. Kawabe, Y. X. Wang, I. W. McKinnell, M. T. Bedford, andM. A. Rudnicki, “Carm1 regulates Pax7 transcriptional activitythrough MLL1/2 recruitment during asymmetric satellite stemcell divisions,” Cell Stem Cell, vol. 11, no. 3, pp. 333–345, 2012.
[28] S. J. Prasanna, D. Gopalakrishnan, S. R. Shankar, and A. B.Vasandan, “Pro-inflammatory cytokines, IFNγ and TNFα,influence immune properties of human bone marrow andWharton jelly mesenchymal stem cells differentially,” PLoSOne, vol. 5, no. 2, article e9016, 2010.
[29] T. Deuse, M. Stubbendorff, K. Tang-Quan et al., “Immunoge-nicity and immunomodulatory properties of umbilical cordlining mesenchymal stem cells,” Cell Transplantation, vol. 20,no. 5, pp. 655–667, 2011.
[30] R. Sarugaser, D. Lickorish, D. Baksh, M. M. Hosseini, and J. E.Davies, “Human umbilical cord perivascular (HUCPV) cells: asource of mesenchymal progenitors,” Stem Cells, vol. 23, no. 2,pp. 220–229, 2005.
[31] S. B. Goodman, P. Huie, Y. Song et al., “Cellular profile andcytokine production at prosthetic interfaces: study of tissuesretrieved from revised hip and knee replacements,” The Jour-nal of Bone and Joint Surgery, vol. 80, no. 3, pp. 531–539, 1998.
[32] N. M. Moll and R. M. Ransohoff, “CXCL12 and CXCR4 inbone marrow physiology,” Expert Review of Hematology,vol. 3, no. 3, pp. 315–322, 2010.
14 Stem Cells International

[33] E. C. Butcher and L. J. Picker, “Lymphocyte homing andhomeostasis,” Science, vol. 272, no. 5258, pp. 60–67, 1996.
[34] L. da Silva Meirelles, A. M. Fontes, D. T. Covas, and A. I.Caplan, “Mechanisms involved in the therapeutic propertiesof mesenchymal stem cells,” Cytokine & Growth FactorReviews, vol. 20, no. 5-6, pp. 419–427, 2009.
[35] S. Zwingenberger, Z. Yao, A. Jacobi et al., “Enhancement ofBMP-2 induced bone regeneration by SDF-1α mediated stemcell recruitment,” Tissue Engineering Part A, vol. 20, no. 3-4,pp. 810–818, 2014.
[36] I. Majore, P. Moretti, F. Stahl, R. Hass, and C. Kasper, “Growthand differentiation properties of mesenchymal stromal cellpopulations derived from whole human umbilical cord,” StemCell Reviews and Reports, vol. 7, no. 1, pp. 17–31, 2011.
[37] S. Karahuseyinoglu, O. Cinar, E. Kilic et al., “Biology of stemcells in human umbilical cord stroma: in situ and in vitro sur-veys,” Stem Cells, vol. 25, no. 2, pp. 319–331, 2007.
[38] D. J. Hadjidakis and I. I. Androulakis, Bone Remodeling,Annals of the New York Academy of Sciences, 2006.
[39] U. Kini and B. N. Nandeesh, “Physiology of bone formation,remodeling, and metabolism,” in Radionuclide and HybridBone Imaging, pp. 29–57, Springer, Berlin, Heidelberg, 2012.
[40] L. J. Raggatt and N. C. Partridge, “Cellular and molecularmechanisms of bone remodeling,” Journal of Biological Chem-istry, vol. 285, no. 33, pp. 25103–25108, 2010.
[41] S. Kohli and V. Kohli, “Role of RANKL-RANK/osteoproteg-erin molecular complex in bone remodeling and its immuno-pathologic implications,” Indian Journal of Endocrinologyand Metabolism, vol. 15, no. 3, pp. 175–181, 2011.
[42] T. L. Andersen, M. E. Abdelgawad, H. B. Kristensen et al.,“Understanding coupling between bone resorption and forma-tion,” The American Journal of Pathology, vol. 183, no. 1,pp. 235–246, 2013.
[43] M. Borhani-Haghighi, T. Talaei-Khozani, M. Ayatollahi, andZ. Vojdani, “Wharton’s jelly-derived mesenchymal stem cellscan differentiate into hepatocyte-like cells by HepG2 cell lineextract,” Iranian Journal of Medical Sciences, vol. 40, no. 2,pp. 143–151, 2015.
[44] D. Bharti, S. B. Shivakumar, J.-K. Park et al., “Comparativeanalysis of human Wharton’s jelly mesenchymal stem cellsderived from different parts of the same umbilical cord,” Celland Tissue Research, vol. 372, no. 1, pp. 51–65, 2018.
[45] D. T. Denhardt and M. Noda, “Osteopontin expression andfunction: role in bone remodeling,” Journal of Cellular Bio-chemistry, vol. 72, no. S30-S31, pp. 92–102, 1998.
[46] J. Klein-Nulend, J. Roelofsen, C. M. Semeins, A. L. J. J. Bronck-ers, and E. H. Burger, “Mechanical stimulation of osteopontinmRNA expression and synthesis in bone cell cultures,” Journalof Cellular Physiology, vol. 170, no. 2, pp. 174–181, 1997.
[47] T. M. Liu and E. H. Lee, “Transcriptional regulatory cascadesin Runx2-dependent bone development,” Tissue EngineeringPart B: Reviews, vol. 19, no. 3, pp. 254–263, 2013.
[48] T. Komori, “Signaling networks in RUNX2-dependent bonedevelopment,” Journal of Cellular Biochemistry, vol. 112,no. 3, pp. 750–755, 2011.
[49] T. Komori, H. Yagi, S. Nomura et al., “Targeted disruption ofCbfa1 results in a complete lack of bone formation owing tomaturational arrest of osteoblasts,” Cell, vol. 89, no. 5,pp. 755–764, 1997.
[50] Q. Tu, J. Zhang, L. James et al., “Cbfa1/Runx2-deficiencydelays bone wound healing and locally delivered Cbfa1/Runx2
promotes bone repair in animal models,” Wound Repair andRegeneration, vol. 15, no. 3, pp. 404–412, 2007.
[51] J. H. Jonason, G. Xiao, M. Zhang, L. Xing, and D. Chen, “Post-translational regulation of Runx2 in bone and cartilage,” Jour-nal of Dental Research, vol. 88, no. 8, pp. 693–703, 2009.
[52] R. T. Franceschi, G. Xiao, D. Jiang, R. Gopalakrishnan, S. Yang,and E. Reith, “Multiple signaling pathways converge on theCbfa1/Runx2 transcription factor to regulate osteoblast differ-entiation,” Connective Tissue Research, vol. 44, no. 1, pp. 109–116, 2003.
[53] M. D. Yazid, S. H. Z. Ariffin, S. Senafi, M. A. Razak, and R. M.A. Wahab, “Determination of the differentiation capacities ofmurines’ primary mononucleated cells and MC3T3-E1 cells,”Cancer Cell International, vol. 10, no. 1, p. 42, 2010.
[54] F. Ng, S. Boucher, S. Koh et al., “PDGF, TGF-β, and FGF sig-naling is important for differentiation and growth of mesen-chymal stem cells (MSCs): transcriptional profiling canidentify markers and signaling pathways important in differ-entiation of MSCs into adipogenic, chondrogenic, and osteo-genic lineages,” Blood, vol. 112, no. 2, pp. 295–307, 2008.
[55] G. Xiao, D. Jiang, P. Thomas et al., “MAPK pathways activateand phosphorylate the osteoblast-specific transcription factor,Cbfa1,” Journal of Biological Chemistry, vol. 275, no. 6,pp. 4453–4459, 2000.
[56] N. Rucci, “Molecular biology of bone remodelling,” ClinicalCases in Mineral and Bone Metabolism, vol. 5, no. 1, pp. 49–56, 2008.
[57] L. F. Bonewald and G. R. Mundy, “Role of transforminggrowth factor-beta in bone remodeling,” Clinical Orthopaedicsand Related Research, no. 250, pp. 261–276, 1990.
[58] J. M. Hock, M. Centrella, and E. Canalis, “Insulin-like growthfactor I has independent effects on bone matrix formation andcell replication,” Endocrinology, vol. 122, no. 1, pp. 254–260,1988.
[59] R. M. Locklin, R. O. Oreffo, and J. T. Triffitt, “Effects of TGFβand BFGF on the differentiation of human bone marrow stro-mal fibroblasts,” Cell Biology International, vol. 23, no. 3,pp. 185–194, 1999.
[60] E. Torreggiani, G. Lisignoli, C. Manferdini et al., “Role of slugtranscription factor in human mesenchymal stem cells,” Jour-nal of Cellular and Molecular Medicine, vol. 16, no. 4, pp. 740–751, 2012.
[61] Á. Szepesi, Z. Matula, A. Szigeti et al., “In vitro characterizationof human mesenchymal stem cells isolated from different tis-sues with a potential to promote complex bone regeneration,”Stem Cells International, vol. 2016, Article ID 3595941, 9pages, 2016.
[62] A. Subramanian, C. Y. Fong, A. Biswas, and A. Bongso, “Com-parative characterization of cells from the various compart-ments of the human umbilical cord shows that theWharton’s jelly compartment provides the best source of clin-ically utilizable mesenchymal stem cells,” PLoS One, vol. 10,no. 6, article e0127992, 2015.
[63] F. Bustos, H. Sepúlveda, C. P. Prieto et al., “Runt-relatedtranscription factor 2 induction during differentiation ofWharton’s jelly mesenchymal stem cells to osteoblasts isregulated by Jumonji AT-rich interactive domain 1B histonedemethylase,” Stem Cells, vol. 35, no. 12, pp. 2430–2441,2017.
[64] Z. Qu, S. Mi, and G. Fang, “Clinical study on treatment of bonenonunion with MSCs derived from human umbilical cord,”
15Stem Cells International

Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi, vol. 23, no. 3,pp. 345–347, 2009.
[65] P. Li, K. Cui, B. Zhang et al., “Transplantation of humanumbilical cord-derived mesenchymal stems cells for the treat-ment of Becker muscular dystrophy in affected pedigree mem-bers,” International Journal of Molecular Medicine, vol. 35,no. 4, pp. 1051–1057, 2015.
[66] I. H. Dilogo, M. R. A. Primaputra, J. A. Pawitan, and I. K. Liem,“Modified Masquelet technique using allogeneic umbilicalcord-derived mesenchymal stem cells for infected non-unionfemoral shaft fracture with a 12 cm bone defect: a case report,”International Journal of Surgery Case Reports, vol. 34, pp. 11–16, 2017.
[67] J. Cai, Z. Wu, L. Huang et al., “Cotransplantation of bone mar-row mononuclear cells and umbilical cord mesenchymal stemcells in avascular necrosis of the femoral head,” Transplanta-tion Proceedings, vol. 46, no. 1, pp. 151–155, 2014.
[68] M. Shi, S. Yu, R. Xu, and F. S. Wang, “Human mesenchymalstem cell therapy is feasible for liver cirrhosis associated withHBV infection,” Hepatology International, vol. 10, no. 1,pp. S341–S342, 2016.
[69] N. Morishima, K. Nakanishi, K. Tsuchiya, T. Shibata, andE. Seiwa, “Translocation of Bim to the endoplasmic reticulum(ER) mediates ER stress signaling for activation of caspase-12during ER stress-induced apoptosis,” Journal of BiologicalChemistry, vol. 279, no. 48, pp. 50375–50381, 2004.
[70] A. Patel and N. Riordan, “Allogeneic transplantation of humanumbilical cord mesenchymal stem cells (UC-MSC) for a singlemale patient with duchenne muscular dystrophy (DMD),”Cytotherapy, vol. 17, no. 6, article S46, 2015.
[71] D.-W. Kim, M. Staples, K. Shinozuka, P. Pantcheva, S.-D. Kang, and C. Borlongan, “Wharton’s jelly-derived mesen-chymal stem cells: phenotypic characterization and optimizingtheir therapeutic potential for clinical applications,” Interna-tional Journal of Molecular Sciences, vol. 14, no. 6,pp. 11692–11712, 2013.
[72] A. Can, F. T. Celikkan, and O. Cinar, “Umbilical cord mesen-chymal stromal cell transplantations: a systemic analysis ofclinical trials,” Cytotherapy, vol. 19, no. 12, pp. 1351–1382,2017.
[73] M. S. Choudhery, M. Badowski, A. Muise, J. Pierce, and D. T.Harris, “Donor age negatively impacts adipose tissue-derivedmesenchymal stem cell expansion and differentiation,” Journalof Translational Medicine, vol. 12, no. 1, p. 8, 2014.
[74] O. Karadas, D. Yucel, H. Kenar, G. Torun Kose, and V. Hasirci,“Collagen scaffolds with in situ-grown calcium phosphate forosteogenic differentiation of Wharton’s jelly and menstrualblood stem cells,” Journal of Tissue Engineering and Regenera-tive Medicine, vol. 8, no. 7, pp. 534–545, 2014.
[75] M. Torkaman, M. Ghollasi, M. Mohammadnia-Afrouzi,A. Salimi, and A. Amari, “The effect of transplanted humanWharton’s jelly mesenchymal stem cells treated with IFN-γon experimental autoimmune encephalomyelitis mice,” Cellu-lar Immunology, vol. 311, pp. 1–12, 2017.
[76] K. O’Donoghue, M. Choolani, J. Chan et al., “Identification offetal mesenchymal stem cells in maternal blood: implicationsfor non-invasive prenatal diagnosis,” Molecular HumanReproduction, vol. 9, no. 8, pp. 497–502, 2003.
[77] D. Baksh, R. Yao, and R. S. Tuan, “Comparison of proliferativeand multilineage differentiation potential of human mesen-chymal stem cells derived from umbilical cord and bone mar-row,” Stem Cells, vol. 25, no. 6, pp. 1384–1392, 2007.
[78] I. Arutyunyan, A. Elchaninov, A. Makarov, andT. Fatkhudinov, “Umbilical cord as prospective source formesenchymal stem cell-based therapy,” Stem Cells Interna-tional, vol. 2016, Article ID 6901286, 17 pages, 2016.
[79] J. Lim, Z. R. M. Razi, J. Law, A. M. Nawi, R. B. H. Idrus, andM. H. Ng, “MSCs can be differentially isolated from maternal,middle and fetal segments of the human umbilical cord,”Cytotherapy, vol. 18, no. 12, pp. 1493–1502, 2016.
[80] S. Kargozar, M. Mozafari, S. J. Hashemian et al., “Osteogenicpotential of stem cells-seeded bioactive nanocomposite scaf-folds: a comparative study between human mesenchymal stemcells derived from bone, umbilical cord Wharton’s jelly, andadipose tissue,” Journal of Biomedical Materials Research PartB: Applied Biomaterials, vol. 106, no. 1, pp. 61–72, 2018.
[81] M. R. Todeschi, R. el Backly, C. Capelli et al., “Transplantedumbilical cord mesenchymal stem cells modify the in vivomicroenvironment enhancing angiogenesis and leading tobone regeneration,” Stem Cells and Development, vol. 24,no. 13, pp. 1570–1581, 2015.
[82] L. Polo-Corrales, M. Latorre-Esteves, and J. E. Ramirez-Vick,“Scaffold design for bone regeneration,” Journal ofNanoscience and Nanotechnology, vol. 14, no. 1, pp. 15–56,2014.
[83] A. K. Batsali, C. Pontikoglou, D. Koutroulakis et al., “Differen-tial expression of cell cycle and WNT pathway-related genesaccounts for differences in the growth and differentiationpotential of Wharton’s jelly and bone marrow-derived mesen-chymal stem cells,” Stem Cell Research & Therapy, vol. 8, no. 1,p. 102, 2017.
[84] A. Zajdel, M. Kałucka, E. Kokoszka-Mikołaj, and A. Wilczok,“Osteogenic differentiation of human mesenchymal stem cellsfrom adipose tissue andWharton’s jelly of the umbilical cord,”Acta Biochimica Polonica, vol. 64, no. 2, pp. 365–369, 2017.
[85] R. K. Schneider, A. Puellen, R. Kramann et al., “The osteogenicdifferentiation of adult bone marrow and perinatal umbilicalmesenchymal stem cells and matrix remodelling in three-dimensional collagen scaffolds,” Biomaterials, vol. 31, no. 3,pp. 467–480, 2010.
[86] S. Bose, M. Roy, and A. Bandyopadhyay, “Recent advances inbone tissue engineering scaffolds,” Trends in Biotechnology,vol. 30, no. 10, pp. 546–554, 2012.
[87] H. W. Sun, R. J. Feigal, and H. H. Messer, “Cytotoxicity of glu-taraldehyde and formaldehyde in relation to time of exposureand concentration,” Pediatric Dentistry, vol. 12, no. 5, pp. 303–307, 1990.
[88] S. Mechiche Alami, H. Rammal, C. Boulagnon-Rombi et al.,“Harnessing Wharton’s jelly stem cell differentiation intobone-like nodule on calcium phosphate substrate withoutosteoinductive factors,” Acta Biomaterialia, vol. 49, pp. 575–589, 2017.
[89] L. Penolazzi, S. Mazzitelli, R. Vecchiatini et al., “Human mes-enchymal stem cells seeded on extracellular matrix-scaffold:viability and osteogenic potential,” Journal of Cellular Physiol-ogy, vol. 227, no. 2, pp. 857–866, 2012.
[90] K. E. Mitchell, M. L. Weiss, B. M. Mitchell et al., “Matrix cellsfrom Wharton’s jelly form neurons and glia,” Stem Cells,vol. 21, no. 1, pp. 50–60, 2003.
[91] Y. S. Fu, C. H. Lu, K. A. Chu et al., “Xenograft of human umbil-ical mesenchymal stem cells from Wharton’s jelly differentiat-ing into osteocytes and reducing osteoclast activity reversesosteoporosis in ovariectomized rats,” Cell Transplantation,vol. 27, no. 1, pp. 194–208, 2018.
16 Stem Cells International

[92] F. E. Al Jofi, T. Ma, D. Guo et al., “Functional organic cationtransporters mediate osteogenic response to metformin inhuman umbilical cord mesenchymal stromal cells,” Cytother-apy, vol. 20, no. 5, pp. 650–659, 2018.
[93] A. Ramesh, M.M. Kanafi, and R. R. Bhonde, “Modulus-depen-dent characteristics of Wharton’s jelly mesenchymal stem cells(WJMSC) encapsulated in hydrogel microspheres,” Journal ofBiomaterials Science, Polymer Edition, vol. 25, no. 17,pp. 1946–1961, 2014.
[94] L. Wang, L. Zhao, and M. S. Detamore, “Human umbilicalcord mesenchymal stromal cells in a sandwich approach forosteochondral tissue engineering,” Journal of Tissue Engineer-ing and Regenerative Medicine, vol. 5, no. 9, pp. 712–721, 2011.
17Stem Cells International

Hindawiwww.hindawi.com
International Journal of
Volume 2018
Zoology
Hindawiwww.hindawi.com Volume 2018
Anatomy Research International
PeptidesInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Journal of Parasitology Research
GenomicsInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Hindawiwww.hindawi.com Volume 2018
BioinformaticsAdvances in
Marine BiologyJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Neuroscience Journal
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
Cell BiologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Biochemistry Research International
ArchaeaHindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Genetics Research International
Hindawiwww.hindawi.com Volume 2018
Advances in
Virolog y Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Enzyme Research
Hindawiwww.hindawi.com Volume 2018
International Journal of
MicrobiologyHindawiwww.hindawi.com
Nucleic AcidsJournal of
Volume 2018
Submit your manuscripts atwww.hindawi.com